
The Influence of Oral Drotaverine Administration on Materno–Fetal Circulation during the Second and Third Trimester of Pregnancy


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
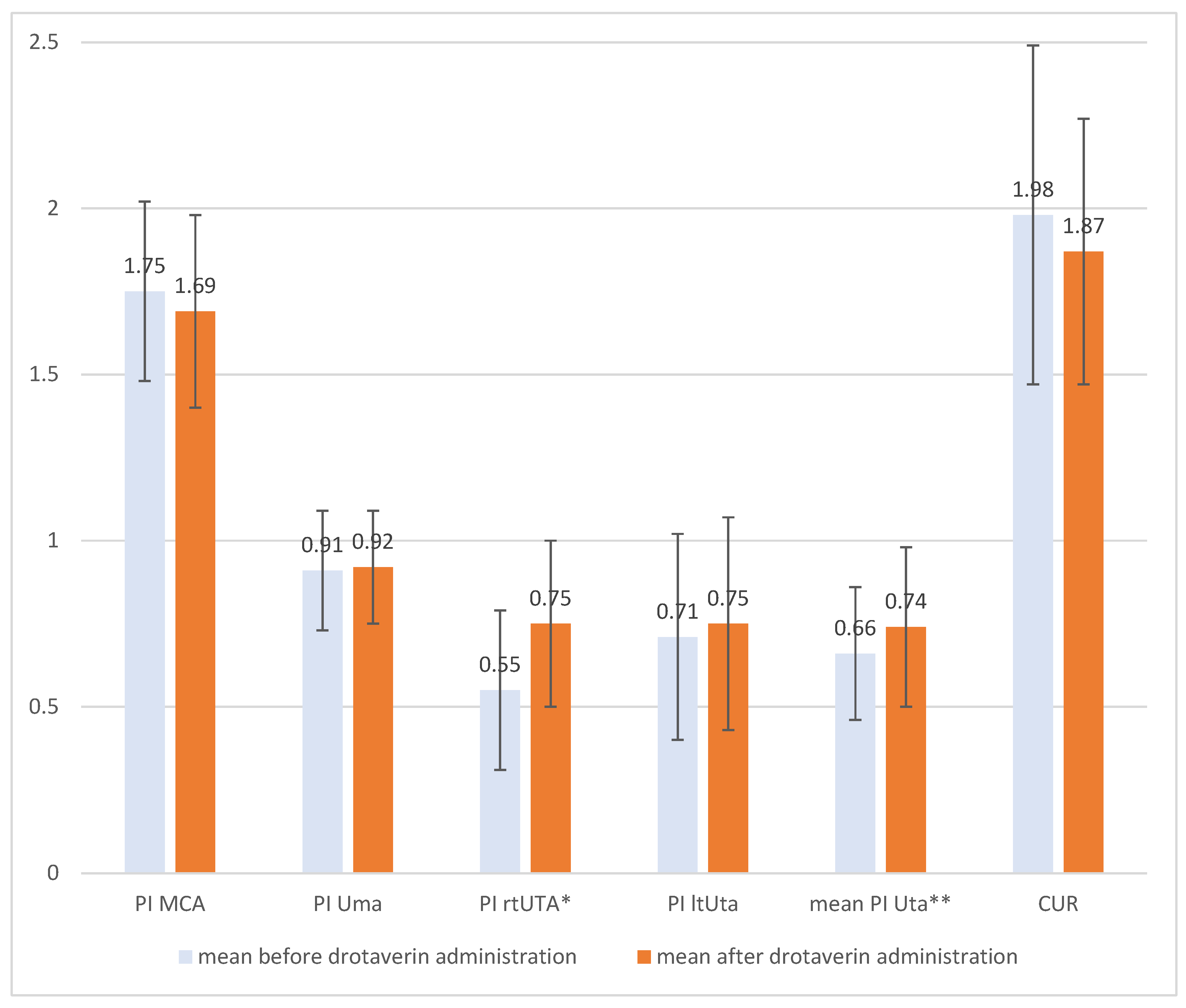
3. Results
4. Discussion
5. Conclusions
- The oral administration of 80 mg of drotaverine did not influence the Doppler flows (Uma, MCA).
