

TENS Improves Cisplatin-Induced Neuropathy in Lung Cancer Patients
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Stefens-Stawna, P.; Piorunek, T.; Gabryel-Batura, H.; Kozubski, W.; Michalak, S. Neurological Paraneoplastic Syndromes in Lung Cancer Patients; Springer: Berlin/Heidelberg, Germany, 2012; Volume 756, pp. 333–339. [Google Scholar] [CrossRef]
- Hausheer, F.H.; Schilsky, R.L.; Bain, S.; Berghorn, E.J.; Lieberman, F. Diagnosis, Management, and Evaluation of Chemotherapy-Induced Peripheral Neuropathy. Semin. Oncol. 2006, 33, 15–49. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Goldstein, D.; Krishnan, A.V.; Lin, C.S.-Y.; Friedlander, M.L.; Cassidy, J.; Koltzenburg, M.; Kiernan, M.C. Chemotherapy-induced peripheral neurotoxicity: A critical analysis. CA Cancer J. Clin. 2013, 63, 419–437. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.K. Drug-Induced Neurological Disorders; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar] [CrossRef]
- Gregg, R.W.; Molepo, J.M.; Monpetit, V.J.; Mikael, N.Z.; Redmond, D.; Gadia, M.; Stewart, D.J. Cisplatin neurotoxicity: The relationship between dosage, time, and platinum concentration in neurologic tissues, and morphologic evidence of toxicity. J. Clin. Oncol. 1992, 10, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Mollman, J.; Glover, D.; Hogan, M.; Furman, R. Cisplatin neuropathy Risk Factors, Prognosis, and Protection by WR-2721 JOAN. Cancer 1988, 61, 2192–2195. [Google Scholar] [CrossRef]
- Andres, A.L.; Gong, X.; Di, K.; Bota, D.A. Low-doses of cisplatin injure hippocampal synapses: A mechanism for ‘chemo’ brain? Exp. Neurol. 2014, 255, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Brydøy, M.; Oldenburg, J.; Klepp, O.; Bremnes, R.M.; Wist, E.A.; Wentzel-Larsen, T.; Hauge, E.R.; Dahl, O.; Fosså, S.D. Observational Study of Prevalence of Long-term Raynaud-Like Phenomena and Neurological Side Effects in Testicular Cancer Survivors. JNCI J. Natl. Cancer Inst. 2009, 101, 1682–1695. [Google Scholar] [CrossRef]
- Von Schlippe, M.; Fowler, C.J.; Harland, S.J. Cisplatin neurotoxicity in the treatment of metastatic germ cell tumour: Time course and prognosis. Br. J. Cancer 2001, 85, 823–826. [Google Scholar] [CrossRef]
- Nalley, C. Risk Factors for Chemotherapy-Induced Peripheral Neuropathy. Oncol. Times 2021, 43, 33. [Google Scholar] [CrossRef]
- Molassiotis, A.; Cheng, H.L.; Leung, K.T.; Li, Y.C.; Wong, K.H.; Au, J.S.K.; Sundar, R.; Chan, A.; De Ng, T.R.; Suen, L.K.P.; et al. Risk factors for chemotherapy-induced peripheral neuropathy in patients receiving taxane- and platinum-based chemotherapy. Brain Behav. 2019, 9, e01312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertz, D.L.; Tofthagen, C.; Faithfull, S. Predisposing Factors for the Development of Chemotherapy-Induced Peripheral Neuropathy (CIPN). In Diagnosis, Management and Emerging Strategies for Chemotherapy-Induced Neuropathy; Springer: Cham, Switzerland, 2021; pp. 19–51. [Google Scholar] [CrossRef]
- Cavaletti, G.; Marmiroli, P. Chemotherapy-induced peripheral neurotoxicity. Curr. Opin. Neurol. 2015, 28, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Huh, B.; Kim, H.K.; Kim, K.-H.; Abdi, S. Treatment of Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Recommendations. Pain Physician 2018, 21, 571–592. [Google Scholar] [PubMed]
- Attal, N.; Cruccu, G.; Baron, R.A.; Haanpää, M.; Hansson, P.; Jensen, T.S.; Nurmikko, T. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur. J. Neurol. 2010, 17, 1113–1188. [Google Scholar] [CrossRef] [PubMed]
- Rowbotham, M.C.; Twilling, L.; Davies, P.S.; Reisner, L.; Taylor, K.; Mohr, D. Oral Opioid Therapy for Chronic Peripheral and Central Neuropathic Pain. New Engl. J. Med. 2003, 348, 1223–1232. [Google Scholar] [CrossRef] [PubMed]
- Cruccu, G.; Aziz, T.Z.; Garcia-Larrea, L.; Hansson, P.; Jensen, T.S.; Lefaucheur, J.-P.; Simpson, B.A.; Taylor, R.S. EFNS guidelines on neurostimulation therapy for neuropathic pain. Eur. J. Neurol. 2007, 14, 952–970. [Google Scholar] [CrossRef]
- Kilinç, M.; Livanelioglu, A.; Yildirim, S.A.; Tan, E. Effects of transcutaneous electrical nerve stimulation in patients with peripheral and central neuropathic pain. J. Rehabil. Med. 2014, 46, 454–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Püsküllüoğlu, M.; Tomaszewski, K.A.; Grela-Wojewoda, A.; Pacholczak-Madej, R.; Ebner, F. Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Chemotherapy-Induced Peripheral Neuropathy in Cancer Patients: A Systematic Review. Medicina 2022, 58, 284. [Google Scholar] [CrossRef]
- Medical Reasrch Council. Aids to the Examination of the Peripheral Nervous System; Her Majesty’s Station Off: London, UK, 1976; pp. 1–61.
