
Genetic Counseling and Management: The First Study to Report NIPT Findings in a Romanian Population

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. Genetic Counseling
2.3. NIPT: NIFTY and NIPS Tests
2.4. Cell Culture
2.5. Cytogenetics
2.6. QF-PCR Assay
2.7. Array CGH
2.8. Data Analysis
3. Results
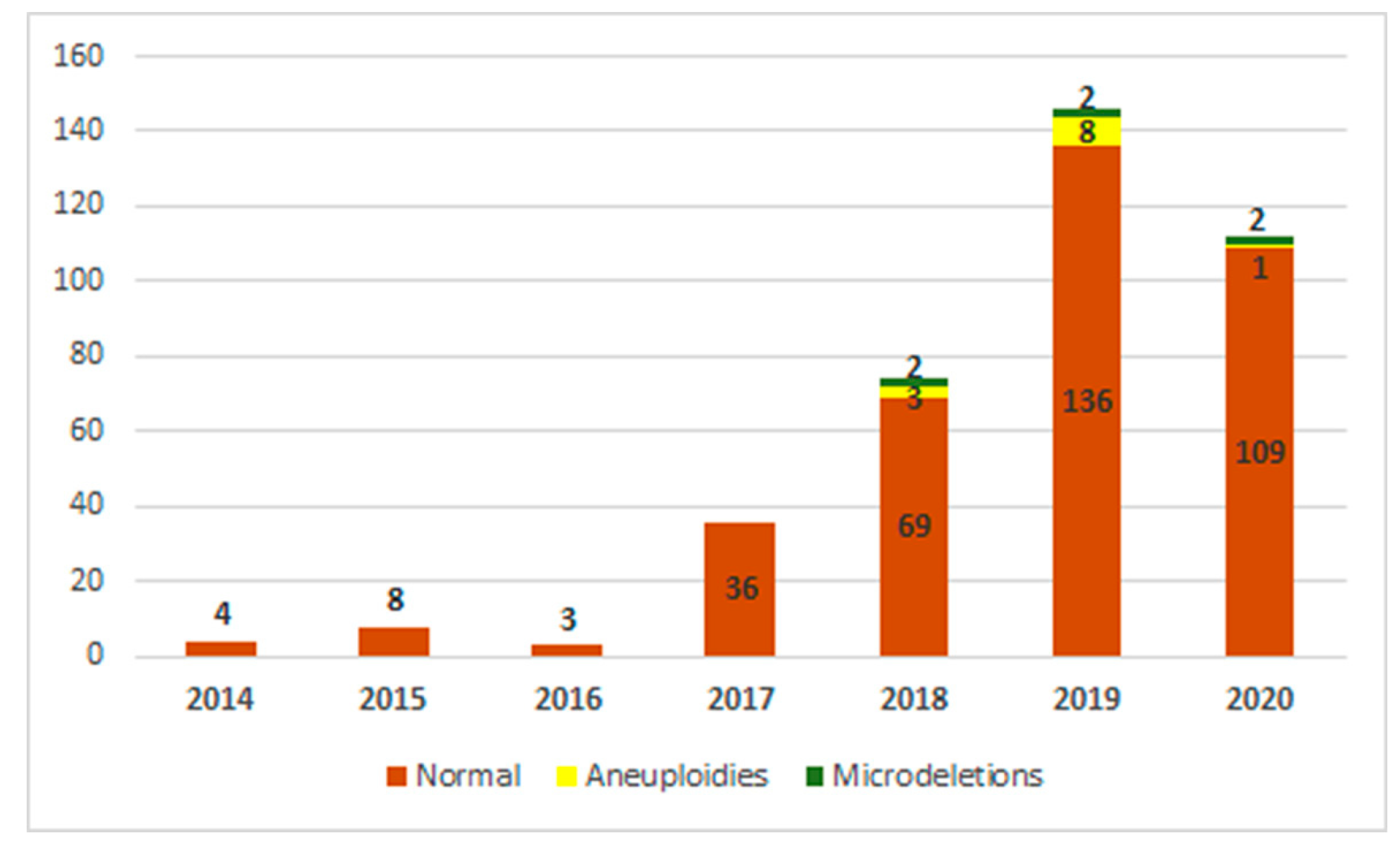
3.1. Distribution of Cases by Years, Depending on the Identified Anomalies
3.2. Analysis Duration for the NIPT
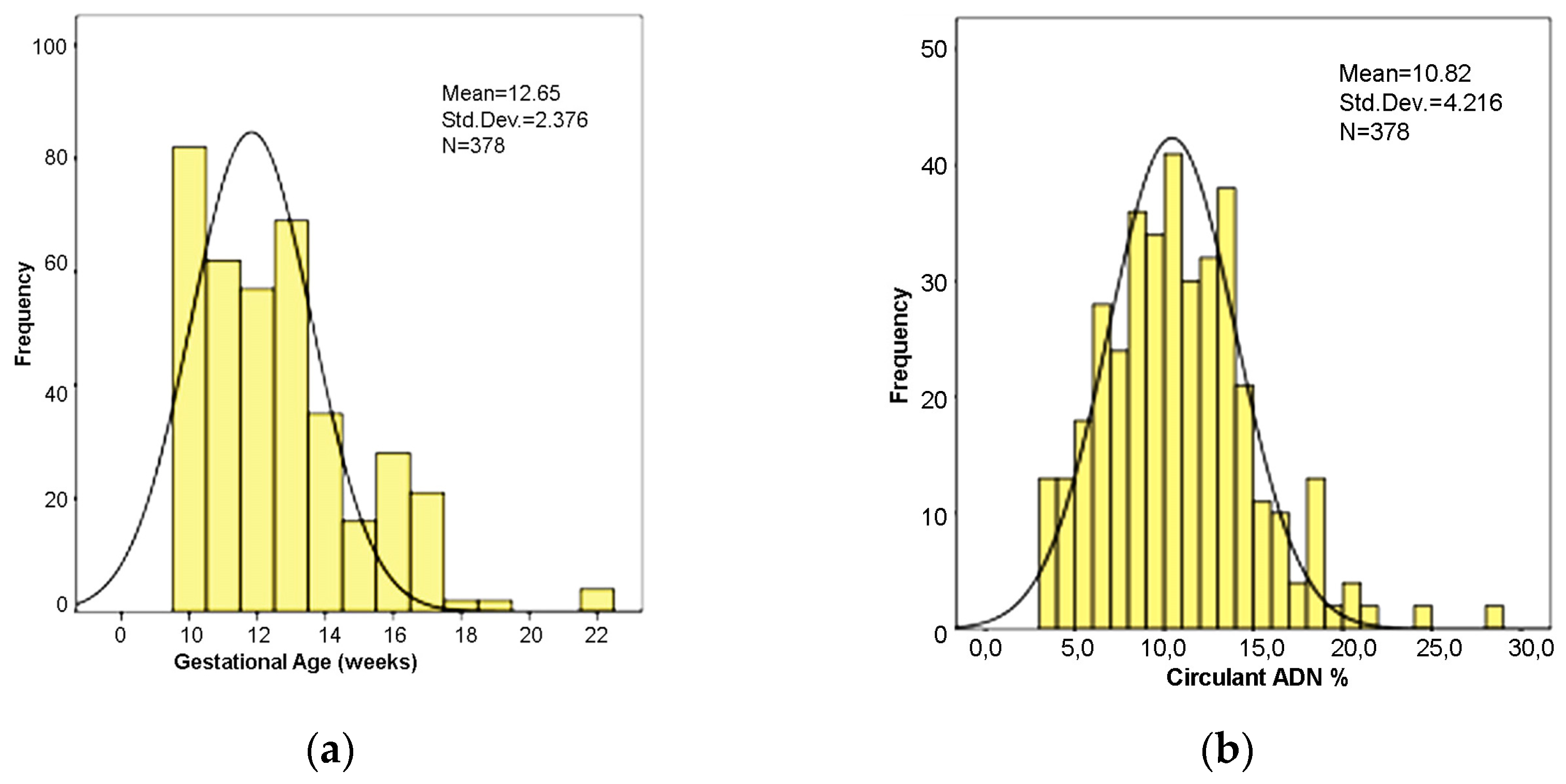
3.3. Gestational Age at the Time of NIPT
3.4. Fetal Fraction
3.5. Sex of the Fetus
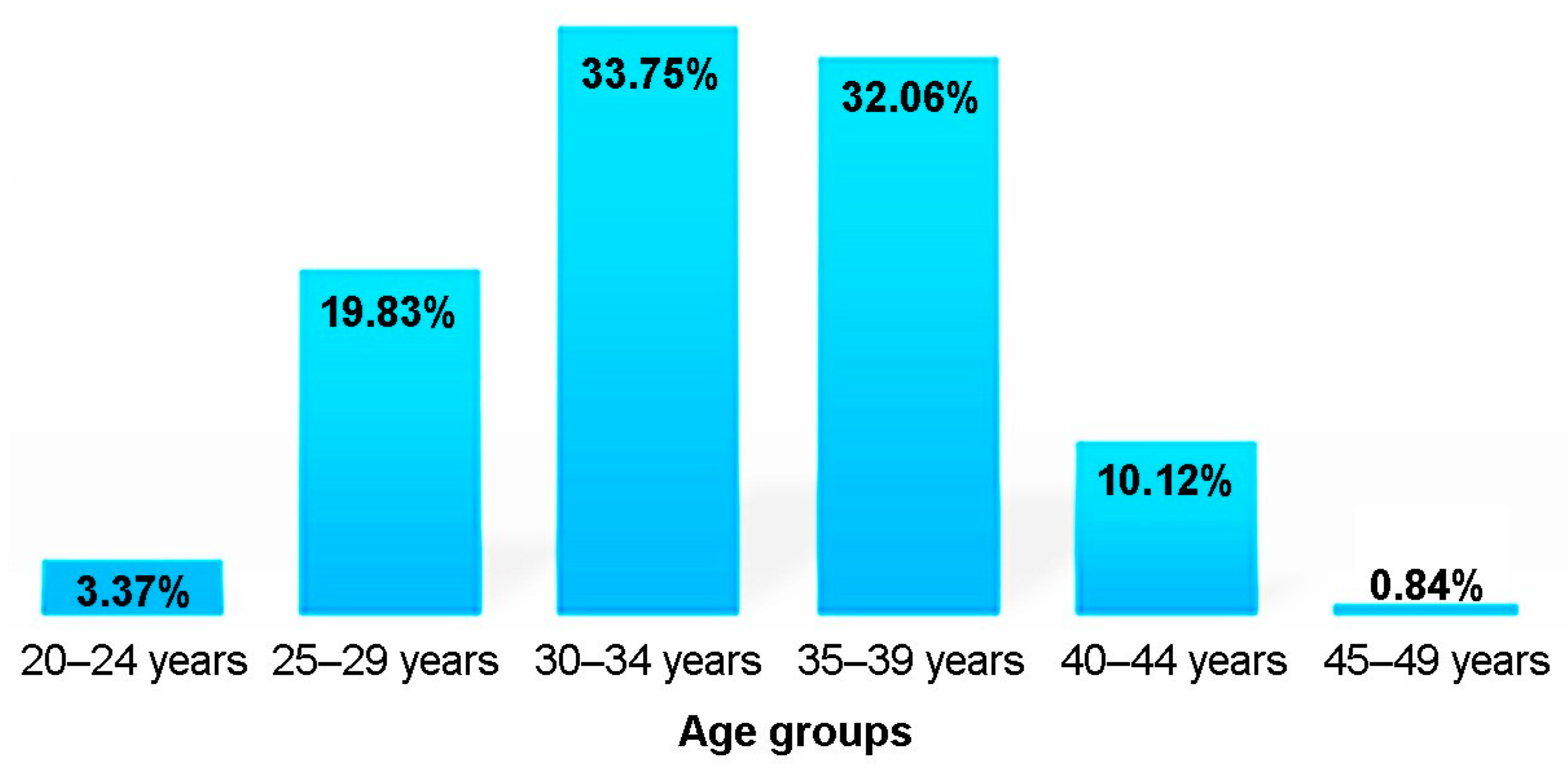
3.6. Maternal Age
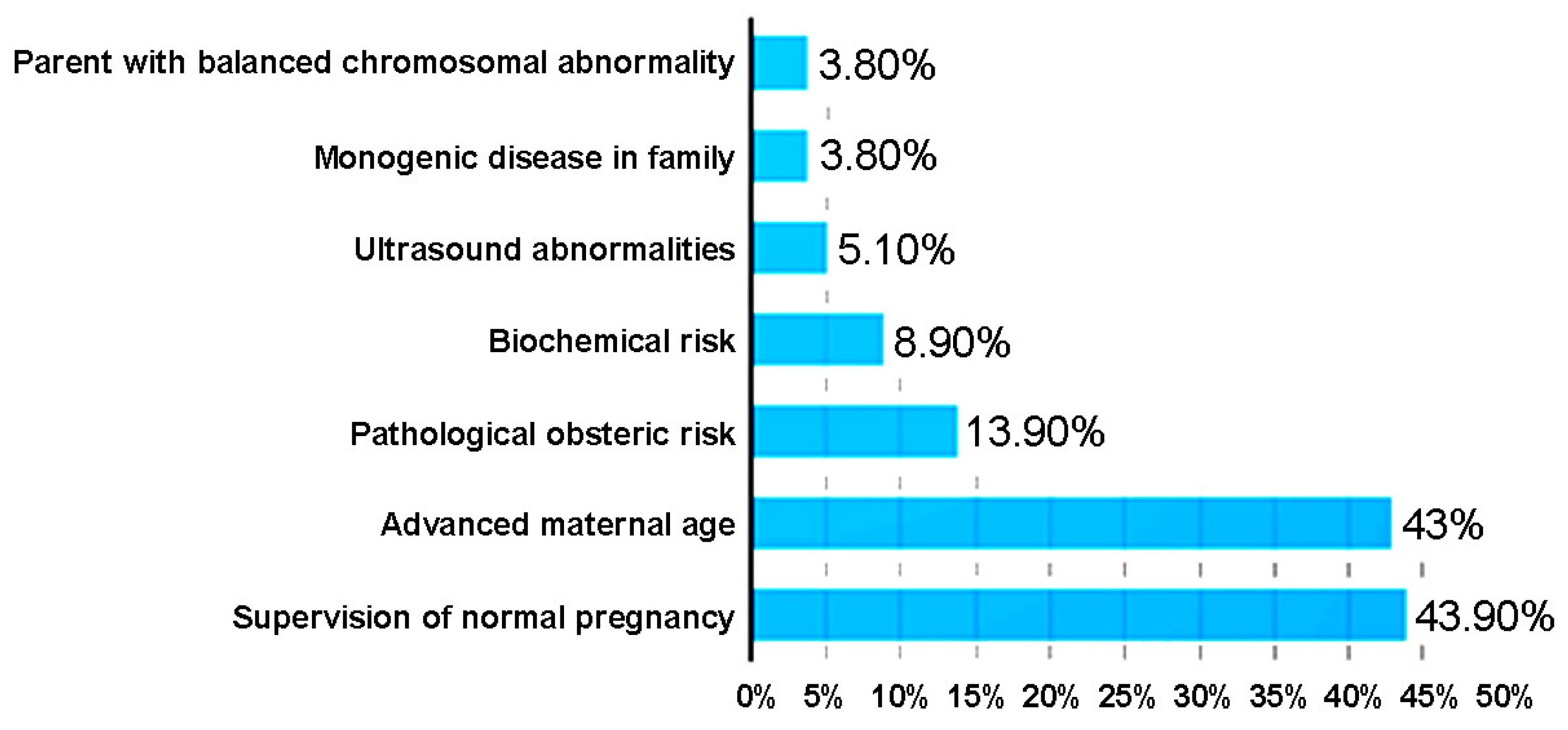
3.7. The Main Indications for the NIPT
3.8. The NIPT Results
3.9. Invasive Methods for Verifying (Confirmation/Exclusion) NIPT Results
3.10. Positive Predictive Value (PPV)
4. Discussion
4.1. Fetal Fraction
4.2. Maternal Age
4.3. Aneuploidies
4.4. Twins
4.5. Microdeletion/Microduplication Syndromes
4.6. Pre-Eclampsia
4.7. Genetic Counseling
4.8. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Yu, D.; Zhang, K.; Han, M.; Wei, P.; Ying, C.; Yunfeng, W.; Hongyan, J.; Ling, D.; Qiying, Z.; Xiaojie, S.; et al. Noninvasive prenatal testing for fetal subchromosomal copy number variations and chromosomal aneuploidy by low-pass whole-genome sequencing. Mol. Genet. Genom. Med. 2019, 7, e674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benn, P.; Cuckle, H.; Pergament, E. Non-invasive prenatal testing for aneuploidy: Current status and future prospects. Ultrasound Obstet. Gynecol. 2013, 42, 15–33. [Google Scholar] [CrossRef] [PubMed]
- Minear, M.A.; Lewis, C.; Pradhan, S.; Chandrasekharan, S. Global perspectives on clinical adoption of NIPT. Prenat. Diagn. 2015, 35, 959–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, Y.M.D.; Corbetta, N.; Chamberlain, P.F.; Rai, V.; Sargent, I.L.; Redman, C.W.; Wainscoat, J.S. Presence of fetal DNA in maternal plasma and serum. Lancet 1997, 350, 485–487. [Google Scholar] [CrossRef]
- Wang, Y.; Li, S.; Wang, W.; Dong, Y.; Zhang, M.; Wang, X.; Yin, C. Cell-free DNA screening for sex chromosome aneuploidies by non-invasive prenatal testing in maternal plasma. Mol. Cytogenet. 2020, 13, 1–8. [Google Scholar] [CrossRef]
- Russo, M.L.; Blakemore, K.J. A historical and practical review of first trimester aneuploidy screening. Semin. Fetal Neonatal Med. 2014, 19, 183–187. [Google Scholar] [CrossRef]
- Health Quality Ontario. Noninvasive Prenatal Testing for Trisomies 21, 18, and 13, Sex Chromosome Aneuploidies, and Mi-crodeletions: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2019, 19, 1–166. [Google Scholar]
- Nicolaides, K. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat. Diagn. 2011, 31, 7–15. [Google Scholar] [CrossRef]
- Gorduza, E.V.; Socolov, D.G.; Socolov, R.V. Prenatal Biochemical and Ultrasound Markers in Chromosomal Anomalies. In Congenital Anomalies-From the Embryo to the Neonate, 1st ed.; IntechOpen: Zagreb, Croatia, 2018; Volume 1, pp. 365–396. [Google Scholar] [CrossRef] [Green Version]