- There is a correlation between the Doppler cerebro–umbilical ratio—CUR, and the height and bodyweight of a patient after the oral administration of 80 mg of drotaverine.
- After an oral dose of 80 mg of drotaverine the cerebro–umbilical ratio (CUR) did not change to abnormal values, and there were no signs of fetal cerebral blood flow centralization.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Piyamongkol, W. Preterm labour management-An evidence-update. J. Med. Assoc. Thai. 2004, 87, S154–S157. [Google Scholar] [PubMed]
- Wielgoś, M.; Bomba-Opoń, D.A. Tocolysis in preterm labour- current recommendations. Ginekol Pol. 2014, 85, 332–334. [Google Scholar] [CrossRef] [PubMed]
- Blasko, G. Pharmacology, mechanism of action and clinical significance of a convenient antispasmodic agent: Drotavarine. J. Am. Med. Assoc. India 1998, 1, 63–69. [Google Scholar]
- Yuel, V.I.; Kaur, V.; Kaur, D. Programmed labor for optimizing labor and delivery. JK Sci. 2008, 10, 62–64. [Google Scholar]
- Romics, I.; Molnár, D.L.; Timberg, G.; Mrklic, B.; Jelakovic, B.; Köszegi, G. The effect of drotaverine hydrochloride in acute colicky pain caused by renal and ureteric stones. BJU Int. 2003, 92, 92–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sommers De, K. Sommers’ Pharmacology. Pretoria: UP systematic review. Lancet 2006, 367, 1066–1074. [Google Scholar]
- Madhu, C.; Mahavarkar, S.; Bhave, S. A randomised controlled study comparing drotaverine hydrochloride and valethamate bromide in the augmentation of labour. Arch. Gynecol. Obstet. 2010, 282, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Rouamba, T.; Valea, I.; Bognini, J.D.; Kpoda, H.; Mens, P.F.; Gomes, M.F.; Tinto, H. Safety profile of drug use during pregnancy at peripheral health centers in Burkina Faso: A prospective observational Cohort Study. Fati. Kirakoya-Samadoulougou Drugs Real World Outcomes 2018, 5, 193–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, K.C.; Jain, P.; Goel, N.; Saxena, A. Drotaverine hydrochloride for augmentation of labor. Int. J. Gynaecol. Obs. 2004, 84, 17–22. [Google Scholar] [CrossRef]
- Ibrahim, M.I.; Alzeeniny, H.A.; Ellaithy, M.I.; Salama, A.H.; Abdellatif, M.A. Drotaverine to improve progression of labor among nulliparous women. Int. J. Gynaecol. Obs. 2014, 124, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.B.; Pundir, P.; Kumar, A.; Murthy, N.S. Drotaverine hydrochloride vs valethamate bromide in acceleration of labor. J. Gynaecol. Obs. 2001, 71, 255–260. [Google Scholar] [CrossRef]
- Rohwer, A.C.; Khondowe, O.; Young, T. Antispasmodic for Labour. Cochrane Database Syst. Rev. 2013, CD009243, 1–123. [Google Scholar] [CrossRef] [Green Version]
- Bolaji, O.O.; Onyeji, C.O.; Ogundaini, A.O.; Olugbade, T.A.; Ogunbona, F.A. Pharmacokinetics and bioavailability of drotaverine in humans. Eur. J. Drug Metab. Pharmacokinet. 1996, 21, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Szatmári, I.; Simon, G.; Vargay, Z.; Tóth, E.; Szüts, T. The fate of drotaverine-acephyllinate in rat and man. I. Absorption, distribution and excretion in the rat. Eur. J. Drug Metab. Pharmacokinet. 1984, 9, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Dyderski, S.; Grześkowiak, E.; Drobnik, L.; Szałek, E.; Balcerkiewicz, M.; Dubai, V. Bioavailability study of drotaverine from capsule and tablet preparations in healthy volunteers. Arzneimittelforschung 2004, 54, 298–302. [Google Scholar] [CrossRef] [PubMed]