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brochet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.H.S.; Patterson, D.G. Experimental development of the graphic rating method. Psychol. Bull. 1921, 18, 98–99. [Google Scholar]
- Bergman, B.; Aaronson, N.; Ahmedzai, S.; Kaasa, S.; Sullivan, M. The EORTC QLQ-LC13: A modular supplement to the EORTC core quality of life questionnaire (QLQ-C30) for use in lung cancer clinical trials. Eur. J. Cancer 1994, 30, 635–642. [Google Scholar] [CrossRef]
- Cella, D.F.; Bonomi, A.E.; Lloyd, S.R.; Tulsky, D.S.; Kaplan, E.; Bonomi, P. Reliability and validity of the Functional Assessment of Cancer Therapy-Lung (FACT-L) quality of life instrument. Lung Cancer 1995, 12, 199–220. [Google Scholar] [CrossRef]
- Weissgerber, T.L.; Savic, M.; Winham, S.J.; Stanisavljevic, D.; Garovic, V.D.; Milic, N.M. Data visualization, bar naked: A free tool for creating interactive graphics. J. Biol. Chem. 2017, 292, 20592–20598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SPSS for Windows, release 25.0; SPSS: Chicago, IL, USA, 2017.
- Starobova, H.; Vetter, I. Pathophysiology of Chemotherapy-Induced Peripheral Neuropathy. Front. Mol. Neurosci. 2017, 10, 174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, S.; Barton, D.; Kottschade, L.; Grothey, A.; Loprinzi, C. Chemotherapy-induced peripheral neuropathy: Prevention and treatment strategies. Eur. J. Cancer 2008, 44, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, S.; Coraci, D.; Brau, F.; Galluzzo, V.; Loreti, C.; Caliandro, P.; Padua, L.; Maccauro, G.; Biscotti, L.; Bernabei, R. Neuropathic Pain in the Elderly. Diagnostics 2021, 11, 613. [Google Scholar] [CrossRef] [PubMed]
- Mc Leod, J. Paraneoplastic neuropathies. In Peripheral Neuropathy. II; Dyck, P.J., Thomas, P.K., Eds.; Saunders: Philadelphia, PA, USA, 1993; pp. 1583–1590. [Google Scholar]
