
Differences in Femoral Artery Occlusion Pressure between Sexes and Dominant and Non-Dominant Legs

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Blood Flow Measurements
2.4. Measurement of Arterial Occlusion Pressure
2.5. Measurement of Arterial Blood Flow
2.6. Data Analysis
3. Results
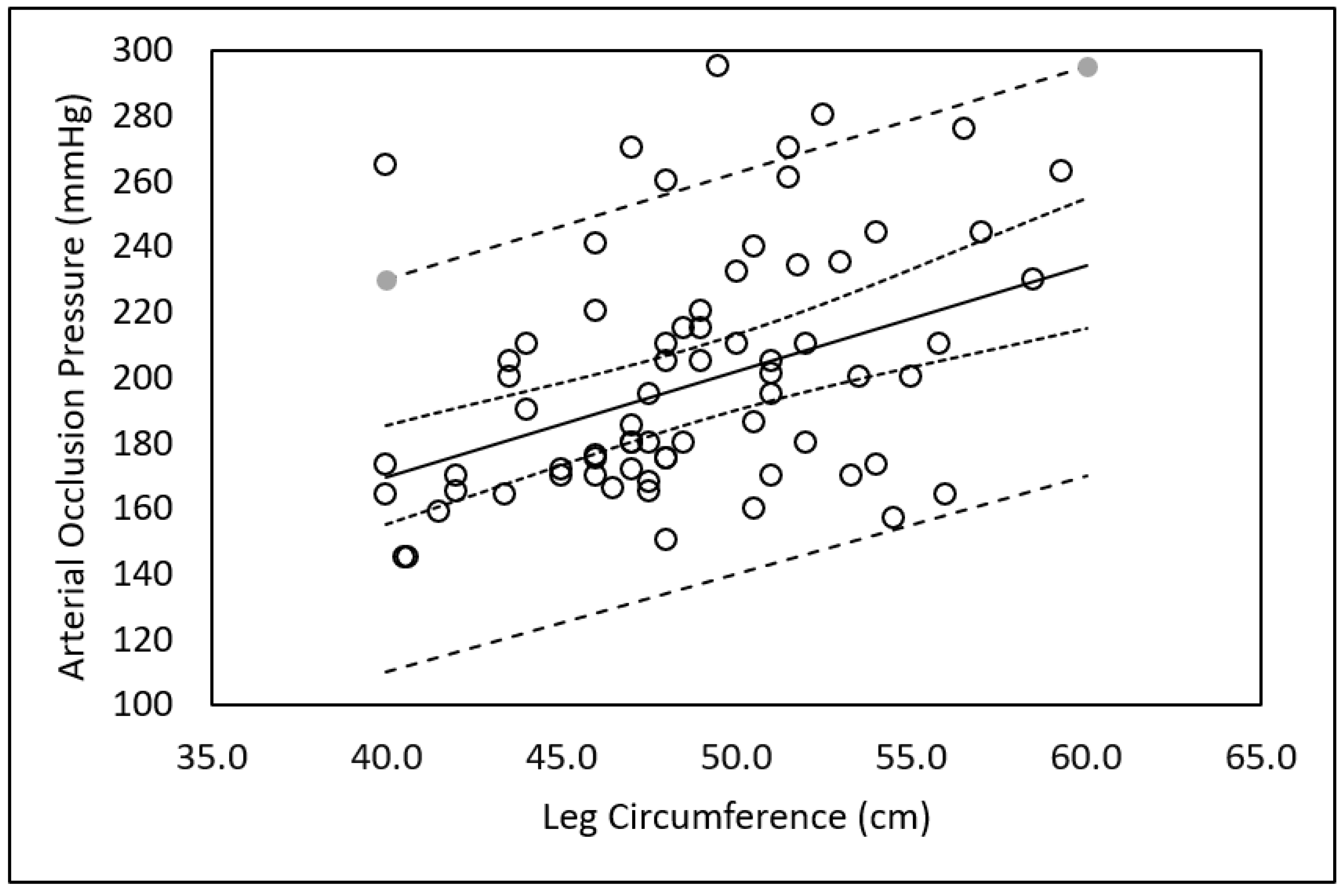
3.1. Arterial Occlusion Pressure
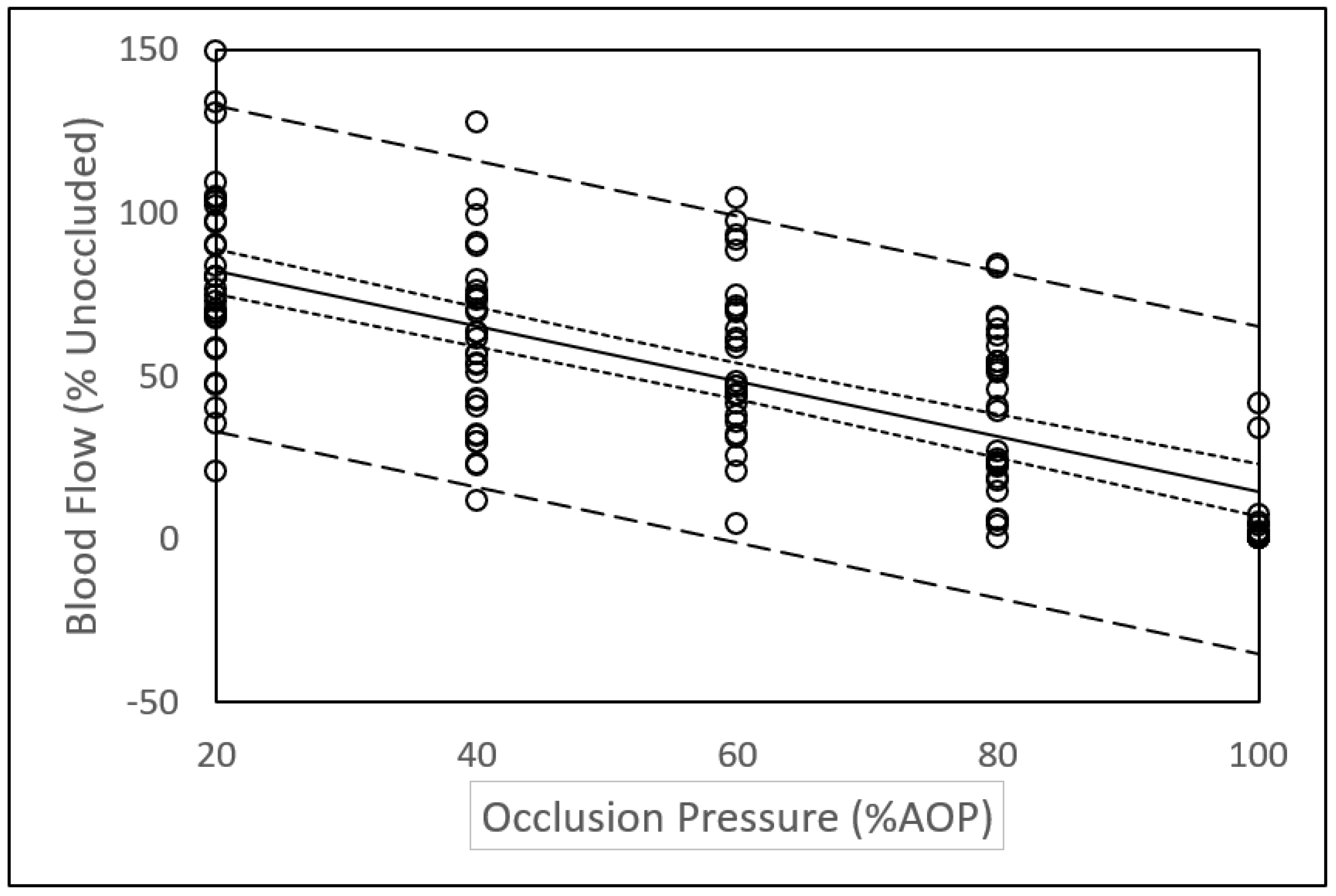
3.2. Arterial Blood Flow
4. Discussion
4.1. Sex and Limb Differences in Arterial Occlusion Pressure
4.2. Arterial Blood Flow
4.3. Variance in Blood Flow Measurements
4.4. Study Limitations
4.5. Direction for Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loenneke, J.P.; Wilson, J.M.; Marin, P.J.; Zourdos, M.C.; Bemben, M.G. Low intensity blood flow restriction training: A meta-analysis. Eur. J. Appl. Physiol. 2012, 112, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Staunton, C.A.; May, A.K.; Brandner, C.R.; Warmington, S.A. Haemodynamics of aerobic and resistance blood flow restriction exercise in young and older adults. Eur. J. Appl. Physiol. 2015, 115, 2293–2302. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Wilson, J.M.; Bemben, M.G. Blood flow restriction: The metabolite/volume threshold theory. Med. Hypotheses 2011, 77, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Loenneke, J.P.; Ye, X.; Bemben, D.A.; Beck, T.W.; Larson, R.D.; Bemben, M.G. Low-load resistance training with low relative pressure produces muscular changes similar to high-load resistance training. Muscle Nerve 2017, 56, E126–E133. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Exercise with blood flow restriction: An updated evidence-based approach for enhanced muscular development. Sports Med. 2015, 45, 313–325. [Google Scholar] [CrossRef]
- Pope, Z.K.; Willardson, J.M.; Schoenfeld, B.J. Exercise and blood flow restriction. J. Strength Cond. Res. 2013, 27, 2914–2926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iida, H.; Takano, H.; Meguro, K.; Asada, K.; Oonuma, H.; Morita, T.; Kurano, M.; Sakagami, F.; Uno, K.; Hirose, K.; et al. Hemodynamic and autonomic nervous responses to the restriction of femoral blood flow by KAATSU. Int. J. KAATSU Train. Res. 2005, 1, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Iida, H.; Kurano, M.; Takano, H.; Kubota, N.; Morita, T.; Meguro, K.; Sato, Y.; Abe, T.; Yamazaki, Y.; Uno, K.; et al. Hemodynamic and neurohumoral responses to the restriction of femoral blood flow by KAATSU in healthy subjects. Eur. J. Appl. Physiol. 