- Sidrah, A.; Eman, T.; Omar Akhlaq, B.; Shahbaz Ahmad, K.; Saba, M. Evaluation of hypotension and allergic reaction with parenteral drotaverine in a tertiary care hospital. Can. J. App Sci. 2017, 7, 1–4. [Google Scholar]
- Dębski, R.; Niemiec, T.; Mazurek, M.; Dębska, M. Porównanie skuteczności i tolerancji 80 mg Drotaweryny i 400 mg Ibuprofenu u pacjnetek z pierwotnym bolesnym miesiączkowaniem badanie DOROTA. Ginekol. Pol. 2007, 78, 933–938. [Google Scholar] [PubMed]
- Muhammad, M.; Sanaullah, J.; Iqbal Hussain, P.; Muhammad, J. When drotaverine [No-Spa] injected in to the perivascular tissues of internal mammary artery [IMA] relives the peri-operative vascular spasm and increases the blood flow in IMA when used as a pedicle graft in CABG. Med. Forum Mon. 2015, 26, 62–65. [Google Scholar]
- Zakharov, A.G.; Ivanov, L.S.; Khmelevskiĭ, E.V.; Bozhenko, V.K.; Shishkin, A.M. Effect of the drug no-spa on the status of the arterioles in rat skeletal muscles after total gamma-irradiation with a dose of 1 Gy. Biull. Eksp. Biol. Med. 1994, 117, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Lorca, R.A.; Wakle-Prabagaran, M.; Freeman, W.E.; Pillai, M.K.; England, S.K. The large-conductive voltage and Ca2+-activated K+ channel and its v1-subunit modulate mouse uterine artery function during pregnancy. J. Physiol. 2018, 15, 1019–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Time of Administration Drotaverine (90–120 min) | Obstetric History | AFI | Body Weight | Height | Gestation Week | Fertility | RR Systolic | RR Diastolic | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean PI Uta | Correlation Coefficient | 0.25 | −0.06 | 0.23 | −0.07 | 0.17 | −0.27 | 0.13 | −0.29 | −0.24 |
| p-value | 0.16 | 0.76 | 0.19 | 0.7 | 0.34 | 0.12 | 0.48 | 0.11 | 0.19 | |
| % change in CUR | Correlation Coefficient | 0.21 | −0.03 | 0.12 | 0.34 | 0.37 | −0.07 | 0.09 | −0.04 | −0.08 |
| p-value | 0.25 | 0.87 | 0.50 | 0.049 | 0.03 | 0.69 | 0.62 | 0.81 | 0.65 | |
| Change in CUR | Correlation Coefficient | 0.12 | −0.06 | 0.07 | 0.38 | 0.38 | −0.13 | −0.04 | −0.05 | −0.05 |
| p-value | 0.51 | 0.76 | 0.72 | 0.03 | 0.03 | 0.47 | 0.83 | 0.77 | 0.79 |
| Time of Administration Drotaverine (90–120 min) | Obstetric History | AFI | Body Weight | Height | Gestation Week | ||
|---|---|---|---|---|---|---|---|
| Mean PI Uta | Correlation Coefficient | 0.44 | 0.29 | −0.34 | −0.01 | 0.24 | −0.19 |
| p-value | 0.04 | 0.17 | 0.11 | 0.96 | 0.25 | 0.39 | |
| %deltCUR | Correlation Coefficient | 0.16 | −0.06 | 0.20 | 0.39 | 0.42 | −0.18 |
| p-value | 0.46 | 0.78 | 0.36 | 0.06 | 0.04 | 0.4 | |
| deltCUR | Correlation Coefficient | 0.05 | −0.07 | 0.13 | 0.40 | 0.45 | −0.24 |
