
Efficacy of Whole-Blood Del Nido Cardioplegia Compared with Diluted Del Nido Cardioplegia in Coronary Artery Bypass Grafting: A Retrospective Monocentric Analysis of Pakistan


Abstract
:1. Introduction
2. Materials and Methods
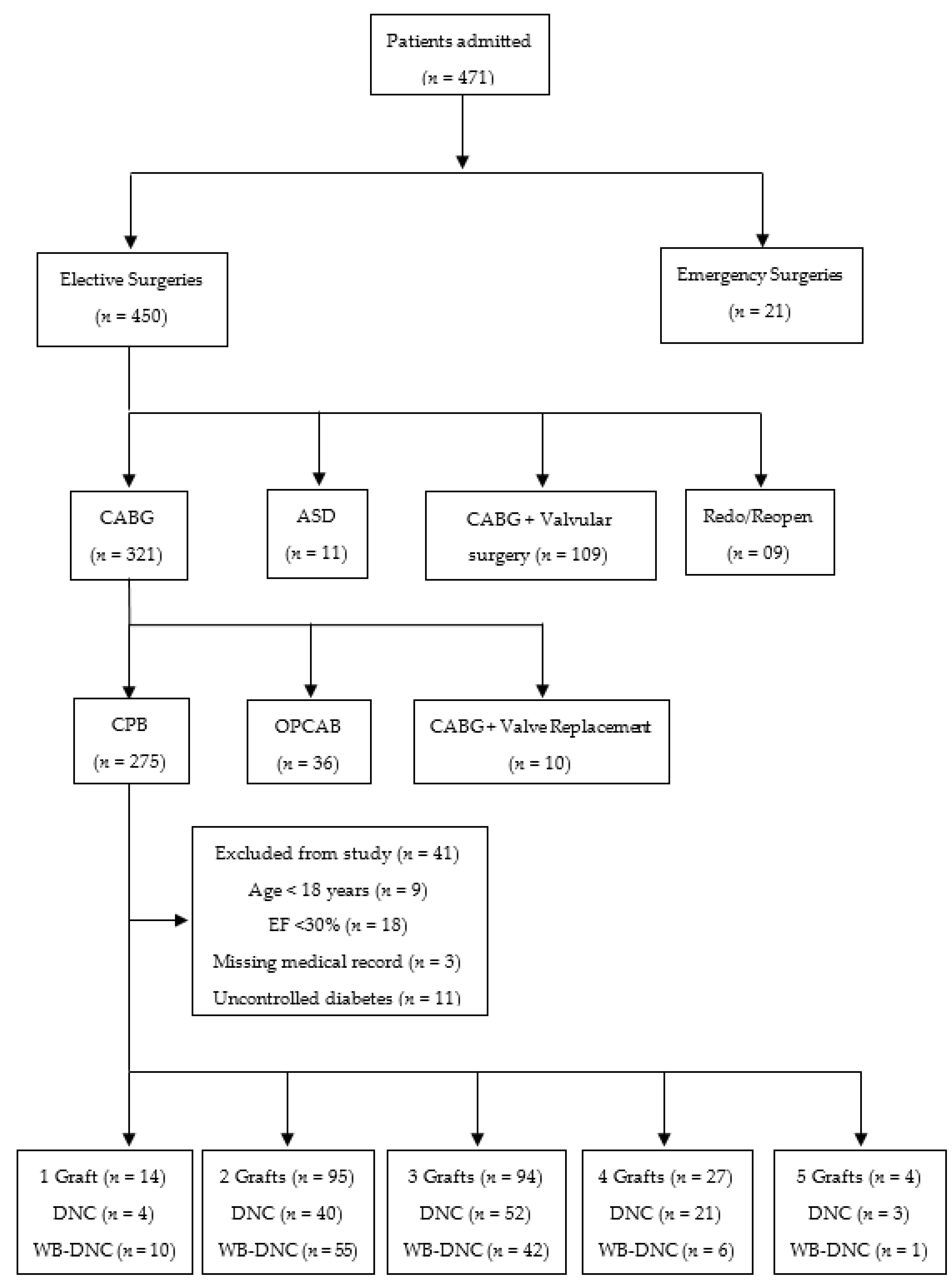
2.1. Study Design and Patients
2.2. Preoperative Details
2.3. Perioperative Details
2.4. Cardioplegia Protocol
2.5. Post-Operative Details
2.6. Study Endpoints
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Allen, B.S. Myocardial protection: A forgotten modality. Eur. J. Cardio-Thorac. Surg. 2020, 57, 263–270. [Google Scholar] [CrossRef]
- Moktan Lama, P.B.; Khakural, P.; Sigdel, S.; Raj Bhatta, M.; Sah Teli, R.; Baral, R.K.; Bhattarai, A.; Pradhan, B.; Koirala, B. Del Nido Cardioplegia in Coronary Artery Bypass Grafting Surgery: A safe, efficacious and economic alternative to St. Thomas solution; an experience from a developing nation. Perfusion 2021, 36, 0267659121991033. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Jeong, J.H.; Moon, S.J.; Ahn, H.; Hwang, H.Y. Sufficient myocardial protection of del Nido cardioplegia regardless of ventricular mass and myocardial ischemic time in adult cardiac surgical patients. J. Thorac. Dis. 2016, 8, 2004. [Google Scholar] [CrossRef] [Green Version]
- Matte, G.S.; Pedro, J. History and use of del Nido cardioplegia solution at Boston Children’s Hospital. J. Extra-Corpor. Technol. 2012, 44, 98. [Google Scholar] [PubMed]
- Li, Y.; Lin, H.; Zhao, Y.; Li, Z.; Liu, D.; Wu, X.; Ji, B.; Gao, B. Del Nido cardioplegia for myocardial protection in adult cardiac surgery: A systematic review and meta-analysis. Asaio J. 2018, 64, 360–367. [Google Scholar] [CrossRef]
- James, T.M.; Stamou, S.C.; Faber, C.; Nores, M.A. Whole Blood del Nido versus Cold Blood Microplegia in Adult Cardiac Surgery: A Propensity-Matched Analysis. Int. J. Angiol. 2019. [Google Scholar] [CrossRef]
