
A Thoracic Outlet Syndrome That Concealed a Glioblastoma. Findings from a Case Report

 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
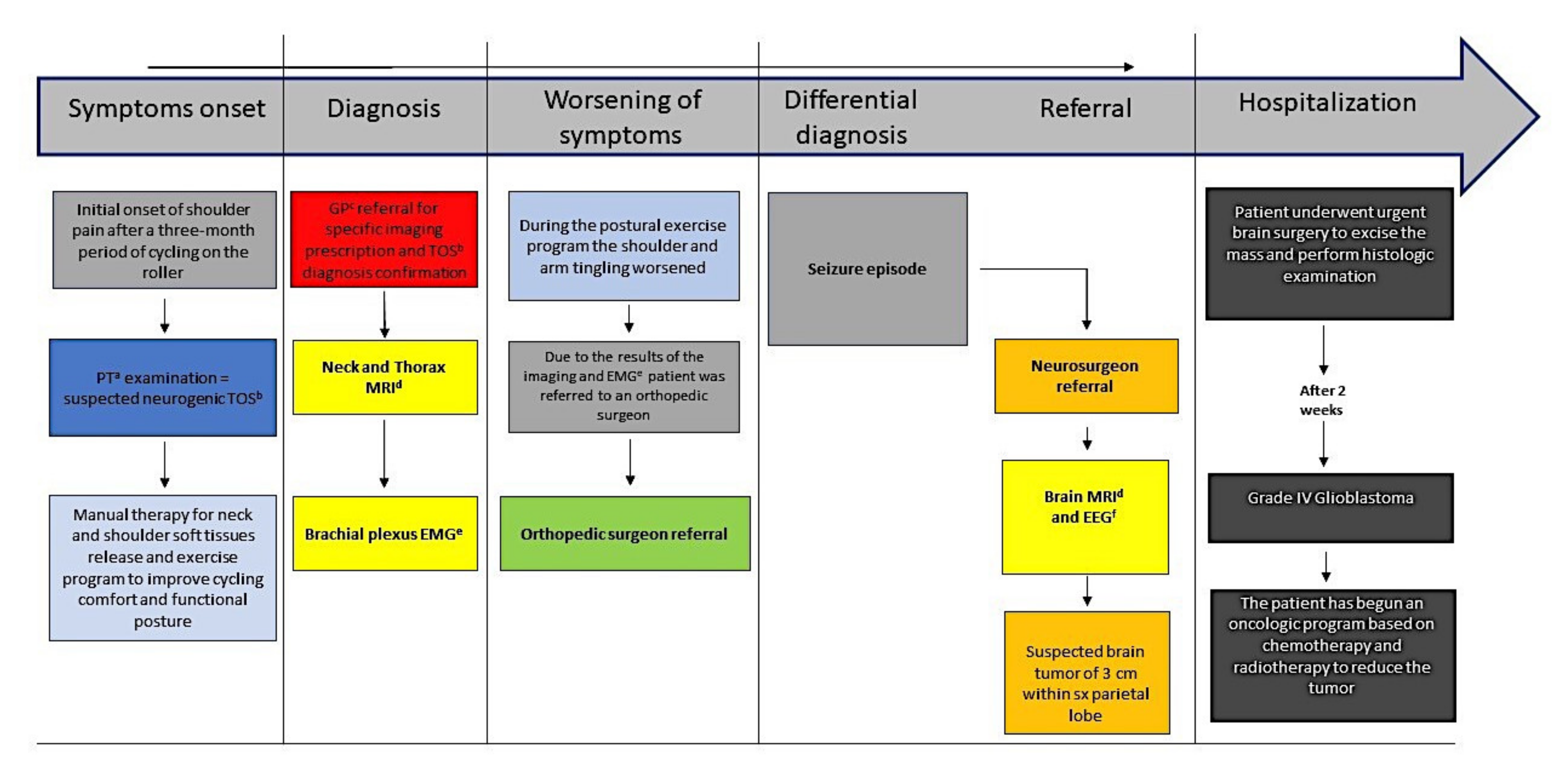
2. Case Presentation
Investigations
3. Results
3.1. Differential Diagnosis
3.2. Treatment
3.3. Outcome and Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malavolta, E.A.; Gracitelli, M.E.C.; Assunção, J.H.; Pinto, G.d.M.R.; da Silveira, A.Z.F.; Neto, A.A.F. Shoulder disorders in an outpatient clinic: An epidemiological study. Acta. Ortop. Bras. 2017, 25, 78–80. [Google Scholar] [CrossRef] [Green Version]
- Greving, K.; Dorrestijn, O.; Winters, J.C.; Groenhof, F.; Van Der Meer, K.; Stevens, M.; Diercks, R. Incidence, prevalence, and consultation rates of shoulder complaints in general practice. Scand. J. Rheumatol. 2011, 41, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Hegedus, E.J.; Goode, A.; Campbell, S.; Morin, A.; Tamaddoni, M.; Moorman, C.T.; Cook, C. Physical examination tests of the shoulder: A systematic review with meta-analysis of individual tests. Br. J. Sports Med. 2008, 42, 80–92. [Google Scholar] [CrossRef] [Green Version]
- Ristori, D.; Miele, S.; Rossettini, G.; Monaldi, E.; Arceri, D.; Testa, M. Towards an integrated clinical framework for patient with shoulder pain. Arch. Physiother. 2018, 8, 7. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Adebajo, A.; Hay, E.; Carr, A. Shoulder pain: Diagnosis and management in primary care. BMJ 2005, 331, 1124–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storari, L.; Barbari, V.; Brindisino, F.; Testa, M.; Filippo, M. An unusual presentation of acute myocardial infarction in physiotherapy direct access: Findings from a case report. Arch. Physiother. 2021, 11, 5. [Google Scholar] [CrossRef]
- Nichols, A.W. Diagnosis and Management of Thoracic Outlet Syndrome. Curr. Sports Med. Rep. 2009, 8, 240–249. [Google Scholar] [CrossRef]
- Illig, K.A.; Donahue, D.; Duncan, A.; Freischlag, J.; Gelabert, H.; Johansen, K.; Jordan, S.; Sanders, R.; Thompson, R. Reporting standards of the Society for Vascular Surgery for thoracic outlet syndrome. J. Vasc. Surg. 2016, 64, e23–e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illig, K.A.; Rodriguez-Zoppi, E.; Bland, T.; Muftah, M.; Jospitre, E. The Incidence of Thoracic Outlet Syndrome. Ann. Vasc. Surg. 2021, 70, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 1. Overview of the thoracic outlet syndromes and review of true neurogenic thoracic outlet syndrome. Muscle Nerve 2017, 55, 782–793. [Google Scholar] [CrossRef]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 2. The arterial, venous, neurovascular, and disputed tho-racic outlet syndromes. Muscle Nerve 2017, 56, 663–673. [Google Scholar] [CrossRef]