- Dey, M.; Sharma, S.; Aggarwal, S. Prenatal screening methods for aneuploidies. N. Am. J. Med. Sci. 2013, 5, 182–190. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Wang, C.; Sun, Y.; Tang, J.; Tong, K.; Zhu, J. Noninvasive prenatal testing for assessing foetal sex chromosome aneu-ploidy: A retrospective study of 45,773 cases. Mol. Cytogenet. 2021, 14, 1. [Google Scholar] [CrossRef]
- Zarrei, M.; MacDonald, J.; Merico, D.; Scherer, S. A copy number variation map of the human genome. Nat. Rev. Genet. 2015, 16, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Popescu, R.; Grămescu, M.; Caba, L.; Pânzaru, M.-C.; Butnariu, L.; Braha, E.; Popa, S.; Rusu, C.; Cardos, G.; Zeleniuc, M.; et al. A Case of Inherited t(4;10)(q26;q26.2) Chromosomal Translocation Elucidated by Multiple Chromosomal and Molecular Analyses. Case Report and Review of the Literature. Genes 2021, 12, 1957. [Google Scholar] [CrossRef] [PubMed]
- Gug, C.; Stoicanescu, D.; Mozos, I.; Nussbaum, L.; Cevei, M.; Stambouli, D.; Pavel, A.G.; Doros, G. De novo 8p21.3→p23.3 Duplication With t(4;8)(q35;p21.3) Translocation Associated With Mental Retardation, Autism Spectrum Disorder, and Con-genital Heart Defects: Case Report With Literature Review. Front. Pediatr. 2020, 8, 375. [Google Scholar] [CrossRef] [PubMed]
- LaLonde, E.; Rentas, S.; Lin, F.; Dulik, M.C.; Skraban, C.M.; Spinner, N.B. Genomic Diagnosis for Pediatric Disorders: Revolution and Evolution. Front. Pediatr. 2020, 8, 373. [Google Scholar] [CrossRef] [PubMed]
- Gug, C.; Huțanu, D.; Vaida, M.; Doroş, G.; Popa, C.; Stroescu, R.; Furău, G.; Furau, C.; Grigorita, L.; Mozos, I. De novo un-balanced translocation t(15;22)(q26.2;q12) with velo-cardio-facial syndrome: A case report and review of the literature. Exp. Ther. Med. 2018, 16, 3589–3595. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, P. An Update on Common Chromosome Microdeletion and Microduplication Syndromes. Pediatr. Ann. 2018, 47, e198–e203. [Google Scholar] [CrossRef]
- Wapner, R.; Babiarz, J.E.; Levy, B.; Stosic, M.; Zimmermann, B.; Sigurjonsson, S.; Wayham, N.; Ryan, A.; Banjevic, M.; Lacroute, P.; et al. Expanding the scope of noninvasive prenatal testing: Detection of fetal microdeletion syndromes. Am. J. Obstet. Gynecol. 2015, 212, 332.e1–332.e9. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Gao, Y.; Hu, Z.; Lin, L.; Yin, X.; Wang, J.; Chen, D.; Chen, F.; Jiang, H.; Ren, J.; et al. Performance Evaluation of NIPT in Detection of Chromosomal Copy Number Variants Using Low-Coverage Whole-Genome Sequencing of Plasma DNA. PLoS ONE 2016, 11, e0159233. [Google Scholar] [CrossRef]
- Sun, X.; Lu, J.; Ma, X. An efficient method for noninvasive prenatal diagnosis of fetal trisomy 13, trisomy 18, and trisomy 21. PLoS ONE 2019, 14, e0215368. [Google Scholar] [CrossRef] [Green Version]
- Samura, O. Update on noninvasive prenatal testing: A review based on current worldwide research. J. Obstet. Gynaecol. Res. 2020, 46, 1246–1254. [Google Scholar] [CrossRef]
