
Early and Late Outcomes after Arterial Switch Operation: A 40-Year Journey in a Single Low Case Volume Center

Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Operative Technique and Myocardial Protection
3. Results
3.1. Surgical Mortality
3.2. Early Morbidity
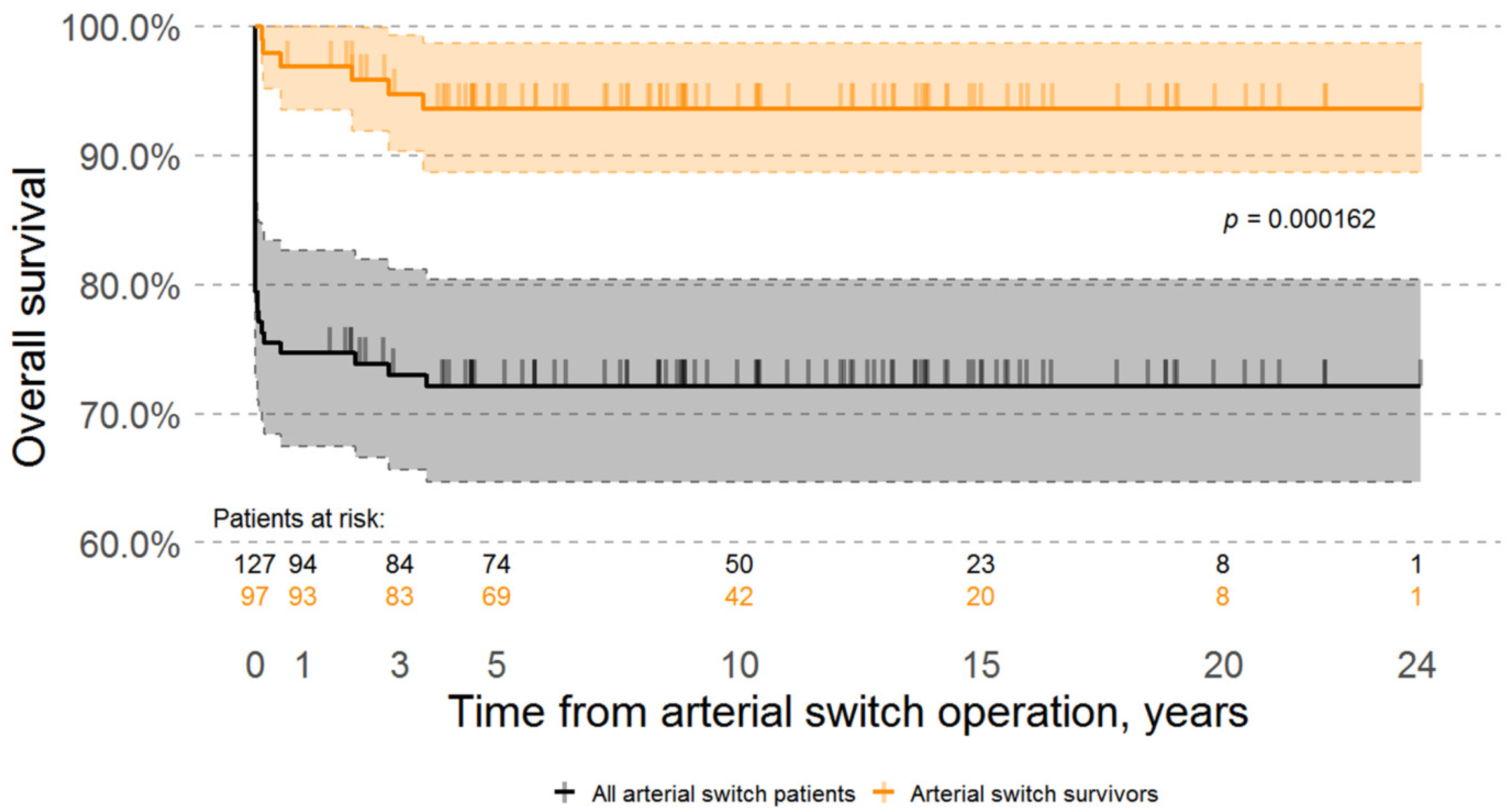
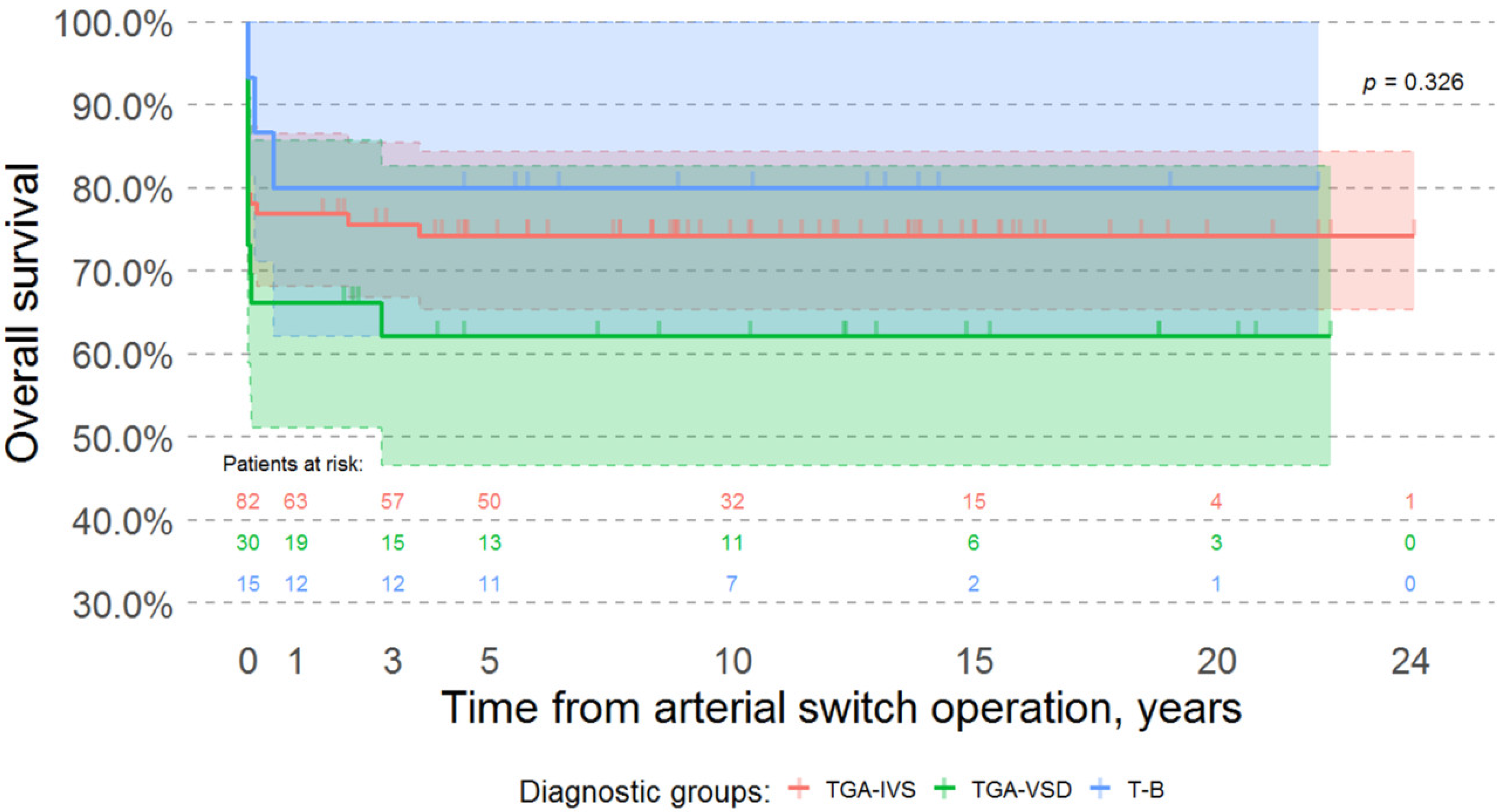
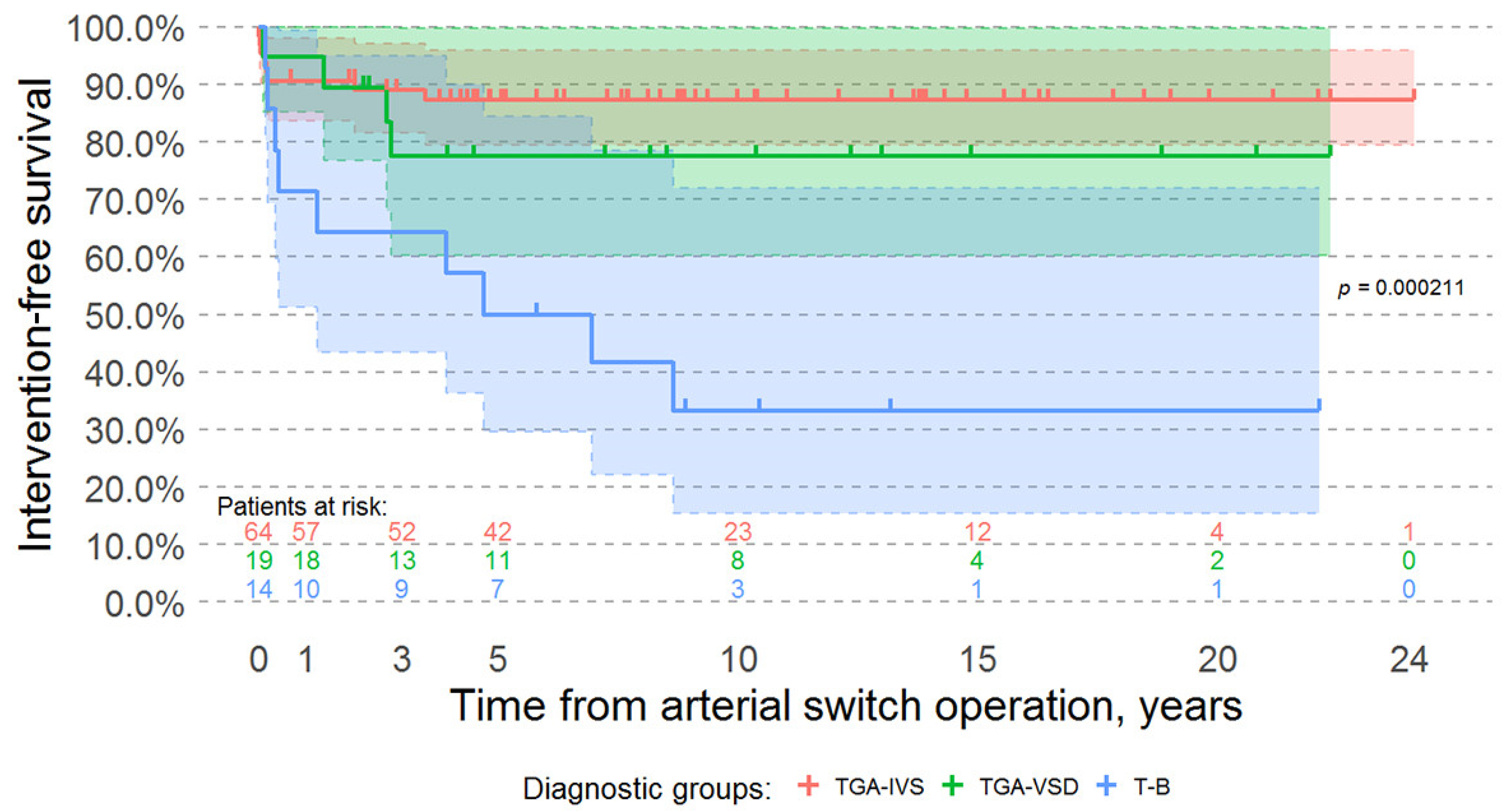
3.3. Survival Analysis, Late Mortality, and Morbidity
3.4. Late Neurological Outcomes
3.5. Late Cardiovascular Outcomes
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| IQR | interquartile range |
References
- Baillie, M. The Morbid Anatomy of Some of the Most Important Parts of the Human Body; Johnson and Nichol: London, UK, 1797. [Google Scholar]
- Farre, J.R. Pathalogical Researches. Essay 1: On Malformation of the Human Heart; Longman, Hurst, Rees, Orme, Brown: London, UK, 1814. [Google Scholar]
- Jatene, A.D.; Fontes, V.F.; Paulista, P.P.; de Souza, L.C.; Neger, F.; Galantier, M.; Souza, J.E. Successful Anatomic Correction of Transposition of the Great Vessels. A Preliminary Report. Arq. Bras. Cardiol. 1975, 28, 461–464. [Google Scholar]
- Lecompte, Y.; Zannini, L.; Hazan, E.; Jarreau, M.M.; Bex, J.P.; Tu, T.V.; Neveux, J.Y. Anatomic Correction of Transposition of the Great Arteries. J. Thorac. Cardiovasc. Surg. 1981, 82, 629–631. [Google Scholar] [CrossRef]
- Hörer, J.; Schreiber, C.; Cleuziou, J.; Vogt, M.; Prodan, Z.; Busch, R.; Holper, K.; Lange, R. Improvement in Long-Term Survival after Hospital Discharge but Not in Freedom from Reoperation after the Change from Atrial to Arterial Switch for Transposition of the Great Arteries. J. Thorac. Cardiovasc. Surg. 2009, 137, 347–354. [Google Scholar] [CrossRef] [Green Version]
- Prifti, E.; Crucean, A.; Bonacchi, M.; Bernabei, M.; Murzi, B.; Luisi, S.V.; Vanini, V. Early and Long Term Outcome of the Arterial Switch Operation for Transposition of the Great Arteries: Predictors and Functional Evaluation. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2002, 22, 864–873. [Google Scholar] [CrossRef]
- Michalak, K.W.; Moll, J.A.; Sobczak-Budlewska, K.; Moll, M.; Dryżek, P.; Moszura, T.; Szymczyk, K.; Moll, J.J. Reoperations and Catheter Interventions in Patients with Transposition of the Great Arteries after the Arterial Switch Operation. Eur. J. Cardiothorac. Surg. 2017, 51, 34–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moll, J.J.; Michalak, K.W.; Młudzik, K.; Moszura, T.; Kopala, M.; Moll, M.; Moll, J.A. Long-Term Outcome of Direct Neopulmonary Artery Reconstruction During the Arterial Switch Procedure. Ann. Thorac. Surg. 2012, 93, 177–184. [Google Scholar] [CrossRef]