- Watson, L.; Pizzari, T.; Balster, S. Thoracic outlet syndrome part 1: Clinical manifestations, differentiation and treatment pathways. Man. Ther. 2009, 14, 586–595. [Google Scholar] [CrossRef] [PubMed]
- McNeill, K.A. Epidemiology of Brain Tumors. Neurol. Clin. 2016, 34, 981–998. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. CBTRUS statis-tical report: Primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. J. Neuro-Oncol. 2014, 16, iv1–iv63. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; Snyder, A.R.; Leggin, B.G. Responsiveness of the Numeric Pain Rating Scale in Patients With Shoulder Pain and the Effect of Surgical Status. J. Sport Rehabil. 2011, 20, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Gismervik, S.; Drogset, J.O.; Granviken, F.; Rø, M.; Leivseth, G. Physical examination tests of the shoulder: A systematic review and meta-analysis of diagnostic test performance. BMC Musculoskelet. Disord. 2017, 18, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, K.C.; Lee, H.S.; Lee, J.H. Cervical Radiculopathy Focus on Characteristics and Differential Diagnosis. Asian Spine J. 2020, 14, 921–930. [Google Scholar] [CrossRef]
- Jones, M.R.; Prabhakar, A.; Viswanath, O.; Urits, I.; Green, J.B.; Kendrick, J.B.; Brunk, A.J.; Eng, M.R.; Orhurhu, V.; Cornett, E.M.; et al. Thoracic Outlet Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Pain Ther. 2019, 8, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Povlsen, B.; Hansson, T.; Povlsen, S.D. Treatment for thoracic outlet syndrome. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Povlsen, B.; Belzberg, A.; Hansson, T.; Dorsi, M. Treatment for thoracic outlet syndrome. Cochrane Database Syst Rev. 2010, CD007218. [Google Scholar] [CrossRef]
- Mintken, P.E.; Glynn, P.; Cleland, J.A. Psychometric properties of the shortened disabilities of the Arm, Shoulder, and Hand Questionnaire (QuickDASH) and Numeric Pain Rating Scale in patients with shoulder pain. J. Should. Elb. Surg. 2009, 18, 920–926. [Google Scholar] [CrossRef]
- Jordan, S.E.; Ahn, S.S.; Gelabert, H.A. Differentiation of thoracic outlet syndrome from treatment-resistant cervical brachial pain syndromes: Development and utilization of a questionnaire, clinical examination and ultrasound evaluation. Pain Physician 2007, 10, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Hixson, K.M.; Horris, H.B.; McLeod, T.C.V.; Bacon, C.E.W. The Diagnostic Accuracy of Clinical Diagnostic Tests for Thoracic Outlet Syndrome. J. Sport Rehabil. 2017, 26, 459–465. [Google Scholar] [CrossRef]
- Vanti, C.; Natalini, L.; Romeo, A.; Tosarelli, D.; Pillastrini, P. Conservative treatment of thoracic outlet syndrome. A review of the literature. Eur. Med. 2006, 43, 55–70. [Google Scholar]