- Koumbaris, G.; Achilleos, A.; Nicolaou, M.; Loizides, C.; Tsangaras, K.; Kypri, E.; Mina, P.; Sismani, C.; Velissariou, V.; Christopoulou, G.; et al. Targeted capture enrichment followed by NGS: Development and validation of a single comprehensive NIPT for chromosomal aneuploidies, microdeletion syndromes and monogenic diseases. Mol. Cytogenet. 2019, 12, 48. [Google Scholar] [CrossRef] [Green Version]
- Gug, C.; Chiriac, V.D.; Catu, D.; Budau, G.; Costa, S.D.; Navolan, D.B. Prenatal Cytogenetic Diagnosis in Timisoara: 1 Year Experience. Timis. Med. J. 2003, 53, 113–117. [Google Scholar]
- Yao, H.; Jiang, F.; Hu, H.; Gao, Y.; Zhu, Z.; Zhang, H.; Wang, Y.; Guo, Y.; Liu, L.; Yuan, Y.; et al. Detection of fetal sex chro-mosome aneuploidy by massively parallel sequencing of maternal plasma DNA: Initial experience in a Chinese hospital. Ul-trasound Obstet. Gynecol. 2014, 44, 17–24. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, D.W.; Platt, L.D.; Goldberg, J.D.; Abuhamad, A.Z.; Sehnert, A.J.; Rava, R.P. Genome-Wide Fetal Aneuploidy Detection by Maternal Plasma DNA Sequencing. Obstet. Gynecol. 2012, 119, 890–901. [Google Scholar] [CrossRef]
- Bianchi, D.W.; Chiu, R.W.K. Sequencing of Circulating Cell-free DNA during Pregnancy. N. Engl. J. Med. 2018, 379, 464–473. [Google Scholar] [CrossRef]
- Taneja, P.A.; Prosen, T.L.; De Feo, E.; Kruglyak, K.M.; Halks-Miller, M.; Curnow, K.J.; Bhatt, S. Fetal aneuploidy screening with cell-free DNA in late gestation. J. Matern. Neonatal Med. 2017, 30, 338–342. [Google Scholar] [CrossRef] [Green Version]
- Hestand, M.S.; Bessem, M.; Van Rijn, P.; De Menezes, R.X.; Sie, D.; Bakker, I.; Boon, E.M.J.; Sistermans, E.A.; Weiss, M.M. Fetal fraction evaluation in non-invasive prenatal screening (NIPS). Eur. J. Hum. Genet. 2018, 27, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Yang, J.; Huang, Y.; Qi, Y.; Hou, Y.; Peng, H.; Wang, D.; Wang, Y.; Luo, X.; Li, Y.; et al. Association between fetal fraction at the second trimester and subsequent spontaneous preterm birth. Prenat. Diagn. 2019, 39, 1191–1197. [Google Scholar] [CrossRef]
- Hou, Y.; Yang, J.; Qi, Y.; Guo, F.; Peng, H.; Wang, D.; Wang, Y.; Luo, X.; Li, Y.; Yin, A. Factors affecting cell-free DNA fetal fraction: Statistical analysis of 13,661 maternal plasmas for non-invasive prenatal screening. Hum. Genom. 2019, 13, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hudecova, I.; Sahota, D.; Heung, M.M.S.; Jin, Y.; Lee, W.S.; Leung, T.Y.; Lo, Y.M.D.; Chiu, R.W. Maternal Plasma Fetal DNA Fractions in Pregnancies with Low and High Risks for Fetal Chromosomal Aneuploidies. PLoS ONE 2014, 9, e88484. [Google Scholar] [CrossRef] [PubMed]
- Ashoor, G.; Poon, L.C.; Syngelaki, A.; Mosimann, B.; Nicolaides, K.H. Fetal Fraction in Maternal Plasma Cell-Free DNA at 11–13 Weeks’ Gestation: Effect of Maternal and Fetal Factors. Fetal Diagn. Ther. 2012, 31, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Palomaki, G.E.; Kloza, E.M.; Lambert-Messerlian, G.M.; van den Boom, D.; Ehrich, M.; Deciu, C.; Bombard, A.T.; Haddow, J.E. Circulating cell free DNA testing: Are some test failures informative? Prenat. Diagn. 2015, 35, 289–293. [Google Scholar] [CrossRef] [PubMed]
