
Therapeutic Exercise and Conservative Injection Treatment for Early Knee Osteoarthritis in Athletes: A Scoping Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
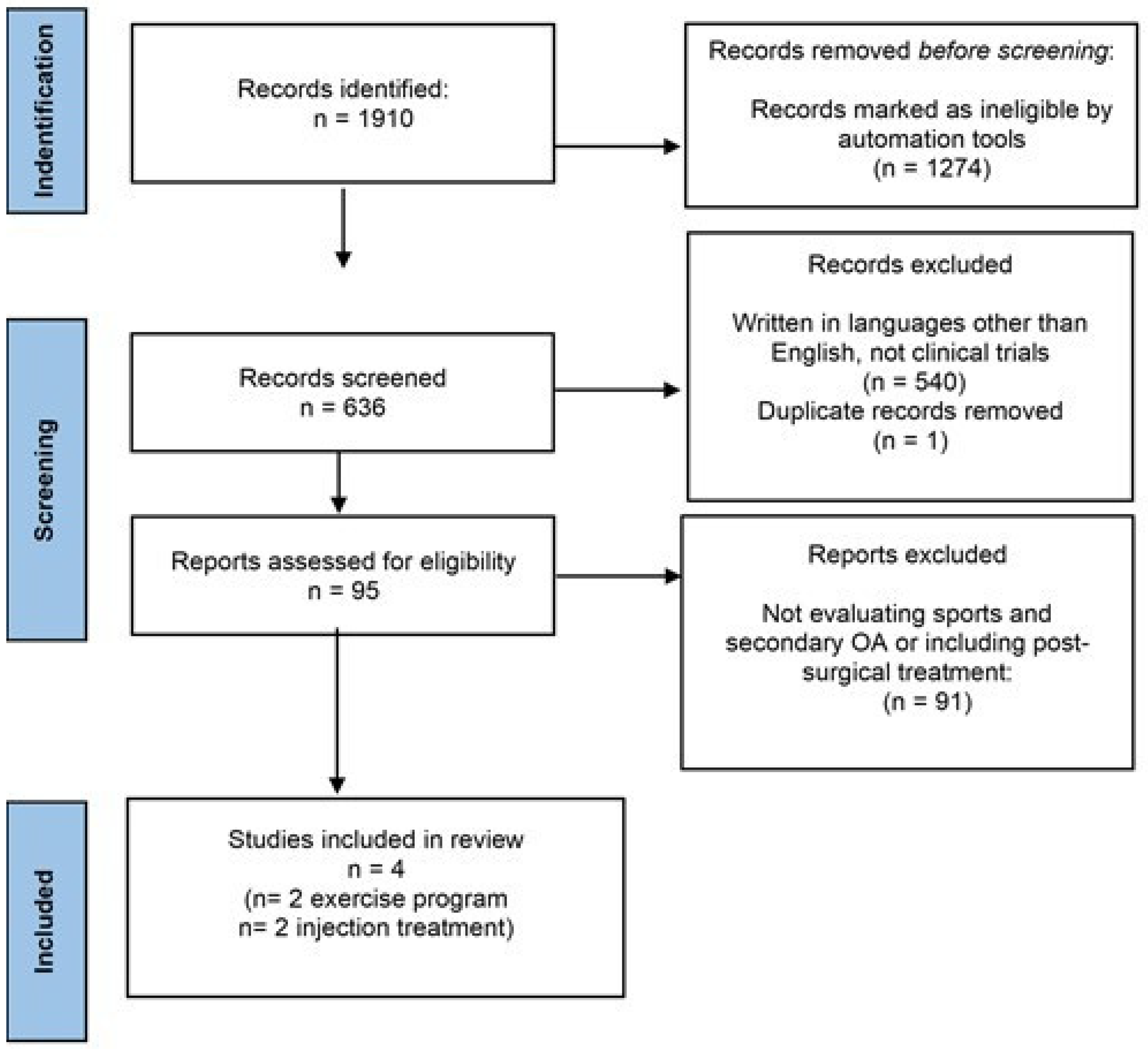
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
3. Results
3.1. Selected Studies
3.2. Therapeutic Exercise
3.3. Injection Treatment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wang, X.-Q.; Huang, L.-Y.; Liu, Y.; Li, J.-X.; Wu, X.; Li, H.-P.; Wang, L. Effects of tai chi program on neuromuscular function for patients with knee osteoarthritis: Study protocol for a randomized controlled trial. Trials 2013, 14, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Adams, T.; Band-Entrup, D.; Kuhn, S.; Legere, L.; Mace, K.; Paggi, A.; Penney, M. Physical Therapy Management of Knee Osteoarthritis in the Middle-aged Athlete. Sports Med. Arthrosc. Rev. 2013, 21, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felson, D.T.; Naimark, A.; Anderson, J.; Kazis, L.; Castelli, W.; Meenan, R.F. The prevalence of knee osteoarthritis in the elderly. the framingham osteoarthritis study. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1987, 30, 914–918. [Google Scholar] [CrossRef]
- Lau, E.C.; Cooper, C.; Lam, D.; Chan, V.N.H.; Tsang, K.K.; Sham, A. Factors associated with osteoarthritis of the hip and knee in Hong Kong Chinese: Obesity, joint injury, and occupational activities. Am. J. Epidemiol. 2000, 152, 855–862. [Google Scholar] [CrossRef] [Green Version]
- Palazzo, C.; Ravaud, J.F.; Papelard, A.; Ravaud, P.; Poiraudeau, S. The burden of musculoskeletal conditions. PLoS ONE 2014, 9, e90633. [Google Scholar] [CrossRef]
- Amoako, A.O.; Pujalte, G.G.A. Osteoarthritis in Young, Active, and Athletic Individuals. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2014, 7, 27–32. [Google Scholar] [CrossRef] [Green Version]
- Luyten, F.P.; Denti, M.; Filardo, G.; Kon, E.; Engebretsen, L. Definition and classification of early osteoarthritis of the knee. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Vignon, É.; Valat, J.-P.; Rossignol, M.; Avouac, B.; Rozenberg, S.; Thoumie, P.; Avouac, J.; Nordin, M.; Hilliquin, P. Osteoarthritis of the knee and hip and activity: A systematic international review and synthesis (OASIS). Jt. Bone Spine 2006, 73, 442–455. [Google Scholar] [CrossRef]
- Kujala, U.M.; Kaprio, J.; Sarno, S. Osteoarthritis of weight bearing joints of lower limbs in former elite male athletes. BMJ 1994, 308, 231–234. [Google Scholar] [CrossRef]
- Tran, G.; Smith, T.; Grice, A.; Kingsbury, S.R.; McCrory, P.; Conaghan, P.G. Does sports participation (including level of performance and previous injury) increase risk of osteoarthritis? A systematic review and meta-analysis. Br. J. Sports Med. 2016, 50, 1459–1466. [Google Scholar] [CrossRef] [Green Version]
- Majewski, M.; Susanne, H.; Klaus, S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006, 13, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Tibbetts, A.S.; Covassin, T.; Cheng, G.; Nayar, S.; Heiden, E. Epidemiology of Overuse and Acute Injuries among Competitive Collegiate Athletes. J. Athl. Train. 2012, 47, 198–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vannini, F.; Spalding, T.; Andriolo, L.; Berruto, M.; Denti, M.; Espregueira-Mendes, J.; Menetrey, J.; Peretti, G.; Seil, R.; Filardo, G. Sport and early osteoarthritis: The role of sport in aetiology, progression and treatment of knee osteoarthritis. Knee Surgery Sports Traumatol. Arthrosc. 2016, 24, 1786–1796. [Google Scholar] [CrossRef]
