
Multiple Free Flap Reconstruction of a Complex Intraoral Defect after Squamous Cell Carcinoma Excision: A Case Report

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
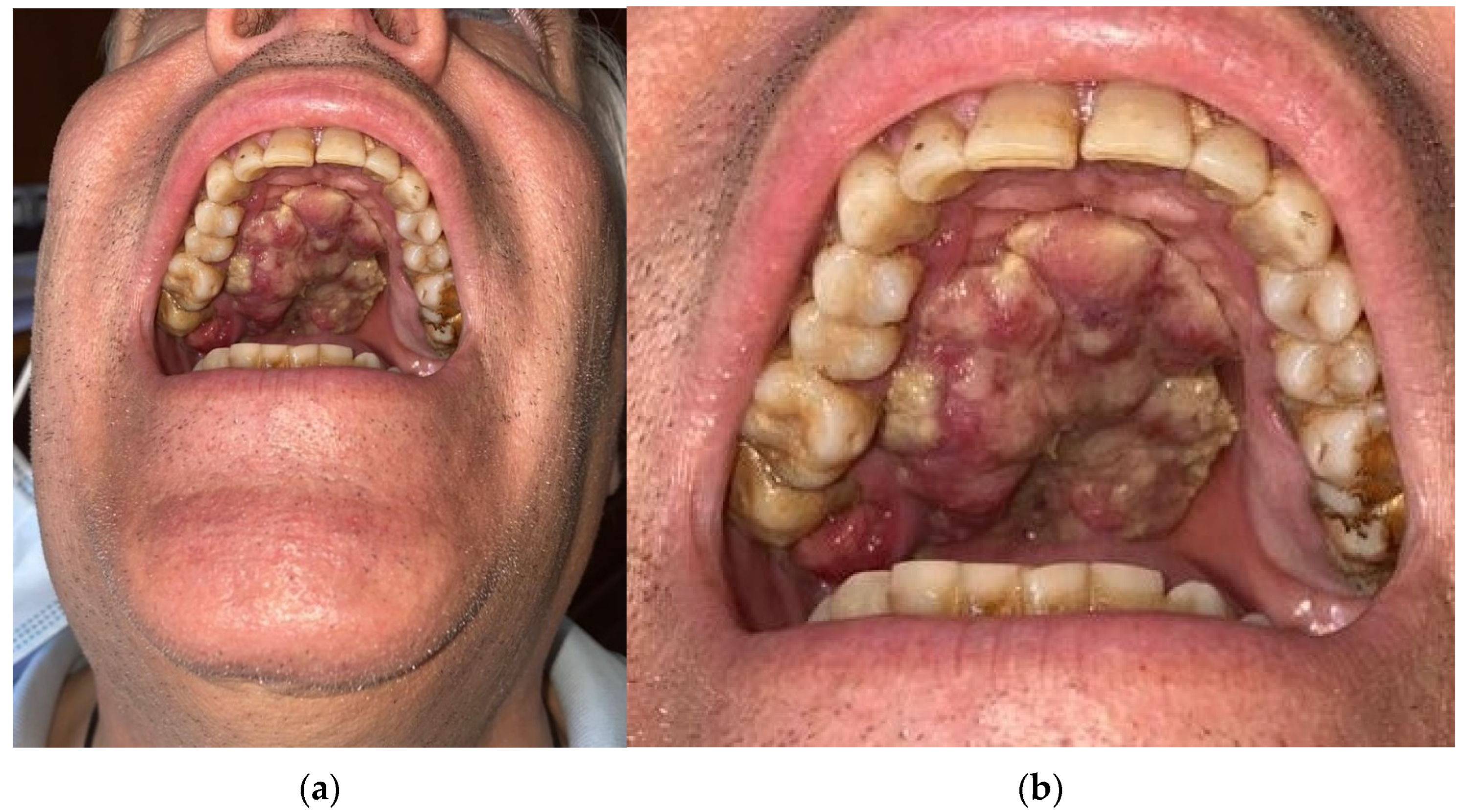
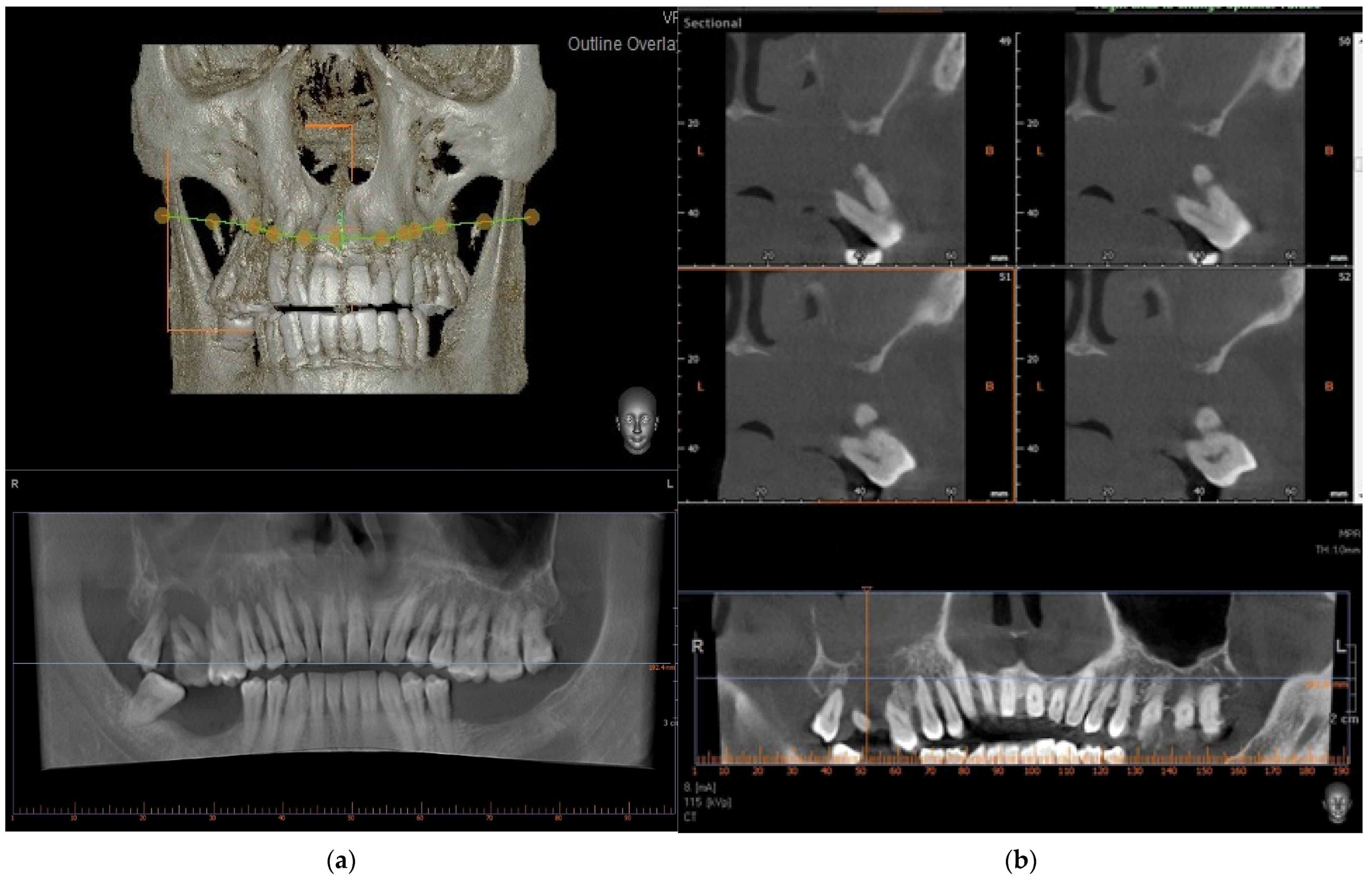
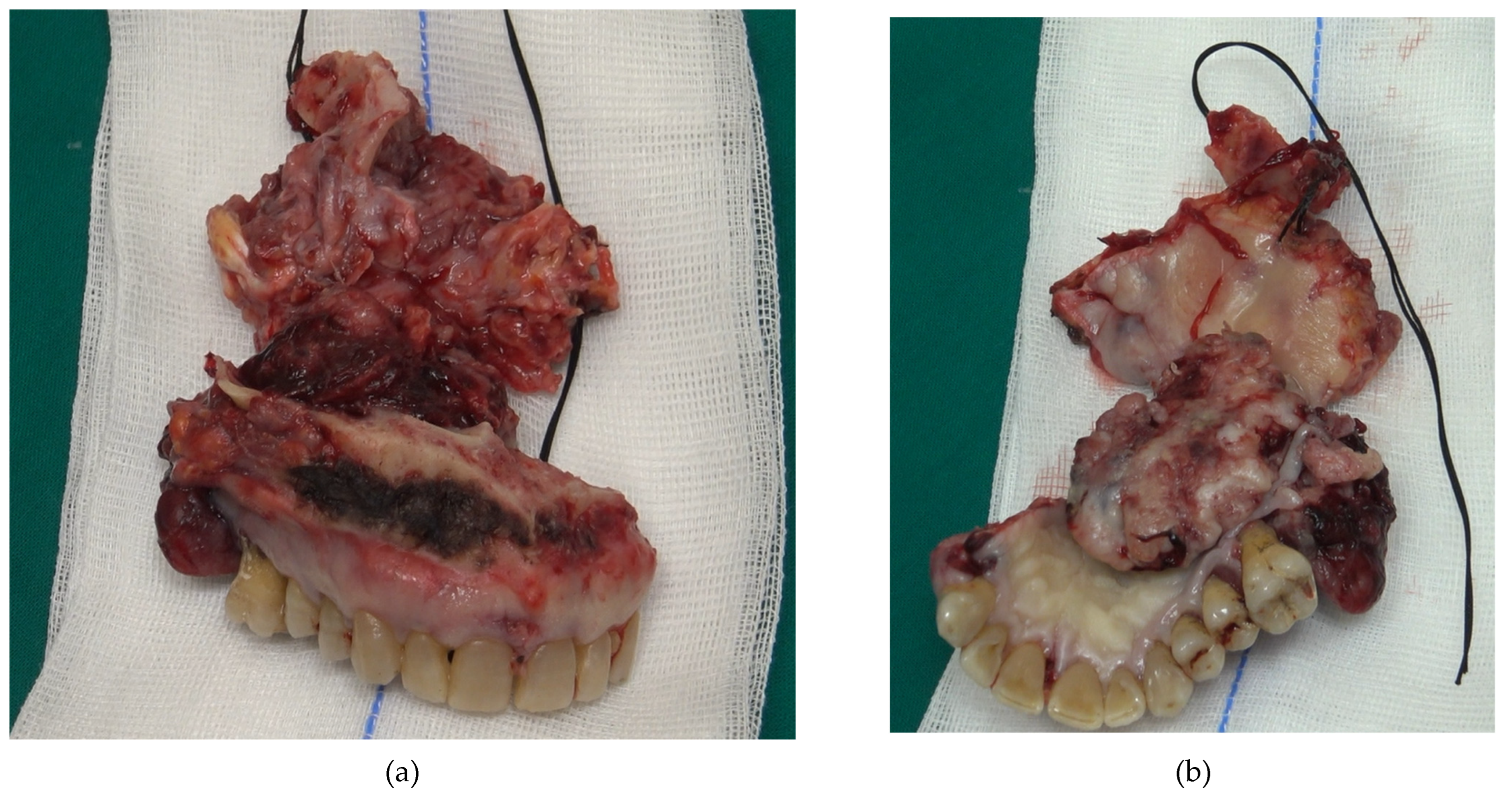
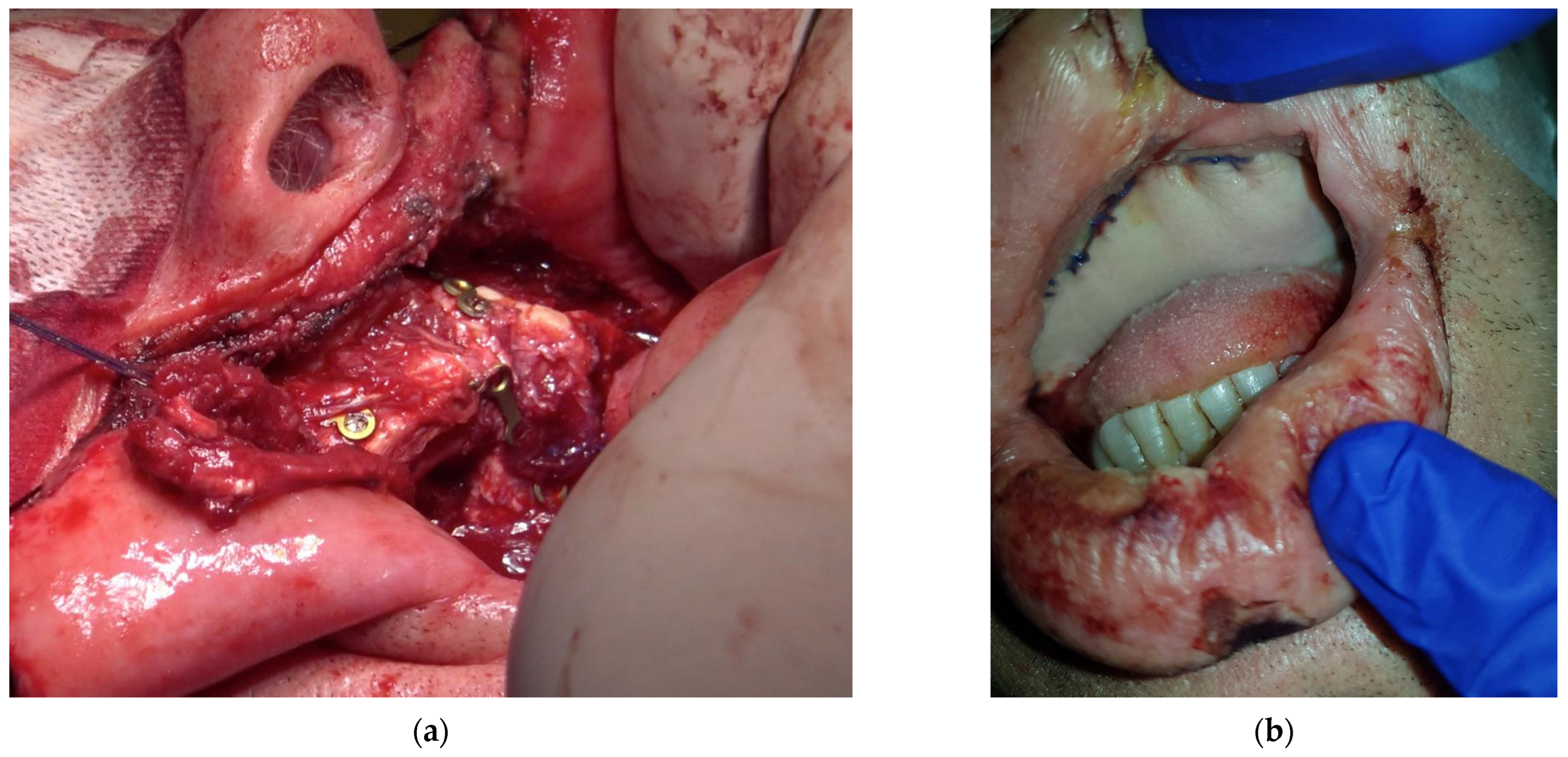
2. Case Presentation
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- D’Addazio, G.; Artese, L.; Traini, T.; Rubini, C.; Caputi, S.; Sinjari, B. Immunohistochemical study of osteopontin in oral squamous cell carcinoma allied to fractal dimension. J. Biol. Regul. Homeost. Agents 2018, 32, 1033–1038. [Google Scholar]
- Thomson, P.J. Perspectives on oral squamous cell carcinoma prevention-proliferation, position, progression and prediction. J. Oral. Pathol. Med. 2018, 47, 803–807. [Google Scholar] [CrossRef]
- Kain, J.J.; Birkeland, A.C.; Udayakumar, N.; Morlandt, A.B.; Stevens, T.M.; Carroll, W.R.; Rosenthal, E.L.; Warram, J.M. Surgical margins in oral cavity squamous cell carcinoma: Current practices and future directions. Laryngoscope 2020, 130, 128–138. [Google Scholar] [CrossRef]
- Elhousiny, M.; Miller, K.; Ariyawadana, A.; Nimmo, A. Identification of inflammatory mediators associated with metastasis of oral squamous cell carcinoma in experimental and clinical studies: Systematic review. Clin. Exp. Metastasis 2019, 36, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Oreamuno, Y.V.B. Oral Squamous Cell Carcinoma: A Case Report and Review of Literature. Int. J. Dent. Sci. 2017, 18, 61–67. [Google Scholar]
