
Association between Bone Mineral Density and Bone Turnover Markers in Breast Cancer Patients and Bone-Only Metastasis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurement of Bone Mineral Density (BMD)
2.2. Measurement of Concentrations of Bone Turnover Markers
2.2.1. Measurement of Concentrations of Serum NTx
2.2.2. Measurement of Concentrations of Urine α-CTx
2.2.3. Measurement of Concentrations of Tumor Markers
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clemons, M.; Cole, D.E.C.; Gainford, M.C. Can bone markers guide more effective treatment of bone metastases from breast cancer? Breast Cancer Res. Treat. 2006, 97, 81–90. [Google Scholar] [CrossRef]
- Zulauf, N.; Brüggmann, D.; Groneberg, D.; Oremek, G.M. Expressiveness of bone markers in breast cancer with bone metastases. Oncology 2019, 97, 236–244. [Google Scholar] [CrossRef]
- Kamby, C. The pattern of metastases in human breast cancer: Methodological aspects and influence of prognostic factors. Cancer Treat. Rev. 1990, 17, 37–61. [Google Scholar] [CrossRef]
- Cook, G.J.R.; Azad, G.K.; Goh, V. Imaging bone metastases in breast cancer: Staging and response assessment. J. Nucl. Med. 2016, 57, 27S–33S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires, A.O.; Borges, U.S.; Lopes-Costa, P.V.; Gebrim, L.H.; da Silva, B.B. Evaluation of bone metastases from breast cancer by bone scintigraphy and positron emission tomography/computed tomography imaging. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 180, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Xinhua, Q.; Zhang, X.; Qin, A.; Guangwang, L.; Zhai, Z.; Hao, Y.; Huiwu, L.; Zhu, Z.; Dai, K. Bone mineral density and risk of breast cancer in postmenopausal women. Breast Cancer Res. Treat. 2013, 138, 261–271. [Google Scholar]
- Arnaud, C.D. Osteoporosis: Using ‘bone markers’ for diagnosis and monitoring. Geriatrics (Basel Switz.) 1996, 51, 24–30. [Google Scholar]