- McKanna, T.; Ryan, A.; Krinshpun, S.; Kareht, S.; Marchand, K.; Grabarits, C.; Ali, M.; McElheny, A.; Gardiner, K.; Lechien, K.; et al. Fetal fraction-based risk algorithm for non-invasive prenatal testing: Screening for trisomies 13 and 18 and triploidy in women with low cell-free fetal DNA. Ultrasound Obstet. Gynecol. 2019, 53, 73–79. [Google Scholar] [CrossRef]
- Gug, C.; Rațiu, A.; Navolan, D.; DrĂgan, I.; Groza, I.-M.; Păpurică, M.; Vaida, M.-A.; Mozoș, I.; Jurcă, M.C. Incidence and Spectrum of Chromosome Abnormalities in Miscarriage Samples: A Retrospective Study of 330 Cases. Cytogenet. Genome Res. 2019, 158, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Gug, C.; Burada, F.; Ioana, M.; Riza, A.L.; Moldovan, M.; Mozoș, I.; Rațiu, A.; Martiniuc, V.; Gorduza, E.V. Polyploidy in First and Second Trimester Pregnancies in Romania—A Retrospective Study. Clin Lab. 2020, 66, 517–527. [Google Scholar] [CrossRef]
- Chen, E.Z.; Chiu, R.W.K.; Sun, H.; Akolekar, R.; Chan, K.C.A.; Leung, T.Y.; Jiang, P.; Zheng, Y.W.L.; Lun, F.M.F.; Chan, L.Y.S.; et al. Noninvasive Prenatal Diagnosis of Fetal Trisomy 18 and Trisomy 13 by Maternal Plasma DNA Sequencing. PLoS ONE 2011, 6, e21791. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.M.D.; Chan, K.C.A.; Sun, H.; Chen, E.Z.; Jiang, P.; Lun, F.M.F.; Zheng, Y.W.; Leung, T.Y.; Lau, T.K.; Cantor, C.R.; et al. Maternal Plasma DNA Sequencing Reveals the Genome-Wide Genetic and Mutational Profile of the Fetus. Sci. Transl. Med. 2010, 2, 61ra91. [Google Scholar] [CrossRef]
- Yamada, T.; Sekizawa, A.; Fujii, Y.; Hirose, T.; Samura, O.; Suzumori, N.; Miura, K.; Sawai, H.; Hirahara, F.; Murotsuki, J. Maternal age-specific risk for trisomy 21 based on the clinical performance of NIPT and empirically derived NIPT age-specific positive and negative predictive values in Japan. J. Hum. Genet. 2018, 63, 1035–1040. [Google Scholar] [CrossRef]
- Zhang, H.; Gao, Y.; Jiang, F.; Fu, M.; Yuan, Y.; Guo, Y.; Zhu, Z.; Lin, M.; Liu, Q.; Tian, Z.; et al. Non-invasive prenatal testing for trisomies 21, 18 and 13: Clinical experience from 146 958 pregnancies. Ultrasound Obstet. Gynecol. 2015, 45, 530–538. [Google Scholar] [CrossRef]
- Jiang, F.; Ren, J.; Chen, F.; Zhou, Y.; Xie, J.; Dan, S.; Su, Y.; Xie, J.; Yin, B.; Su, W.; et al. Noninvasive Fetal Trisomy (NIFTY) test: An advanced noninvasive prenatal diagnosis methodology for fetal autosomal and sex chromosomal aneuploidies. BMC Med Genom. 2012, 5, 57. [Google Scholar] [CrossRef] [Green Version]
- Vaida, M.A.; Streian, C.G.; Gug, C.; Damen, N.S.; Jianu, A.M.; Grigoriță, A.; Grigoriță, L. Morphological Study of Fossa Ovalis in Formalin-Fixed Human Hearts and Its Clinical Importance. Medicina 2021, 57, 1254. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.C.Y.; Chan, K.C.A.; Zheng, Y.W.L.; Jiang, P.; Liao, G.J.W.; Sun, H.; Akolekar, R.; Leung, T.Y.; Go, A.T.J.I.; van Vugt, J.M.G.; et al. Size-based molecular diagnostics using plasma DNA for noninvasive prenatal testing. Proc. Natl. Acad. Sci. USA 2014, 111, 8583–8588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleinfinger, P.; Lohmann, L.; Luscan, A.; Trost, D.; Bidat, L.; Debarge, V.; Castaigne, V.; Senat, M.-V.; Brechard, M.-P.; Guilbaud, L.; et al. Strategy for Use of Genome-Wide Non-Invasive Prenatal Testing for Rare Autosomal Aneuploidies and Unbalanced Structural Chromosomal Anomalies. J. Clin. Med. 2020, 9, 2466. [Google Scholar] [CrossRef] [PubMed]