- Pollice, P.A.; Frodel, J.L. Secondary reconstruction of upper midface and orbit after total maxillectomy. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Triana, R.J.; Uglesic, V.; Virag, M.; Varga, S.G.; Knezevic, P.; Milenovic, A.; Aljinovic, N.; Murakami, C.S.; Futran, N.D. Microvascular free flap reconstructive options in patients with partial and total maxillectomy defects. Arch. Facial Plast. Surg. 2000, 2, 91–101. [Google Scholar] [CrossRef]
- Klotch, D.W.; Gump, J.; Kuhn, L. Reconstruction of mandibular defects in irradiated patients. Am. J. Surg. 1990, 160, 396–398. [Google Scholar] [CrossRef]
- Urken, M.L.; Bridger, A.G.; Zur, K.B.; Genden, E.M. The scapular osteofasciocutaneous flap: A 12-year experience. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 862–869. [Google Scholar]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Sanderson, R.J.; Ironside, J.A. Squamous cell carcinomas of the head and neck. BMJ 2002, 325, 822–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, B.; Ferrari, S.; Poli, T.; Bertolini, F.; Raho, T.; Sesenna, E. Oromandibular reconstruction with simultaneous free flaps: Experience on 10 cases. Acta Otorhinolaryngol. Ital. 2003, 4, 281–290. [Google Scholar]
