
Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Chemotherapy-Induced Peripheral Neuropathy in Cancer Patients: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Methods
- Primary—patient-reported pain/CIPN with the usage of commonly accepted and validated scales;
- Secondary—patients’ functioning; quality of life; intake of painkillers; adverse events (patients’ safety);
- Two authors, MA and KAT, judged the risk of the following biases in selected articles—selection bias; performance bias; detection bias; attrition bias; reporting bias. The Cochrane Collaboration’s risk of bias tool as described in the Cochrane Handbook for Systematic Review of Interventions was used. Any disagreement was resolved by a discussion between authors until a consensus was reached.
3. Results
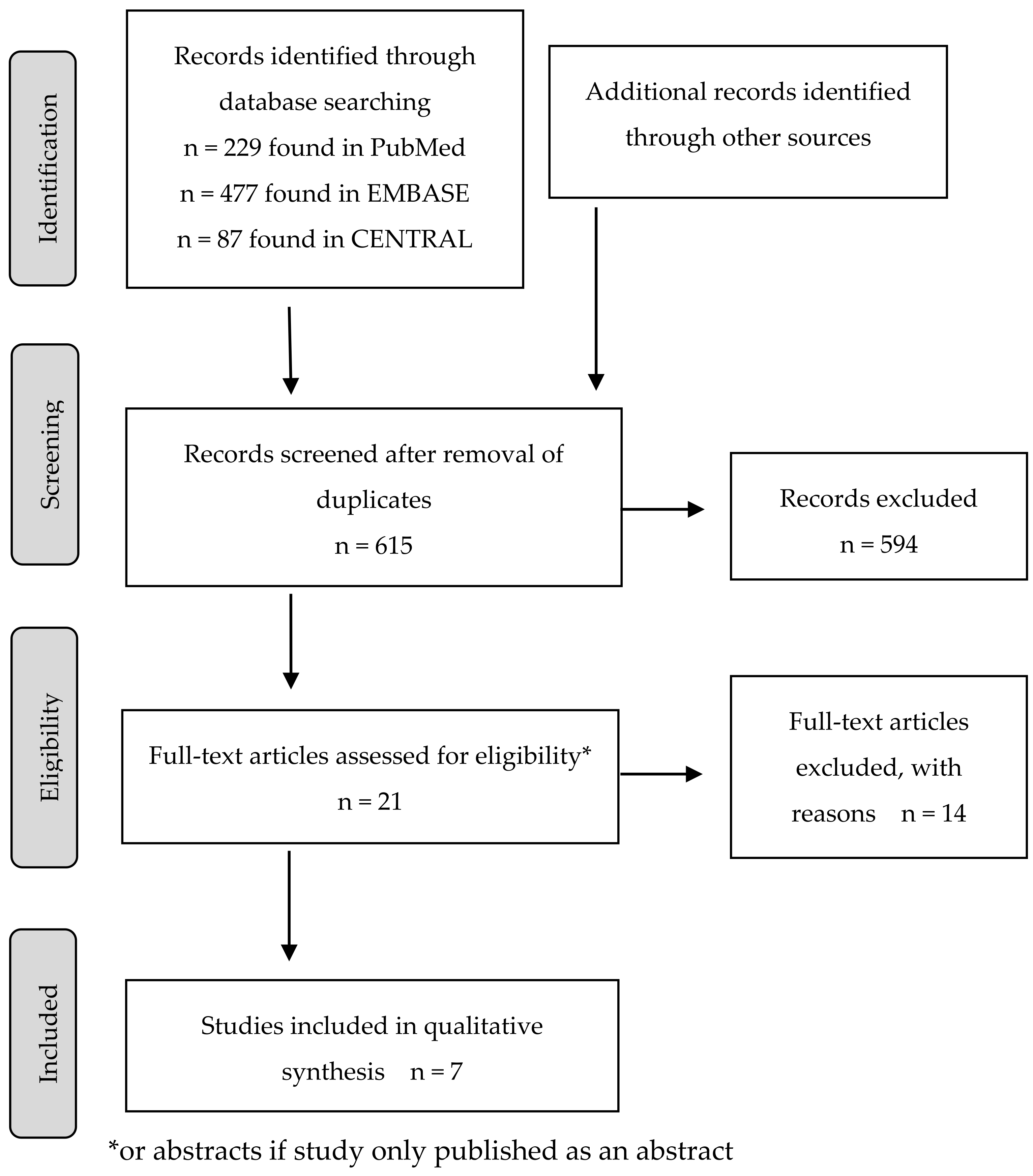
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Type of Studies Included
3.2.2. Patient Population
3.2.3. Details of Pain Treated by Interventions
3.2.4. Characteristics of Interventions
3.2.5. Outcomes
3.2.6. Effects of Intervention
3.3. Risk of Bias
4. Discussion
- TENS cannot be implemented as a standard procedure for pain or CIPN treatment in the cancer patient population;
- TENS can be used in patients with cancer and pain or CIPN, but this decision should be individualized and performed in a multidisciplinary team setting;
- TENS is a safe procedure with a small number of AEs;
- Staff should be trained in terms of what TENS is and where the cancer patients with pain or CIPN not reacting to standard treatment can access this treatment option.
- Patients should be informed about the possibility of using TENS in the case of different types of pain or CIPN not responding to standard treatment;
- Patients should be trained in terms of TENS device usage if they wish to use it;
- Patients should not resign from the standard pain treatment in order to implement TENS;
- If TENS application leads to the lowering of the dose of analgesics, it can be allowed;
- TENS can be applied as a safe and easy-to-use procedure.
- Validated scales (e.g., for pain measurement, HRQoL) should be implemented and patients should be trained in terms of using them;
- Minimal sample size should be counted according to existing suggestions/power calculations should be applied;
- Pain characteristics should be precisely described (pain at rest, on movement, relief in pain, maximal pain intensity, etc.);
- Efforts should be applied to blind a procedure, patients, and staff;
- Short- and long-term AEs should be followed up;
- Follow-up period should be planned;
- TENS settings should be described (e.g., type of device, frequency, intensity, length and frequency of application);
- Planned trials should be multicenter;
- Separate trials regarding the treatment of CIPN should be planned in a cancer patient population.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Minello, C.; George, B.; Allano, G.; Maindet, C.; Burnod, A.; Lemaire, A. Assessing cancer pain-the first step toward improving patients’ quality of life. Support. Care Cancer 2019, 27, 3095–3104. [Google Scholar] [CrossRef]