| p-value | 0.82 | 0.8 | 0.54 | 0.06 | 0.03 | 0.26 |
| Time of Administration Drotaverine (90–120 min) | Obstetric History | AFI | Body Weight | Height | Gestation Week | Fertility | RR Systolic | RR Diastolic | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean PI Uta | Correlation Coefficient | 0.22 | 0.21 | 0.33 | −0.10 | 0.30 | −0.26 | 0.14 | −0.27 | −0.29 |
| p-value | 0.28 | 0.31 | 0.10 | 0.62 | 0.13 | 0.20 | 0.50 | 0.20 | 0.15 | |
| %deltCUR | Correlation Coefficient | 0.30 | −0.02 | 0.01 | 0.44 | 0.37 | −0.11 | 0.12 | −0.05 | 0.22 |
| p-value | 0.13 | 0.94 | 0.97 | 0.03 | 0.06 | 0.58 | 0.57 | 0.83 | 0.29 | |
| 0.29 deltCUR | Correlation Coefficient | 0.18 | −0.05 | 0.02 | 0.47 | 0.40 | −0.16 | −0.01 | −0.05 | −0.05 |
| p-value | 0.37 | 0.83 | 0.91 | 0.02 | 0.04 | 0.43 | 0.95 | 0.81 | 0.8 |
| Time of Administration Drotaverine (90–120 min) | Obstetric History | AFI | Body Weight | Height | Gestation Week | RR Systolic | RR Diastolic | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean PI Uta | Correlation Coefficient | 0.17 | −0.38 | 0.42 | −0.06 | 0.61 | −0.26 | −0.57 | −0.47 |
| p-value | 0.59 | 0.21 | 0.18 | 0.85 | 0.04 | 0.20 | 0.05 | 0.12 | |
| %deltCUR | Correlation Coefficient | −0.05 | 0.30 | 0.14 | 0.33 | −0.44 | −0.35 | −0.12 | −0.15 |
| p-value | 0.88 | 0.35 | 0.66 | 0.30 | 0.15 | 0.26 | 0.72 | 0.63 | |
| deltCUR | Correlation Coefficient | 0.01 | 0.24 | 0.18 | 0.37 | −0.42 | −0.34 | −0.13 | −0.20 |
| p-value | 0.97 | 0.45 | 0.57 | 0.24 | 0.17 | 0.28 | 0.70 | 0.54 |
| Time of Administration Drotaverine (90–120 min) | Obstetric History | AFI | Body Weight | Height | Gestation Week | RR Systolic | RR Diastolic | ||
|---|---|---|---|---|---|---|---|---|---|
| Mean PI Uta | Correlation Coefficient | 0.29 | 0.54 | −0.44 | −0.07 | 0.05 | −0.36 | −0.16 | −0.12 |
| p-value | 0.21 | 0.01 | 0.048 | 0.75 | 0.83 | 0.11 | 0.49 | 0.61 | |
| 0.61%deltCUR | Correlation Coefficient | 0.18 | −0.14 | 0.19 | 0.48 | 0.45 | −0.12 | −0.05 | −0.08 |
| p-value | 0.43 | 0.56 | 0.41 | 0.03 | 0.04 | 0.62 | 0.84 | 0.74 | |
| 0.74 deltCUR | Correlation Coefficient | 0.11 | −0.14 | 0.12 | 0.51 | 0.48 | −0.15 | −0.05 | −0.02 |
| p-value | 0.64 | 0.53 | 0.61 | 0.02 | 0.03 | 0.52 | 0.85 | 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rzymski, P.; Tomczyk, K.M.; Wilczak, M. The Influence of Oral Drotaverine Administration on Materno–Fetal Circulation during the Second and Third Trimester of Pregnancy. Medicina 2022, 58, 235. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020235
Rzymski P, Tomczyk KM, Wilczak M. The Influence of Oral Drotaverine Administration on Materno–Fetal Circulation during the Second and Third Trimester of Pregnancy. Medicina. 2022; 58(2):235. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020235
Chicago/Turabian StyleRzymski, Paweł, Katarzyna Maria Tomczyk, and Maciej Wilczak. 2022. "The Influence of Oral Drotaverine Administration on Materno–Fetal Circulation during the Second and Third Trimester of Pregnancy" Medicina 58, no. 2: 235. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020235