- Fricke, T.A.; d’Udekem, Y.; Richardson, M.; Thuys, C.; Dronavalli, M.; Ramsay, J.M.; Wheaton, G.; Grigg, L.E.; Brizard, C.P.; Konstantinov, I.E. Outcomes of the Arterial Switch Operation for Transposition of the Great Arteries: 25 Years of Experience. Ann. Thorac. Surg. 2012, 94, 139–145. [Google Scholar] [CrossRef]
- Khairy, P.; Clair, M.; Fernandes, S.M.; Blume, E.D.; Powell, A.J.; Newburger, J.W.; Landzberg, M.J.; Mayer, J.E., Jr. Cardiovascular Outcomes after the Arterial Switch Operation for D-Transposition of the Great Arteries. Circulation 2013, 127, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, R.; Cleuziou, J.; Hörer, J.; Holper, K.; Vogt, M.; Tassani-Prell, P.; Schreiber, C. Risk Factors for Aortic Insufficiency and Aortic Valve Replacement after the Arterial Switch Operation. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2008, 34, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Hutter, P.A.; Kreb, D.L.; Mantel, S.F.; Hitchcock, J.F.; Meijboom, E.J.; Bennink, G.B.W.E. Twenty-Five Years’ Experience with the Arterial Switch Operation. J. Thorac. Cardiovasc. Surg. 2002, 124, 790–797. [Google Scholar] [CrossRef] [Green Version]
- Fraser, C.D. The Neonatal Arterial Switch Operation: Technical Pearls. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2017, 20, 38–42. [Google Scholar] [CrossRef]
- Manso, P.H.; Amaral, F.T.V.; Júnior, T.J.S.; Jurca, M.C.; Haddad, J.; Vicente, W.V.A.; Sgarbieri, R.N.; Carmona, F. Outcomes of Patients after Arterial Switch Operation: 18 Years of Experience in a Single Medium-Volume Center. Pediatr. Cardiol. 2015, 36, 1657–1661. [Google Scholar] [CrossRef]
- Shim, M.; Jun, T.-G.; Yang, J.-H.; Park, P.W.; Kang, I.S.; Huh, J.; Song, J.Y. Current Expectations of the Arterial Switch Operation in a Small Volume Center: A 20-Year, Single-Center Experience. J. Cardiothorac. Surg. 2016, 11, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettersen, M.D.; Du, W.; Skeens, M.E.; Humes, R.A. Regression Equations for Calculation of z Scores of Cardiac Structures in a Large Cohort of Healthy Infants, Children, and Adolescents: An Echocardiographic Study. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2008, 21, 922–934. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Gittenberger-de Groot, A.C.; Koenraadt, W.M.C.; Bartelings, M.M.; Bökenkamp, R.; DeRuiter, M.C.; Hazekamp, M.G.; Bogers, A.J.J.C.; Quaegebeur, J.M.; Schalij, M.J.; Vliegen, H.W.; et al. Coding of Coronary Arterial Origin and Branching in Congenital Heart Disease: The Modified Leiden Convention. J. Thorac. Cardiovasc. Surg. 2018, 156, 2260–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebetkevicius, V.; Tarutis, V.; Zilinskas, V.; Lankutis, K.; Nogiene, G.; Liekiene, D.; Sudikiene, R.; Sirvydis, V. Congenital heart surgery in neonates. Med. Kaunas Lith. 2002, 38 (Suppl. 2), 188–190. [Google Scholar]
