
Upper Hemi-Sternotomy Provides Benefit for Patients with Isolated or Combined Mitral Valve Surgery

 ,
,
Abstract
:1. Introduction
2. Material and Methods
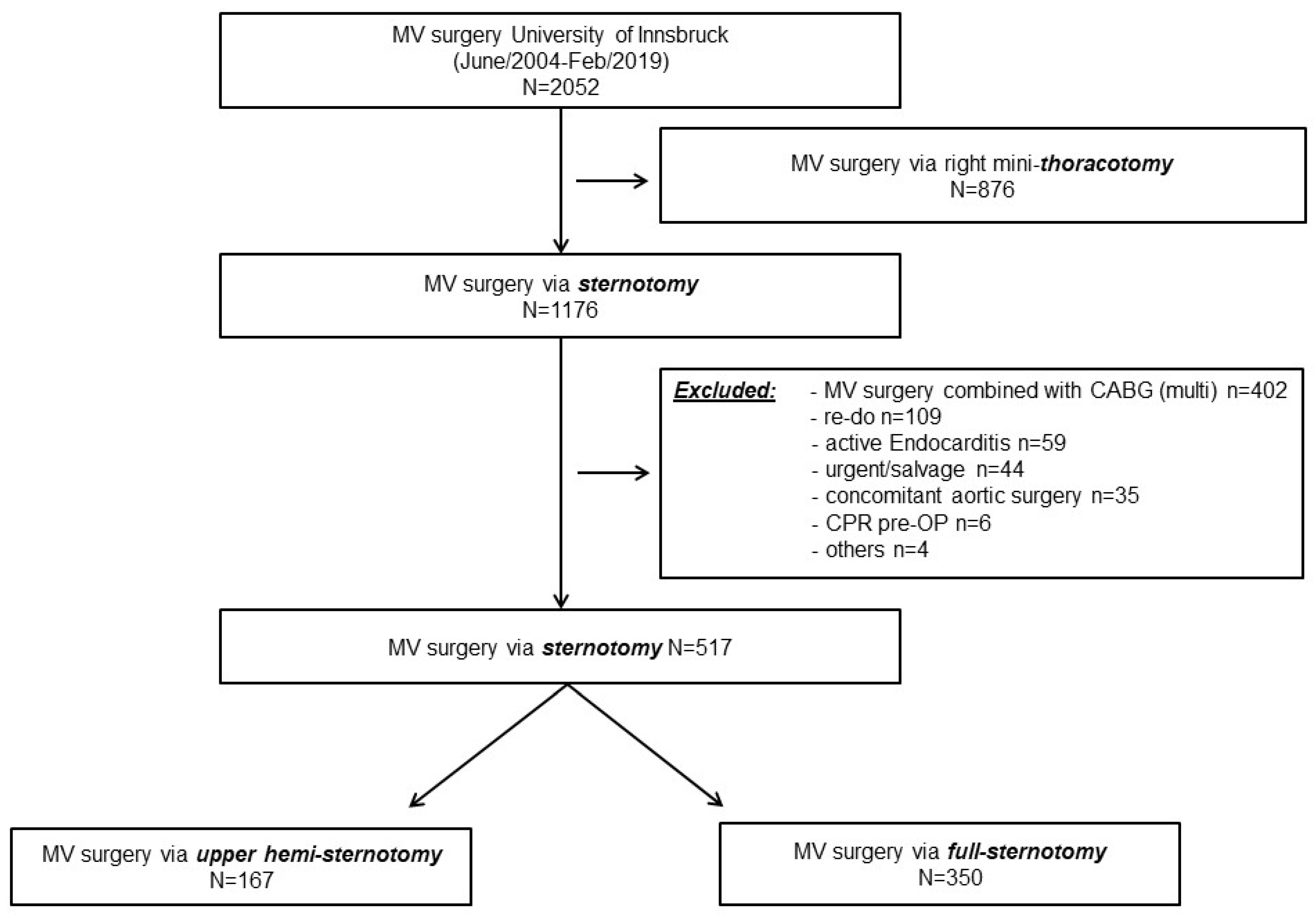
2.1. Patients
2.2. Study Cohort
2.3. Surgical Procedures
2.4. Outcome Parameters
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Outcomes
3.2.1. 30-Day Mortality and 1-Year Survival
3.2.2. Additional Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beckmann, A.; Meyer, R.; Lewandowski, J.; Markewitz, A.; Harringer, W. German Heart Surgery Report 2018: The Annual Updated Registry of the German Society for Thoracic and Cardiovascular Surgery. Thorac. Cardiovasc. Surg. 2019, 67, 331–344. [Google Scholar] [CrossRef] [Green Version]
- Ward, A.F.; Grossi, E.A.; Galloway, A.C. Minimally invasive mitral surgery through right mini-thoracotomy under direct vision. J. Thorac. Dis. 2013, 5 (Suppl. S6), S673–S679. [Google Scholar] [CrossRef]
- Glauber, M.; Miceli, A.; Canarutto, D.; Lio, A.; Murzi, M.; Gilmanov, D.; Ferrarini, M.; Farneti, P.A.; Quaini, E.L.; Solinas, M. Early and long-term outcomes of minimally invasive mitral valve surgery through right minithoracotomy: A 10-year experience in 1604 patients. J. Cardiothorac. Surg. 2015, 10, 181. [Google Scholar] [CrossRef] [Green Version]
- Grossi, E.A.; Goldman, S.; Wolfe, J.A.; Mehall, J.; Smith, J.M.; Ailawadi, G.; Salemi, A.; Moore, M.; Ward, A.; Gunnarsson, C.; et al. Minithoracotomy for mitral valve repair improves inpatient and postdischarge economic savings. J. Thorac. Cardiovasc. Surg. 2014, 148, 2818–2822.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vollroth, M.; Seeburger, J.; Garbade, J.; Borger, M.A.; Misfeld, M.; Mohr, F.W. Conversion rate and contraindications for minimally invasive mitral valve surgery. Ann. Cardiothorac. Surg. 2013, 2, 853–854. [Google Scholar] [CrossRef]
- Marin Cuartas, M.; Javadikasgari, H.; Pfannmueller, B.; Seeburger, J.; Gillinov, A.M.; Suri, R.M.; Borger, M.A. Mitral valve repair: Robotic and other minimally invasive approaches. Prog. Cardiovasc. Dis. 2017, 60, 394–404. [Google Scholar] [CrossRef] [PubMed]
- Saunders, P.C.; Grossi, E.A.; Sharony, R.; Schwartz, C.F.; Ribakove, G.H.; Culliford, A.T.; Delianides, J.; Baumann, F.G.; Galloway, A.C.; Colvin, S.B. Minimally invasive technology for mitral valve surgery via left thoracotomy: Experience with forty cases. J. Thorac. Cardiovasc. Surg. 2004, 127, 1026–1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semsroth, S.; Matteucci Gothe, R.; Raith, Y.R.; de Brabandere, K.; Hanspeter, E.; Kilo, J.; Kofler, M.; Muller, L.; Ruttman-Ulmer, E.; Grimm, M. Comparison of Two Minimally Invasive Techniques and Median Sternotomy in Aortic Valve Replacement. Ann. Thorac. Surg. 2017, 104, 877–883. [Google Scholar] [CrossRef] [Green Version]
