
Female Patients with Pneumonia on Intensive Care Unit Are under Risk of Fatal Outcome

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
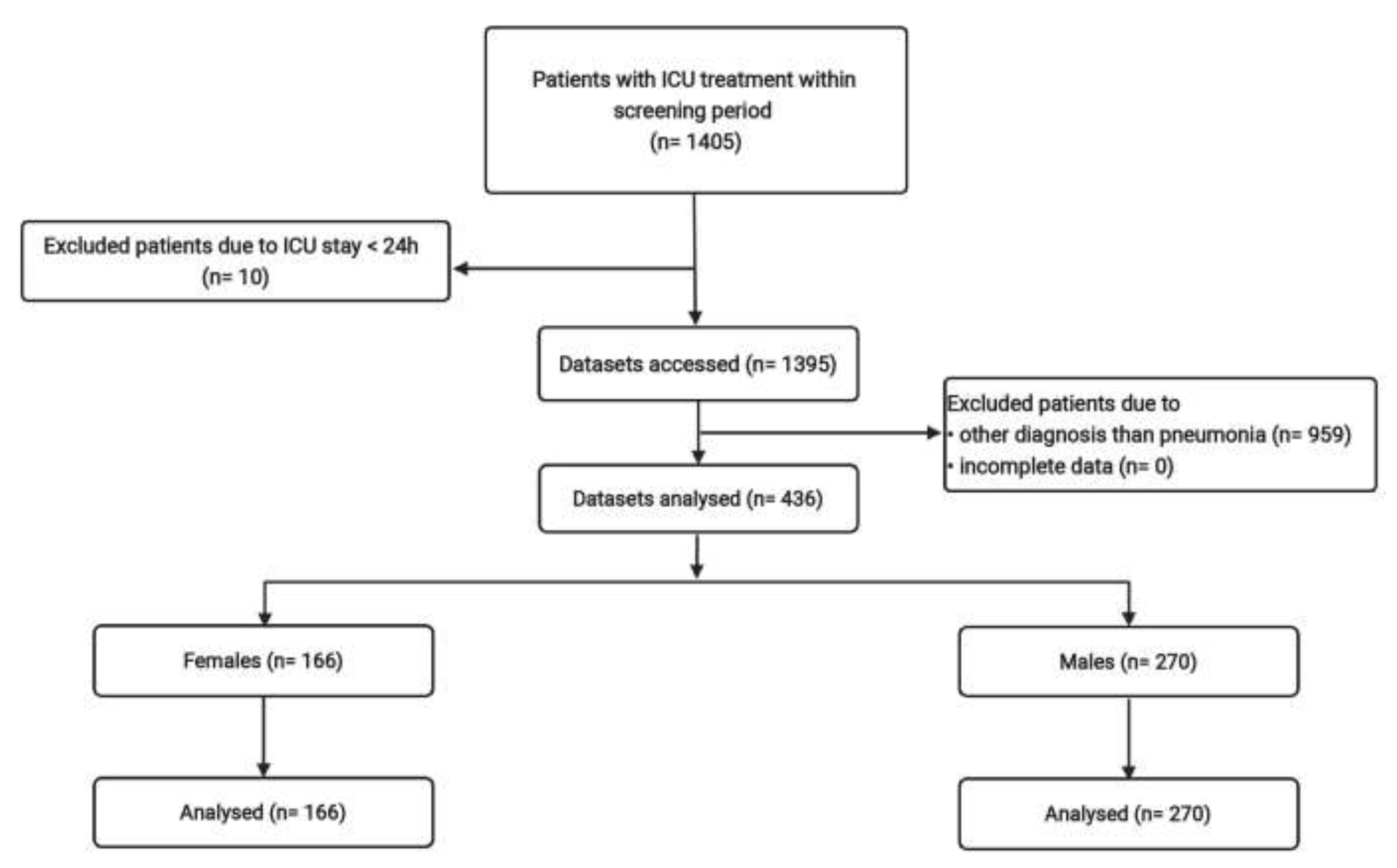
2.1. Study Design, Location and Patients
2.2. Variables
2.3. Statistical Analysis
3. Results
3.1. Basic Characteristics
3.2. Differences of Patient-Centered Care
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAP | Community-acquired pneumonia |
| COPRA | Computer Organized Patient Report Assistant |
| HAP | Hospital-acquired pneumonia |
| IQR | Interquartile range |
| ICU | Intensive care unit |
| PDMS | Patient data management system |
| SOFA | Sequential organ failure assessment |
| SD | Standard deviation |
| SOP | Standard operating procedure |
| VAP | Ventilator-associated pneumonia |
References
- Sharpe, J.P.; Magnotti, L.J.; Weinberg, J.A.; Brocker, J.A.; Schroeppel, T.J.; Zarzaur, B.L.; Fabian, T.C.; Timothy, C.; Croce, M.A. Gender disparity in ventilator-associated pneumonia following trauma: Identifying risk factors for mortality. J. Trauma Acute Care Surg. 2014, 77, 161–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gannon, C.J.; Pasquale, M.; Tracy, J.K.; McCarter, R.J.; Napolitano, L.M. Male gender is associated with increased risk for postinjury pneumonia. Shock 2004, 21, 410–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kollef, M.H.; O’Brien, J.D.; Silver, P. The impact of gender on outcome from mechanical ventilation. Chest 1997, 111, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachtigall, I.; Tafelski, S.; Rothbart, A.; Kaufner, L.; Schmidt, M.; Tamarkin, A.; Kartachov, M.; Zebedies, D.; Trefzer, T.; Wernecke, K.-D.; et al. Gender-related outcome difference is related to course of sepsis on mixed ICUs: A prospective, observational clinical study. Crit. Care 2011, 15, R151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachtigall, I.; Bonsignore, M.; Thürmann, P.; Hohenstein, S.; Jóźwiak, K.; Hauptmann, M.; Eifert, S.; Dengler, J.; Bollmann, A.; Groesdonk, H.V.; et al. Sex Differences in Clinical Course and Intensive Care Unit Admission in a National Cohort of Hos-pitalized Patients with COVID-19. J. Clin. Med. 2021, 10, 4954. [Google Scholar] [CrossRef] [PubMed]
- Ponce-Alonso, M.; Fernández-Félix, B.M.; Halperin, A.; Rodríguez-Domínguez, M.; Sánchez-Díaz, A.M.; Cantón, R.; Muriel, A.; Zamora, J.; Del Campo, R. Propensity-Score Analysis Reveals that Sex Is Not a Prognosis Factor for Mortality in Intensive Care Unit-Admitted Patients with Sepsis. Int. J. Infect. Dis. 2021, 110, 36–44. [Google Scholar] [CrossRef]