- Parezanović, V.; Mrđen, M.; Ilić, S.; Vulićević, I.; Đukić, M.; Jovanović, I.; Stefanović, I.; Ilisić, T.; Kalanj, J.; Mimić, B.; et al. Midterm Results after Complete Surgical Correction of Transposition of the Great Arteries. Srp. Arh. Celok. Lek. 2014, 142, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Puras, M.J.; Cabeza-Letrán, L.; Romero-Vazquianez, M.; Santos de Soto, J.; Hosseinpour, R.; Gil Fournier, M.; Alvarez Madrid, A.; González, A.; Pérez, P.; Gallego, P. Mid-Term Morbidity and Mortality of Patients after Arterial Switch Operation in Infancy for Transposition of the Great Arteries. Rev. Esp. Cardiol. Engl. Ed. 2014, 67, 181–188. [Google Scholar] [CrossRef]
- Jung, J.C.; Kwak, J.G.; Kim, E.R.; Bang, J.H.; Min, J.; Lim, J.H.; Kim, W.-H. Reoperation for Coronary Artery Stenosis after Arterial Switch Operation. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 169–176. [Google Scholar] [CrossRef]
- Blume, E.D.; Altmann, K.; Mayer, J.E.; Colan, S.D.; Gauvreau, K.; Geva, T. Evolution of Risk Factors Influencing Early Mortality of the Arterial Switch Operation. J. Am. Coll. Cardiol. 1999, 33, 1702–1709. [Google Scholar] [CrossRef] [Green Version]
- Kempny, A.; Wustmann, K.; Borgia, F.; Dimopoulos, K.; Uebing, A.; Li, W.; Chen, S.S.; Piorkowski, A.; Radley-Smith, R.; Yacoub, M.H.; et al. Outcome in Adult Patients after Arterial Switch Operation for Transposition of the Great Arteries. Int. J. Cardiol. 2013, 167, 2588–2593. [Google Scholar] [CrossRef]
- Lalezari, S.; Bruggemans, E.F.; Blom, N.A.; Hazekamp, M.G. Thirty-Year Experience with the Arterial Switch Operation. Ann. Thorac. Surg. 2011, 92, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-G.; Kim, W.-H.; Lee, J.R.; Kim, Y.J. Long-Term Results of the Arterial Switch Operation for Ventriculo-Arterial Discordance. Eur. J. Cardiothorac. Surg. 2013, 43, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Martins, P.; Castela, E. Transposition of the Great Arteries. Orphanet J. Rare Dis. 2008, 3, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruys, T.P.E.; van der Bosch, A.E.; Cuypers, J.A.A.E.; Witsenburg, M.; Helbing, W.A.; Bogers, A.J.J.C.; van Domburg, R.; McGhie, J.S.; Geleijnse, M.L.; Henrichs, J.; et al. Long-Term Outcome and Quality of Life after Arterial Switch Operation: A Prospective Study with a Historical Comparison. Congenit. Heart Dis. 2013, 8, 203–210. [Google Scholar] [CrossRef]
