
Low Intensity Extracorporeal Shock Wave Therapy as a Novel Treatment for Stress Urinary Incontinence: A Randomized-Controlled Clinical Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
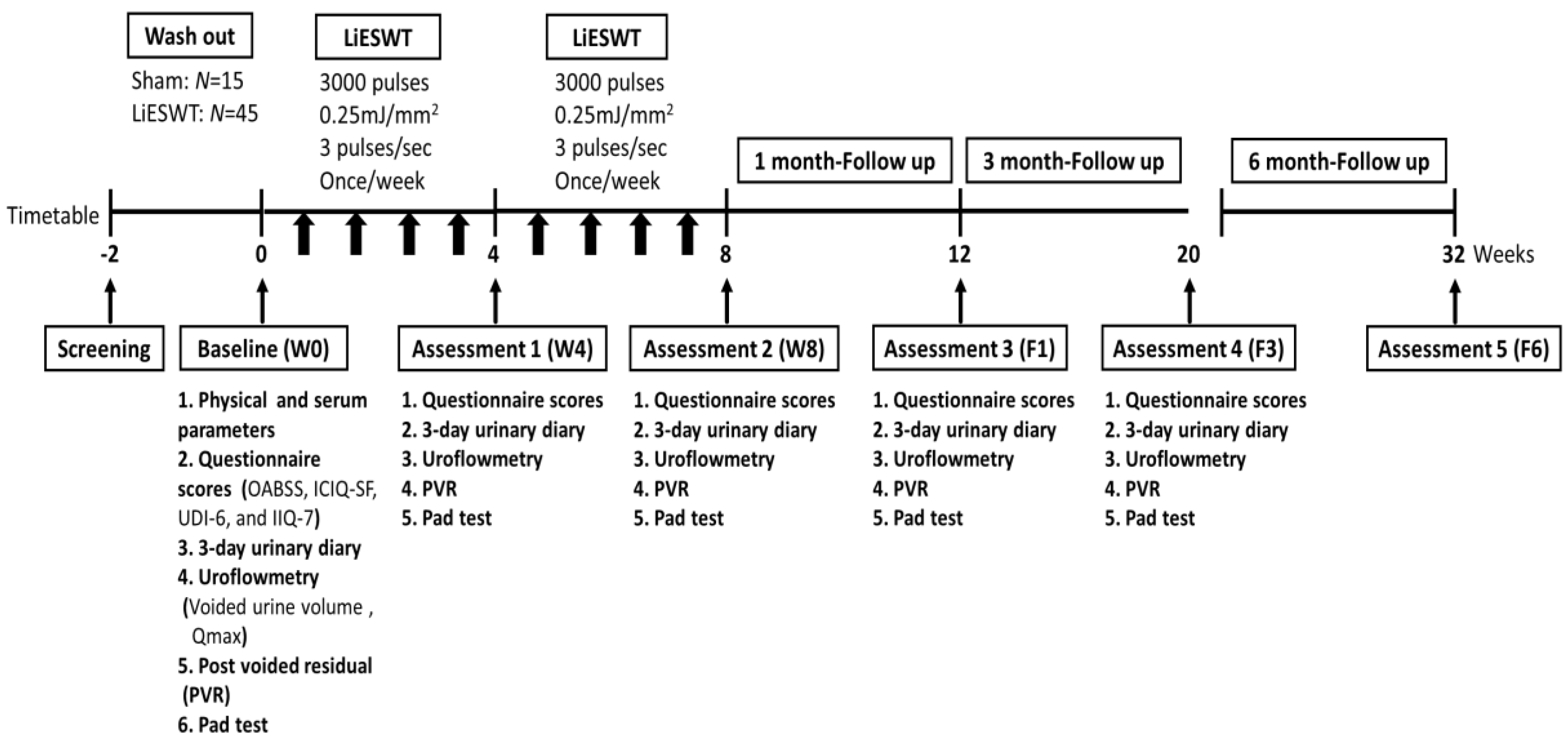
2.1. Design
2.2. Physical Indicators and Biochemical Parameters of Studied Participants
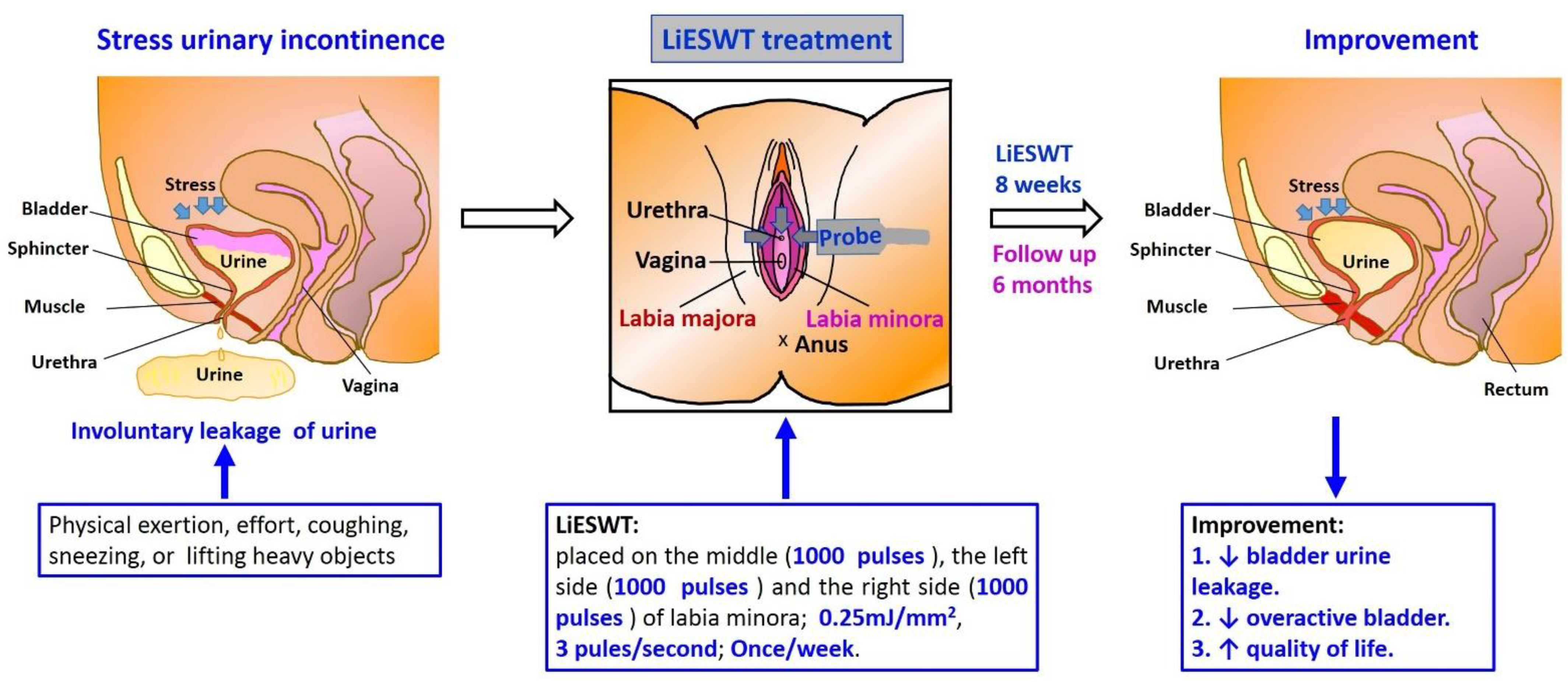
2.3. Procedure and Medical Information of LiESWT
2.4. Pad Test for the Evaluation of SUI
2.5. Outcomes Measures and Therapeutic Efficacy Assessment for LiESWT
2.6. Statistical Analysis
3. Results
3.1. Diagnoses
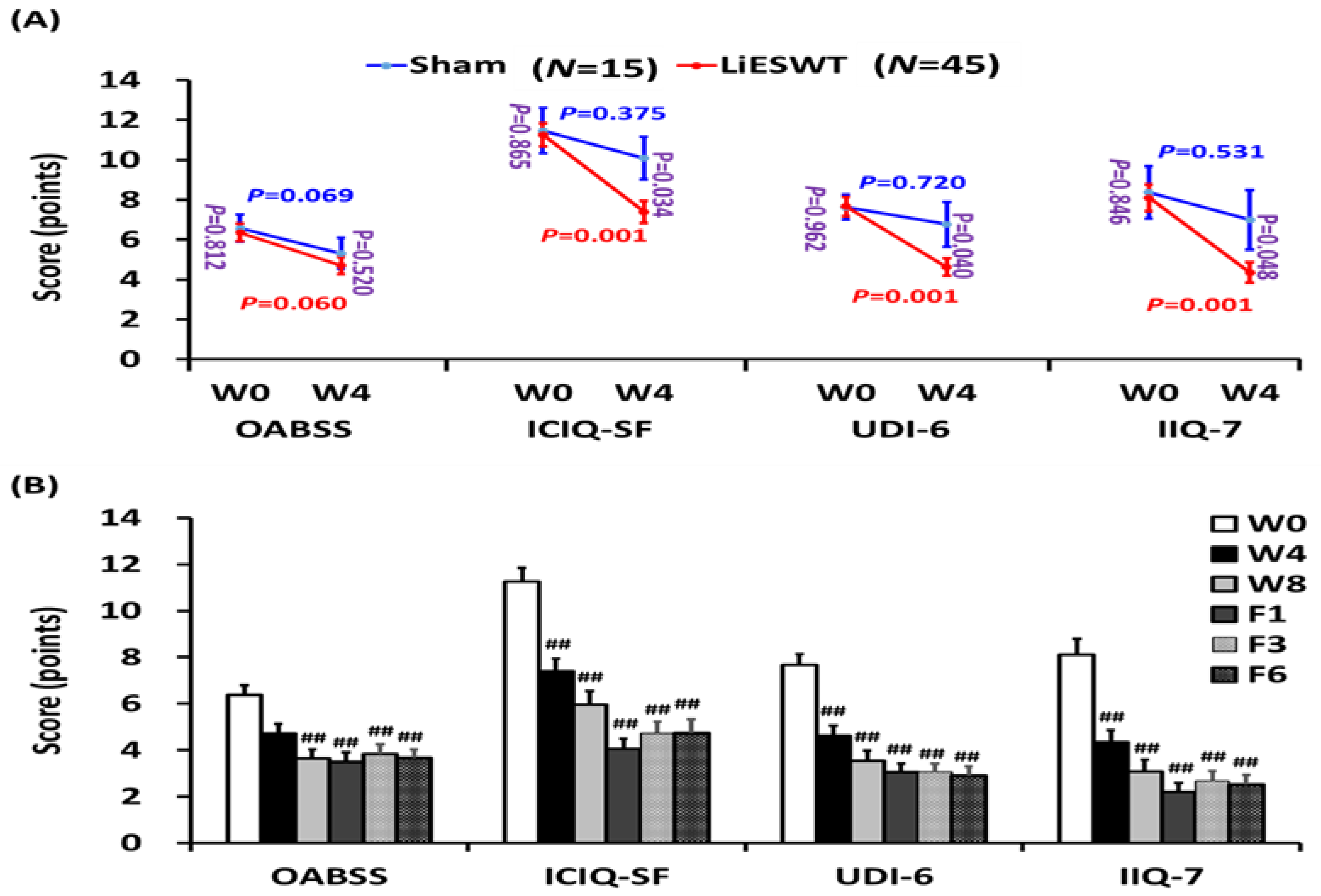
3.2. Primary and Secondary End Points
3.3. Safety and Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-Committee of the International Continence Society. The standardisation of terminology in lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Urology 2003, 61, 37–49. [Google Scholar] [CrossRef]
- Hannestad, Y.S.; Rortveit, G.; Sandvik, H.; Hunskaar, S. A community-based epidemiological survey of female urinary incontinence: The Norwegian EPINCONT study. J. Clin. Epidemiol. 2000, 53, 1150–1157. [Google Scholar] [CrossRef]
- Dumoulin, C.; Hay-Smith, E.J.; Mac Habee-Seguin, G. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database Syst. Rev. 2014, CD005654. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.A.; Rogerson, L.; Cody, J.D.; Ogah, J. Mid-urethral sling operations for stress urinary incontinence in women. Cochrane Database Syst. Rev. 2015, CD006375. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.H.; Lee, C.K.; Chang, S.D.; Chien, P.C.; Hsu, Y.Y.; Tseng, L.H. Focusing on long-term complications of mid-urethral slings among women with stress urinary incontinence as a patient safety improvement measure: A protocol for systematic review and meta-analysis. Medicine 2021, 100, e26257. [Google Scholar] [CrossRef]