2007, 100, 275–285. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Pujol, T.J. The Use of Occlusion Training to Produce Muscle Hypertrophy. Strength Cond. J. 2009, 31, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Lowery, R.P.; Joy, J.M.; Loenneke, J.P.; de Souza, E.; Machado, M.; Dudeck, J.E.; Wilson, J.M. Practical blood flow restriction training increases muscle hypertrophy during a periodized resistance training programme. Clin. Phsiol. Funct. Imaging 2014, 34, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Lowery, R.P.; Joy, J.M.; Loenneke, J.P.; Naimo, M.A. Practical blood flow restriction training increases acute determinants on hypertrophy without increasing indices of muscle damage. J. Strength Cond. Res. 2013, 27, 3068–3075. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.E.; Stodart, C.; Ferguson, R.A. The influence of participant characteristics on the relationship between cuff pressure and level of blood flow restriction. Eur. J. Appl. Physiol. 2016, 116, 1421–1432. [Google Scholar] [CrossRef] [Green Version]
- Meister, C.B.; Kutianski, F.A.T.; Carstens, L.C.; Andrade, S.L.F.; Rodacki, A.L.F.; Martins de Souza, R. Effects of two programs of metabolic resistance training on strength and hypertrophy. Fisioterpia Mov. 2016, 29, 147–155. [Google Scholar] [CrossRef]
- Pope, Z.K.; Willardson, J.M.; Schoenfeld, B.J.; Emmett, J.; Owen, J.D. Hypertrophic and strength response to exxcentric resistance training with blood flow restriction. Int. J. Sports Sci. 2015, 10, 919–931. [Google Scholar]
- Sumide, T.; Sakuraba, K.; Sawaki, K.; Ohmura, H.; Tamura, Y. Effect of resistance exercise training combined with relatively low vascular occlusion. J. Sci. Med. Sport 2009, 12, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Wernbom, M.; Augustsson, J.; Thomee, R. Effects of vascular occlusion on muscular endurance in dynamic knee extension exercise at different submaximal loads. J. Strength Cond. Res. 2006, 20, 372–377. [Google Scholar] [CrossRef] [PubMed]
- McEwen, J.A.; Owens, J.G.; Jeyasurya, J. Why is it crucial to use personalized occlusion pressures in blood flow restriction (BFR) rehabilitation? J. Med. Biol. Eng. 2019, 39, 173–177. [Google Scholar] [CrossRef] [Green Version]