- Costello, M.; Puentedura, E.J.; Cleland, J.; Ciccone, C.D. The immediate effects of soft tissue mobilization versus therapeutic ultrasound for patients with neck and arm pain with evidence of neural mechanosensitivity: A randomized clinical trial. J. Man. Manip. Ther. 2016, 24, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, N.A.; Rigby, B.R. Thoracic Outlet Syndrome: Biomechanical and Exercise Considerations. Healthcare 2018, 6, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Serratus anterior or pectoralis minor: Which muscle has the upper hand during protraction exercises? Man. Ther. 2016, 22, 158–164. [Google Scholar] [CrossRef]
- George, S.Z.; Beneciuk, J.M.; Lentz, T.; Wu, S.S. The Optimal Screening for Prediction of Referral and Outcome (OSPRO) in patients with musculoskeletal pain conditions: A longitudinal validation cohort from the USA. BMJ Open 2017, 7, e015188. [Google Scholar] [CrossRef] [Green Version]
- George, S.; Beneciuk, J.M.; Bialosky, J.E.; Lentz, T.A.; Zeppieri, G.; Pei, Q.; Wu, S.S.; Zeppieri, J.G. Development of a Review-of-Systems Screening Tool for Orthopaedic Physical Therapists: Results From the Optimal Screening for Prediction of Referral and Outcome (OSPRO) Cohort. J. Orthop. Sports Phys. Ther. 2015, 45, 512–526. [Google Scholar] [CrossRef]
- Fisher, R.S.; Cross, J.H.; D’Souza, C.; French, J.A.; Haut, S.R.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshé, S.L.; et al. Instruction manual for the ILAE 2017 operational classification of seizure types. Epilepsia 2017, 58, 531–542. [Google Scholar] [CrossRef] [Green Version]
- Khasnis, A.; Gokula, R.M. Romberg’s test. J. Postgrad. Med. 2003, 49, 169–172. [Google Scholar] [PubMed]
- Li, N.; Dierks, G.; Vervaeke, H.E.; Jumonville, A.; Kaye, A.D.; Myrcik, D.; Paladini, A.; Varrassi, G.; Viswanath, O.; Urits, I. Thoracic Outlet Syndrome: A Narrative Review. J. Clin. Med. 2021, 10, 962. [Google Scholar] [CrossRef] [PubMed]
- Beliaev, A.M.; Fougere, C. Thoracic outlet syndrome secondary to a mid-clavicle malunion. BMJ Case Rep. 2015, 2015, bcr2015209583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.Y.; Oh, K.S.; Yoo, H.Y.; Lee, J.G. Case Report: Thoracic Outlet Syndrome in an Elite Archer in Full-draw Position. Clin. Orthop. Relat. Res. 2013, 471, 3056–3060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styrke, J.; Stålnacke, B.M.; Bylund, P.O.; Sojka, P.; Björnstig, U. A 10-year incidence of acute whiplash injuries after road traf-fic crashes in a defined population in Northern Sweden. PM R 2012, 4, 739–747. [Google Scholar]
