
Complete Response in Metastatic Hepatocellular Carcinoma with Cardiac and Lung Involvement via Multimodality Treatment

 , , , and
, , , and 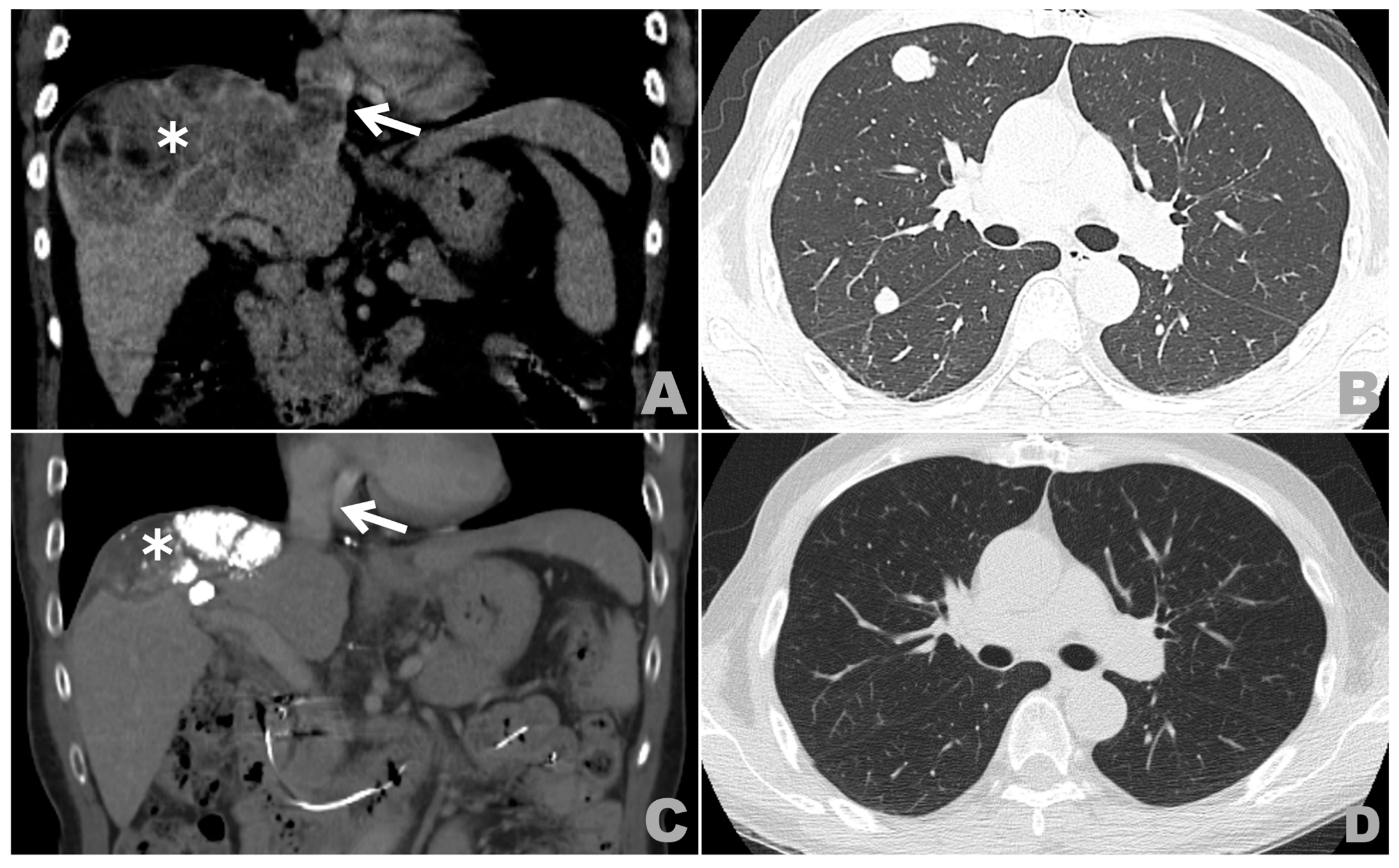{kind=link}
{kind=link}
Abstract
:1. Introduction
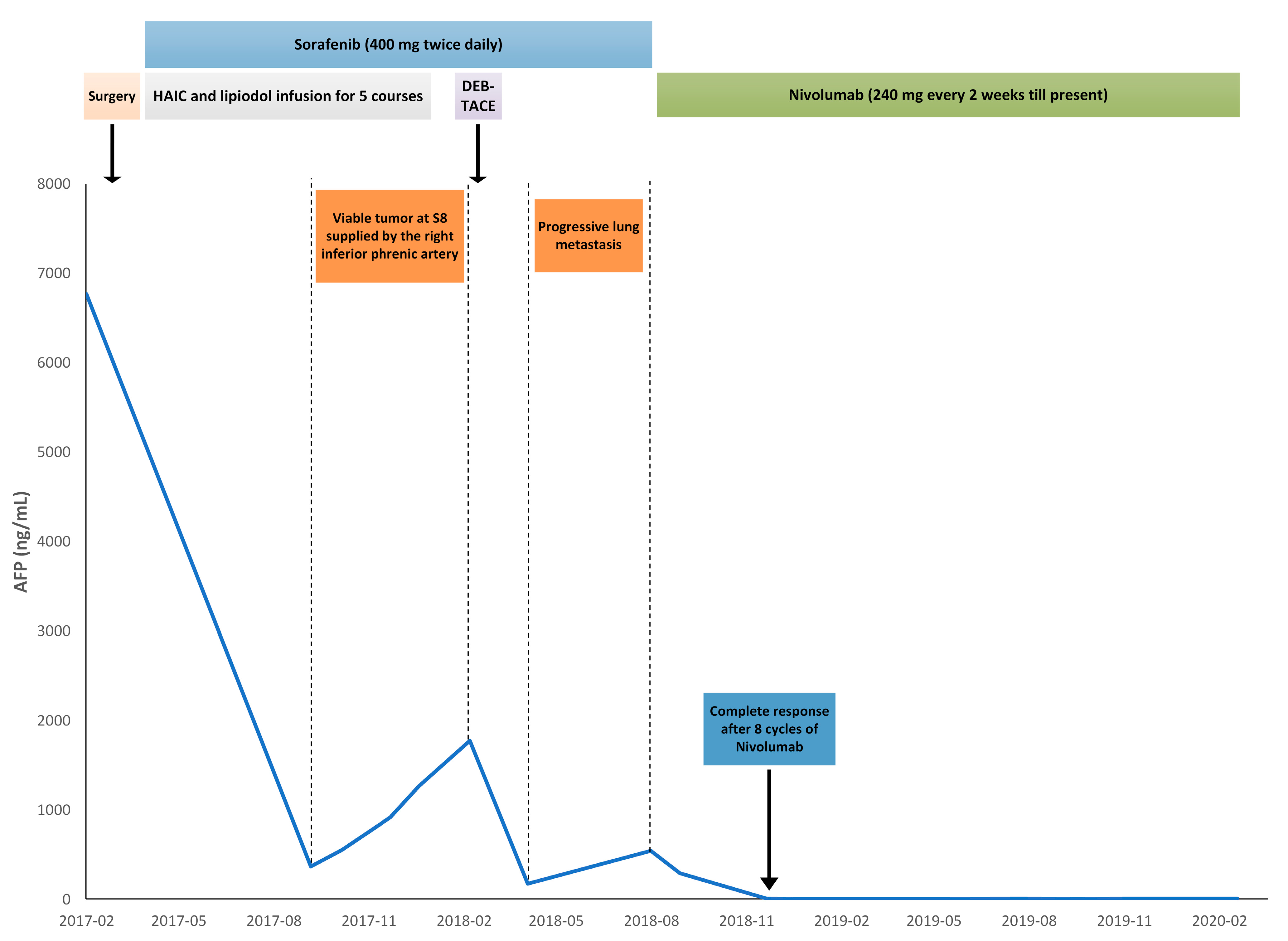
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wakayama, K.; Kamiyama, T.; Yokoo, H.; Kakisaka, T.; Kamachi, H.; Tsuruga, Y.; Nakanishi, K.; Shimamura, T.; Todo, S.; Taketomi, A. Surgical management of hepatocellular carcinoma with tumor thrombi in the inferior vena cava or right atrium. World J. Surg. Oncol. 2013, 11, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.T.; Tsai, K.F.; Leung, H.W.; Chan, A.L.; Wang, S.Y.; Liang, H.L.; Tang, S.Y.; Chou, C.K.; Chen, H.Y.; Chan, S.H.; et al. Hepatic Arterial Infusion Chemotherapy Followed by Lipiodol Infusion for Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: A Single-Center Experience. Medicina 2021, 57, 779. [Google Scholar] [CrossRef]
- Lee, I.J.; Chung, J.W.; Kim, H.C.; Yin, Y.H.; So, Y.H.; Jeon, U.B.; Jae, H.J.; Cho, B.H.; Park, J.H. Extrahepatic collateral artery supply to the tumor thrombi of hepatocellular carcinoma invading inferior vena cava: The prevalence and determinant factors. J. Vasc. Interv. Radiol. 2009, 20, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bustamante, J.; Castells, A.; Vilana, R.; Ayuso, M.D.C.; Sala, M.; Brú, C.; Rodés, J.; Bruix, J. Natural history of untreated nonsurgical hepatocellular carcinoma: Rationale for the design and evaluation of therapeutic trials. Hepatology 1999, 29, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yuan, L.; Ge, R.L.; Sun, Y.; Wei, G. Survival benefit of surgical treatment for hepatocellular carcinoma with inferior vena cava/right atrium tumor thrombus: Results of a retrospective cohort study. Ann. Surg. Oncol. 