- Gillinov, A.M.; Cosgrove, D.M. Minimally invasive mitral valve surgery: Mini-sternotomy with extended transseptal approach. Semin. Thorac. Cardiovasc. Surg. 1999, 11, 206–211. [Google Scholar] [CrossRef]
- Meyer, B.W.; Verska, J.J.; Lindesmith, G.G.; Jones, J.C. Open Repair of Mitral Valve Lesions: The Superior Approach. Ann. Thorac. Surg. 1965, 1, 453–457. [Google Scholar] [CrossRef]
- Esposito, G.; Cappabianca, G.; Bichi, S.; Patrini, D.; Pellegrino, P. Left atrial roof: An alternative minimal approach for mitral valve surgery. Innovations 2012, 7, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Risteski, P.; Monsefi, N.; Miskovic, A.; Josic, T.; Bala, S.; Salem, R.; Zierer, A.; Moritz, A. Triple valve surgery through a less invasive approach: Early and mid-term results. Interact. Cardiovasc. Thorac. Surg. 2017, 24, 677–682. [Google Scholar] [CrossRef] [Green Version]
- Oezpeker, C.; Barbieri, F.; Hoefer, D.; Schneider, B.; Bonaros, N.; Grimm, M.; Mueller, L. Mitral Valve Surgery via Partial Upper Sternotomy: Closing the Gap between Conventional Sternotomy and Right Lateral Minithoracotomy. Thorac. Cardiovasc. Surg. 2019, 67, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Downs, E.A.; Johnston, L.E.; LaPar, D.J.; Ghanta, R.K.; Kron, I.L.; Speir, A.M.; Fonner, C.E.; Kern, J.A.; Ailawadi, G. Minimally Invasive Mitral Valve Surgery Provides Excellent Outcomes Without Increased Cost: A Multi-Institutional Analysis. Ann. Thorac. Surg. 2016, 102, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Cao, C.; Gupta, S.; Chandrakumar, D.; Nienaber, T.A.; Indraratna, P.; Ang, S.C.; Phan, K.; Yan, T.D. A meta-analysis of minimally invasive versus conventional mitral valve repair for patients with degenerative mitral disease. Ann. Cardiothorac. Surg. 2013, 2, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Zhang, G.; Zhang, X. Review: Minimally invasive versus conventional dynamic hip screw fixation in elderly patients with intertrochanteric fractures: A systematic review and meta-analysis. Surg. Innov. 2011, 18, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Goldstone, A.B.; Atluri, P.; Szeto, W.Y.; Trubelja, A.; Howard, J.L.; MacArthur, J.W., Jr.; Newcomb, C.; Donnelly, J.P.; Kobrin, D.M.; Sheridan, M.A.; et al. Minimally invasive approach provides at least equivalent results for surgical correction of mitral regurgitation: A propensity-matched comparison. J. Thorac. Cardiovasc. Surg. 2013, 145, 748–756. [Google Scholar] [CrossRef] [Green Version]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2012, 41, 734–744. [Google Scholar] [CrossRef] [Green Version]