- Valentin, A.; Jordan, B.; Lang, T.; Hiesmayr, M.; Metnitz, P.G. Gender-related differences in intensive care: A multiple-center cohort study of therapeutic interventions and outcome in critically ill patients. Crit. Care Med. 2003, 31, 1901–1907. [Google Scholar] [CrossRef]
- Sunden-Cullberg, J.; Nilsson, A.; Inghammar, M. Sex-based differences in ED management of critically ill patients with sepsis: A nationwide cohort study. Intensiv. Care Med. 2020, 46, 727–736. [Google Scholar] [CrossRef] [Green Version]
- Fowler, R.A.; Sabur, N.; Li, P.; Juurlink, D.N.; Pinto, R.; Hladunewich, M.A.; Adhikari, N.K.; Sibbald, W.J.; Martin, C.M. Sex-and age-based differences in the delivery and outcomes of critical care. Can. Med Assoc. J. 2007, 177, 1513–1519. [Google Scholar] [CrossRef] [Green Version]
- Bolego, C.; Poli, A.; Paoletti, R. Smoking and gender. Cardiovasc. Res. 2002, 53, 568–576. [Google Scholar] [CrossRef] [Green Version]
- Johnston, N.; Jönelid, B.; Christersson, C.; Kero, T.; Renlund, H.; Schenck-Gustafsson, K.; Lagerqvist, B. Effect of Gender on Patients With ST-Elevation and Non-ST-Elevation Myocardial Infarction without Obstructive Coronary Artery Disease. Am. J. Cardiol. 2015, 115, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- Baumhäkel, M.; Müller, U.; Böhm, M. Influence of gender of physicians and patients on guideline-recommended treatment of chronic heart failure in a cross-sectional study. Eur. J. Heart Fail. 2009, 11, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Rosano, G.M.C.; Spoletini, I.; Vitale, C. Cardiovascular disease in women, is it different to men? The role of sex hormones. Climacteric 2017, 20, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Al-Lami, R.A.; Urban, R.J.; Volpi, E.; Algburi, A.M.A.; Baillargeon, J. Sex Hormones and Novel Corona Virus Infectious Disease (COVID-19). Mayo Clin. Proc. 2020, 95, 1710–1714. [Google Scholar] [CrossRef]
- Kristensen, M.L.; Vestergaard, T.R.; Bülow, H.-H. Gender differences in randomised, controlled trials in intensive care units. Acta Anaesthesiol. Scand. 2014, 58, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Caceres, F.; Welch, V.L.; Kett, D.H.; Scerpella, E.G.; Peyrani, P.; Ford, K.D.; Ramirez, J.A.; The IMPACT-HAP Study Group. Absence of Gender-Based Differences in Outcome of Patients with Hospital-Acquired Pneumonia. J. Women’s Health 2013, 22, 1069–1075. [Google Scholar] [CrossRef]
- Zettersten, E.; Jäderling, G.; Larsson, E.; Bell, M. The impact of patient sex on intensive care unit admission: A blinded randomized survey. Sci. Rep. 2019, 9, 14222. [Google Scholar] [CrossRef]
- Nouri-Pasovsky, P.A.; Nachtigall, I.; Krannich, A.; Spies, C.; Tafelski, S. Evaluation of sex-associated differences in validity of the SOFA score in ICU patients. Ital. J. Gend. Specif. Med. 2021, 7, 7–14. [Google Scholar]