- Stalder, M.W.; Mundinger, G.S.; Bartow, M.; Pharo, A.; Patterson, C.; Sharma, S.; Aslam, R.; St Hilaire, H. Single Versus Simultaneous Double Free Flaps for Head and Neck Reconstruction: Comparison of Flap Outcomes and Donor-Site Morbidity. Ann. Plast. Surg. 2019, 82, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Pogrel, M.A.; Podlesh, S.; Anthony, J.P.; Alexander, J. A comparison of vascularized and nonvascularized bone grafts for reconstruction of mandibular continuity defects. J. Oral Maxillofac. Surg. 1997, 55, 1200–1206. [Google Scholar] [CrossRef]
- Gabr, E.; Kobayashi, M.R.; Salibian, A.H.; Armstrong, W.B.; Sundine, M.; Calvert, J.W.; Evans, G.R. Mandibular reconstruction: Are two flaps better than one? Ann. Plast. Surg. 2004, 52, 31–35. [Google Scholar] [CrossRef]
- Andrades, P.; Bohannon, I.A.; Baranano, C.F.; Wax, M.K.; Rosenthal, E. Indications and outcomes of double free flaps in head and neck reconstruction. Microsurgery 2009, 29, 171–177. [Google Scholar] [CrossRef]
- Boyd, J.B.; Mulholland, R.S.; Davidson, J.; Gullane, P.J.; Rotstein, L.E.; Brown, D.H.; Freeman, J.E.; Irish, J.C. The free flap and plate in oromandibular reconstruction: Long-term review and indications. Plast. Reconstr. Surg. 1995, 95, 1018–1028. [Google Scholar] [CrossRef]
- Osborn, T.M.; Helal, D.; Mehra, P. Iliac crest bone grafting for mandibular reconstruction: 10-year experience outcomes. J. Oral Biol. Craniofac. Res. 2018, 8, 25–29. [Google Scholar] [CrossRef] [Green Version]