- Vergnat, M.; Baruteau, A.-E.; Houyel, L.; Ly, M.; Roussin, R.; Capderou, A.; Lambert, V.; Belli, E. Late Outcomes after Arterial Switch Operation for Taussig-Bing Anomaly. J. Thorac. Cardiovasc. Surg. 2015, 149, 1124–1132. [Google Scholar] [CrossRef] [Green Version]
- Kirzner, J.; Pirmohamed, A.; Ginns, J.; Singh, H.S. Long-Term Management of the Arterial Switch Patient. Curr. Cardiol. Rep. 2018, 20, 68. [Google Scholar] [CrossRef] [PubMed]
- Jonas, K.; Jakutis, V.; Sudikienė, R.; Lebetkevičius, V.; Tarutis, V. Interventions after Arterial Switch: A Single Low Case-Volume Center Experience. Medicina (Mex.) 2021, 57, 401. [Google Scholar] [CrossRef]
- van der Palen, R.L.F.; van der Bom, T.; Dekker, A.; Tsonaka, R.; van Geloven, N.; Kuipers, I.M.; Konings, T.C.; Rammeloo, L.A.J.; Harkel, A.D.J.T.; Jongbloed, M.R.M.; et al. Progression of Aortic Root Dilatation and Aortic Valve Regurgitation after the Arterial Switch Operation. Heart 2019, 105, 1732–1740. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Shahbah, D.A.; El-Said, H.; Rios, R.; Ratnayaka, K.; Moore, J. Pulmonary Artery Interventions after the Arterial Switch Operation: Unique and Significant Risks. Congenit. Heart Dis. 2019, 14, 288–296. [Google Scholar] [CrossRef]
- Angeli, E.; Raisky, O.; Bonnet, D.; Sidi, D.; Vouhé, P.R. Late Reoperations after Neonatal Arterial Switch Operation for Transposition of the Great Arteries. Eur. J. Cardiothorac. Surg. 2008, 34, 32–36. [Google Scholar] [CrossRef] [Green Version]
- Andropoulos, D.B.; Easley, R.B.; Brady, K.; McKenzie, E.D.; Heinle, J.S.; Dickerson, H.A.; Shekerdemian, L.; Meador, M.; Eisenman, C.; Hunter, J.V.; et al. Changing Expectations for Neurological Outcomes After the Neonatal Arterial Switch Operation. Ann. Thorac. Surg. 2012, 94, 1250–1256. [Google Scholar] [CrossRef] [Green Version]
- Kasmi, L.; Calderon, J.; Montreuil, M.; Geronikola, N.; Lambert, V.; Belli, E.; Bonnet, D.; Kalfa, D. Neurocognitive and Psychological Outcomes in Adults with Dextro-Transposition of the Great Arteries Corrected by the Arterial Switch Operation. Ann. Thorac. Surg. 2018, 105, 830–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMaso, D.R.; Labella, M.; Taylor, G.A.; Forbes, P.W.; Stopp, C.; Bellinger, D.C.; Rivkin, M.J.; Wypij, D.; Newburger, J.W. Psychiatric Disorders and Function in Adolescents with D-Transposition of the Great Arteries. J. Pediatr. 2014, 165, 760–766. [Google Scholar] [CrossRef] [Green Version]