- Bennett, M.I.; Eisenberg, E.; Ahmedzai, S.H.; Bhaskar, A.; O’Brien, T.; Mercadante, S.; Krčevski Škvarč, N.; Vissers, K.; Wirz, S.; Wells, C.; et al. Standards for the management of cancer-related pain across Europe—A position paper from the EFIC Task Force on Cancer Pain. Eur. J. Pain 2019, 23, 660–668. [Google Scholar] [CrossRef]
- Bjordal, J.M.; Johnson, M.I.; Ljunggreen, A.E. Transcutaneous electrical nerve stimulation (TENS) can reduce postoperative analgesic consumption. A meta-analysis with assessment of optimal treatment parameters for postoperative pain. Eur. J. Pain 2003, 7, 181–188. [Google Scholar] [CrossRef]
- Chwistek, M. Recent advances in understanding and managing cancer pain. F1000Research 2017, 6, 945. [Google Scholar] [CrossRef]
- Loh, J.; Gulati, A. The Use of Transcutaneous Electrical Nerve Stimulation (TENS) in a Major Cancer Center for the Treatment of Severe Cancer-Related Pain and Associated Disability. Pain Med. 2015, 16, 1204–1210. [Google Scholar] [CrossRef] [Green Version]
- Neufeld, N.J.; Elnahal, S.M.; Alvarez, R.H. Cancer pain: A review of epidemiology, clinical quality and value impact. Futur Oncol. 2017, 13, 833–841. [Google Scholar] [CrossRef]
- Cavaletti, G.; Marmiroli, P. Chemotherapy-induced peripheral neurotoxicity. Curr. Opin. Neurol. 2015, 28, 500–507. [Google Scholar] [CrossRef]
- Hou, S.; Huh, B.; Kim, H.K.; Kim, K.-H.; Abdi, S. Treatment of Chemotherapy-Induced Peripheral Neuropathy: Systematic Review and Recommendations. Pain Physician 2018, 21, 571–592. [Google Scholar]
- Salarvand, S.; Hemati, S.; Adibi, P.; Taleghani, F. The quality of guidelines in non-pharmacological prevention and management of chemotherapy-induced neuropathy: A review. Oncol. Rev. 2018, 12, 359. [Google Scholar] [CrossRef]
- Staff, N.P.; Grisold, A.; Grisold, W.; Windebank, A.J. Chemotherapy-induced peripheral neuropathy: A current review. Ann. Neurol. 2017, 81, 772–781. [Google Scholar] [CrossRef]
- Zajączkowska, R.; Kocot-Kępska, M.; Leppert, W.; Wrzosek, A.; Mika, J.; Wordliczek, J. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int. J. Mol. Sci. 2019, 20, 1451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, M. Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and Evidence. Rev. Pain 2007, 1, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Walsh, D. Transcutaneous electrical nerve stimulation: Basic science mechanisms and clinical effectiveness. J. Pain 2003, 4, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Teoli, D.; An, J. Transcutaneous Electrical Nerve Stimulation. Updated 31 August 2021; In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK537188/ (accessed on 2 November 2021).
- Gozani, S.N. Remote Analgesic Effects of Conventional Transcutaneous Electrical Nerve Stimulation: A Scientific and Clinical Review with A Focus on Chronic Pain. J. Pain Res. 2019, 12, 3185–3201. [Google Scholar] [CrossRef] [Green Version]
- Hurlow, A.; Bennett, M.I.; Robb, K.A.; Johnson, M.I.; Simpson, K.H.; Oxberry, S.G. Transcutaneous electric nerve stimulation (TENS) for cancer pain in adults. Cochrane Database Syst. Rev. 2012, 2012, CD006276. [Google Scholar] [CrossRef]