- Jessee, M.B.; Buckner, S.L.; Mouser, J.G.; Mattocks, K.T.; Loenneke, J.P. Letter to the editor: Applying the blood flow restriction pressure: The elephant in the room. Am. J. Physiol. Heart Circ. Physiol. 2016, 310, H132–H133. [Google Scholar] [CrossRef] [Green Version]
- Loenneke, J.P.; Thiebaud, R.S.; Fahs, C.A.; Rossow, L.M.; Abe, T.; Bemben, M.G. Blood flow restriction does not result in prolonged decrements in torque. Eur. J. Appl. Physiol. 2013, 113, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Sherk, V.D.; Thiebaud, R.S.; Abe, T.; Bemben, D.A.; Bemben, M.G. Effects of cuff width on arterial occlusion: Implications for blood flow restricted exercise. Eur. J. Appl. Physiol. 2012, 112, 2903–2912. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Allen, K.M.; Mouser, J.G.; Thiebaud, R.S.; Kim, D.; Abe, T.; Bemben, M.G. Blood flow restriction in the upper and lower limbs is predicted by limb circumference and systolic blood pressure. Eur. J. Appl. Physiol. 2015, 115, 397–405. [Google Scholar] [CrossRef]
- Barnett, B.E.; Dankel, S.J.; Counts, B.R.; Nooe, A.L.; Abe, T.; Loenneke, J.P. Blood flow occlusion pressure at rest and immediately after a bout of low load exercise. Clin. Physiol. Funct. Imaging 2016, 36, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Counts, B.R.; Dankel, S.J.; Barnett, B.E.; Kim, D.; Mouser, J.G.; Allen, K.M.; Thiebaud, R.S.; Abe, T.; Bemben, M.G.; Loenneke, J.P. Influence of relative blood flow restriction pressure on muscle activation and muscle adaptation. Muscle Nerve 2016, 53, 438–445. [Google Scholar] [CrossRef]
- Brandner, C.R.; Kidgell, D.J.; Warmington, S.A. Unilateral bicep curl hemodynamics: Low-pressure continuous vs high-pressure intermittent blood flow restriction. Scand. J. Med. Sci. Sports 2015, 25, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Mouser, J.G.; Dankiel, S.J.; Mattocks, K.T.; Jessee, M.B.; Buckner, S.L.; Abe, T.; Loenneke, J.P. Blood flow restriction and cuff width: Effect on blood flow in the legs. Clin. Phsiol. Funct. Imaging 2018, 38, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Crossley, K.W.; Porter, D.A.; Ellsworth, J.; Caldwell, T.; Feland, J.B.; Mitchell, U.H.; Johnson, A.W.; Egget, D.; Gifford, J.R. Effect of cuff pressure on blood flow during blood flow-restricted rest and exercise. Med. Sci. Sports Exerc. 2019, 52, 746–753. [Google Scholar] [CrossRef]