- de Leval, M.R.; François, K.; Bull, C.; Brawn, W.; Spiegelhalter, D. Analysis of a Cluster of Surgical Failures: Application to a Series of Neonatal Arterial Switch Operations. J. Thorac. Cardiovasc. Surg. 1994, 107, 914–924. [Google Scholar] [CrossRef] [Green Version]
- Karamlou, T.; Jacobs, M.L.; Pasquali, S.; He, X.; Hill, K.; O’Brien, S.; McMullan, D.M.; Jacobs, J.P. Surgeon and Center Volume Influence on Outcomes after Arterial Switch Operation: Analysis of the STS Congenital Heart Surgery Database. Ann. Thorac. Surg. 2014, 98, 904–911. [Google Scholar] [CrossRef]
- Vouhé, P.R. Editorial Comment: Arterial Switch Operation: Is the Glass Half Full or Half Empty? Eur. J. Cardiothorac. Surg. 2013, 43, 334–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yacoub, M.; Hosny, H.; Afifi, A. Surgery for TGA in Developing Countries: The End of the Beginning. J. Am. Coll. Cardiol. 2017, 69, 52–55. [Google Scholar] [CrossRef]
- Baliulis, G.; Lipnevičius, A.; Sudikiene, R.; Lebetkevičius, V.; Versockas, K.; Lankutis, K.; Nogienė, G.; Žilinskas, V.; Sirvydis, V.; Haw, M.P.; et al. Sustainable Knowledge Transfer in Pediatric Cardiac Surgery: A Team Approach to Shared Learning. World J. Pediatr. Congenit. Heart Surg. 2011, 2, 225–230. [Google Scholar] [CrossRef]
- Jonas, R.A. Congenital Heart Surgery in Developing Countries. Semin. Thorac. Cardiovasc. Surg. Pediatr. Card. Surg. Annu. 2008, 11, 3–6. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | TGA-IVS | TGA-VSD | T-B | Total |
|---|---|---|---|---|
| n (%) | 82 (64.6) | 30 (23.6) | 15 (11.8) | 127 (100) |
| Female, n (%): Male, n (%) | 37 (45.1): 45 (54.9) | 14 (46.7): 16 (53.3) | 8 (53.3): 7 (46.7) | 59 (46.5): 68 (53.5) |
| Median age, days (IQR) | 11 (8–15) | 26 (12–75) | 21 (10–61) | 13 (9–22) |
| Age ≤ 28 days, n (%) | 77 (93.9) | 16 (53.3) | 8 (53.3) | 101 (79.5) |
| Median weight, kg (IQR) | 3.4 (3.1–3.8) | 3.8 (3.3–4.4) | 3.7 (3.5–4.2) | 3.5 (3.2–3.9) |
| Coronary pattern * | ||||
| Normal, n (%) | 66 (80.5) | 24 (80.0) | 2 (13.3) | 93 (73.2) |
| Anomalous, n (%) | 16 (19.5) | 6 (20.0) | 13 (86.7) | 35 (27.6) |
| Intramural course #, n (%) | 3 (18.8) | 1 (16.7) | 0 (0.0) | 4 (11.4) |
| Concomitant cardiovascular malformations | ||||
| AoCo, n (%) | 2 (2.4) | 0 (0.0) | 8 (53.3) | 10 (7.9) |
| HAA, n (%) | 1 (1.2) | 0 (0.0) | 6 (40) | 7 (5.5) |
| IAA, n (%) | 0 (0.0) | 0 (0.0) | 1 (6.7) | 1 (0.8) |
| Prior procedures | ||||
| BAS, n (%) | 48 (58.5) | 14 (46.6) | 0 (0.0) | 62 (48.8) |
| PAB, n (%) | 0 (0.0) | 1 (3.33) | 2 (13.3) | 3 (2.4) |