- Gewandter, J.S.; Chaudari, J.; Ibegbu, C.; Kitt, R.; Serventi, J.; Burke, J.; Culakova, E.; Kolb, N.; Sluka, K.A.; Tejani, M.A.; et al. Wireless transcutaneous electrical nerve stimulation device for chemotherapy-induced peripheral neuropathy: An open-label feasibility study. Support. Care Cancer 2019, 27, 1765–1774. [Google Scholar] [CrossRef]
- Lakshman, A.R.; Babu, G.S.; Rao, S. Evaluation of effect of transcutaneous electrical nerve stimulation on salivary flow rate in radiation induced xerostomia patients: A pilot study. J. Cancer Res. Ther. 2015, 11, 229–233. [Google Scholar] [CrossRef]
- Li, W.; Li, D. Effect of electrical stimulation for chemotherapy-induced nausea and vomiting in patients with liver cancer. Medicine 2019, 98, e15255. [Google Scholar] [CrossRef]
- Cameron, M.H.; Lonergan, E.; Lee, H. Transcutaneous Electrical Nerve Stimulation (TENS) for dementia. Cochrane Database Syst. Rev. 2003, 2003, CD004032. [Google Scholar] [CrossRef]
- Robb, K.; Oxberry, S.G.; Bennett, M.I.; Johnson, M.I.; Simpson, K.H.; Searle, R.D. A cochrane systematic review of transcutaneous electrical nerve stimulation for cancer pain. J. Pain Symptom Manage. 2009, 37, 746–753. [Google Scholar] [CrossRef]
- Gibson, W.; Wand, B.M.; Meads, C.; Catley, M.J.; O’Connell, N.E. Transcutaneous electrical nerve stimulation (TENS) for chronic pain—An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 4, CD011890. [Google Scholar] [CrossRef]
- Furness, S.; Bryan, G.; McMillan, R.; Birchenough, S.; Worthington, H.V. Interventions for the management of dry mouth: Non-pharmacological interventions. In: Furness, S., editor. Cochrane Database Syst. Rev. 2013, 2013, CD009603. [Google Scholar] [CrossRef]
- Ezzo, J.; Richardson, M.A.; Vickers, A.; Allen, C.; Dibble, S.; Issell, B.F.; Lao, L.; Pearl, M.; Ramirez, G.; Roscoe, J.; et al. Acupuncture-poInt. stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst. Rev. 2006, 2006, CD002285. [Google Scholar] [CrossRef] [Green Version]
- Ezzo, J.; Richardson, M.A.; Vickers, A.; Allen, C.; Dibble, S.; Issell, B.F.; Lao, L.; Pearl, M.; Ramirez, G.; Roscoe, J.A.; et al. Acupuncture-poInt. stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst. Rev. 2014, 11, CD002285. [Google Scholar] [CrossRef]
- Stein, C.; Eibel, B.; Sbruzzi, G.; Lago, P.D.; Plentz, R.D.M. Electrical stimulation and electromagnetic field use in patients with diabetic neuropathy: Systematic review and meta-analysis. Brazilian J. Phys. Ther 2013, 17, 93–104. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, D.; Caulfield, B.; Lennon, O. The efficacy and prescription of neuromuscular electrical stimulation (NMES) in adult cancer survivors: A systematic review and meta-analysis. Support. Care Cancer 2018, 26, 3985–4000. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Lin, J.; Demner-Fushman, D. Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu. Symp. Proc. 2006, 2006, 359–363. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Gadsby, J.G.; Franks, A.; Jarvis, P.; Dewhurst, F. Acupuncture-like transcutaneous electrical nerve stimulation within palliative care: A pilot study. Complement. Ther. Med. 1997, 5, 13–18. [Google Scholar] [CrossRef]