- Ota, T.; Yerebakan, H.; Neely, R.C.; Mongero, L.; George, I.; Takayama, H.; Williams, M.R.; Naka, Y.; Argenziano, M.; Bacha, E. Short-term outcomes in adult cardiac surgery in the use of del Nido cardioplegia solution. Perfusion 2016, 31, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Owen, C.M.; Asopa, S.; Smart, N.A.; King, N. Microplegia in cardiac surgery: Systematic review and meta-analysis. J. Card. Surg. 2020, 35, 2737–2746. [Google Scholar] [CrossRef] [PubMed]
- Algarni, K.D.; Weisel, R.D.; Caldarone, C.A.; Maganti, M.; Tsang, K.; Yau, T.M. Microplegia during coronary artery bypass grafting was associated with less low cardiac output syndrome: A propensity-matched comparison. Ann. Thorac. Surg. 2013, 95, 1532–1538. [Google Scholar] [CrossRef] [PubMed]
- Gerdisch, M.W.; Robinson, S.; David, G.; Makepeace, S.; Ryan, M.P.; Gunnarsson, C. Clinical and economic benefits of advanced microplegia delivery system in cardiac surgery: Evidence from 250 hospitals. J. Comp. Eff. Res. 2018, 7, 673–683. [Google Scholar] [CrossRef] [Green Version]
- Grimm, K.; Twerenbold, R.; Abaecherli, R.; Boeddinghaus, J.; Nestelberger, T.; Koechlin, L.; Troester, V.; Bourtzou, A.; Keller, D.I.; Geigy, N. Diagnostic and prognostic value of ST-segment deviation scores in suspected acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 857–868. [Google Scholar] [CrossRef]
- Albacker, T.B.; Chaturvedi, R.; Al Kindi, A.H.; Al-Habib, H.; Al-Atassi, T.; De Varennes, B.; Lachapelle, K. The effect of using microplegia on perioperative morbidity and mortality in elderly patients undergoing cardiac surgery. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. Euroscore ii. Eur. J. Cardio-Thorac. Surg. 2012, 41, 734–745. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, J.P.; Mavroudis, C.; Jacobs, M.L.; Maruszewski, B.; Tchervenkov, C.I.; Lacour-Gayet, F.G.; Clarke, D.R.; Yeh, T., Jr.; Walters, H.L., III; Kurosawa, H. What is operative mortality? Defining death in a surgical registry database: A report of the STS Congenital Database Taskforce and the Joint EACTS-STS Congenital Database Committee. Ann. Thorac. Surg. 2006, 81, 1937–1941. [Google Scholar] [CrossRef] [PubMed]
- Vickerstaff, V.; Omar, R.Z.; Ambler, G. Methods to adjust for multiple comparisons in the analysis and sample size calculation of randomised controlled trials with multiple primary outcomes. BMC Med Res. Methodol. 2019, 19, 129. [Google Scholar]