- Carpentier, A.; Filsoufi, F. Carpentier’s Reconstructive Valve Surgery, 1st ed.; Saunders: London, UK, 2010; 368p. [Google Scholar]
- Svensson, L.G. Minimally invasive surgery with a partial sternotomy “J” approach. Semin. Thorac. Cardiovasc. Surg. 2007, 19, 299–303. [Google Scholar] [CrossRef]
- Radwan, M.; Salewski, C.; Hecker, F.; Miskovic, A.; Risteski, P.; Hlavicka, J.; Moritz, A.; Walther, T.; Holubec, T. Mitral Valve Surgery via Upper Ministernotomy: Single-Centre Experience in More than 400 Patients. Medicina 2021, 57, 1179. [Google Scholar] [CrossRef]
- Svensson, L.G.; Atik, F.A.; Cosgrove, D.M.; Blackstone, E.H.; Rajeswaran, J.; Krishnaswamy, G.; Jin, U.; Gillinov, A.M.; Griffin, B.; Navia, J.L.; et al. Minimally invasive versus conventional mitral valve surgery: A propensity-matched comparison. J. Thorac. Cardiovasc. Surg. 2010, 139, 926–932.e2. [Google Scholar] [CrossRef] [Green Version]
- Oezpeker, U.C.; Barbieri, F.; Hoefer, D.; Bonaros, N.; Grimm, M.; Mueller, L. Partial Upper Sternotomy is a Safe Alternative in Mitral Annulus Decalcification. Semin. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lukac, P.; Hjortdal, V.E.; Pedersen, A.K.; Mortensen, P.T.; Jensen, H.K.; Hansen, P.S. Superior transseptal approach to mitral valve is associated with a higher need for pacemaker implantation than the left atrial approach. Ann. Thorac. Surg. 2007, 83, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Vlahakes, G.J. Right ventricular failure after cardiac surgery. Cardiol. Clin. 2012, 30, 283–289. [Google Scholar] [CrossRef]
- Zanobini, M.; Loardi, C.; Poggio, P.; Tamborini, G.; Veglia, F.; Di Minno, A.; Myasoedova, V.; Mammana, L.F.; Biondi, R.; Pepi, M.; et al. The impact of pericardial approach and myocardial protection onto postoperative right ventricle function reduction. J. Cardiothorac. Surg. 2018, 13, 55. [Google Scholar] [CrossRef]
- Rupprecht, L.; Schmid, C. Deep sternal wound complications: An overview of old and new therapeutic options. Open J. Cardiovasc. Surg. 2013, 6, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Doenst, T.; Diab, M.; Sponholz, C.; Bauer, M.; Farber, G. The Opportunities and Limitations of Minimally Invasive Cardiac Surgery. Dtsch. Arztebl. Int. 2017, 114, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salenger, R.; Gammie, J.S.; Collins, J.A. Minimally Invasive Aortic Valve Replacement. J. Card. Surg. 2016, 31, 38–50. [Google Scholar] [CrossRef]