- Driban, J.B.; Hootman, J.M.; Sitler, M.R.; Harris, K.; Cattano, N.M. Is Participation in Certain Sports Associated With Knee Osteoarthritis? A Systematic Review. J. Athl. Train. 2017, 52, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.C.; Hubbard-Turner, T.; Wikstrom, E.A.; Palmieri-Smith, R.M. Epidemiology of Posttraumatic Osteoarthritis. J. Athl. Train. 2017, 52, 491–496. [Google Scholar] [CrossRef] [Green Version]
- Buckwalter, J.A.; Martin, J.A.; Brown, T.D. Perspectives on chondrocyte mechanobiology and osteoarthritis. Biorheology 2006, 43, 603–609. [Google Scholar] [PubMed]
- Yang, G.-Y.; Sabag, A.; Hao, W.-L.; Zhang, L.-N.; Jia, M.-X.; Dai, N.; Zhang, H.; Ayati, Z.; Cheng, Y.-J.; Zhang, C.-H.; et al. Tai Chi for health and well-being: A bibliometric analysis of published clinical studies between 2010 and 2020. Complement. Ther. Med. 2021, 60, 102748. [Google Scholar] [CrossRef]
- Bijlsma, J.W.J.; Berenbaum, F.; Lafeber, F.P.J.G. Osteoarthritis: An update with relevance for clinical practice. Lancet 2011, 377, 2115–2126. [Google Scholar] [CrossRef]
- Nelson, A.E.; Allen, K.D.; Golightly, Y.; Goode, A.P.; Jordan, J.M. A systematic review of recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the U.S. Bone and Joint Initiative. Semin. Arthritis Rheum. 2014, 43, 701–712. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, S.; Doherty, M. Lifestyle changes in the management of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2001, 15, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, L.; Hagen, K.B.; Bijlsma, J.W.J.; Andreassen, O.; Christensen, P.; Conaghan, P.; Doherty, M.; Geenen, R.; Hammond, A.; Kjeken, I.; et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann. Rheum. Dis. 2013, 72, 1125–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazi, C.; Nyland, J.; Whaley, R.; Rogers, T.; Wera, J.; Henzman, C. Social cognitive or learning theory use to improve self-efficacy in musculoskeletal rehabilitation: A systematic review and meta-analysis. Physiother. Theory Pract. 2018, 34, 495–504. [Google Scholar] [CrossRef]
- Letizia Mauro, G.; Scaturro, D.; Gimigliano, F.; Paoletta, M.; Liguori, S.; Toro, G.; Iolascon, G.; Moretti, A. Physical agent modalities in early osteoarthritis: A scoping review. Medicine 2021, 57, 1165. [Google Scholar] [CrossRef]
- Cudejko, T.; Van Der Esch, M.; Schrijvers, J.; Richards, R.; Noort, J.C.V.D.; Wrigley, T.; Van Der Leeden, M.; Roorda, L.D.; Lems, W.; Harlaar, J.; et al. The immediate effect of a soft knee brace on dynamic knee instability in persons with knee osteoarthritis. Rheumatology 2018, 57, 1735–1742. [Google Scholar] [CrossRef] [Green Version]
- Mao, H.-Y.; Hu, M.-T.; Yen, Y.-Y.; Lan, S.-J.; Lee, S.-D. Kinesio Taping Relieves Pain and Improves Isokinetic Not Isometric Muscle Strength in Patients with Knee Osteoarthritis—A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10440. [Google Scholar] [CrossRef]