- Valooran, G.J.; Nair, S.K.; Chandrasekharan, K.; Simon, R.; Dominic, C. del Nido cardioplegia in adult cardiac surgery-scopes and concerns. Perfusion 2016, 31, 6–14. [Google Scholar] [CrossRef]
- Nardi, P.; Pisano, C.; Bertoldo, F.; Ruvolo, G. New insights on the use of del Nido cardioplegia in the adult cardiac surgery. J. Thorac. Dis. 2018, 10, S3233. [Google Scholar] [CrossRef]
- Loberman, D.; Neely, R.; Fitzgerald, D.; McGurk, S.; Rajab, T.K. Modified del Nido cardioplegia in adult cardiac surgery; safety and efficacy. J. Cardiol. Curr. Res. 2014, 1, 00042. [Google Scholar]
- Lomivorotov, V.V.; Efremov, S.M.; Kirov, M.Y.; Fominskiy, E.V.; Karaskov, A.M. Low-cardiac-output syndrome after cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2017, 31, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Habib, R.H.; Zacharias, A.; Schwann, T.A.; Riordan, C.J.; Engoren, M.; Durham, S.J.; Shah, A. Role of hemodilutional anemia and transfusion during cardiopulmonary bypass in renal injury after coronary revascularization: Implications on operative outcome. Crit. Care Med. 2005, 33, 1749–1756. [Google Scholar] [CrossRef] [PubMed]
- Fukui, M.; Généreux, P.; Cavalcante, J.L. Assessment of Cardiac Damage in Aortic Stenosis. Cardiol. Clin. 2020, 38, 23–31. [Google Scholar] [CrossRef]
- Devereaux, P.; Xavier, D.; Pogue, J.; Guyatt, G.; Sigamani, A.; Garutti, I.; Leslie, K.; Rao-Melacini, P.; Chrolavicius, S.; Yang, H. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: A cohort study. Ann. Intern. Med. 2011, 154, 523–528. [Google Scholar] [CrossRef]
- Landesberg, G.; Shatz, V.; Akopnik, I.; Wolf, Y.G.; Mayer, M.; Berlatzky, Y.; Weissman, C.; Mosseri, M. Association of cardiac troponin, CK-MB, and postoperative myocardial ischemia with long-term survival after major vascular surgery. J. Am. Coll. Cardiol. 2003, 42, 1547–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, Y.; Ohtani, M.; Hiraishi, T.; Kobayashi, Y.; Nakamura, T. “Initial, continuous and intermittent bolus” administration of minimally-diluted blood cardioplegia supplemented with potassium and magnesium for hypertrophied hearts. Heart Lung Circ. 2006, 15, 325–331. [Google Scholar] [CrossRef]