- De Vicente, J.C.; Rodríguez-Santamarta, T.; Rosado, P.; Peña, I.; de Villalaín, L. Survival after free flap reconstruction in patients with advanced oral squamous cell carcinoma. J. Oral Maxillofac. Surg. 2012, 70, 453–459. [Google Scholar] [CrossRef]
- Meglioli, M.; Naveau, A.; Macaluso, G.M.; Catros, S. 3D printed bone models in oral and cranio-maxillofacial surgery: A systematic review. 3D Print Med. 2020, 6, 30. [Google Scholar] [CrossRef]
- Cordeiro, P.G.; Disa, J.J.; Hidalgo, D.A.; Hu, Q.Y. Reconstruction of the mandible with osseous free flaps: A 10-year experience with 150 consecutive patients. Plast. Reconstr. Surg. 1999, 104, 1314–1320. [Google Scholar] [CrossRef]
- Jacek, B.; Maciej, P.; Tomasz, P.; Agata, B.; Wiesław, K.; Radosław, W.; Filip, G. 3D printed models in mandibular reconstruction with bony free flaps. J. Mater. Sci. Mater. Med. 2018, 29, 23. [Google Scholar] [CrossRef] [Green Version]
- Kumar, B.P.; Venkatesh, V.; Kumar, K.A.; Yadav, B.Y.; Mohan, S.R. Mandibular Reconstruction: Overview. J. Maxillofac. Oral Surg. 2016, 15, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Alfouzan, A.F. Review of surgical resection and reconstruction in head and neck cancer. Traditional versus current concepts. Saudi Med. J. 2018, 39, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Frodel, J.L., Jr.; Funk, G.F.; Capper, D.T.; Fridrich, K.L.; Blumer, J.R.; Haller, J.R.; Hoffman, H.T. Osseointegrated implants: A comparative study of bone thickness in four vascularized bone flaps. Plast. Reconstr. Surg. 1993, 92, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Moscoso, J.F.; Keller, J.; Genden, E.; Weinberg, H.; Biller, H.F.; Buchbinder, D.; Urken, M.L. Vascularized bone flaps in oromandibular reconstruction. A comparative anatomic study of bone stock from various donor sites to assess suitability for enosseous dental implants. Arch. Otolaryngol. Head Neck Surg. 1994, 120, 36–43. [Google Scholar] [CrossRef]
- Aksoyler, D.; Losco, L.; Bolletta, A.; Ercan, A.; Chen, S.H.; Velazquez-Mujica, J.; Tang, Y.B.; Chen, H.C. Three salvage strategies in microvascular fibula osteocutaneous flap for mandible reconstruction with vascular compromise and establishment of an algorithm. Microsurgery 2021, 41, 223–232. [Google Scholar] [CrossRef]
- Zhang, S.; Li, P.; Liu, C.; Wu, H.; Gong, Z. Application of Suprafascially Harvested Anterolateral Thigh Perforator Flap for the Reconstruction of Oral and Maxillofacial Defects. J. Craniofac. Surg. 2020, 31, 673–676. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Steps | ||
|---|---|---|
| Timing (Hours) | Equipe 1 | Equipe 2 |
| 0–1 | General anesthesia and tracheotomy | |
| 1–3 | Maxillectomy | Fibula free flap |