- Ogden, J.A.; Toth-Kischkat, A.; Schultheiss, R. Principles of shock wave therapy. Clin. Orthop. Relat. Res. 2001, 387, 8–17. [Google Scholar] [CrossRef]
- Wu, A.K.; Zhang, X.; Wang, J.; Ning, H.; Zaid, U.; Villalta, J.D.; Wang, G.; Banie, L.; Lin, G.; Lue, T.F. Treatment of stress urinary incontinence with low-intensity extracorporeal shock wave therapy in a vaginal balloon dilation induced rat model. Transl. Androl. Urol. 2018, 7, S7–S16. [Google Scholar] [CrossRef] [Green Version]
- Hsiao, C.C.; Huang, W.H.; Cheng, K.H.; Lee, C.T. Low-Energy Extracorporeal Shock Wave Therapy Ameliorates Kidney Function in Diabetic Nephropathy. Oxid. Med. Cell. Longev. 2019, 2019, 8259645. [Google Scholar] [CrossRef]
- Chung, E.; Cartmill, R. Evaluation of clinical efficacy, safety and patient satisfaction rate after low-intensity extracorporeal shockwave therapy for the treatment of male erectile dysfunction: An Australian first open-label single-arm prospective clinical trial. BJU Int. 2015, 115 (Suppl. 5), 46–49. [Google Scholar] [CrossRef] [Green Version]
- Kitrey, N.D.; Vardi, Y.; Appel, B.; Shechter, A.; Massarwi, O.; Abu-Ghanem, Y.; Gruenwald, I. Low Intensity Shock Wave Treatment for Erectile Dysfunction—How Long Does the Effect Last? J. Urol. 2018, 200, 167–170. [Google Scholar] [CrossRef]
- Chung, E.; Wang, J. A state-of-art review of low intensity extracorporeal shock wave therapy and lithotripter machines for the treatment of erectile dysfunction. Expert Rev. Med. Devices 2017, 14, 929–934. [Google Scholar] [CrossRef]