- Erden, S.; Celik, S.S. The effect of transcutaneous electrical nerve stimulation on post-thoracotomy pain. Contemp. Nurse. 2015, 51, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, M.; Erdogan, A.; Erbil, N.; Karakaya, H.; Demircan, A. Prospective, randomized, placebo-controlled study of the effect of TENS on postthoracotomy pain and pulmonary function. World J. Surg. 2005, 29, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.I.; Johnson, M.I.; Brown, S.R.; Radford, H.; Brown, J.M.; Searle, R.D. Feasibility Study of Transcutaneous Electrical Nerve Stimulation (TENS) for Cancer Bone Pain. J. Pain 2010, 11, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.C.; Issy, A.M.; Sakata, R.K. Assessing the effects of transcutaneous electrical nerve stimulation (TENS) in post-thoracotomy analgesia. Rev. Bras. Anestesiol. 2011, 61, 564–567. [Google Scholar] [CrossRef] [Green Version]
- Fiorelli, A.; Morgillo, F.; Milione, R.; Pace, M.C.; Passavanti, M.B.; Laperuta, P.; Aurilio, C.; Santini, M. Control of post-thoracotomy pain by transcutaneous electrical nerve stimulation: Effect on serum cytokine levels, visual analogue scale, pulmonary function and medication. Eur. J. Cardio-Thoracic Surg. 2012, 41, 861–868. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.E.; Anderson, C.M.; Perkhounkova, Y.; Sleeuwenhoek, B.M.; Louison, R.R. Transcutaneous Electrical Nerve Stimulation Reduces Resting Pain in Head and Neck Cancer Patients. Cancer Nurs 2019, 42, 218–228. [Google Scholar] [CrossRef]
- Robb, K.A.; Newham, D.J.; Williams, J.E. Transcutaneous Electrical Nerve Stimulation vs. Transcutaneous Spinal Electroanalgesia for Chronic Pain Associated with Breast Cancer Treatments. J. Pain Symptom Manage. 2007, 33, 410–419. [Google Scholar] [CrossRef]
- Siemens, W.; Boehlke, C.; Bennett, M.I.; Offner, K.; Becker, G.; Gaertner, J. Transcutaneous electrical nerve stimulation for advanced cancer pain inpatients in specialist palliative care-a blinded, randomized, sham-controlled pilot cross-over trial. Support. Care Cancer. 2020, 28, 5323–5333. [Google Scholar] [CrossRef] [Green Version]
- Paice, J.A.; Portenoy, R.; Lacchetti, C.; Campbell, T.; Cheville, A.; Citron, M.; Constine, L.S.; Cooper, A.; Glare, P.; Keefe, F.; et al. Management of Chronic Pain in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 3325–3345. [Google Scholar] [CrossRef] [Green Version]
- Harris, S.R.; Schmitz, K.H.; Campbell, K.L.; McNeely, M.L. Clinical practice guidelines for breast cancer rehabilitation. Cancer 2012, 118, 2312–2324. [Google Scholar] [CrossRef] [PubMed]
- Electrophysical Agents. Contraindications and Precautions: An Evidence-Based Approach to Clinical Decision Making in Physical Therapy. Physiother. Can. 2010, 62, 1–80. [Google Scholar] [CrossRef] [PubMed]
- Robertson, V.J.; Chipchase, L.S.; Laakso, L.E.; Whelan, K.M.; McKenna, L.J. Guidelines for the Clinical Use of Electrophysical Agents. Australian Physiotherapy Association: Camberwell, VIC, Australia, 2001. Available online: https://espace.library.uq.edu.au/view/UQ:40361, (accessed on 2 November 2021).