- Giuliano, A.E.; Connolly, J.L.; Edge, S.B.; Mittendorf, E.A.; Rugo, H.S.; Solin, L.J.; Weaver, D.L.; Winchester, D.J.; Hortobagyi, G.N. Breast cancer—Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA A Cancer J. Clin. 2017, 67, 290–303. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.E.; Major, P.; Lipton, A.; Brown, J.E.; Lee, K.A.; Smith, M.; Saad, F. Predictive value of bone resorption and formation markers in cancer patients with bone metastases receiving the bisphosphonate zoledronic acid. J. Clin. Oncol. 2005, 23, 4925–4935. [Google Scholar] [CrossRef]
- Ali, S.M.; Demers, L.M.; Leitzel, K.; Harvey, H.A.; Clemens, D.; Mallinak, N.; Engle, L.; Chinchilli, V.; Costa, L.; Brady, C.; et al. Baseline serum NTx levels are prognostic in metastatic breast cancer patients with bone-only metastasis. Ann. Oncol. 2004, 15, 455–459. [Google Scholar] [CrossRef]
- Clemons, M.J.; Dranitsaris, G.; Ooi, W.S.; Yogendran, G.; Sukovic, T.; Wong, B.Y.L.; Verma, S.; Pritchard, K.I.; Trudeau, M.; Cole, D.E.C. Phase II trial evaluating the palliative benefit of second-line zoledronic acid in breast cancer patients with either a skeletal-related event or progressive bone metastases despite first-line bisphosphonate therapy. J. Clin. Oncol. 2006, 24, 4895–4900. [Google Scholar] [CrossRef]
- Costa, L.; Demers, L.M.; Oliveira, A.G.; Schaller, J.; Costa, E.B.; De Moura, M.C.; Allan, L. Prospective evaluation of the peptide-bound collagen type I cross-links N-telopeptide and C-telopeptide in predicting bone metastases status. J. Clin. Oncol. 2002, 20, 850–856. [Google Scholar] [CrossRef]
- Brown, J.; Rathbone, E.; Hinsley, S.; Gregory, W.; Fatma, G.; Marshall, H.; Burkinshaw, R.; Shulver, H.; Thandar, H.; Thandar, H.; et al. Associations between serum bone biomarkers in early breast cancer and development of bone metastasis: Results from the AZURE (BIG01/04) trial. JNCI J. Natl. Cancer Inst. 2018, 110, 871–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cloos, P.A.C.; Christgau, S.; Lyubimova, N.; Body, J.J.; Qvist, P. Christiansen, C. Breast cancer patients with bone metastases are characterised by increased levels of nonisomerised type I collagen fragments. Breast Cancer Res. 2003, 5, 1–7. [Google Scholar]