2013, 20, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Bangaru, S.; Marrero, J.A.; Singal, A.G. Review article: New therapeutic interventions for advanced hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2020, 51, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Ray, C.E., Jr.; Brown, A.C.; Green, T.J.; Winston, H.; Curran, C.; Kreidler, S.M.; Glueck, D.H.; Rochon, P.J. Survival outcomes in patients with advanced hepatocellular carcinoma treated with drug-eluting bead chemoembolization. AJR Am. J. Roentgenol. 2015, 204, 440–447. [Google Scholar] [CrossRef] [PubMed]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H., III; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, K.-F.; Tsai, J.C.H.; Li, M.-F.; Tan, J.W.H.; Chou, C.-K.; Liang, H.-L.; Chan, S.-H. Complete Response in Metastatic Hepatocellular Carcinoma with Cardiac and Lung Involvement via Multimodality Treatment. Medicina 2021, 57, 849. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080849
Tsai K-F, Tsai JCH, Li M-F, Tan JWH, Chou C-K, Liang H-L, Chan S-H. Complete Response in Metastatic Hepatocellular Carcinoma with Cardiac and Lung Involvement via Multimodality Treatment. Medicina. 2021; 57(8):849. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080849
Chicago/Turabian StyleTsai, Kun-Feng, Jerry C. H. Tsai, Ming-Feng Li, Jimmy W. H. Tan, Chu-Kuang Chou, Huei-Lung Liang, and Shan-Ho Chan. 2021. "Complete Response in Metastatic Hepatocellular Carcinoma with Cardiac and Lung Involvement via Multimodality Treatment" Medicina 57, no. 8: 849. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57080849