- Antoine, J.-C.; Mosnier, J.-F.; Absi, L.; Convers, P.; Honnorat, J.; Michel, D. Carcinoma associated paraneoplastic peripheral neuropathies in patients with and without anti-onconeural antibodies. J. Neurol. Neurosurg. Psychiatry 1999, 67, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanaji, N.; Watanabe, N.; Kita, N.; Bandoh, S.; Tadokoro, A.; Ishii, T.; Dobashi, H.; Matsunaga, T. Paraneoplastic syndromes associated with lung cancer Nobuhiro Kanaji, Naoki Watanabe, Nobuyuki Kita, Shuji Bandoh, Akira Tadokoro, Tomoya Ishii, Hiroaki Dobashi, Takuya Matsunaga. World J. Clin. Oncol. 2014, 5, 197–223. [Google Scholar] [CrossRef]
- Miltenburg, N.C.; Boogerd, W. Chemotherapy-induced neuropathy: A comprehensive survey. Cancer Treat. Rev. 2014, 40, 872–882. [Google Scholar] [CrossRef]
- Tofthagen, C. Patient Perceptions Associated With Chemotherapy-Induced Peripheral Neuropathy. Clin. J. Oncol. Nurs. 2010, 14, E22–E28. [Google Scholar] [CrossRef] [Green Version]
- Ruelle, L.; Bentea, G.; Sideris, S.; El Koulali, M.; Holbrechts, S.; Lafitte, J.-J.; Grigoriu, B.; Sculier, C.; Meert, A.-P.; Durieux, V.; et al. Autoimmune paraneoplastic syndromes associated to lung cancer: A systematic review of the literature Part 4: Neurological paraneoplastic syndromes, involving the peripheral nervous system and the neuromuscular junction and muscles. Lung Cancer 2017, 111, 150–163. [Google Scholar] [CrossRef]
- Krarup-Hansen, A.; Helweg-Larsen, S.; Schmalbruch, H.; Rorth, M.; Krarup, C. Neuronal involvement in cisplatin neuropathy: Prospective clinical and neurophysiological studies. Brain 2006, 130, 1076–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McQuay, H.J.; Moore, R.A.; Eccleston, C.; Morley, S.; Williams, A.C. Systematic review of outpatient services for chronic pain control. Health Technol. Assess. 1997, 1, i–iv. [Google Scholar] [CrossRef] [PubMed]