| Senning repair, n (%) | 1 (1.22) | 0 (0.0) | 0 (0.0) | 1 (0.8) |
| Surgical data | ||||
| Median CPB, min (IQR) | 198 (174–227) | 234 (213–262) | 302 (260–354) | 220 (181–245) |
| Median AoX, min (IQR) | 125 (112–140) | 133 (124–151) | 174 (150–245) | 130 (118–150) |
| Surgical mortality, % | 22 | 36.7 | 6.7 | 23.6 |
| Coronary Pattern # | TGA-IVS (n = 82) n (%) | TGA-VSD (n = 30) n (%) | T-B (n = 15) n (%) | Total (n = 127) n (%) |
|---|---|---|---|---|
| 1LCx *–2R | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 1IB–2LCx, R | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 1L–2RCx | 7 (43.75%) | 2 (33.32%) | 3 (23.1%) | 12 (34.29%) |
| 2R, LCx * | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 1LR–2Cx | 1 (6.25%) | 0 (0.0%) | 1 (7.7%) | 2 (5.71%) |
| 1LCX, IB–2R | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 2LCx *, R | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 2L, RCx | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 1LCxR | 1 (6.25%) | 1 (16.67%) | 1 (7.7%) | 3 (8.57%) |
| 1L, R–2Cx | 1 (6.25%) | 0 (0.0%) | 0 (0.0%) | 1 (2.86%) |
| 2LCxR | 0 (0.0%) | 1 (16.67%) | 0 (0.0%) | 1 (2.86%) |
| 1LCx–2R, R | 0 (0.0%) | 1 (16.67%) | 0 (0.0%) | 1 (2.86%) |
| 1LCx *, R | 0 (0.0%) | 1 (16.67%) | 0 (0.0%) | 1 (2.86%) |
| 1R–2LCx | 0 (0.0%) | 0 (0.0%) | 5 (38.4%) | 5 (14.29%) |
| 1RCx, IB–2L | 0 (0.0%) | 0 (0.0%) | 1 (7.7%) | 1 (2.86%) |
| 1IB–2LCxR | 0 (0.0%) | 0 (0.0%) | 2 (15.4%) | 2 (5.71%) |
| Surgical Mortality (%) | Fisher Exact p-Value against First Period | |
|---|---|---|
| First period (1977–1998) (n = 17) | 88.24 | - |
| Second period (1999–2002) (n = 24) | 41.7 | 0.0035 |
| Third period (2003–2019) (n = 86) | 5.81 | <0.001 |
| TGA-IVS (n = 64) | TGA-VSD (n = 30) | T-B (n = 14) | Total (n = 97) | |
|---|---|---|---|---|
| Late mortality (%) | 4.7 | 5.3 | 14.3 | 6 (6.2) |
| FU visit > 2 years ago, n (%) | 11 (17.2) | 2 (10.5) | 0 (0.0) | 13 (13.4) |
| FU time, years (IQR) | 9.13 (5.79–14.53) | 11.24 (4.24–15.73) | 11.5 (6.16–13.85) | 10.1 (5.69–14.53) |
| Height, cm (IQR) | 135 (106–160) | 129 (105–161) | 146 (116–158) | 135 (106–160) |
| Weight, kg (IQR) | 29 (17–50) | 27.5 (16.8–55.3) | 36.5 (18.4–51.5) | 29 (16.8–50) |
| Cardiac function | ||||
| LV EF, % (IQR) | 64 (62–66) | 65 (62–70) | 63 (61–66) | 64 (62–68) |
| LV EF ≥ 55%, n (%) | 49 (98.0) | 15 (93.75) | 12 (100) | 76 (97.4) |
| LV EF 45–54%, n (%) | 1 (2.0) | 1 (6.25) | 0 (0.0) | 2 (2.6) |
| LVEDD, cm (IQR) | 3.9 (3.4–4.6) | 4.2 (3.2–4.6) | 4.5 (3.8–4.8) | 4 (3.4–4.6) |
| iLVEDD, cm/m2 (IQR) | 3.8 (3.1–5.1) | 3.8 (3.1–4.9) | 3.8 (3.5–4.4) | 3.8 (3.1–5.0) |