- Xiong, Z.; Deng, G.; Huang, X.; Li, X.; Xie, X.; Wang, J.; Shuang, Z.; Wang, X. Bone metastasis pattern in initial metastatic breast cancer: A population-based study. Cancer Manag. Res. 2018, 10, 287–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leeming, D.J.; Delling, G.; Koizumi, M.; Henriksen, K.; Karsdal, M.A.; Li, B.; Qvist, P.; Tankó, L.B.; Byrjalsen, I. Alpha CTX as a biomarker of skeletal invasion of breast cancer: Immunolocalization and the load dependency of urinary excretion. Cancer Epidemiol. Prev. Biomark. 2006, 15, 1392–1395. [Google Scholar] [CrossRef] [Green Version]
- Christgau, S.; Rosenquist, C.; Alexandersen, P.; Bjarnason, N.H.; Ravn, P.; Fledelius, C.; Herling, C.; Qvist, P.; Christiansen, C. Clinical evaluation of the Serum CrossLaps One Step ELISA, a new assay measuring the serum concentration of bone-derived degradation products of type I collagen C-telopeptides. Clin. Chem. 1998, 44, 2290–2300. [Google Scholar] [CrossRef] [Green Version]
- Rosen, H.N.; Moses, A.C.; Garber, J.; Iloputaife, I.D.; Ross, D.S.; Lee, S.L.; Greenspan, S.L. Serum CTX: A new marker of bone resorption that shows treatment effect more often than other markers because of low coefficient of variability and large changes with bisphosphonate therapy. Calcif. Tissue Int. 2000, 66, 100–103. [Google Scholar] [CrossRef]
- Nguyen-Pamart, M.; Caty, A.; Feutrie, M.L.; Fournier, C.; Gosselin, P.; Mazeman, E. The diagnostic value of urinary Crosslaps and serum alkaline phosphatase in patients with prostate cancer. British Journal of Urology 1997, 80, 452–455. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.E.; Purohit, O.P.; Black, C.; Vinholes, J.J.F.; Schlosser, K.; Huss, H.; Quinn, K.J.; Kanis, J. Double-blind, randomised, placebo-controlled, dose-finding study of oral ibandronate in patients with metastatic bone disease. Ann. Oncol. 1999, 10, 311–316. [Google Scholar] [CrossRef]