- Whitacre, C.C. Sex differences in autoimmune disease. Nat. Immunol. 2001, 2, 777–780. [Google Scholar] [CrossRef] [PubMed]
- Voskuhl, R. Sex differences in autoimmune diseases. Biol. Sex Differ. 2011, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Epstein, S.K.; Vuong, V. Lack of Influence of Gender on Outcomes of Mechanically Ventilated Medical ICU Patients. Chest 1999, 116, 732–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combes, A.; Luyt, C.E.; Trouillet, J.L.; Nieszkowska, A.; Chastre, J. Gender impact on the outcomes of critically ill patients with nosocomial infections. Crit. Care Med. 2009, 37, 2506–2511. [Google Scholar] [CrossRef] [PubMed]
- Pietropaoli, A.P.; Glance, L.G.; Oakes, D.; Fisher, S.G. Gender differences in mortality in patients with severe sepsis or septic shock. Gend. Med. 2010, 7, 422–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikby, A.; Månsson, I.A.; Johansson, B.; Strindhall, J.; Nilsson, S.E. The immune risk profile is associated with age and gender: Findings from three Swedish population studies of individuals 20–100 years of age. Biogerontology 2008, 9, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.H. The Complex Role of Estrogens in Inflammation. Endocr. Rev. 2007, 28, 521–574. [Google Scholar] [CrossRef] [Green Version]
- Sarchielli, E.; Guarnieri, G.; Idrizaj, E.; Squecco, R.; Mello, T.; Comeglio, P.; Gallina, P.; Maggi, M.; Vannelli, G.B.; Morelli, A. The G protein-coupled oestrogen receptor, GPER1, mediates direct anti-inflammatory effects of oestrogens in human cholinergic neurones from the nucleus basalis of Meynert. J. Neuroendocrinol. 2020, 32, e12837. [Google Scholar] [CrossRef]
- Wang, Y.; Cela, E.; Gagnon, S.; Sweezey, N.B. Estrogen aggravates inflammation in Pseudomonas aeruginosa pneumonia in cystic fibrosis mice. Respir. Res. 2010, 11, 166. [Google Scholar] [CrossRef] [Green Version]
- Jansson, L.; Holmdahl, R. Estrogen-mediated immunosuppression in autoimmune diseases. Agents Actions 1998, 47, 290–301. [Google Scholar] [CrossRef]
- Angele, M.K.; Pratschke, S.; Hubbard, W.J.; Chaudry, I.H. Gender differences in sepsis: Cardiovascular and immunological aspects. Virulence 2014, 5, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender differences in patients with COVID-19: Focus on severity and mortality. Front. Public Health 2020, 152, 8. [Google Scholar] [CrossRef] [PubMed]
- Channappanavar, R.; Fett, C.; Mack, M.; Ten Eyck, P.P.; Meyerholz, D.K.; Perlman, S. Sex-Based Differences in Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Infection. J. Immunol. 2017, 198, 4046–4053. [Google Scholar] [CrossRef] [PubMed]