- Reichstein, L.; Labrenz, S.; Ziegler, D.; Martin, S. Effective treatment of symptomatic diabetic polyneuropathy by high-frequency external muscle stimulation. Diabetologia 2005, 48, 824–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, D.; Marshall, H.J. Diabetic Peripheral Neuropathy: Amelioration of Pain With Transcutaneous Electrostimulation. Diabetes Care 1997, 20, 1702–1705. [Google Scholar] [CrossRef] [PubMed]
- Hamza, M.A.; White, P.F.; Craig, W.F.; Ghoname, E.S.; Ahmed, H.E.; Proctor, T.J.; Noe, C.E.; Vakharia, A.S.; Gajraj, N. Percutaneous electrical nerve stimulation: A novel analgesic therapy for diabetic neuropathic pain. Diabetes Care 2000, 23, 365–370. [Google Scholar] [CrossRef] [Green Version]
- Forst, T.; Nguyen, M.; Forst, S.; Disselhoff, B.; Pohlmann, T.; Pfützner, A. Impact of low fre- quency transcutaneous electrical nerve stimulation on symptomatic diabetic neuropathy using the new salutaris device. Diabetes 2004, 17, 163–168. [Google Scholar]
- Cheing, G.L.Y.; Luk, M.L.M. Transcutaneous electrical nerve stimulation for neuropathic pain. J. Hand Surg. 2005, 30, 50–55. [Google Scholar] [CrossRef]
- Thorsteinsson, G.; Stonnington, H.H.; Stillwell, G.K.; Elveback, L.R. Transcutaneous electrical stimulation: A double-blind trial of its efficacy for pain. Arch. Phys. Med. Rehabil. 1977, 58, 8–13. [Google Scholar] [CrossRef]
- Rutgers, M.; Van Romunde, L.; Osman, P. A small randomized comparative trial of acupuncture versus transcutaneous electrical neurostimulation in postherpetic neuralgia. Pain Clin. 1988, 2, 87–89. [Google Scholar]
- Bloodworth, D.M.; Nguyen, B.N.; Garver, W.; Moss, F.; Pedroza, C.; Tran, T.; Chiou-Tan, F.Y. Comparison of stochastic vs. conventional transcutaneous electrical stimulation for pain modulation in patients with electromyographically documented radiculopathy. Am. J. Phys. Med. Rehabil. 