- Scott, F.; Bonifacio, M.; Sandow, R.; Ellis, K.; Smet, M.E.; McLennan, A. Rare autosomal trisomies: Important and not so rare. Prenat Diagn. 2018, 38, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Lv, Y.; Yin, S.; Liu, H.; Li, X.; Liang, B.; Kong, L.; Liu, C. Screening of fetal chromosomal aneuploidy diseases using noninvasive prenatal testing in twin pregnancies. Expert Rev. Mol. Diagn. 2019, 19, 189–196. [Google Scholar] [CrossRef]
- Hartwig, T.S.; Ambye, L.; Werge, L.; Weiergang, M.P.; Nørgaard, P.; Sørensen, S.; Jørgensen, F.S. Non-Invasive Prenatal Testing (NIPT) in pregnancies with trisomy 21, 18 and 13 performed in a public setting—Factors of importance for correct in-terpretation of results. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 226, 35–39. [Google Scholar] [CrossRef]
- Qi, Y.; Yang, J.; Hou, Y.; Hu, R.; Wang, D.; Peng, H.; Yin, A. Potential influence of parental copy number variations on non-invasive prenatal testing (NIPT): Two case reports. Mol. Cytogenet. 2020, 13, 18. [Google Scholar] [CrossRef]
- Wapner, R.J.; Martin, C.L.; Levy, B.; Ballif, B.C.; Eng, C.M.; Zachary, J.M.; Savage, M.; Platt, L.D.; Saltzman, D.; Grobman, W.A.; et al. Chromosomal microarray versus karyotyping for prenatal diagnosis. N. Engl. J Med. 2012, 367, 2175–2184. [Google Scholar] [CrossRef] [Green Version]
- van der Meij, K.R.; Sistermans, E.A.; Macville, M.V.; Stevens, S.J.; Bax, C.J.; Bekker, M.N.; Bilardo, C.M.; Boon, E.M.; Boter, M.; Diderich, K.E.; et al. TRIDENT-2: National Implementation of Genome-wide Non-invasive Prenatal Testing as a First-Tier Screening Test in the Netherlands. Am. J. Hum. Genet. 2019, 105, 1091–1101. [Google Scholar] [CrossRef]
- Hu, H.; Wang, L.; Wu, J.; Zhou, P.; Fu, J.; Sun, J.; Cai, W.; Liu, H.; Yang, Y. Noninvasive prenatal testing for chromosome aneuploidies and subchromosomal microdeletions/microduplications in a cohort of 8141 single pregnancies. Hum. Genom. 2019, 13, 14. [Google Scholar] [CrossRef] [Green Version]
- Mozos, I.; Jianu, D.; Gug, C.; Stoian, D. Links between High-Sensitivity C-Reactive Protein and Pulse Wave Analysis in Middle-Aged Patients with Hypertension and High Normal Blood Pressure. Dis. Markers 2019, 2019, 2568069. [Google Scholar] [CrossRef] [Green Version]
- Mozos, I.; Gug, C.; Mozos, C.; Stoian, D.; Pricop, M.; Jianu, D. Associations between Intrinsic Heart Rate, P Wave and QT Interval Durations and Pulse Wave Analysis in Patients with Hypertension and High Normal Blood Pressure. Int. J. Environ. Res. Public Health 2020, 17, 4350. [Google Scholar] [CrossRef]
- Contro, E.; Bernabini, D.; Farina, A. Cell-Free Fetal DNA for the Prediction of Pre-Eclampsia at the First and Second Trimesters: A Systematic Review and Meta-Analysis. Mol. Diagn. Ther. 2017, 21, 125–135. [Google Scholar] [CrossRef]