- Arden, N.K.; Perry, T.A.; Bannuru, R.R.; Bruyère, O.; Cooper, C.; Haugen, I.K.; Hochberg, M.C.; McAlindon, T.E.; Mobasheri, A.; Reginster, J.-Y. Non-surgical management of knee osteoarthritis: Comparison of ESCEO and OARSI 2019 guidelines. Nat. Rev. Rheumatol. 2021, 17, 59–66. [Google Scholar] [CrossRef]
- Bruyère, O.; Honvo, G.; Veronese, N.; Arden, N.K.; Branco, J.; Curtis, E.; Al-Daghri, N.M.; Herrero-Beaumont, G.; Martel-Pelletier, J.; Pelletier, J.-P.; et al. An updated algorithm recommendation for the management of knee osteoarthritis from the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Semin. Arthritis Rheum. 2019, 49, 337–350. [Google Scholar] [CrossRef]
- Van Ginckel, A.; Baelde, N.; Almqvist, K.F.; Roosen, P.; McNair, P.; Witvrouw, E. Functional adaptation of knee cartilage in asymptomatic female novice runners compared to sedentary controls. A longitudinal analysis using delayed Gadolinium Enhanced Magnetic Resonance Imaging of Cartilage (dGEMRIC). Osteoarthr. Cartil. 2010, 18, 1564–1569. [Google Scholar] [CrossRef]
- Willy, R.W.; Meardon, S.A.; Schmidt, A.; Blaylock, N.R.; Hadding, S.A.; Willson, J. Changes in tibiofemoral contact forces during running in response to in-field gait retraining. J. Sports Sci. 2016, 34, 1602–1611. [Google Scholar] [CrossRef]
- Tamburrino, P.; Castellacci, E. Intra-articular injections of HYADD4-G in male professional soccer players with traumatic or degenerative knee chondropathy. A pilot, prospective study. J. Sports Med. Phys. Fit. 2016, 56, 1534–1539. [Google Scholar]
- Papalia, R.; Zampogna, B.; Russo, F.; Vasta, S.; Tirindelli, M.C.; Nobile, C.; Di Martino, A.C.; Vadala, G.; Denaro, V. Comparing hibryd hyaluronic acid with prp in end career athletes with degenerative cartilage lesions of the knee. J. Biol. Regul. Homeost. Agents 2016, 30, 17–23. [Google Scholar]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [Green Version]
- Magnusson, S.P.; Hansen, M.; Langberg, H.; Miller, B.; Haraldsson, B.; Westh, E.K.; Koskinen, S.; Aagaard, P.; Kjaer, M. The adaptability of tendon to loading differs in men and women. Int. J. Exp. Pathol. 2007, 88, 237–240. [Google Scholar] [CrossRef]
- Carter, D.R.; Beaupré, G.S.; Wong, M.; Smith, R.L.; Andriacchi, T.P.; Schurman, D.J. The Mechanobiology of Articular Cartilage Development and Degeneration. Clin. Orthop. Relat. Res. 2004, 427S, S69–S77. [Google Scholar] [CrossRef]
- Smith, J. Exercise as an Adjuvant to Cartilage Regeneration Therapy. Int. J. Mol. Sci. 2020, 21, 9471. [Google Scholar] [CrossRef] [PubMed]
- Miyaguchi, M.; Kobayashi, A.; Kadoya, Y.; Ohashi, H.; Yamano, Y.; Takaoka, K. Biochemical change in joint fluid after isometric quadriceps exercise for patients with osteoarthritis of the knee. Osteoarthr. Cartil. 2003, 11, 252–259. [Google Scholar] [CrossRef] [Green Version]
- Sharma, L. Osteoarthritis of the knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Bricca, A.; Juhl, C.; Grodzinsky, A.; Roos, E. Impact of a daily exercise dose on knee joint cartilage—A systematic review and meta-analysis of randomized controlled trials in healthy animals. Osteoarthr. Cartil. 2017, 25, 1223–1237. [Google Scholar] [CrossRef]