- Guu, S.J.; Geng, J.H.; Chao, I.T.; Lin, H.T.; Lee, Y.C.; Juan, Y.S.; Liu, C.C.; Wang, C.J.; Tsai, C.C. Efficacy of Low-Intensity Extracorporeal Shock Wave Therapy on Men with Chronic Pelvic Pain Syndrome Refractory to 3-As Therapy. Am. J. Men’s Health 2018, 12, 441–452. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, R.; Cumpanas, A.; Miclea, F.; Janetschek, G. Extracorporeal shock wave therapy for the treatment of chronic pelvic pain syndrome in males: A randomised, double-blind, placebo-controlled study. Eur. Urol. 2009, 56, 418–424. [Google Scholar] [CrossRef]
- Zhang, X.; Ruan, Y.; Wu, A.K.; Zaid, U.; Villalta, J.D.; Wang, G.; Banie, L.; Reed-Maldonado, A.B.; Lin, G.; Lue, T.F. Delayed Treatment with Low-intensity Extracorporeal Shock Wave Therapy in an Irreversible Rat Model of Stress Urinary Incontinence. Urology 2020, 141, e181–e187. [Google Scholar] [CrossRef]
- Long, C.Y.; Lin, K.L.; Lee, Y.C.; Chuang, S.M.; Lu, J.H.; Wu, B.N.; Chueh, K.S.; Ker, C.R.; Shen, M.C.; Juan, Y.S. Therapeutic effects of Low intensity extracorporeal low energy shock wave therapy (LiESWT) on stress urinary incontinence. Sci. Rep. 2020, 10, 5818. [Google Scholar] [CrossRef] [Green Version]
- Ströher, R.L.M.; Sartori, M.G.F.; Takano, C.C.; de Araújo, M.P.; Girão, M. Metabolic syndrome in women with and without stress urinary incontinence. Int. Urogynecol. J. 2020, 31, 173–179. [Google Scholar] [CrossRef]
- Krhut, J.; Zachoval, R.; Smith, P.P.; Rosier, P.F.; Valansky, L.; Martan, A.; Zvara, P. Pad weight testing in the evaluation of urinary incontinence. Neurourol. Urodyn. 2014, 33, 507–510. [Google Scholar] [CrossRef]