2004, 83, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Dubinsky, R.M.; Miyasaki, J. Assessment: Efficacy of transcutaneous electric nerve stimulation in the treatment of pain in neurologic disorders (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2009, 74, 173–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siemens, W.; Boehlke, C.; Bennett, M.I.; Offner, K.; Becker, G.; Gaertner, J. Transcutaneous electrical nerve stimulation for advanced cancer pain inpatients in specialist palliative care—A blinded, randomized, sham-controlled pilot cross-over trial. Support Care Cancer 2020, 28, 5323–5333. [Google Scholar] [CrossRef] [Green Version]
- Laurent, H.; Galvaing, G.; Thivat, E.; Coudeyre, E.; Aubreton, S.; Richard, R.; Kwiatkowski, F.; Costes, F.; Filaire, M. Effect of an intensive 3-week preoperative home rehabilitation programme in patients with chronic obstructive pulmonary disease eligible for lung cancer surgery: A multicentre randomised controlled trial. BMJ Open 2017, 7, e017307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagnon, G.J.; Nasr, N.M.; Liao, J.J.; Molzahn, I.; Marsh, D.; McRae, D.; Henderson, F.C., Sr. Treatment of spinal tumors using cyberKnife fractionated stereotactic radiosurgery: Pain and quality-of-life assessment after treatment in 200 patients. Neurosurgery 2009, 64, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Fiorelli, A.; Morgillo, F.; Milione, R.; Pace, M.C.; Passavanti, M.B.; Laperuta, P.; Aurilio, C.; Santini, M. Control of post-thoracotomy pain by transcutaneous electrical nerve stimulation: Effect on serum cytokine levels, visual analogue scale, pulmonary function and medication. Eur. J. Cardio-Thorac. Surg. 2011, 41, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, F.C.; Issy, A.M.; Sakata, R.K. Avaliação do efeito da estimulação nervosa elétrica transcutânea (TENS) para analgesia após toracotomia. Rev. Bras. Anestesiol. 2011, 61, 564–567. [Google Scholar] [CrossRef]
- Solak, O.; Turna, A.; Pekcolaklar, A.; Metin, M.; Sayar, A.; Gürses, A. Transcutaneous Electric Nerve Stimulation for the Treatment of Postthoracotomy Pain: A Randomized Prospective Study. Thorac. Cardiovasc. Surg. 2007, 55, 182–185. [Google Scholar] [CrossRef] [PubMed]