- Postacchini, F.; Gumina, S.; De Santis, P.; Albo, F. Epidemiology of clavicle fractures. J. Should. Elb. Surg. 2002, 11, 452–456. [Google Scholar] [CrossRef]
- Amer, K.M.; Congiusta, D.V.; Suri, P.; Choudhry, A.; Otero, K.; Adams, M. Clavicle fractures: Associated trauma and morbidity. J. Clin. Orthop. Trauma 2021, 13, 53–56. [Google Scholar] [CrossRef]
- Dessureault-Dober, I.; Bronchti, G.; Bussières, A. Diagnostic Accuracy of Clinical Tests for Neurogenic and Vascular Thoracic Outlet Syndrome: A Systematic Review. J. Manip. Physiol. Ther. 2018, 41, 789–799. [Google Scholar] [CrossRef]
- Watson, L.; Pizzari, T.; Balster, S. Thoracic outlet syndrome Part 2: Conservative management of thoracic outlet. Man. Ther. 2010, 15, 305–314. [Google Scholar] [CrossRef]
- Hardy, A.; Pougès, C.; Wavreille, G.; Behal, H.; Demondion, X.; Lefebvre, G. Thoracic Outlet Syndrome: Diagnostic Accuracy of MRI. Orthop. Traumatol. Surg. Res. 2019, 105, 1563–1569. [Google Scholar] [CrossRef]
- Anwar, H.; Khan, Q.U.; Nadeem, N.; Pervaiz, I.; Ali, M.; Cheema, F.F. Epileptic seizures. Discoveries 2020, 8, e110. [Google Scholar] [CrossRef]
- Liang, S.; Fan, X.; Zhao, M.; Shan, X.; Li, W.; Ding, P.; You, G.; Hong, Z.; Yang, X.; Luan, G.; et al. Clinical practice guidelines for the diagnosis and treatment of adult diffuse glioma-related epi-lepsy. Cancer Med. 2019, 8, 4527–4535. [Google Scholar] [CrossRef] [Green Version]
- Pallud, J.; Audureau, E.; Blonski, M.; Sanai, N.; Bauchet, L.; Fontaine, D.; Mandonnet, E.; Dezamis, E.; Psimaras, D.; Guyotat, J.; et al. Epileptic seizures in diffuse low-grade gliomas in adults. Brain 2013, 137, 449–462. [Google Scholar] [CrossRef] [Green Version]
- Kerkhof, M.; Vecht, C.J. Seizure characteristics and prognostic factors of gliomas. Epilepsia 2013, 54, 12–17. [Google Scholar] [CrossRef]
- You, G.; Sha, Z.; Jiang, T. Clinical Diagnosis and Perioperative Management of Glioma-Related Epilepsy. Front. Oncol. 2021, 10, 550353. [Google Scholar] [CrossRef]
- Maselli, F.; Palladino, M.; Barbari, V.; Storari, L.; Rossettini, G.; Testa, M. The diagnostic value of Red Flags in thoracolumbar pain: A systematic review. Disabil. Rehabil. 2020, 1–17. [Google Scholar] [CrossRef]
- Valton, L.; Benaiteau, M.; Denuelle, M.; Rulquin, F.; Le Camus, C.H.; Hein, C.; Viguier, A.; Curot, J. Etiological assessment of status epilepticus. Rev. Neurol. 2020, 176, 408–426. [Google Scholar] [CrossRef]
- Davis, M.E. Glioblastoma: Overview of Disease and Treatment. Clin. J. Oncol. Nurs. 2016, 20, S2–S8. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Friedmann-Morvinski, D. Glioblastoma Heterogeneity and Cancer Cell Plasticity. Crit. Rev. Oncog. 2014, 19, 327–336. [Google Scholar] [CrossRef]