- Shehada, S.E.; Ozturk, O.; Wottke, M.; Lange, R. Propensity score analysis of outcomes following minimal access versus conventional aortic valve replacement. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2016, 49, 464–469; discussion 469–470. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, N.; Johnson, J.; Brodin, L.A.; Gomes-Bernardes, A.; Sartipy, U.; Svenarud, P.; Dalen, M.; Back, M.; Alam, M.; Winter, R. Right ventricular mechanics and contractility after aortic valve replacement surgery: A randomised study comparing minimally invasive versus conventional approach. Open Heart 2018, 5, e000842. [Google Scholar] [CrossRef] [Green Version]
- McMurry, T.L.; Hu, Y.; Blackstone, E.H.; Kozower, B.D. Propensity scores: Methods, considerations, and applications in the Journal of Thoracic and Cardiovascular Surgery. J. Thorac. Cardiovasc. Surg. 2015, 150, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unmatched Data | After Propensity Score-Matching | |||||
|---|---|---|---|---|---|---|
| Full Sternotomy n = 350 | Upper Hemi-Sternotomy n = 167 | p-Value | Full Sternotomy n = 164 | Upper Hemi-Sternotomy n = 164 | p-Value | |
| Age (years) 1 | 69 (60–74) | 71 (63–77) | 0.027 | 72 (64–76) | 71 (63–77) | 0.859 |
| Gender, males (%, n) | 47.7 (167) | 44.3 (74) | 0.468 | 50 (82) | 43.3 (71) | 0.223 |
| Body surface area (m2) | 1.81 (1.66–1.96) | 1.81 (1.65–1.93) | 0.323 | 1.79 (1.65–1.94) | 1.81 (1.65–1.93) | 0.830 |
| Diabetes Mellitus (%, n) | 12 (42) | 18.3 (18) | 0.055 | 12.2 (20) | 18.3 (30) | 0.125 |
| Arterial hypertension (%, n) | 64.2 (224) | 85.9 (85) | <0.001 | 68.3 (112) | 81.1 (133) | 0.008 |
| COPD (%, n) | 35.4 (124) | 30.5 (51) | 0.292 | 35.4 (58) | 30.5 (50) | 0.347 |
| PAOD (%, n) | 2.3 (8) | 4.2 (7) | 0.223 | 2.4 (4) | 4.3 (7) | 0.358 |
| Dialysis (%, n) | 0.9 (3) | 3 (5) | 0.064 | 0.6 (1) | 3.0 (5) | 0.099 |
| Prev.CVE (%, n) | 4.3 (15) | 4.8 (8) | 0.762 | 6.7 (11) | 4.9 (8) | 0.478 |
| Acute HF < 3 months (%, n) | 4 (14) | 12.6 (21) | <0.001 | 5.5 (9) | 12.8 (21) | 0.022 |
| EuroSCORE II (%) 1 | 3.04 (1.69–4.84) | 3.0 (1.67–4.74) | 0.874 | 3.14 (1.88–4.95) | 3.0 (1.67–4.74) | 0.267 |
| LV-ejection fraction (%) 1 | 55 (47–61) | 59 (50–65) | 0.005 | 57 (49–63) | 59 (50–65) | 0.659 |
| NYHA III (%, n) | 54.0 (189) | 59.3 (99) | 0.228 | 56.1 (92) | 59.8 (98) | 0.502 |
| NYHA IV (%, n) | 5.7 (20) | 5.4 (9) | 0.893 | 5.5 (9) | 5.5 (9) | n.a |
| Interm.-atrial fibrillation (%, n) | 46.9 (164) | 37.1 (62) | 0.054 | 43.9 (72) | 37.8 (62) | 0.261 |
| Perm.-atrial fibrillation (%, n) | 23.2 (81) | 17.4 (29) | 0.159 | 22.0 (36) | 17.7 (29) | 0.332 |
| sPAP (mmHg) 1 | 50 (36–60) | 45 (36–57) | 0.135 | 50 (40–60) | 45 (36–57) | 0.024 |
| NT-proBNP (ng/L) 1 | 1189 (619–2498) | 1080 (414–2535) | 0.323 | 1248 (618–2476) | 1080 (430–2451) | 0.238 |