- Chandra, A.; Banavaliker, J.N.; Das, P.K.; Hasti, S. Use of transcutaneous electrical nerve stimulation as an adjunctive to epidural analgesia in the management of acute thoracotomy pain. Indian J. Anaesth. 2010, 54, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, M.; Erdogan, A.; Erbil, N.; Karakaya, H.; Demircan, A. Prospective, Randomized, Placebo-controlled Study of the Effect of TENS on Postthoracotomy Pain and Pulmonary Function. World J. Surg. 2005, 29, 1563–1570. [Google Scholar] [CrossRef]
- DeSantana, J.M.; Sluka, K.A.; Lauretti, G.R. High and low frequency TENS reduce postoperative pain intensity after laparoscopic tubal ligation: A randomized controlled trial. Clin. J. Pain 2009, 25, 12–19. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
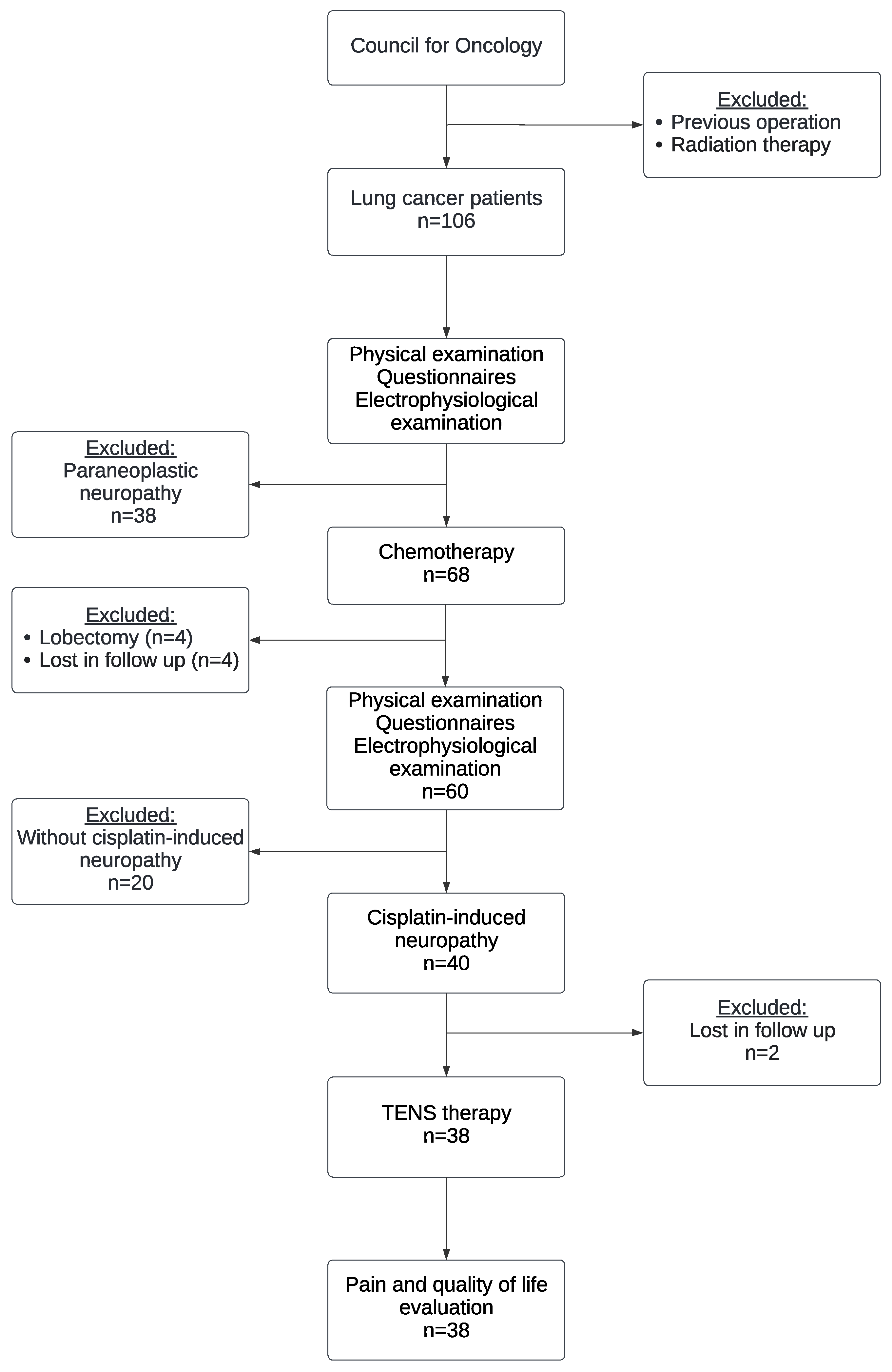
| All Lung Cancer Patients n = 106 | without Neuropathy n = 68 | with Neuropathy n = 38 | Patients without Neuropathy before Cisplatin Therapy n = 60 | Patients without Neuropathy after Cisplatin Therapy n = 20 | Cisplatin-Induced Neuropathy n = 40 | |
|---|---|---|---|---|---|---|
| Gender, n (%) | ||||||
| Male | 74 (70%) | 45 (66%) | 29 (76%) | 42 (70%) | 15 (75%) | 27 (68%) |
| Female | 32 (30%) | 23 (34%) | 9 (24%) | 18 (30%) | 5 (25%) | 13 (32%) |
| Age, mean (range) | 64 (47–83) | 62 (47–83) | 65 (51–77) | 63 (47–82) | 63 (49–78) | 63 (47–82) |
| Smoking habits, n (%) | ||||||
| Never | 1 (1%) | 0 (0%) | 1 (3%) | 0 (0%) | 0 (0%) | 0 (0%) |
| ex | 33 (31%) | 24 (35%) | 9 (24%) | 23 (38%) | 11 (55%) | 12 (30%) |
| Smoker | 72 (68%) | 44 (65%) | 28 (74%) | 37 (62%) | 9 (45%) | 28 (70%) |
| Stage of disease, n (%) | ||||||
| I | 2 (2%) | 1 (1%) | 1 (3%) | 1 (2%) | 0 (0%) | 1 (3%) |
| II | 5 (5%) | 2 (3%) | 3 (8%) | 1 (2%) | 0 (0%) | 1 (3%) |
| III | 55 (53%) | 35 (52%) | 20 (54%) | 31 (53%) | 13 (65%) | 18 (46%) |
| IV | 42 (40%) | 29 (43%) | 13 (35%) | 26 (44%) | 7 (35%) | 19 (49%) |