- Morcos, N.Y.S.; Zakhary, N.I.; Said, M.M.; Tadros, M.M.M. Postoperative simple biochemical markers for prediction of bone metastases in Egyptian breast cancer patients. Ecancermedicalscience 2013, 7, 305. [Google Scholar] [PubMed]
- Pectasides, D.; Farmakis, D.; Nikolaou, M.; Kanakis, I.; Kostopoulou, V.; Papaconstantinou, I.; Karamanos, N.K.; Economopoulos, T.; Raptis, S.A. Diagnostic value of bone remodeling markers in the diagnosis of bone metastases in patients with breast cancer. J. Pharm. Biomed. 2005, 37, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Seibel, M.J.; Koeller, M.; Van der Velden, B.; Diel, I. Markers of bone turnover do not predict bone metastases in breast cancer. Clin. Lab. 2002, 48, 583–588. [Google Scholar]
- Lipton, A.; Costa, L.; Ali, S.; Demers, L. Use of markers of bone turnover for monitoring bone metastases and the response to therapy. Semin. Oncol. 2001, 28, 54–59. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 20) | Breast Cancer (n = 50) | p | |
|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | ||
| Age (years) | 55.55 ± 5.85 | 57.74 ± 10.28 | 0.375 |
| CEA (ng/mL) | 1.61 ± 1.55 | 2.48 ± 2.68 | 0.179 |
| CA 125 (U/mL) | 16.96 ± 10.63 | 16.04 ± 8.63 | 0.711 |
| CA 15-3 (U/mL) | 13.06 ± 6.50 | 18.50 ± 16.24 | 0.160 |
| AST (U/L) | 18.53 ± 4.02 | 21.53 ± 8.38 | 0.143 |
| ALT (U/L) | 17.53 ± 7.62 | 21.67 ± 10.33 | 0.123 |
| GGT (U/L) | 23.75 ± 17.21 | 50.13 ± 104.29 | 0.420 |
| ALP (U/L) | 60.53 ± 20.08 | 183.97 ± 623.50 | 0.408 |
| PTH (pg/mL) | 57.80 ± 11.95 | 71.85 ± 19.18 | 0.001 |
| P (mg/dL) | 3.24 ± 0.47 | 3.46 ± 0.57 | 0.137 |
| Ca (mg/dL) | 10.07 ± 1.31 | 9.37 ± 0.33 | 0.001 |
| Creatinine (mg/dL) | 0.76 ± 0.10 | 0.86 ± 0.15 | 0.012 |
| Urea (mg/dL) | 0.76 ± 0.10 | 0.86 ± 0.15 | 0.012 |
| Uric acid (mg/dL) | 0.80 ± 0.00 | 0.90 ± 0.10 | 0.000 |
| Serum NTx (nMBCE/L) | 7.70 ± 2.02 | 13.31 ± 7.53 | 0.004 |
| Urine α-CTx (μg/mmol Cr) | 2.86 ± 1.67 | 6.12 ± 2.84 | 0.000 |
| Lumbar spine BMD (g/cm2) | 0.90 ± 0.10 | 0.80 ± 0.00 | 0.000 |
| Femoral neck BMD (g/cm2) | 0.73 ± 0.15 | 0.60 ± 0.00 | 0.001 |