- Thurik, F.F.; Ruiter, M.L.-D.; Javadi, A.; Kwee, A.; Woortmeijer, H.; Page-Christiaens, G.C.M.L.; Franx, A.; Van Der Schoot, C.E.; Koster, M.P.H. Absolute first trimester cell-free DNA levels and their associations with adverse pregnancy outcomes. Prenat. Diagn. 2016, 36, 1104–1111. [Google Scholar] [CrossRef] [PubMed]
- Suzumori, N.; Sekizawa, A.; Ebara, T.; Samura, O.; Sasaki, A.; Akaishi, R.; Wada, S.; Hamanoue, H.; Hirahara, F.; Izumi, H.; et al. Fetal cell-free DNA fraction in maternal plasma for the prediction of hypertensive disorders of pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 224, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Gerson, K.D.; Truong, S.; Haviland, M.J.; O’Brien, B.M.; Hacker, M.R.; Spiel, M.H. Low fetal fraction of cell-free DNA predicts placental dysfunction and hypertensive disease in pregnancy. Pregnancy Hypertens. 2019, 16, 148–153. [Google Scholar] [CrossRef]
- Koelper, N.C.; Sammel, M.D.; Dugoff, L.; Bender, W.R. Association of Fetal Fraction of Cell-Free DNA and Hypertensive Disorders of Pregnancy. Am. J. Perinatol. 2018, 36, 311–316. [Google Scholar] [CrossRef]
- Rolnik, D.L.; Costa, F.D.S.; Lee, T.J.; Schmid, M.; McLennan, A.C. Association Between Fetal Fraction on Cell-Free DNA Testing and First-Trimester Markers for Pre-eclampsia. Obstet. Gynecol. Surv. 2019, 74, 265–266. [Google Scholar] [CrossRef]
- Buchanan, A.; Sachs, A.; Toler, T.; Tsipis, J. NIPT: Current utilization and implications for the future of prenatal genetic counseling. Prenat. Diagn. 2014, 34, 850–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wax, J.R.; Cartin, A.; Chard, R.; Lucas, F.L.; Pinette, M.G. Noninvasive prenatal testing: Impact on genetic counseling, invasive prenatal diagnosis, and trisomy 21 detection. J. Clin. Ultrasound 2015, 43, 1–6. [Google Scholar] [CrossRef]
- Pan, X.; Zhang, C.; Li, X.; Chen, S.; Huijuan, G.; Zhang, Y.; Chen, F.; Jiang, H.; Jiang, F.; Zhang, H.; et al. Noninvasive fetal sex determination by maternal plasma sequencing and application in X-linked disorder counseling. J. Matern Fetal Neonatal Med. 2014, 27, 1829–1833. [Google Scholar] [CrossRef] [PubMed]
- Belengeanu, V.; Rozsnyai, K.; Gug, C.; Bănăţeanu, M.; Farcaş, S.; Belengeanu, A. Ambras syndrome: Report on two affected siblings with no prior family history. Clin. Dysmorphol. 2004, 13, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Gug, C.; Mihaescu, A.; Mozos, I. Two mutations in the thiazide-sensitive NaCl co-transporter gene in a Romanian Gitelman syndrome patient: Case report. Ther. Clin. Risk Manag. 2018, 14, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gug, C.; Gorduza, E.V.; Lăcătuşu, A.; Vaida, M.A.; Bîrsăşteanu, F.; Puiu, M.; Stoicănescu, D. CHARGE syndrome associated with de novo (I1460Rfs*15) frameshift mutation of CHD7 gene in a patient with arteria lusoria and horseshoe kidney. Exp. Ther. Med. 2020, 20, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Gug, C.; Caba, L.; Mozos, I.; Stoian, D.; Atasie, D.; Gug, M.; Gorduza, E.V. Rare splicing mutation in COL1A1 gene identified by whole exomes sequencing in a patient with osteogenesis imperfecta type I followed by prenatal diagnosis: A case report and review of the literature. Gene 2020, 741, 144565. [Google Scholar] [CrossRef]