- Koechlin, L.; Rrahmani, B.; Gahl, B.; Berdajs, D.; Grapow, M.T.; Eckstein, F.S.; Reuthebuch, O. Microplegia versus Cardioplexol® in coronary artery bypass surgery with minimal extracorporeal circulation: Comparison of two cardioplegia concepts. Thorac. Cardiovasc. Surg. 2020, 68, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Duan, L.; Zhang, C.f.; Luo, W.j.; Gao, Y.; Chen, R.; Hu, G. Does magnesium-supplemented cardioplegia reduce cardiac injury? A meta-analysis of randomized controlled trials. J. Card. Surg. 2015, 30, 338–345. [Google Scholar] [CrossRef]
- McCann, C.J.; Glover, B.M.; Menown, I.B.; Moore, M.J.; McEneny, J.; Owens, C.G.; Smith, B.; Sharpe, P.C.; Young, I.S.; Adgey, J.A. Novel biomarkers in early diagnosis of acute myocardial infarction compared with cardiac troponin T. Eur. Heart J. 2008, 29, 2843–2850. [Google Scholar] [CrossRef] [Green Version]
- Ad, N.; Holmes, S.D.; Massimiano, P.S.; Rongione, A.J.; Fornaresio, L.M.; Fitzgerald, D. The use of del Nido cardioplegia in adult cardiac surgery: A prospective randomized trial. J. Thorac. Cardiovasc. Surg. 2018, 155, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Currigan, D.A.; Hughes, R.J.; Wright, C.E.; Angus, J.A.; Soeding, P.F. Vasoconstrictor responses to vasopressor agents in human pulmonary and radial arteries: An in vitro study. Anesthesiology 2014, 121, 930–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamazaki, Y.; Oba, K.; Matsui, Y.; Morimoto, Y. Vasoactive-inotropic score as a predictor of morbidity and mortality in adults after cardiac surgery with cardiopulmonary bypass. J. Anesth. 2018, 32, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Paparella, D.; Guida, P.; Caparrotti, S.; Fanelli, V.; Martinelli, G.; Mazzei, V.; Zaccaria, S.; Bisceglia, L.; Scrascia, G. Myocardial damage influences short-and mid-term survival after valve surgery: A prospective multicenter study. J. Thorac. Cardiovasc. Surg. 2014, 148, 2373–2379.e2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adabag, A.S.; Rector, T.; Mithani, S.; Harmala, J.; Ward, H.B.; Kelly, R.F.; Nguyen, J.T.; McFalls, E.O.; Bloomfield, H.E. Prognostic significance of elevated cardiac troponin I after heart surgery. Ann. Thorac. Surg. 2007, 83, 1744–1750. [Google Scholar] [CrossRef] [PubMed]