- Jessee, M.B.; Buckner, S.L.; Dankel, S.J.; Counts, B.R.; Abe, T.; Loenneke, J.P. The Influence of Cuff Width, Sex, and Race on Arterial Occlusion: Implications for Blood Flow Restriction Research. Sports Med. 2016, 46, 913–921. [Google Scholar] [CrossRef]
- Mattocks, K.T.; Jessee, M.B.; Counts, B.R.; Buckner, S.L.; Grant Mouser, J.; Dankel, S.J.; Laurentino, G.C.; Loenneke, J.P. The effects of upper body exercise across different levels of blood flow restriction on arterial occlusion pressure and perceptual responses. Physiol. Behav. 2017, 171, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Sieljacks, P.; Knudsen, L.; Wernbom, M.; Vissing, K. Body position influences arterial occlusion pressure: Implications for the standardization of pressure during blood flow restricted exercise. Eur. J. Appl. Physiol. 2018, 118, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.G.; van Cingel, R.E.H. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spitz, R.W.; Chatakondi, R.N.; Bell, Z.W.; Wong, V.; Dankel, S.J.; Abe, T.; Loenneke, J.P. The impact of cuff width and biological sex on cuff prefference and the percieve discomfort to blood-flow-restricted exercise. Physiol. Meas. 2019, 40, 055001. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.; Abe, T.; Chatakondi, R.N.; Bell, Z.W.; Spitz, R.W.; Dankel, S.J.; Loenneke, J.P. The influence of biological sex and cuff width on muscle swelling, echo intensity, and the fatigue response to blood flow restricted exercise. J. Sports Sci. 2019, 37, 1865–1873. [Google Scholar] [CrossRef]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Blood flow restricted exercise for athletes: A review of available evidence. J. Sci. Med. Sport 2016, 19, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Mouser, J.G.; Ade, C.J.; Black, C.D.; Bemben, D.A.; Bemben, M.G. Brachial blood flow under relative levels of blood flow restriction in decreased in a nonlinear fashion. Clin. Physiol. Funct. Imaging 2018, 38, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Mouser, J.G.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Buckner, S.L.; Counts, B.R.; Loenneke, J.P. A tale of three cuffs: The hemodynamics of blood flow restriction. Eur. J. Appl. Physiol. 2017, 117, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Spranger, M.D.; Krishnan, A.C.; Levy, P.D.; O’Leary, D.S.; Smith, S.A. Blood flow restriction training and the exercise pressor reflex: A call for concern. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H1440–H1452. [Google Scholar] [CrossRef] [PubMed]