| Breast Cancer without Metastasis n = 20 | Breast Cancer with Metastasis n = 30 | p | |
|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | ||
| Age (years) | 55.30 ± 11.55 | 59.56 ± 9.02 | 0.163 |
| CEA (ng/mL) | 2.89 ± 3.80 | 2.17 ± 1.38 | 0.367 |
| CA 125 (U/mL) | 15.70 ± 8.00 | 16.28 ± 9.20 | 0.824 |
| CA 15-3 (U/mL) | 19.23 ± 23.16 | 17.74 ± 8.04 | 0.757 |
| AST (U/L) | 23.33 ± 12.05 | 20.24 ± 4.00 | 0.307 |
| ALT (U/L) | 23.33 ± 12.78 | 20.42 ± 8.10 | 0.372 |
| GGT (U/L) | 75.63 ± 157.19 | 31.59 ± 25.63 | 0.284 |
| ALP (U/L) | 78.55 ± 34.66 | 230.41 ± 758.64 | 0.377 |
| PTH (pg/mL) | 69.40 ± 19.84 | 73.67 ± 18.85 | 0.457 |
| P (mg/dL) | 3.60 ± 0.50 | 3.35 ± 0.60 | 0.137 |
| Ca (mg/dL) | 9.45.13.60 | 10.63 ± 1.21 | 0.103 |
| Creatinine (mg/dL) | 0.84 ± 0.14 | 0.88 ± 0.16 | 0.421 |
| Urea (mg/dL) | 0.84 ± 0.14 | 0.88 ± 0.16 | 0.421 |
| Uric acid (mg/dL) | 0.80 ± 0.00 | 0.80 ± 0.00 | 1.000 |
| Serum NTx (nMBCE/L) | 13.36 ± 7.38 | 15.17 ± 11.32 | 0.536 |
| Urine α-CTx (mg/mL) | 2.13 ± 2.05 | 5.91 ± 4.61 | 0.001 |
| Urine α-CTx (μg/mmol Cr) | 3.96 ± 2.41 | 7.33 ± 2.34 | 0.001 |
| Lumbar spine BMD (g/cm2) | 0.80 ± 0.00 | 0.80 ± 0.00 | 1.000 |
| Femoral neck BMD (g/cm2) | 0.60 ± 0.00 | 0.60 ± 0.00 | 1.000 |
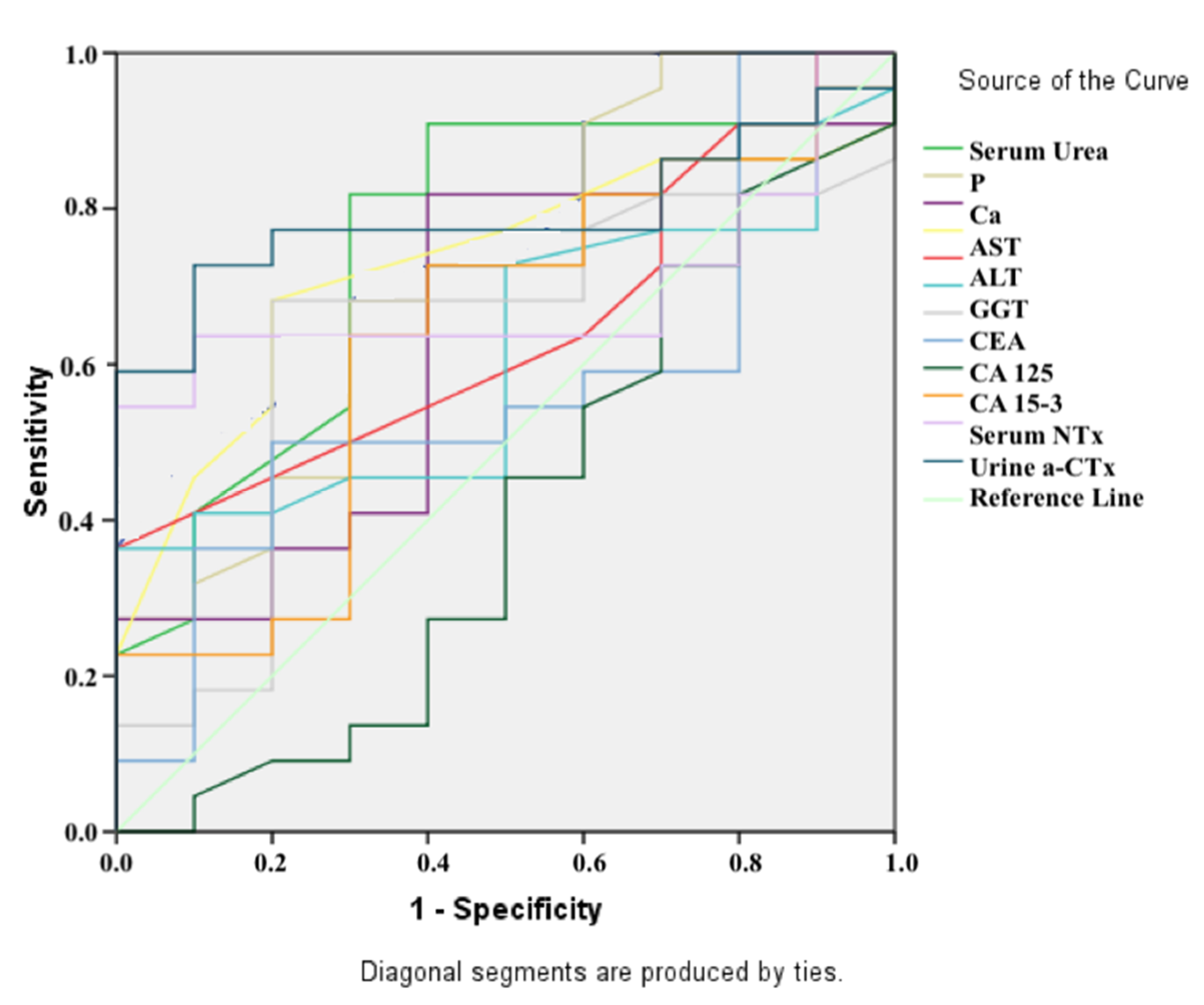
| Variables | AUC | p | Asymptotic 95% CI | Cut-Off Points | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Serum Urea (mg/dL) | 0.76 | 0.022 | 0.57 | 0.94 | 26.50 | 82% | 70% |
| ALP (U/L) | 0.71 | 0.056 | 0.52 | 0.91 | N.S. | N.S. | N.S. |
| P (mg/dL) | 0.64 | 0.208 | 0.43 | 0.85 | N.S. | N.S. | N.S. |
| Ca (mg/dL) | 0.73 | 0.042 | 0.55 | 0.90 | 9.55 | 68% | 80% |
| AST (U/L) | 0.65 | 0.193 | 0.45 | 0.84 | N.S. | N.S. | N.S. |
| ALT (U/L) | 0.61 | 0.329 | 0.41 | 0.81 | N.S. | N.S. | N.S. |
| GGT (U/L) | 0.63 | 0.238 | 0.42 | 0.84 | N.S. | N.S. | N.S. |
| CEA (ng/mL) | 0.57 | 0.542 | 0.35 | 0.78 | N.S. | N.S. | N.S. |
| CA 125 (U/mL) | 0.40 | 0.393 | 0.18 | 0.63 | N.S. | N.S. | N.S. |