| Propensity Score Matched | |||
|---|---|---|---|
| Full Sternotomy n = 164 | Upper Hemi-Sternotomy n = 164 | p-Value | |
| MV-etiology | |||
| Primary (%, n) | 87.7 (144) | 86.0 (141) | 0.624 |
| Secondary (%, n) | 12.2 (20) | 14.0 (23) | 0.624 |
| Moderate to severe AC (%, n) | 35.4 (58) | 36.0 (59) | 0.908 |
| Surgical interventions | |||
| MVS isolated (%, n) | 47.6 (78) | 50.6 (83) | 0.581 |
| MV repair (%, n) | 59.8 (98) | 65.2 (107) | 0.305 |
| MV + TV-surgery (%, n) | 30.5 (50) | 31.1 (51) | 0.905 |
| MV + AV-surgery (%, n) | 18.3 (30) | 15.9 (26) | 0.557 |
| MV + AV + TV-surgery (%, n) | 3.7 (6) | 2.4 (4) | 0.521 |
| Atrial fibrillation surgery (%, n) | 15.2 (25) | 7.9 (13) | 0.038 |
| Full Sternotomy n = 164 | Upper Hemi-Sternotomy n = 164 | p-Value | |
|---|---|---|---|
| CPB time (min) 1 | 161 (130–196) | 164 (140–196) | 0.262 |
| Aortic X-clamp time (min) 1 | 107 (81–133) | 106 (88–132) | 0.829 |
| Second pump run/X-clamp (%, n) | 9.8 (16) | 6.1 (10) | 0.220 |
| ECMO (%, n) | 2.4 (4) | 1.2 (2) | 0.545 |
| LOS (%, n) | 31.1 (51) | 18.9 (31) | 0.011 |
| Tamponade or excessive bleeding (%, n) | 4.3 (7) | 3.0 (5) | 0.556 |
| Hemofiltration/-dialysis new (%, n) | 17.1 (28) | 12.8 (21) | 0.278 |
| Ventilation length (h) 1 | 13 (7–30) | 8 (5–17) | <0.001 |
| Red blood units (first 24 h) 1 | 1 (0–3) | 1 (0–3) | n.a. |
| ICU length (days) 1 | 2 (1–14) | 1 (1–3) | <0.001 |
| Hospital stay (days) 1 | 9 (8–13) | 8 (7–10) | <0.001 |
| MOF (%, n) | 6.7 (11) | 4.3 (7) | 0.332 |
| Sepsis (%, n) | 5.5 (9) | 2.4 (4) | 0.157 |
| Pneumonia (%, n) | 4.9 (8) | 3.0 (5) | 0.396 |
| Deep wound infection (%, n) | 3.7 (6) | 3.0 (5) | 0.759 |
| Stroke (%, n) | 3.0 (5) | 1.2 (2) | 0.252 |
| PM-implantation (%, n) | 5.5 (9) | 3.7 (6) | 0.428 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oezpeker, C.U.; Barbieri, F.; Hoefer, D.; Bonaros, N.; Grimm, M.; Mueller, L. Upper Hemi-Sternotomy Provides Benefit for Patients with Isolated or Combined Mitral Valve Surgery. Medicina 2022, 58, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020142
Oezpeker CU, Barbieri F, Hoefer D, Bonaros N, Grimm M, Mueller L. Upper Hemi-Sternotomy Provides Benefit for Patients with Isolated or Combined Mitral Valve Surgery. Medicina. 2022; 58(2):142. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020142
Chicago/Turabian StyleOezpeker, Cenk Ulvi, Fabian Barbieri, Daniel Hoefer, Nikolaos Bonaros, Michael Grimm, and Ludwig Mueller. 2022. "Upper Hemi-Sternotomy Provides Benefit for Patients with Isolated or Combined Mitral Valve Surgery" Medicina 58, no. 2: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020142