| Residual VSD, n (%) | - | 3 (15.79) | 3 (21.4) | 6 (7.7) |
| NAA, cm (IQR) | 1.9 (1.6–2.2) | 1.83 (1.45–2.15) | 2.1 (1.8–2.43) | 1.9 (1.5–2.2) |
| NAA Z-score (IQR) | 1.7 (0.9–3.1) | 1.8 (1.42–2.3) | 2.3 (1.3–4.1) | 1.8 (1.1–3.1) |
| NAA Z-score ≥ 2, n (%) | 23 (46) | 6 (37.5) | 7 (50) | 36 (46.2) |
| NAS, cm (IQR) | 2.6 (2.2–2.9) | 2.6 (2.3–3.1) | 3 (2.6–3.2) | 2.6 (2.3–3.1) |
| NAS Z-score (IQR) | 2 (1.1–2.8) | 2.2 (1.7–2.7) | 3.1 (2.2–3.4) | 2.2 (1.3–2.9) |
| NAS Z-score ≥ 2, n (%) | 26 (52) | 9 (56.3) | 10 (71.4) | 45 (57.7) |
| NASTJ, cm (IQR) | 2 (1.7–2.3) | 1.8 (1.5–2.6) | 2.1 (1.7–2.5) | 2 (1.7–2.3) |
| NASTJ Z-score (IQR) | 1.2 (0.5–1.7) | 1.1 (0.2–2.1) | 1.1 (0.8–1.9) | 1.2 (0.4–1.9) |
| NASTJ Z-score ≥ 2, n (%) | 6 (12) | 4 (25) | 2 (14.3) | 12 (15.4) |
| NAVR on discharge, n (%) | 2 (3.1) | 4 (21.1) | 3 (21.4) | 9 (9.3) |
| NAVR during follow–up | ||||
| Trivial, n (%) | 20 (40) | 7 (43.75) | 2 (14.3) | 29 (37.2) |
| Mild, n (%) | 10 (20) | 5 (31.25) | 3 (21.4) | 18 (23.1) |
| Moderate, n (%) | 5 (10) | 0 (0.0) | 2 (14.3) | 7 (9) |
| Severe, n (%) | 1 (2) | 0 (0.0) | 0 (0.0) | 1 (1.3) |
| NPAPDG, mmHg (IQR) | 12.1 (7.8–19.3) | 12.3 (9.9–23) | 15.2 (13–44.6) | 13 (8.3–23) |
| NPAMDG, mmHg (IQR) | 6 (4.9–11.7) | 6.8 (5.1–11.2) | 7.7 (6.7–31.6) | 6.6 (5.1–11.8) |
| NPAPDV, m/s (IQR) | 1.7 (1.4–2.2) | 1.8 (1.6–2.4) | 1.9 (1.7–2.6) | 1.8 (1.4–2.4) |
| NPAPDG < 36, n (%) | 45 (90) | 14 (87.5) | 9 (64.3) | 68 (87.2) |
| NPAPDG > 64, n (%) | 1 (2) | 1 (6.3) | 3 (21.4) | 5 (6.4) |
| NPAPDV > 3, n (%) | 4 (8) | 2 (12.5) | 3 (21.4) | 9 (11.5) |
| Additional treatment due to | ||||
| NAAO, n (%) | 1 (1.6) | 1 (5.3) | 0 (0.0) | 2 (2.1) |
| RAAO, n (%) | 0 (0.0) | 0 (0.0) | 5 (35.7) | 5 (5.2) |
| RVOTO, n (%) | 3 (4.7) | 3 (15.8) | 5 (35.7) | 11 (11.3) |
| Variables | Data | Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| Event = 0 * (n = 97) | Event = 1 # (n = 30) | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Female, n (%) | 47(48.5) | 12 (40) | 1.06 | 0.44–2.6 | 0.892 | |||
| Age, days; M (IQR) | 11 (8–19) | 15 (11.3–38.8) | 0.999 | 0.995–1.004 | 0.76 | |||
| Weight, kg; M (IQR) | 3.5 (3.2–3.9) | 3.45(3.3–3.9) | 0.86 | 0.55–1.34 | 0.509 | |||
| Complex TGA, n (%) | 33 (34) | 12 (40) | 1.39 | 0.56–3.45 | 0.485 | |||
| AAO, n (%) | 15 (15.5) | 2 (6.7) | 0.5 | 0.11–2.34 | 0.376 | |||
| Coronary pattern other than 1LCx-2R, n (%) | 30 (30.9) | 5 (16.7) | 0.59 | 0.2–1.72 | 0.333 | |||
| AoX, min; M (IQR) | 126 (117–149) | 139 (130–151) | 1.0076 | 0.998–1.02 | 0.119 | 1.02 | 1–1.05 | 0.026 |