| Type of lung cancer, n (%) | ||||||
| Small-cell | 33 (31%) | 23 (34%) | 10 (26%) | 22 (37%) | 11 (55%) | 11 (28%) |
| Adenocarcinoma | 33 (31%) | 22 (33%) | 11 (29%) | 18 (31%) | 3 (15%) | 15 (38%) |
| Squamous | 39 (37%) | 22 (33%) | 17 (45%) | 19 (32%) | 6 (30%) | 13 (33%) |
| Small-cell/non-small-cell, n (%) | ||||||
| Small-cell | 32 (30%) | 22 (32%) | 10 (26%) | 21 (35%) | 10 (50%) | 11 (28%) |
| Non-small-cell | 74 (70%) | 46 (68%) | 28 (74%) | 39 (65%) | 10 (50%) | 29 (72%) |
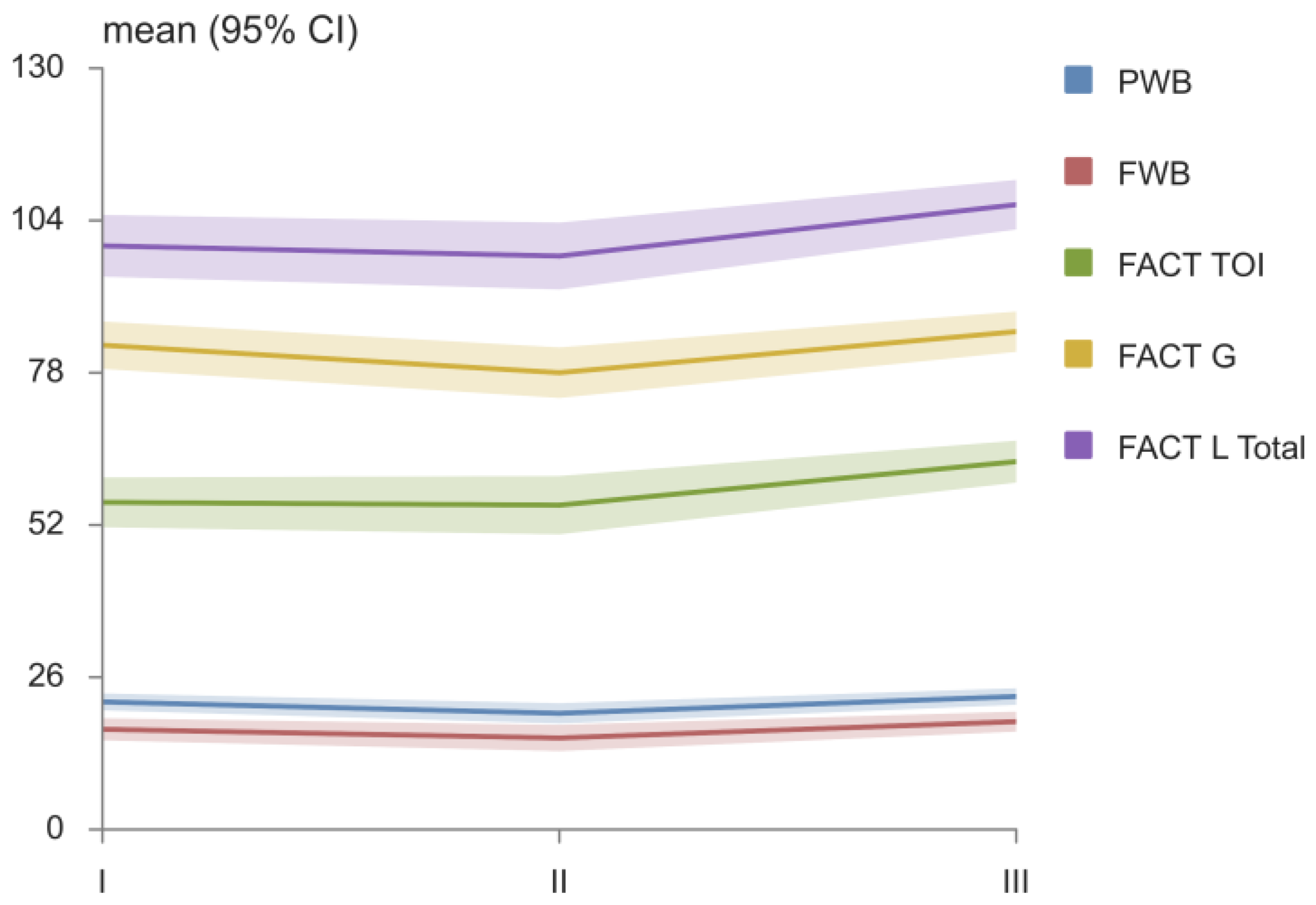
| FACT Domains | I | II | III | p |
|---|---|---|---|---|
| PWB, mean (95% CI) | 21.8 (20.4–23.2) | 19.8 (18.1–21.6) | 22.7 (21.3–24.1) | II vs. III * |
| SWB, mean (95% CI) | 25.3 (24.3–26.3) | 23.4 (22.7–24.1) | 23.4 (22.7–24.1) | I vs. II*, I vs. III * |
| EWB, mean (95% CI) | 18.5 (17.2–19.9) | 19.1 (17.9–20.4) | 20.5 (19.3–21.7) | I vs. III * |
| FWB, mean (95% CI) | 17.1 (15.2–19.0) | 15.6 (13.4–17.9) | 18.4 (16.7–20.1) | II vs. III * |
| LCS, mean (95% CI) | 17.0 (15.2–18.8) | 19.9 (18.1–21.7) | 21.7 (20.6–22.8) | I vs. II *, I vs. III *, II vs. III * |
| FACT L TOI, mean (95% CI) | 55.9 (51.6–60.1) | 55.4 (50.4–60.4) | 62.8 (59.3–66.4) | I vs. III *, II vs. III * |
| FACT G, mean (95% CI) | 82.7 (78.7–86.7) | 78.0 (73.7–82.3) | 85.0 (81.6–88.4) | II vs. III* |
| FACT L TOTAL, mean (95% CI) | 99.7 (94.4–104.9) | 97.9 (92.2–103.6) | 106.7 (102.5–110.9) | I vs. III *, II vs. III * |
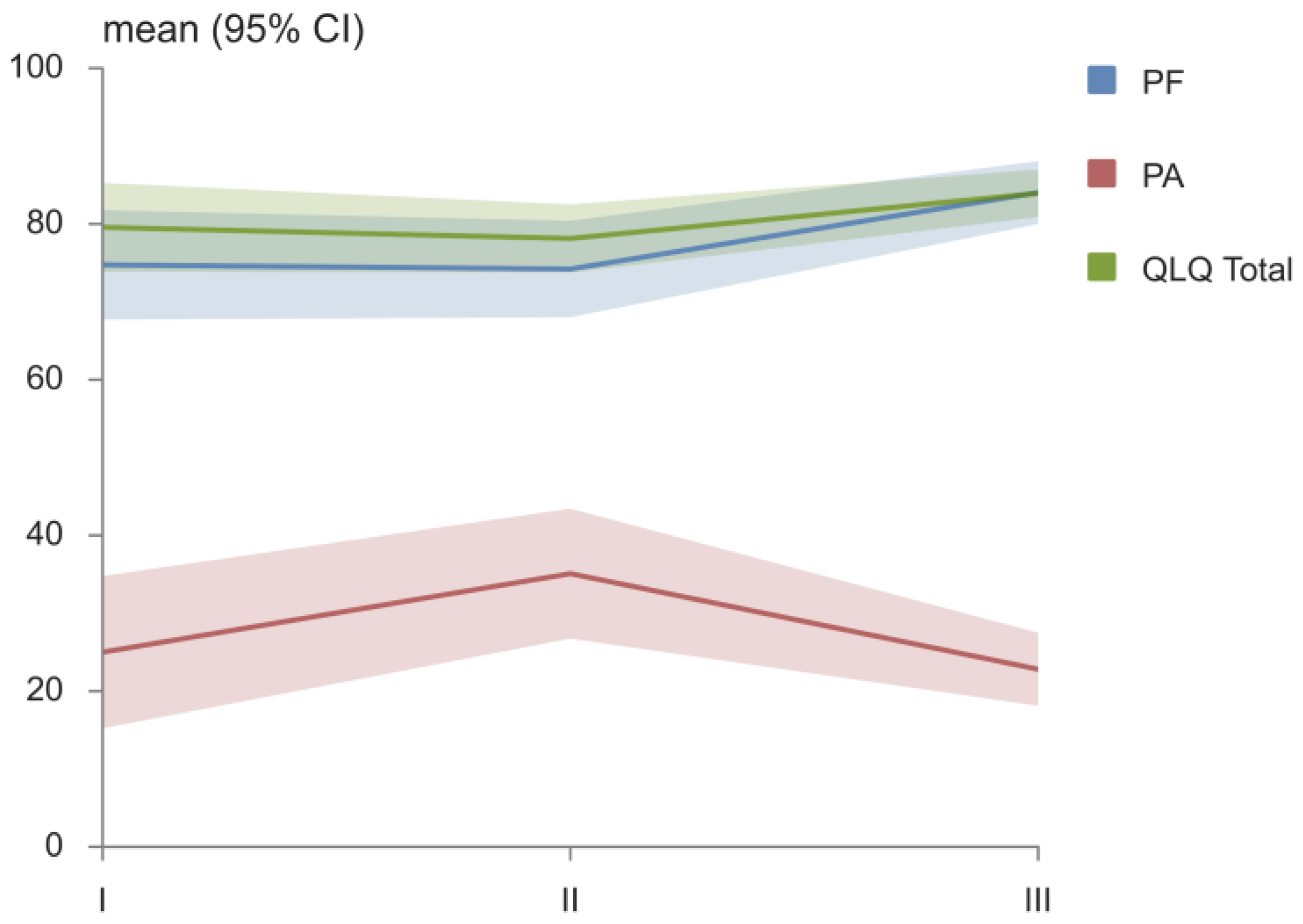
| EORTC QLQ-C30 Domains | I | II | III | p |
|---|---|---|---|---|
| PF, mean (95% CI) | 74.7 (67.7–81.7) | 74.2 (68.0–80.4) | 84.0 (80.0–88.1) | I vs. III *, II vs. III * |
| RF, mean (95% CI) | 67.6 (58.5–76.5) | 64.9 (55.2–74.6) | 71.1 (62.7–79.4) | II vs. III * |
| EF, mean (95% CI) | 73.9 (65.4–82.4) | 76.3 (69.4–83.2) | 79.8 (72.8–86.9) | |
| CF, mean (95% CI) | 93.4 (88.6–98.3) | 92.1 (86.0–98.2) | 94.7 (89.5–100.0) | |
| SF, mean (95% CI) | 82.9 (75.2–90.6) | 72.4 (64.2–80.6) | 76.8 (70.2–83.3) | |