- Yi, Y.A.; Keith, C.G.; Graziano, C.E.; Davenport, M.T.; Bergeson, R.L.; Christine, B.S.; Morey, A.F. Strong correlation between standing cough test and 24-h pad weights in the evaluation of male stress urinary incontinence. Neurourol. Urodyn. 2020, 39, 319–323. [Google Scholar] [CrossRef]
- Tervonen, T.; Karjalainen, K. Periodontal disease related to diabetic status: A pilot study of the response to periodontal therapy in type 1 diabetes. J. Clin. Periodontol. 1997, 24, 505–510. [Google Scholar] [CrossRef]
- Al Edwan, G.M.; Muheilan, M.M.; Atta, O.N. Long term efficacy of extracorporeal shock wave therapy [ESWT] for treatment of refractory chronic abacterial prostatitis. Ann. Med. Surg. 2017, 14, 12–17. [Google Scholar] [CrossRef]
- Harvey, M.A. Pelvic floor exercises during and after pregnancy: A systematic review of their role in preventing pelvic floor dysfunction. J. Obstet. Gynaecol. Can. 2003, 25, 487–498. [Google Scholar] [CrossRef]
- Souders, C.P.; Eilber, K.S.; McClelland, L.; Wood, L.N.; Souders, A.R.; Steiner, V.; Anger, J.T. The Truth behind Transvaginal Mesh Litigation: Devices, Timelines, and Provider Characteristics. Female Pelvic Med. Reconstr. Surg. 2018, 24, 21–25. [Google Scholar] [CrossRef]
- Shafik, A. A study of the continence mechanism of the external urethral sphincter with identification of the voluntary urinary inhibition reflex. J. Urol. 1999, 162, 1967–1971. [Google Scholar] [CrossRef]
- Shafik, A.; Shafik, I.A. Overactive bladder inhibition in response to pelvic floor muscle exercises. World J. Urol. 2003, 20, 374–377. [Google Scholar] [CrossRef]
- Mahoney, C.; Smith, A.; Marshall, A.; Reid, F. Pelvic floor dysfunction and sensory impairment: Current evidence. Neurourol. Urodyn. 2017, 36, 550–556. [Google Scholar] [CrossRef]