- Johnson, M.I.; Claydon, L.S.; Herbison, G.P.; Jones, G.; Paley, C.A. Transcutaneous electrical nerve stimulation (TENS) for fibromyalgia in adults. Cochrane Database Syst. Rev. 2017, 10, CD012172. [Google Scholar] [CrossRef] [PubMed]
- Gibson, W.; Wand, B.M.; O’Connell, N.E. Transcutaneous electrical nerve stimulation (TENS) for neuropathic pain in adults. Cochrane Database Syst. Rev. 2017, 9, CD011976. [Google Scholar] [CrossRef] [Green Version]
- Johnson, M.I.; Mulvey, M.R.; Bagnall, A. Transcutaneous electrical nerve stimulation (TENS) for phantom pain and stump pain following amputation in adults. Cochrane Database Syst. Rev. 2015, 8, CD007264. [Google Scholar] [CrossRef]
- Johnson, M.; Martinson, M. Efficacy of electrical nerve stimulation for chronic musculoskeletal pain: A meta-analysis of randomized controlled trials. Pain 2007, 130, 157–165. [Google Scholar] [CrossRef]
- Rodrigues, J.C.; Avila, M.A.; Driusso, P. Transcutaneous electrical nerve stimulation for women with primary dysmenorrhea: Study protocol for a randomized controlled clinical trial with economic evaluation. PLoS ONE 2021, 16, e0250111. [Google Scholar] [CrossRef]
- Lewis, M.; Chesterton, L.S.; Sim, J.; Mallen, C.D.; Hay, E.M.; van der Windt, D.A. An Economic Evaluation of TENS in Addition to Usual Primary Care Management for the Treatment of Tennis Elbow: Results from the TATE Randomized Controlled Trial. PLoS ONE 2015, 10, e0135460. [Google Scholar] [CrossRef]
- Pivec, R.; Stokes, M.; Chitnis, A.S.; Paulino, C.B.; Harwin, S.F.; Mont, M.A. Clinical and economic impact of TENS in patients with chronic low back pain: Analysis of a nationwide database. Orthopedics 2013, 36, 922–928. [Google Scholar] [CrossRef] [Green Version]
- Bennett, M.I.; Hughes, N.; Johnson, M.I. Methodological quality in randomised controlled trials of transcutaneous electric nerve stimulation for pain: Low fidelity may explain negative findings. Pain 2011, 152, 1226–1232. [Google Scholar] [CrossRef]
- Rakel, B.; Frantz, R. Effectiveness of transcutaneous electrical nerve stimulation on postoperative pain with movement. J. Pain 2003, 4, 455–464. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Topic | Study Inclusion Criteria |
|---|---|
| Population | Adult patients Conformation of malignancy, history of malignancy Confirmed pain or CIPN requiring treatment |
| Intervention | Conventional TENS applied in the area of pain or proximal to the pain over the nerve bundles |
| Comparator | Sham TENS No treatment Standard management for pain or CIPN |
| Outcome | Pain or CIPN intensity or duration measurement with the usage of approved/standard scales |
| Publication methodology | Randomized controlled trials Quasi-randomized controlled trials Controlled clinical trials |
| Publication type | Article or abstract of original study |
| Publication period | Studies published between April 2007 and May 2020 |
| Language restrictions | Only English accepted |
| Robb et al. | Bennett et al. | Erden and Celic | Fiorelli et al. | Ferreira et al. | Lee et al. | Siemens et al. | |
|---|---|---|---|---|---|---|---|
| Year of publication | 2007 | 2010 | 2015 | 2012 | 2011 | 2019 | 2020 |