- Shaw, J.; Scotchman, E.; Chandler, N.; Chitty, L. Non-invasive prenatal testing for aneuploidy, copy number variants and single gene disorders. Reproduction 2020, 160, A1–A11. [Google Scholar] [CrossRef]
- Belengeanu, V.; Stoicanescu, D.; Stoian, M.; Andreescu, N.; Budisan, C. Ichthyosis congenita, harlequin fetus type: A case report. Adv. Med. Sci. 2009, 54, 113–115. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Result | Number of Cases | Mean FF 1 | SD 2 | Standard Error of the Mean |
|---|---|---|---|---|---|
| Maternal age | Up to 34 years | 215 | 11.23 | 4.28 | 0.37 |
| Over 35 years | 163 | 10.61 | 3.93 | 0.39 | |
| NIPT risk of aneuploidy | No risk | 362 | 11.03 | 4.14 | 0.28 |
| Risk for aneuploidy as a unique abnormality | 10 | 10.40 | 4.18 | 0.82 | |
| NIPT risk of aneuploidy NIPT risk of microdeletion | Risk for aneuploidy and microdeletion | 2 | 10.21 | 4.07 | 0.54 |
| No risk | 372 | 10.93 | 4.16 | 0.27 | |
| Risk for microdeletion as a unique abnormality | 4 | 12.57 | 2.76 | 1.23 | |
| NIPT risk of microdeletion Risk confirmation | Risk for microdeletion and aneuploidy | 2 | 11.03 | 3.07 | 0.89 |
| Not necessary | 362 | 11.00 | 4.22 | 0.28 | |
| Not confirmed | 7 | 9.17 | 2.40 | 0.98 | |
| Risk confirmation | Confirmed | 9 | 11.24 | 2.61 | 0.87 |
| Total | 378 | 10.96 | 4.14 | 0.27 |
| Parameters Associated with FF 1 | Statistical Significance | Statistical Analysis/p Values |
|---|---|---|
| Gestational age | no significant correlation | Spearman Correlation ρ = 0.053/p = 0.418 |
| Pregnant women in the age risk category, over 35 years | insignificantly lower | Mann-Whitney U test/p = 0.400 |
| Maternal age | no significant correlation | Spearman Correlation ρ = −0.022/p = 0.740 |
| Pregnant women who had the NIPT normal result | insignificantly increased | Mann-Whitney U test/p = 0.728 |
| Pregnant women with no risk of aneuploidy | insignificantly increased | Kruskal-Wallis test/p = 0.315 |
| Pregnant women at risk of microdeletion as a single abnormality | insignificantly increased | Kruskal-Wallis test/p = 0.176 |
| Cases confirmed by invasive methods | insignificant association | Kruskal-Wallis test/p = 0.490 |
| Maternal Age (Years) | Mean ± SD 1 | Minimum–Maximum | Number of Cases |
|---|---|---|---|
| Group up to 34 years | 29.8 ± 2.87 | 21–34 | 216 |
| Group over 35 years | 38.2 ± 2.61 | 35–47 | 164 |
| Cases with NIPT risk for trisomy 21 | 34.8 ± 6.38 | 25–42 | 5 |
| Cases with NIPT risk for trisomy 18 | 36.3 ± 7.10 | 30–44 | 3 |
| Cases with NIPT risk for trisomy 13 | 39 | 39 | 1 |
| Cases with NIPT risk for trisomy 14 | 41 | 41 | 1 |
| Cases with NIPT risk for X monosomy | 33.5 ± 4.95 | 30–37 | 2 |
| Group with NIPT risk for all types of tested aneuploidy | 35.83 ± 5.57 | 25–44 | 12 |
| Group with confirmed aneuploidy | 34.5 ± 5.21 | 25-42 | 8 |
| Group with NIPT risk of aneuploidy and microdeletion | 35.5 ± 6.09 | 26–41 | 6 |
| Group with confirmed microdeletion | 41 | 41 | 1 |
| Entire group | 33.4 ± 4.96 | 21–47 | 380 |
| NIPT Risk Assessment | Number of Cases | (%) | Invasive Prenatal Diagnosis | PPV 1 (%) | ||