| 3–4 | Neck block dissection of lymph nodes | Free radial forearm flap |
| 4–7 | Bone graft adaptation and osteosynthesis screw fixation | Donor site suturing |
| 7–8 | Soft tissue reconstruction | |
| 8–10 | Vascular micro-anastomosis | |
| 10–11 | General sutures | |
| Selection Criteria for Bone Reconstruction | Iliac | Scapula | Fibula |
|---|---|---|---|
| Age (Young) | +++ | ++ | ++ |
| Extension (>14 cm) | ++ | +++ | +++ |
| Localization donor site | +++ | + | +++ |
| Bone quality | +++ | ++ | +++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santilli, M.; D’Addazio, G.; Rexhepi, I.; Sinjari, B.; Filippini, A. Multiple Free Flap Reconstruction of a Complex Intraoral Defect after Squamous Cell Carcinoma Excision: A Case Report. Medicina 2022, 58, 54. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010054
Santilli M, D’Addazio G, Rexhepi I, Sinjari B, Filippini A. Multiple Free Flap Reconstruction of a Complex Intraoral Defect after Squamous Cell Carcinoma Excision: A Case Report. Medicina. 2022; 58(1):54. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010054
Chicago/Turabian StyleSantilli, Manlio, Gianmaria D’Addazio, Imena Rexhepi, Bruna Sinjari, and Arnaldo Filippini. 2022. "Multiple Free Flap Reconstruction of a Complex Intraoral Defect after Squamous Cell Carcinoma Excision: A Case Report" Medicina 58, no. 1: 54. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010054