| Year of conducting the study | UNK | UNK | 2013 | 2008–2010 | UNK | 2011–2012 | 2016–2018 |
| Country | United States | United Kingdom | Turkey | Italy | Brazil | United States | Germany |
| Patient population | 49 | 24 | 40 | 50 | 30 | 41 | 26 |
| Age | 38–60 | UNK1 | 24–76 | UNK1 | 18–60 | 45–79 | UNK 1 |
| Comparator arm | TSE/placebo | Placebo TENS | No treatment | Placebo TENS | Placebo TENS | Placebo TENS/no treatment | Placebo TENS |
| Description of intervention | 12 weeks, with 3 weeks for each type of intervention and 3 weeks of breaks in between (6 arms in total) | 2 × 60 min (placebo and active TENS) with 2–7 days between treatments | Between 24th and 72nd hour after thoracotomy. TENS applied 3 times per day for 30 min, then twice daily till the removal of thoracotomy tube | First 5 days after thoracotomy. For the first 48 h every 4 h for 30 min, later twice daily | A one-time procedure in both arms. One day after the operation, one hour after epidural solution application | Three times for 40–45 min during radiotherapy treatment weeks 4th to 6th | Each procedure for 24 h with 24 h wash-out period in between; continuation of procedure as per patient choice |
| Type of population | Breast cancer female; without active malignancy | With any active malignancy; estimated survival > 4 weeks; with bone pain | Undergoing radical thoracotomy due to lung cancer | Undergoing radical thoracotomy due to lung cancer | Undergoing thoracotomy due to lung cancer | With H&N malignancy; during radiotherapy | With any type of cancer; receiving palliative support; estimated survival > 1 week |
| Crossover | Yes | Yes | No | No | No | Yes | Yes |
| Blinding | Yes | Yes | No | Yes | No | Yes | Yes |
| Drop-outs reported | Yes | Yes | No | Yes | No | Yes | Yes |
| Primary measure (for pain) | Pain report, pain relief, pain interference, anxiety and depression, arm mobility, and analgesic consumption. Time points: 3, 6, and 12 months | Pain intensity at rest and on movement at +60 min | Mean pain levels during rest and coughing at time points of 24 h, 48 h, 72 h, 96 h, 120 h | Pain change assessed on VAS at time points after the surgery | Pain change on VAS after TENS and +1 h, at rest, with change in decubitus moving the upper limbs, and coughing. | Overall pain and pain intensity (reported 30 min after procedure) | Change in pain intensity during the preceding 24 h |
| Main outcomes | No differences for worst pain, least pain, or average pain, pain relief scores from the patients’ pain diaries or BPI. For brief questionnaire, TENS significantly more effective than other arms | The difference in the proportion of patients experiencing at least good pain relief on movement with TENS compared to placebo was statistically significant. No significance was seen when using NRS score for pain intensity and pain relief on movement | TENS group scored significantly better for pain level. At rest, TENS group performed better at time point of +72 h; during coughing, the active group had lower pain level at +48 h, +72 h, and +96 h | Pain assessed on VAS was significantly lower in TENS than in the control group at several time points after the surgery: +6 h, +12 h, +24 h, +48 h, +96 h, and +120 h | Pain severity was significantly lower at rest in active group immediately after TENS application | Resting pain measured by SF-MPQ and VAS decreased more after TENS than placebo/no TENS and the results were statistically significant | Change in pain intensity did not differ between groups. Better responder rates for active TENS as a secondary outcome |