- Bhika, S. Does the Use of Microplegia Significantly Improve Outcomes in Congenital Heart Surgery. Ph.D. Thesis, University of Witwatersrand, Johannesburg, South Africa, 2019. [Google Scholar]
- Timek, T.A.; Beute, T.; Robinson, J.A.; Zalizadeh, D.; Mater, R.; Parker, J.L.; Lypka, M.; Willekes, C.L. Del Nido cardioplegia in isolated adult coronary artery bypass surgery. J. Thorac. Cardiovasc. Surg. 2020, 160, 1479–1485.e1475. [Google Scholar] [CrossRef]
- López-Menéndez, J.; Miguelena, J.; Morales, C.; Díaz, C.L.; Callejo, F.; Llosa, J.C.; Silva, J. Celsior versus microplegia: Analysis of myocardial protection in elective aortic valve replacement. Ann. Thorac. Surg. 2017, 103, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Øvrum, E.; Tangen, G.; Tølløfsrud, S.; Øystese, R.; Ringdal, M.-A.L.; Istad, R. Cold blood versus cold crystalloid cardioplegia: A prospective randomised study of 345 aortic valve patients. Eur. J. Cardio-Thorac. Surg. 2010, 38, 745–749. [Google Scholar] [CrossRef]
- Sellevold, O.F.; Berg, E.M.; Levang, O.W. Procaine is effective for minimizing postischemic ventricular fibrillation in cardiac surgery. Anesth. Analg. 1995, 81, 932–938. [Google Scholar]
- Onorati, F.; Santini, F.; Dandale, R.; Ucci, G.; Pechlivanidis, K.; Menon, T.; Chiominto, B.; Mazzucco, A.; Faggian, G. “Polarizing” microplegia improves cardiac cycle efficiency after CABG for unstable angina. Int. J. Cardiol. 2013, 167, 2739–2746. [Google Scholar] [CrossRef] [PubMed]
- Kirmani, B.H.; Muir, A.D.; Poullis, M.P.; Pullan, D.M. Conversion after off-pump coronary artery bypass grafting: Where are the quality markers? Eur. J. Cardio-Thorac. Surg. 2017, 52, 829–830. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Ingredient | Diluted (DNC) | Whole-Blood (WB-DNC) |
|---|---|---|
| Base (1.0 L) | (Blood: Ringer Lactate = 1:4) | Blood |
| KCl (mEq) | 26 | 26 |