- Lin, K.L.; Chou, S.H.; Long, C.Y. Effect of Er:YAG Laser for Women with Stress Urinary Incontinence. BioMed Res. Int. 2019, 2019, 7915813. [Google Scholar] [CrossRef] [Green Version]
- Liedl, B.; Goeschen, K.; Sutherland, S.E.; Roovers, J.P.; Yassouridis, A. Can surgical reconstruction of vaginal and ligamentous laxity cure overactive bladder symptoms in women with pelvic organ prolapse? BJU Int. 2019, 123, 493–510. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Parameter | Sham (Mean ± SE) | LiESWT (Mean ± SE) | Range |
|---|---|---|---|
| Physical parameter | |||
| Female age (years) | 52.8 ± 1.9 | 53.8 ± 1.5 | 20–75 |
| Height (cm) | 158.0 ± 1.6 | 158.9 ± 0.9 | |
| Weight (kg) | 59.4 ± 1.9 | 61.2 ± 1.3 | |
| BMI (kg/m2) | 23.8 ± 0.7 | 24.2 ± 0.4 | 18.5–24 |
| Waistline (cm) | 87.2 ± 2.8 | 85.6 ± 1.4 | |
| Systolic pressure (mmHg) | 124.4 ± 3.0 | 121.4 ± 2.9 | 100–120 |
| Diastolic pressure (mmHg) | 77.9 ± 2.3 | 74.5 ± 1.7 | 60–80 |
| MAP | 93.4 ± 2.3 | 90.1 ± 2.0 | 70–110 |
| Serum parameter | |||
| HbA1C (%) | 5.67 ± 0.12 | 5.63 ± 0.06 | 4–6 |
| AC sugar (mg/dL) | 101.7 ± 3.7 | 101.0 ± 1.6 | 65–109 |
| BUN (mg/dl) | 12.54 ± 0.80 | 12.35 ± 0.45 | 8–20 |
| Creatinine (mg/dL) | 0.67 ± 0.03 | 0.68 ± 0.02 | 0.44–1.03 |
| GOT(AST) (IU/L) | 22.5 ± 1.0 | 23.5 ± 1.3 | 10–42 |
| GPT(ALT) (IU/L) | 23.8 ± 2.2 | 23.9 ± 2.2 | 10–40 |
| Triglycerides (mg/dL) | 92.1 ± 12.3 | 96.9 ± 9.0 | 35–160 |
| Cholesterol (mg/dL) | 214.2 ± 8.2 | 203.7 ± 6.7 | 140–200 |
| HDL (mg/dL) | 61.5 ± 3.6 | 57.2 ± 2.2 | 29–85 |
| LDL (mg/dL) | 134.9 ± 8.3 | 124.9 ± 6.3 | 0–130 |
| Parameter | Sham (N = 15) | LiESWT (N = 45) | ||||||
|---|---|---|---|---|---|---|---|---|
| W0 | W4 | W0 | W4 | W8 | F1 | F3 | F6 | |