|---|---|---|---|---|---|---|
| Confirmed | False Positive | False Negative | ||||
| Total number of cases with NIPT result | 378 | 100 | ||||
| NIPT low risk | 362 | 95.76 | - | - | - | 100 |
| NIPT increased risk | 16 | 4.23 | 8 | |||
| NIPT increased risk for isolated aneuploidies | 10 | 2.64 | 7 | 3 | - | 70 |
| Trisomy 21 | 5 | 1.32 | 5 | 0 | 0 | 100 |
| Trisomy 18 | 3 | 0.79 | 2 | 1 | 0 | 66.66 |
| Trisomy 13 | 0 | 0 | 0 | 1 | 0 | |
| Monosomy X | 2 | 0.53 | 0 | 2 | 0 | 0 |
| NIPT increased risk for aneuploidy and microdeletion | 2 | 0.53 | 1 | 1 | 0 | 16.66 |
| Trisomy 13 and 1p36 microdeletion syndrome | 1 | 0.26 | 0 0 | 1 1 | 0 | 0 |
| Trisomy 14 and del(X)(p22.33-11.21) | 1 | 0.26 | 0 1 | 1 0 | 0 | 0 |
| NIPT increased risk for isolated microdeletions | 4 | 1.04 | 0 | 4 | 0 | 0 |
| del(10q25.2-q26.3) | 1 | 0.26 | 0 | 1 | 0 | 0 |
| del(15)(q11.2-13.1) | 1 | 0.26 | 0 | 1 | 0 | 0 |
| del(20q11.21-q13.13) | 1 | 0.26 | 0 | 1 | 0 | 0 |
| del(22q11.2) microdeletion syndrome | 1 | 0.26 | 0 | 1 | 0 | 0 |
| NIPT High Risk for Microdeletions | Size (Mb 1) Determined by NIPT | FF 2 (%) | Gestational Age (Weeks) | aCGH 3 and Size (Mb) |
|---|---|---|---|---|
| del(X)(p22.33–11.21) | 54.27 | 15.64 | 13 | arr[GRCh37] Xp22.33p11.1 (168551_62051248)x1 61.88 Mb |
| del(10q25.2–q26.3) | 22.57 | 5.3 | 11 | False-positive |
| del(20q11.21–q13.13) | 18.40 | 8.32 | 12 | False-positive |
| del(15)(q11.2–13.1) | 5.60 | 10.96 | 13 | False-positive |
| del(22q11.2) microdeletion syndrome | 2.54 | 9 | 12 | False-positive |
| 1p36 microdeletion syndrome | 2.30 | 12.3 | 16 | False-positive |
| Chromosomal Abnormality | Sensitivity | Specificity | PPV 1 | ||||
|---|---|---|---|---|---|---|---|
| NIFTY BGI | NIPS INVITAE | NIFTY BGI | NIPS INVITAE | NIFTY BGI | NIPS INVITAE | Present study | |
| Trisomy 21 | 99.17% | 99.99% | 99.95% | 99.89% | 92.19% | 92.89 | 100% |
| Trisomy 18 | 98.24%, | 99.99% | 99.95% | 99.99% | 76.61% | 89.11 | 66.66% |
| Trisomy 13 | >99.9% | 99.99% | 99.96% | 99.69% | 32.84% | 73.54 | 0% |
| Monosomy X | >99.9% | 99.99% | - | 99.89% | 40% | 69.15 | 0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gug, C.; Mozos, I.; Ratiu, A.; Tudor, A.; Gorduza, E.V.; Caba, L.; Gug, M.; Cojocariu, C.; Furau, C.; Furau, G.; et al. Genetic Counseling and Management: The First Study to Report NIPT Findings in a Romanian Population. Medicina 2022, 58, 79. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010079
Gug C, Mozos I, Ratiu A, Tudor A, Gorduza EV, Caba L, Gug M, Cojocariu C, Furau C, Furau G, et al. Genetic Counseling and Management: The First Study to Report NIPT Findings in a Romanian Population. Medicina. 2022; 58(1):79. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010079
Chicago/Turabian StyleGug, Cristina, Ioana Mozos, Adrian Ratiu, Anca Tudor, Eusebiu Vlad Gorduza, Lavinia Caba, Miruna Gug, Catalina Cojocariu, Cristian Furau, Gheorghe Furau, and et al. 2022. "Genetic Counseling and Management: The First Study to Report NIPT Findings in a Romanian Population" Medicina 58, no. 1: 79. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58010079