| 8.4% NaHCO3 (mEq) | 13 | 13 |
| 25% Mannitol (mL) | 13 | 13 |
| 50% MgSO4 (mL) | 4 | 4 |
| 2% Lidocaine (mL) | 6.5 | 6.5 |
| Parameter | Group; Median (Range) | p-Value | |
|---|---|---|---|
| DNC (n = 120) | WB-DNC (n = 114) | ||
| Age (year) | 56 (41–76) | 55 (39–72) | 0.554 |
| Sex (male) n (%) | 109 (90.83) | 97 (85.08) | 0.125 |
| Weight (kg) | 72.45 (52.30–126.60) | 72.90 (51.50–105.00) | 0.666 |
| Height (cm) | 165.50 (138–197) | 165 (140–193) | 0.606 |
| Body mass index (kg/m2) * | 27.18 ± 5.05 | 26.74 ± 4.53 | 0.193 |
| Diabetes mellitus (yes); n (%) | 74 (61.66) | 72 (63.15) | 0.460 |
| Smoker (yes) n (%) | 18 (15) | 16 (14.03) | 0.491 |
| Ejection fraction (%) | 54 (32–67) | 54 (30–65) | 0.345 |
| EuroSCORE-II | 1.50 (1.00–3.00) | 1.40 (1.00–3.00) | 0.767 |
| Blood urea (mg/dL) | 28 (16–55) | 32 (18–66) | 0.003 |
| Serum creatinine (mg/dL) | 1.00 (0.50–1.72) | 1.00 (0.50–1.78) | 0.930 |
| Serum bilurubin (mg/dL) | 0.72 (0.35–2.63) | 0.70 (0.29–2.47) | 0.931 |
| Hemoglobin (mg/dL) * | 14.37 ± 1.93 | 14.41 ± 1.65 | 0.117 |
| SGPT (U/L) | 25 (14–78) | 29 (15–79) | 0.081 |
| SGOT (U/L) | 30.50 (16–91) | 35 (15–87) | 0.235 |
| Alkaline phosphatase (U/L) | 104 (46–633) | 102.50 (49–449) | 0.933 |
| White blood cells count (103/μL) | 10.20 (4.20–19.50) | 10.00 (5.00–19.60) | 0.976 |
| Platelets count (103/μL) | 226.50 (110–662) | 210 (87–665) | 0.482 |
| Parameter | Group; Median (Range) | p-Value | |
|---|---|---|---|
| DNC (n = 120) | WB-DNC (n = 114) | ||
| Blood urea (mg/dL) | 38 (20–87) | 32.50 (18–97) | 0.006 |
| Serum creatinine (mg/dL) | 1.24 (0.80–1.90) | 1.10 (0.40–1.80) | 0.001 |
| SGPT (U/L) | 35.50 (17–122) | 29 (13–107) | 0.065 |
| SGOT (U/L) | 73 (20–182) | 52.50 (23–183) | 0.011 |
| White blood cells count (103/uL) | 19.15 (11.70–38.80) | 18 (8.90–39) | 0.027 |
| Platelets count (103/uL) | 160.50 (68–577) | 162 (76–521) | 0.577 |
| Serum potassium (mEq/L) | 4.30 (2.39–5.25) | 4.30 (3.29–5.42) | 0.868 |
| Peak Troponin-T (ng/L) | 394.50 (151–532) | 219.50 (150–518) | 0.001 |
| Peak creatine kinase myocardial band (μg/L) | 25 (15–37) | 14 (9–32) | 0.001 |
| Atrial defibrillation; n (%) yes | 12 (7.75) | 09 (7.56) | 0.370 |