| Pad test (g) | 7.94 ± 2.07 | 7.29 ± 2.21 | 7.93 ± 1.32 | 2.43 ± 0.40 ++,## | 2.29 ± 0.78 ## | 1.02 ± 0.28 ## | 1.27 ± 0.54 ## | 1.18 ± 0.38 ## |
| 3-day urinary diary record | ||||||||
| Intake (mL) | 1698.7 ± 127.7 | 1703.2 ± 127.8 | 1757.6 ± 94.3 | 1822.9 ± 94.8 | 1738.2 ± 74.7 | 1678.5 ± 99.4 | 1680.2 ± 89.8 | 1785.1 ± 75.9 |
| Output (mL) | 1795.3 ± 104.6 | 1727.4 ± 126.4 | 1787.6 ± 107.7 | 1845.1 ± 99.8 | 1779.9 ± 86.7 | 1779.5 ± 104.7 | 1886.2 ± 110.4 | 1780.4 ± 70.1 |
| Average voided volume (mL) | 204.6 ± 15.1 | 221.4 ± 15.6 | 212.4 ± 8.9 | 235.5 ± 9.3 | 245.4 ± 9.2 | 245.4 ± 9.9 | 248.9 ± 8.2 # | 249.0 ± 10.2 # |
| Functional bladder capacity (mL) | 376.6 ± 30.9 | 378.4 ± 30.0 | 374.3 ± 16.8 | 393.2 ± 19.7 | 389.6 ± 18.8 | 380.3 ± 19.5 | 400.8 ± 17.6 | 398.4 ± 19.6 |
| Daytime frequency (times) | 8.86 ± 0.50 | 8.00 ± 0.38 | 8.54 ± 0.32 | 8.42 ± 0.33 | 7.98 ± 0.34 | 7.91 ± 0.30 | 8.12 ± 0.29 | 8.12 ± 0.25 |
| Nocturia (times) | 1.00 ± 0.13 | 0.81 ± 0.17 | 0.81 ± 0.10 | 0.82 ± 0.13 | 0.69 ± 0.12 | 0.59 ± 0.12 | 0.61 ± 0.09 | 0.55 ± 0.11 |
| Urgency (times) | 1.86 ± 0.46 | 1.68 ± 0.51 | 2.09 ± 0.33 | 1.32 ± 0.24 | 1.06 ± 0.22 # | 0.57 ± 0.15 ## | 0.86 ± 0.19 ## | 1.07 ± 0.21 # |
| Uroflowmetry data | ||||||||
| Voided urine volume (mL) | 367.2 ± 38.6 | 378.9 ± 34.9 | 346.4 ± 24.0 | 355.5 ± 25.8 | 394.3 ± 24.4 | 427.0 ± 23.9 # | 433.6 ± 26.4 # | 392.0 ± 24.7 |
| Maximum flow rate (mL/s) | 32.2 ± 3.3 | 33.7 ± 2.9 | 30.1 ± 1.7 | 31.2 ± 2.1 | 33.7 ± 2.4 | 38.0 ± 2.0 # | 36.3 ± 2.2 | 33.1 ± 1.9 |
| PVR (mL) | 50.7 ± 11.5 | 44.3 ± 9.7 | 53.0 ± 5.6 | 35.7 ± 4.3 | 28.3 ± 4.6 # | 27.5 ± 4.1 # | 26.7 ± 5.0 # | 33.5 ± 5.6 |
| Questionnaire score (points) | ||||||||