- Iijima, H.; Aoyama, T.; Ito, A.; Tajino, J.; Yamaguchi, S.; Nagai, M.; Kiyan, W.; Zhang, X.; Kuroki, H. Exercise intervention increases expression of bone morphogenetic proteins and prevents the progression of cartilage-subchondral bone lesions in a post-traumatic rat knee model. Osteoarthr. Cartil. 2016, 24, 1092–1102. [Google Scholar] [CrossRef] [Green Version]
- Assis, L.; Milares, L.; Almeida, T.; Tim, C.; Magri, A.; Fernandes, K.; Medalha, C.; Renno, A.M. Aerobic exercise training and low-level laser therapy modulate inflammatory response and degenerative process in an experimental model of knee osteoarthritis in rats. Osteoarthr. Cartil. 2015, 24, 169–177. [Google Scholar] [CrossRef] [Green Version]
- Castrogiovanni, P.; Di Rosa, M.; Ravalli, S.; Castorina, A.; Guglielmino, C.; Imbesi, R.; Vecchio, M.; Drago, F.; Szychlinska, M.A.; Musumeci, G. Moderate Physical Activity as a Prevention Method for Knee Osteoarthritis and the Role of Synoviocytes as Biological Key. Int. J. Mol. Sci. 2019, 20, 511. [Google Scholar] [CrossRef] [Green Version]
- Spector, T.D.; Harris, P.A.; Hart, D.J.; Cicuttini, F.M.; Nandra, D.; Etherington, J.; Wolman, R.L.; Doyle, D.V. Risk of osteoarthritis associated with long-term weight-bearing sports: A radiologic survey of the hips and knees in female ex-athletes and population controls. Arthritis Rheum. 1996, 39, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-T.; Burton-Wurster, N.; Lust, G.; Bank, R.A.; Tekoppele, J.M. Compositional and metabolic changes in damaged cartilage are peak-stress, stress-rate, and loading-duration dependent. J. Orthop. Res. 1999, 17, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Bernetti, A.; Agostini, F.; Alviti, F.; Giordan, N.; Martella, F.; Santilli, V.; Paoloni, M.; Mangone, M. New Viscoelastic Hydrogel Hymovis MO.RE. Single Intra-articular Injection for the Treatment of Knee Osteoarthritis in Sportsmen: Safety and Efficacy Study Results. Front. Pharmacol. 2021, 12, 1097. [Google Scholar] [CrossRef] [PubMed]
- Waddell, D.D.; Bert, J.M. The Use of Hyaluronan After Arthroscopic Surgery of the Knee. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 105–111. [Google Scholar] [CrossRef]
- Henrotin, Y.; Bannuru, R.; Malaise, M.; Ea, H.-K.; Confavreux, C.; Bentin, J.; Urbin-Choffray, D.; Conrozier, T.; Brasseur, J.-P.; Thomas, P.; et al. Hyaluronan derivative HYMOVIS® increases cartilage volume and Type II collagen turnover in osteoarthritic knee: Data from MOKHA study. BMC Musculoskelet. Disord. 2019, 20, 293. [Google Scholar] [CrossRef]
- De Sire, A.; Marinaro, M.N.; Curci, C.; Invernizzi, M.; Ammendolia, A. Role of Physical Exercise and Nutraceuticals in Modulating Molecular Pathways of Osteoarthritis. IJMS 2021, 22, 5722. [Google Scholar] [CrossRef]
- Russo, F.; D’Este, M.; Vadalà, G.; Cattani, C.; Papalia, R.; Alini, M.; Denaro, V. Platelet Rich Plasma and Hyaluronic Acid Blend for the Treatment of Osteoarthritis: Rheological and Biological Evaluation. PLoS ONE 2016, 11, e0157048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connell, B.; Wragg, N.; Wilson, S.L. The use of PRP injections in the management of knee osteoarthritis. Cell Tissue Res. 2019, 376, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van Der Esch, M.; Simic, M.; Bennell, K. Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br. J. Sports Med. 2015, 49, 1554–1557. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.A.; Glass, N.A.; Torner, J.; Yang, M.; Felson, D.; Sharma, L.; Nevitt, M.; Lewis, C. Quadriceps weakness predicts risk for knee joint space narrowing in women in the MOST cohort. Osteoarthr. Cartil. 2010, 18, 769–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whittaker, J.L.; Truong, L.K.; Dhiman, K.; Beck, C. Osteoarthritis year in review 2020: Rehabilitation and outcomes. Osteoarthr. Cartil. 2020, 29, 190–207. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors (Publication Year) | Study Design | N (M/F) Mean (Years) | Sport | Intervention | Outcomes | Evaluation Times | Main Conclusions |
|---|---|---|---|---|---|---|---|
| Papalia et al., (2016) | RCT | 47 (M) 37.2 (range 34–39) | Soccer | 3 i.a. injections of HHA (3.2% 64 mg/2 mL, 32 mg High-MW 1100–1400 kDa + 32 mg Low-MW 80–100 kDa) at one week interval or 3 i.a. injections of 5.5 mL PRP | VAS, IKDC, KOOS | Baseline, 3, 6 and 12 months | Both treatments showed to be effective in relieving patients’ symptoms |
| Tamburrino and Castellacci (2016) | Single arm clinical trial | 30 (M) 30.7 (range 17–39) | Soccer | 2 i.a. injections of HYADD4-G (3 mL of 8 mg/mL) at one-week interval | VAS, KOOS | Baseline, 1, 3 and 6 months | Significant improvement on symptoms, ADL performance, KOOS and VAS (p < 0.05) |
| Van Ginckel et al., (2010) | Longitudinal | 19 (F) 25.5 (range 22–34) | Running | 10-week STR program | MRI dGEMRIC index | Baseline and at the end of the program | Significant positive change of the median dGEMRIC index compared to sedentary controls (+11.66 ms (95% CI: 25.29, 44.43) vs. 9.56 ms (95% CI:29.55, 5.83), p = 0.006) and with increasing physical activity (p = 0.014) |
| Willy et al., (2016) | RCT | 30 (16/14) 20.99 years (range 18–35) | Running | In-filed running retraining program using mobile biofeedback | Derived peak and cumulative tibiofemoral joint contact force estimated by gait analysis | Baseline, at the end of the program, 1 month | 7.5% increase in step rate during running with a significant reduction in tibiofemoral and medial tibiofemoral joint contact forces per stance phase (9.1% and 8.1%, respectively) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tognolo, L.; Maccarone, M.C.; De Trane, S.; Scanu, A.; Masiero, S.; Fiore, P. Therapeutic Exercise and Conservative Injection Treatment for Early Knee Osteoarthritis in Athletes: A Scoping Review. Medicina 2022, 58, 69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010069
Tognolo L, Maccarone MC, De Trane S, Scanu A, Masiero S, Fiore P. Therapeutic Exercise and Conservative Injection Treatment for Early Knee Osteoarthritis in Athletes: A Scoping Review. Medicina. 2022; 58(1):69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010069
Chicago/Turabian StyleTognolo, Lucrezia, Maria Chiara Maccarone, Stefania De Trane, Anna Scanu, Stefano Masiero, and Pietro Fiore. 2022. "Therapeutic Exercise and Conservative Injection Treatment for Early Knee Osteoarthritis in Athletes: A Scoping Review" Medicina 58, no. 1: 69. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010069