| Type of pain measured | Chronic of min. 6-month duration, treatment-related | Caused by bone metastases from any malignancy. Intensity min. 3/10 NRS | Acute and related to surgical procedure | Acute and related to surgical procedure | Acute and related to surgical procedure | Pain during radiotherapy with intensity of min. 1/10 on NRS | Any, cancer- or treatment-related pain with intensity of min. 3/10 on NRS |
| Scale used for pain assessment | BPI Patients’ diaries A brief questionnaire | VRS, NRS SF-MPQ | VAS | VAS | VAS | VAS SF-MPQ | BPI NRS VRS |
| CIPN allowed | Yes | UNK (no allodynia) | NA | NA | NA | UNK | Yes |
| Function assessment | Yes | No | No | Yes | No | Yes | No |
| AEs assessment | Yes | Yes | No | No | No | No | Yes |
| HRQoL assessment | Yes | No | No | No | No | No | Yes |
| Patients’ satisfaction assessment | Yes | Yes | No | No | No | No | No |
| Analgesics intake evaluation | Yes | No | Yes | Yes | No | No | Yes |
| Follow-up | 12 months | 1 h, then 48 h | 120 h | 120 h | 60 min | UNK | 24 h, then flexible |
| Robb et al.,2007 | Bennett et al.,2010 | Erden and Celic 2015 | Fiorelli et al., 2012 | Ferreira et al., 2011 | Lee et al., 2019 | Siemens et al., 2020 | |
|---|---|---|---|---|---|---|---|
| Random sequence generation (selection bias) | + | + | + | + | + | + | + |
| Allocation concealment (selection bias) | ? | + | − | + | ? | ? | + |
| Blinding participants and personnel (performance bias) | − | − | − | + | − | + | + |
| Blinding outcome assessment (detection bias) | ? | ? | − | + | ? | ? | ? |
| Incomplete outcome data (attrition bias) | ? | + | − | + | − | − | − |
| Selective reporting (reporting bias) | + | + | + | + | + | + | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Püsküllüoğlu, M.; Tomaszewski, K.A.; Grela-Wojewoda, A.; Pacholczak-Madej, R.; Ebner, F. Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Chemotherapy-Induced Peripheral Neuropathy in Cancer Patients: A Systematic Review. Medicina 2022, 58, 284. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020284
Püsküllüoğlu M, Tomaszewski KA, Grela-Wojewoda A, Pacholczak-Madej R, Ebner F. Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Chemotherapy-Induced Peripheral Neuropathy in Cancer Patients: A Systematic Review. Medicina. 2022; 58(2):284. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020284
Chicago/Turabian StylePüsküllüoğlu, Mirosława, Krzysztof A. Tomaszewski, Aleksandra Grela-Wojewoda, Renata Pacholczak-Madej, and Florian Ebner. 2022. "Effects of Transcutaneous Electrical Nerve Stimulation on Pain and Chemotherapy-Induced Peripheral Neuropathy in Cancer Patients: A Systematic Review" Medicina 58, no. 2: 284. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58020284