| Surgery before the international knowledge transfer program, n (%) | 2 (2.1) | 15 (50) | 28.5 | 5.61–144.89 | <0.001 | 41.06 | 5.98–282.11 | <0.001 |
| Variables | Data | Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| Event = 0 * (n = 76) | Event = 1 # (n = 21) | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Female, n (%) | 39 (51.3) | 8 (38.1) | 0.63 | 0.23–1.7 | 0.37 | |||
| Age, days; M (IQR) | 11 (8–17.25) | 13 (9–28) | 0.999 | 0.994–1 | 0.76 | |||
| Weight, kg; M (IQR) | 3.5 (3.2–3.9) | 3.6 (3.3–4.0) | 1.01 | 0.72–1.4 | 0.97 | |||
| Complex TGA, n (%) | 20 (26.3) | 13 (61.9) | 5.38 | 1.87–15.5 | 0.002 | 3.05 | 0.71–13.16 | 0.135 |
| AAO, n (%) | 5 (6.6) | 10 (47.6) | 13.8 | 3.9–48.7 | <0.001 | 10.64 | 1.23–99.19 | 0.032 |
| Coronary pattern other than 1LCx-2R, n (%) | 21 (27.6) | 9 (42.9) | 2.06 | 0.75–5.7 | 0.162 | 0.43 | 0.08–2.31 | 0.324 |
| AoX, min; M (IQR) | 125 (90–141) | 140 (110–203) | 1.02 | 1.01–1.04 | 0.002 | 1.003 | 0.98–1.03 | 0.785 |
| Length of stay, days; M (IQR) | 25 (20–31) | 30 (22.75–39) | 1.06 | 1.01–1.12 | 0.03 | 1.03 | 0.97–1.1 | 0.36 |
| Procedure | Number (%) | |
|---|---|---|
| Diaphragm plication | 2 | (5) |
| Right ventricle outflow tract obstruction repair | 2 | (5) |
| Bi-directional Glenn shunt | 2 | (5) |
| Neo-pulmonary artery balloon dilation | 11 | (27) |
| Neo-pulmonary artery stenting | 1 | (2) |
| Neo-pulmonary artery surgical repair | 6 | (15) |
| New aortic coarctation surgical repair | 1 | (2) |
| New aortic coarctation balloon dilation | 1 | (2) |
| Aortic re-coarctation balloon dilation | 13 | (32) |
| Aortic re-coarctation stenting | 2 | (5) |
| Total | 41 in 16 patients | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jonas, K.; Jakutis, V.; Sudikienė, R.; Lebetkevičius, V.; Baliulis, G.; Tarutis, V. Early and Late Outcomes after Arterial Switch Operation: A 40-Year Journey in a Single Low Case Volume Center. Medicina 2021, 57, 906. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090906
Jonas K, Jakutis V, Sudikienė R, Lebetkevičius V, Baliulis G, Tarutis V. Early and Late Outcomes after Arterial Switch Operation: A 40-Year Journey in a Single Low Case Volume Center. Medicina. 2021; 57(9):906. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090906
Chicago/Turabian StyleJonas, Karolis, Virginijus Jakutis, Rita Sudikienė, Virgilijus Lebetkevičius, Giedrius Baliulis, and Virgilijus Tarutis. 2021. "Early and Late Outcomes after Arterial Switch Operation: A 40-Year Journey in a Single Low Case Volume Center" Medicina 57, no. 9: 906. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090906