| Spontaneous recovery of heart beat; n (%) | 108 (90.00) | 105 (92.10) | 0.573 |
| Pacemaker; n (%) | 3 (2.50) | 0 (0.00) | 0.133 |
| Amount of blood loss (mL) | 515 (40–1680) | 490 (100–1850) | 0.681 |
| Blood transfusions; n (%) yes | 21 (17.50) | 14 (12.28) | 0.175 |
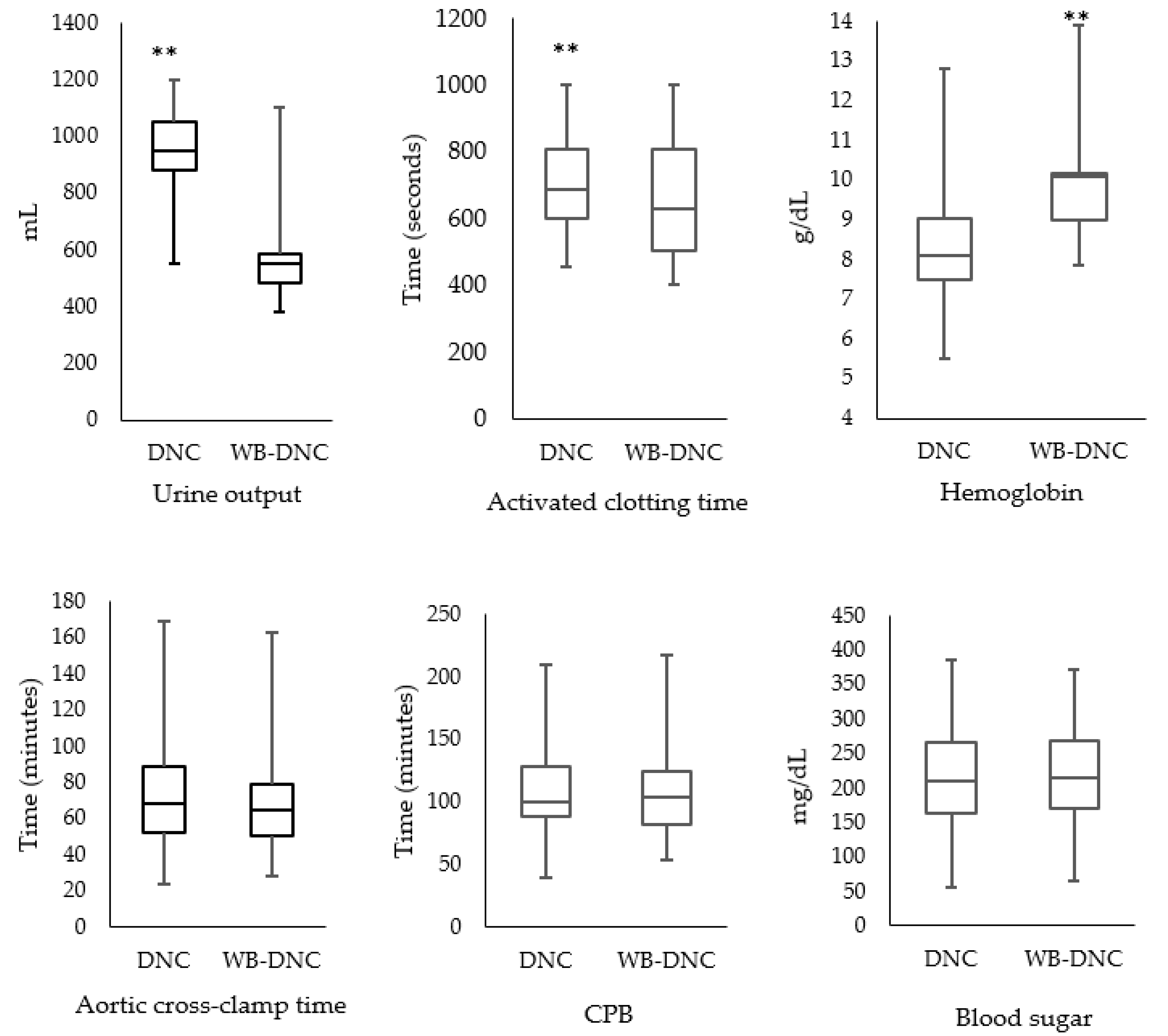
| Hemoglobin (mg/dL) after weaning of CPB | 9.10 (6.40–12.10) | 10.10 (6.90–14.15) | 0.001 |
| Hemoglobin after shifting to ICU (mg/dL) | 10.30 (7.15–14.50) | 11.10 (8.00–15.70) | 0.001 |
| Activated clotting time (seconds) | 107 (90–149) | 112 (92–160) | 0.156 |
| Adrenaline infusion rate (mcg/kg/min) | 0.08 (0.02–0.16) | 0.04 (0–0.12) | <0.001 |
| Dopamin infusion rate (mcg/kg/min) | 4 (3–10) | 4 (2–8) | 0.174 |
| Time to extubation (minutes) | 120 (52–1935) | 120 (24–940) | 0.757 |
| ICU stay (days) | 5 (1–9) | 5 (2–9) | 0.701 |
| In-hospital stay (days) | 8 (5–14) | 7 (5–10) | 0.001 |
| Mortality; n (%) | 2 (1.66) | 1 (0.87) | 0.519 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, A.; Khwaja, I.A.; Khan, A.H.; Yousaf, M.S.; Zaneb, H.; Qureshi, A.B.; Rehman, H. Efficacy of Whole-Blood Del Nido Cardioplegia Compared with Diluted Del Nido Cardioplegia in Coronary Artery Bypass Grafting: A Retrospective Monocentric Analysis of Pakistan. Medicina 2021, 57, 918. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090918
Haider A, Khwaja IA, Khan AH, Yousaf MS, Zaneb H, Qureshi AB, Rehman H. Efficacy of Whole-Blood Del Nido Cardioplegia Compared with Diluted Del Nido Cardioplegia in Coronary Artery Bypass Grafting: A Retrospective Monocentric Analysis of Pakistan. Medicina. 2021; 57(9):918. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090918
Chicago/Turabian StyleHaider, Adnan, Irfan Azmatullah Khwaja, Ammar Hameed Khan, Muhammad Shahbaz Yousaf, Hafsa Zaneb, Abdul Basit Qureshi, and Habib Rehman. 2021. "Efficacy of Whole-Blood Del Nido Cardioplegia Compared with Diluted Del Nido Cardioplegia in Coronary Artery Bypass Grafting: A Retrospective Monocentric Analysis of Pakistan" Medicina 57, no. 9: 918. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090918