- Lewis, P.; Psaila, J.V.; Davies, W.T.; McCarty, K.; Woodcock, J.P. Measurement of volume flow in the human common femoral artery using a duplex ultrasound system. Ultrasound Med. Biol. 1986, 12, 777–784. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Males (N = 16) | Females (N = 19) | Combined (N = 35) | |
|---|---|---|---|
| Age (years) | 23.8 ± 3.6 | 22.9 ± 3.5 | 23.3 ± 3.5 |
| Height (cm) * | 177.6 ± 5.3 | 166.9 ± 8.7 | 171.8 ± 9.1 |
| Body Mass (kg) * | 75.4 ± 10.6 | 63.6 ± 9.6 | 68.8 ± 11.6 |
| BMI (kg/m2) | 23.9 ± 3.6 | 22.7 ± 2.9 | 23.3 ± 3.2 |
| SBP (mmHg) * | 122 ± 5.5 | 114 ± 5 | 117 ± 6.5 |
| DBP (mmHg) | 73 ± 6.4 | 71 ± 6 | 72 ± 6.3 |
| MAP (mmHg) * | 90 ± 5.7 | 85 ± 5 | 87 ± 5.6 |
| Thigh Skinfold (mm) | |||
| Dominant Leg | 25.8 ± 11.0 | 32.6 ± 9.2 | 29.5 ± 10.5 |
| Non-dominant Leg | 25.9 ± 11.6 | 32.8 ± 8.8 | 29.6 ± 10.6 |
| Difference | 0.12 ± 1.63 | 0.26 ± 2.1 | 0.2 ± 1.87 |
| Thigh Circumference (cm) | |||
| Dominant Leg | 48.8 ± 4.2 | 49.2 ± 4.9 | 49.0 ± 4.5 |
| Non-dominant Leg | 47.9 ± 4.5 | 48.5 ± 4.9 | 48.3 ± 4.7 |
| Difference | 0.91 ± 2.6 | 0.68 ± 1.6 | 0.78 ± 2.12 |
| Arterial Occlusion Pressure (AOP) | |||
| Dominant Leg * | 230 ± 41 | 191 ± 27 | 209 ± 39 |
| Non-dominant Leg * | 209 ± 37 | 178 ± 21 | 192 ± 33 |
| Difference | 21 ± 28.7 ^ | 13 ± 27.3 | 17 ± 27.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tafuna’i, N.D.; Hunter, I.; Johnson, A.W.; Fellingham, G.W.; Vehrs, P.R. Differences in Femoral Artery Occlusion Pressure between Sexes and Dominant and Non-Dominant Legs. Medicina 2021, 57, 863. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090863
Tafuna’i ND, Hunter I, Johnson AW, Fellingham GW, Vehrs PR. Differences in Femoral Artery Occlusion Pressure between Sexes and Dominant and Non-Dominant Legs. Medicina. 2021; 57(9):863. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090863
Chicago/Turabian StyleTafuna’i, Nicole D., Iain Hunter, Aaron W. Johnson, Gilbert W. Fellingham, and Pat R. Vehrs. 2021. "Differences in Femoral Artery Occlusion Pressure between Sexes and Dominant and Non-Dominant Legs" Medicina 57, no. 9: 863. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090863