| CA 15-3 (U/mL) | 0.63 | 0.238 | 0.42 | 0.84 | N.S. | N.S. | N.S. |
| Serum NTx (nMBCE/L) | 0.69 | 0.088 | 0.51 | 0.87 | N.S. | N.S. | N.S. |
| Urine α-CTx (μg/mmol Cr) | 0.79 | 0.009 | 0.63 | 0.95 | 4.30 | 73% | 90% |
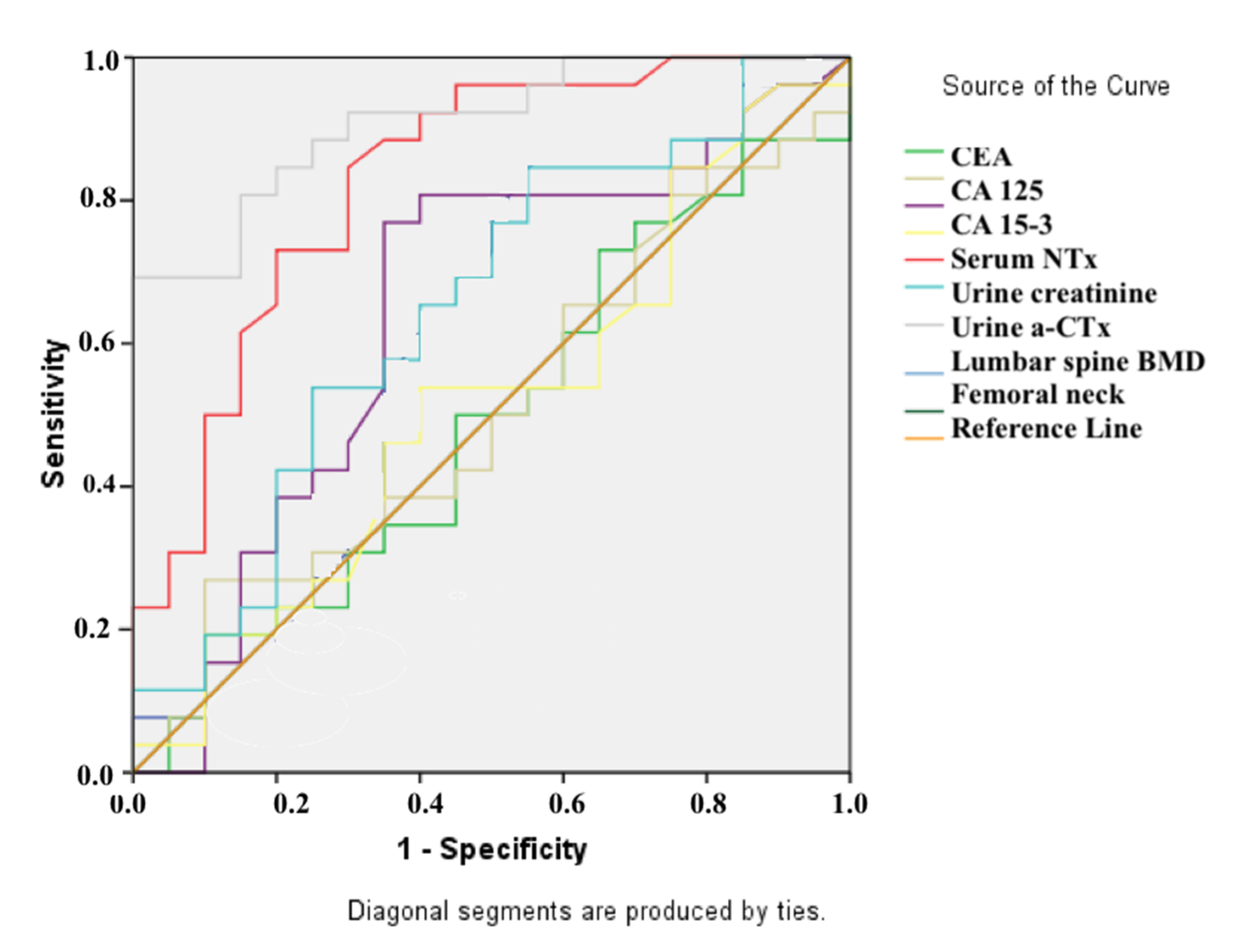
| Variables | AUC | p | Asymptotic 95% CI | Cut-Off Values | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| CEA (ng/mL) | 0.49 | 0.921 | 0.32 | 0.66 | N.S. | N.S. | N.S. |
| oCA 125 (U/mL) | 0.51 | 0.929 | 0.34 | 0.68 | N.S. | N.S. | N.S. |
| CA 15-3 (U/mL) | 0.64 | 0.106 | 0.47 | 0.81 | N.S. | N.S. | N.S. |
| Serum NTx (nMBCE/L) | 0.52 | 0.859 | 0.34 | 0.69 | N.S. | N.S. | N.S. |
| Urine α-CTx (mg/mL) | 0.83 | 0.000 | 0.71 | 0.95 | 2.48 | 85% | 70% |
| Urine Creatinine (µmol/L) | 0.65 | 0.084 | 0.49 | 0.81 | N.S. | N.S. | N.S. |
| Urine α-CTx (μg/mmol Cr) | 0.91 | 0.000 | 0.83 | 0.99 | 7.09 | 69% | 100% |
| Lumbar spine BMD (g/cm2) | 0.50 | 1.000 | 0.33 | 0.67 | N.S. | N.S. | N.S. |
| Femoral neck BMD (g/cm2) | 0.50 | 1.000 | 0.33 | 0.67 | N.S. | N.S. | N.S. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kundaktepe, B.P.; Sozer, V.; Kundaktepe, F.O.; Durmus, S.; Papila, C.; Uzun, H.; Simsek, G.; Gelisgen, R. Association between Bone Mineral Density and Bone Turnover Markers in Breast Cancer Patients and Bone-Only Metastasis. Medicina 2021, 57, 880. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090880
Kundaktepe BP, Sozer V, Kundaktepe FO, Durmus S, Papila C, Uzun H, Simsek G, Gelisgen R. Association between Bone Mineral Density and Bone Turnover Markers in Breast Cancer Patients and Bone-Only Metastasis. Medicina. 2021; 57(9):880. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090880
Chicago/Turabian StyleKundaktepe, Berrin Papila, Volkan Sozer, Fatih Orkun Kundaktepe, Sinem Durmus, Cigdem Papila, Hafize Uzun, Gonul Simsek, and Remise Gelisgen. 2021. "Association between Bone Mineral Density and Bone Turnover Markers in Breast Cancer Patients and Bone-Only Metastasis" Medicina 57, no. 9: 880. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090880