- Desland, F.A.; Hormigo, A. The CNS and the Brain Tumor Microenvironment: Implications for Glioblastoma Immunotherapy. Int. J. Mol. Sci. 2020, 21, 7358. [Google Scholar] [CrossRef]
- Zhou, W.; Wahl, D.R. Metabolic Abnormalities in Glioblastoma and Metabolic Strategies to Overcome Treatment Resistance. Cancers 2019, 11, 1231. [Google Scholar] [CrossRef] [Green Version]
- Gokden, M. If it is Not a Glioblastoma, Then What is it? A Differential Diagnostic Review. Adv. Anat. Pathol. 2017, 24, 379–391. [Google Scholar] [CrossRef]
- Solís, S.T.; Ahicart, G.P.; Lozano, I.I.; Schmidt, C.D.Q.; Coello, A.F.; Panisello, C.H.; Urzaiz, L.L.; Romero, J.C.G.; Valle, R.D.; Sánchez, J.G.; et al. Glioblastoma treatment guidelines: Consensus by the Spanish Society of Neurosurgery Tumor Section. Neurocirugía 2020, 31, 289–298. [Google Scholar] [CrossRef]
- Ceccarelli, C.; Brindisino, F.; Salomon, M.; Heick, J.D.; Maselli, F. A Rare Consequence after Shoulder Dislocation in a Professional Cyclist: A Case Report. Medicina 2019, 55, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maselli, F.; Rossettini, G.; Viceconti, A.; Testa, M. Importance of screening in physical therapy: Vertebral fracture of thoracolumbar junction in a recreational runner. BMJ Case Rep. 2019, 12, e229987. [Google Scholar] [CrossRef]
- Mourad, F.; Cataldi, F.; Patuzzo, A.; Tunnera, S.; Dunning, J.; Fernández-De-Las-Peñas, C.; Maselli, F. Craniopharyngioma in a young woman with symptoms presenting as mechanical neck pain associated with cervicogenic headache: A case report. Physiother. Theory Pract. 2021, 37, 549–558. [Google Scholar] [CrossRef]
- Maselli, F.; Testa, M. Superficial peroneal nerve schwannoma presenting as lumbar radicular syndrome in a non-competitive runner. J. Back Musculoskelet. Rehabil. 2019, 32, 361–365. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Storari, L.; Signorini, M.; Barbari, V.; Mourad, F.; Bisconti, M.; Salomon, M.; Rossettini, G.; Maselli, F. A Thoracic Outlet Syndrome That Concealed a Glioblastoma. Findings from a Case Report. Medicina 2021, 57, 908. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090908
Storari L, Signorini M, Barbari V, Mourad F, Bisconti M, Salomon M, Rossettini G, Maselli F. A Thoracic Outlet Syndrome That Concealed a Glioblastoma. Findings from a Case Report. Medicina. 2021; 57(9):908. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090908
Chicago/Turabian StyleStorari, Lorenzo, Manuel Signorini, Valerio Barbari, Firas Mourad, Mattia Bisconti, Mattia Salomon, Giacomo Rossettini, and Filippo Maselli. 2021. "A Thoracic Outlet Syndrome That Concealed a Glioblastoma. Findings from a Case Report" Medicina 57, no. 9: 908. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090908