| OABSS | 6.57 ± 0.68 | 5.31 ± 0.78 | 6.36 ± 0.43 | 4.70 ± 0.44 | 3.65 ± 0.38 ## | 3.49 ± 0.42 ## | 3.83 ± 0.42 ## | 3.66 ± 0.38 ## |
| ICIQ-SF | 11.47 ± 1.14 | 10.08 ± 1.07 | 11.26 ± 0.59 | 7.39 ± 0.56 +,## | 5.96 ± 0.60 ## | 4.06 ± 0.45 ## | 4.73 ± 0.48 ## | 4.75 ± 0.59 ## |
| UDI-6 | 7.63 ± 0.62 | 6.77 ± 1.12 | 7.67 ± 0.48 | 4.63 ± 0.44 +,## | 3.53 ± 0.45 ## | 3.05 ± 0.37 ## | 3.06 ± 0.36 ## | 2.91 ± 0.39 ## |
| IIQ-7 | 8.38 ± 1.30 | 7.00 ± 1.49 | 8.11 ± 0.67 | 4.36 ± 0.52 +,## | 3.07 ± 0.53 ## | 2.19 ± 0.40 ## | 2.67 ± 0.45 ## | 2.52 ± 0.41 ## |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, K.-L.; Chueh, K.-S.; Lu, J.-H.; Chuang, S.-M.; Wu, B.-N.; Lee, Y.-C.; Wu, Y.-H.; Shen, M.-C.; Sun, T.-W.; Long, C.-Y.; et al. Low Intensity Extracorporeal Shock Wave Therapy as a Novel Treatment for Stress Urinary Incontinence: A Randomized-Controlled Clinical Study. Medicina 2021, 57, 947. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090947
Lin K-L, Chueh K-S, Lu J-H, Chuang S-M, Wu B-N, Lee Y-C, Wu Y-H, Shen M-C, Sun T-W, Long C-Y, et al. Low Intensity Extracorporeal Shock Wave Therapy as a Novel Treatment for Stress Urinary Incontinence: A Randomized-Controlled Clinical Study. Medicina. 2021; 57(9):947. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090947
Chicago/Turabian StyleLin, Kun-Ling, Kuang-Shun Chueh, Jian-He Lu, Shu-Mien Chuang, Bin-Nan Wu, Yung-Chin Lee, Yi-Hsuan Wu, Mei-Chen Shen, Ting-Wei Sun, Cheng-Yu Long, and et al. 2021. "Low Intensity Extracorporeal Shock Wave Therapy as a Novel Treatment for Stress Urinary Incontinence: A Randomized-Controlled Clinical Study" Medicina 57, no. 9: 947. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina57090947