| FA, mean (95% CI) | 36.5 (26.7–46.4) | 33.0 (26.3–39.8) | 28.9 (23.3–34.6) | |
| NV, mean (95% CI) | 7.0 (1.1–12.9) | 9.2 (2.5–15.9) | 6.6 (1.4–11.8) | |
| PA, mean (95% CI) | 25.0 (15.2–34.8) | 35.1 (26.8–43.4) | 22.8 (18.1–27.5) | II vs. III * |
| DY, mean (95% CI) | 22.8 (11.4–34.2) | 12.3 (4.9–19.7) | 14.0 (8.6–19.5) | |
| SL, mean (95% CI) | 25.4 (14.5–36.4) | 27.2 (17.7–36.7) | 15.8 (9.7–21.9) | II vs. III * |
| AP, mean (95% CI) | 24.6 (13.3–35.9) | 26.3 (15.5–37.2) | 14.0 (7.5–20.6) | II vs. III * |
| CO, mean (95% CI) | 12.3 (4.1–20.5) | 9.6 (4.0–15.3) | 8.8 (3.9–13.7) | |
| DI, mean (95% CI) | 4.4 (0.6–8.1) | 11.4 (5.0–17.8) | 4.4 (0.6–8.1) | I vs. II *, II vs. III * |
| FI, mean (95% CI) | 22.8 (12.6–33.0) | 35.1 (24.6–45.6) | 42.1 (30.8–53.4) | I vs. III * |
| QL, mean (95% CI) | 59.4 (52.8–66.0) | 57.0 (53.0–61.1) | 62.5 (59.3–65.7) | II vs. III * |
| QLQ Total, mean (95% CI) | 79.6 (73.9–85.3) | 78.1 (73.8–82.5) | 83.9 (80.9–87.0) | II vs. III * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomanovic Vujadinovic, S.; Ilic, N.; Selakovic, I.; Nedeljkovic, U.; Krstic, N.; Mujovic, N.; Dubljanin Raspopovic, E.; Jovanovic, D. TENS Improves Cisplatin-Induced Neuropathy in Lung Cancer Patients. Medicina 2022, 58, 1405. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101405
Tomanovic Vujadinovic S, Ilic N, Selakovic I, Nedeljkovic U, Krstic N, Mujovic N, Dubljanin Raspopovic E, Jovanovic D. TENS Improves Cisplatin-Induced Neuropathy in Lung Cancer Patients. Medicina. 2022; 58(10):1405. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101405
Chicago/Turabian StyleTomanovic Vujadinovic, Sanja, Nela Ilic, Ivan Selakovic, Una Nedeljkovic, Nevena Krstic, Natasa Mujovic, Emilija Dubljanin Raspopovic, and Dragana Jovanovic. 2022. "TENS Improves Cisplatin-Induced Neuropathy in Lung Cancer Patients" Medicina 58, no. 10: 1405. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58101405