- Kadioglu, A.; Cuppone, A.M.; Trappetti, C.; List, T.; Spreafico, A.; Pozzi, G.; Andrew, P.W.; Oggioni, M.R. Sex-Based Differences in Susceptibility to Respiratory and Systemic Pneumococcal Disease in Mice. J. Infect. Dis. 2011, 204, 1971–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, J.; Jung, N.; Robinson, N.; Lehmann, C. Sex differences in immune responses to infectious diseases. Infection 2015, 43, 399–403. [Google Scholar] [CrossRef]
- Hertz, D.; Schneider, B. Sex differences in tuberculosis. Semin. Immunopathol. 2018, 41, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Todorov, A.; Kaufmann, F.; Arslani, K.; Haider, A.; Bengs, S.; Goliasch, G.; Zellweger, N.; Tontsch, J.; Sutter, R.; Buddeberg, B.; et al. Gender dif-ferences in the provision of intensive care: A Bayesian approach. Intensive Care Med. 2021, 47, 577–587. [Google Scholar] [CrossRef]
- Samuelsson, C.; Sjöberg, F.; Karlström, G.; Nolin, T.; Walther, S.M. Gender differences in outcome and use of resources do exist in Swedish intensive care, but to no advantage for women of premenopausal age. Crit. Care 2015, 19, 129. [Google Scholar] [CrossRef] [Green Version]
- Denny, K.J.; Gartside, J.G.; Alcorn, K.; Cross, J.W.; Maloney, S.; Keijzers, G. Appropriateness of antibiotic prescribing in the Emergency Department. J. Antimicrob. Chemother. 2018, 74, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.S.; Baird, D.D.; Rebecca Darden, F. Measures of menopausal status in relation to demographic, reproductive, and behavioral characteristics in a population-based study of women aged 35–49 years. Am. J. Epidemiol. 2001, 153, 1159–1165. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | Female | Male | p-Value |
|---|---|---|---|
| N = 166 | N = 270 | ||
| Age in years a | 65.1 ± 14.8 | 62.4 ± 15.3 | 0.116 |
| Median b | 68 (57–77) | 67 (52–74) | |
| Initial SAPS Score a | 42.8 ± 18.2 | 42.2 ± 15.8 | 0.899 |
| Median b | 41 (29–54.3) | 41 (31–53) | |
| Initial SOFA Score a | 5.5 ± 4 | 6.5 ± 4.1 | 0.011 |
| Median b | 5.5 (2–8) | 6 (4–9) | |
| Initial TISS-28 Score a | 35.6 ± 11.1 | 36.9 ± 11.1 | 0.317 |
| Median b | 36 (27.8–44.2) | 36.5 (28–44.3) | |
| Immune supression | 21 (12.7) | 18 (6.7) | 0.039 |
| Cardiovascular illness | 63 (38) | 143 (53) | 0.003 |
| Pulmonary illness | 39 (23.5) | 58 (21.5) | 0.637 |
| Chronic liver disease | 17 (10.2) | 31 (11.5) | 0.754 |
| Chronische kidney insufficiency | 37 (22.3) | 68 (25.2) | 0.564 |
| Diabetes mellitus | 85 (51.2) | 114 (42.2) | 0.075 |
| Type of pneumonia n (%) | |||
| CAP (%) | 27 (16.3) | 33 (12.2) | 0.254 |
| HAP (%) | 102 (61.4) | 167 (61.9) | >0.999 |
| VAP (%) | 48 (28.9) | 92 (34.1) | 0.291 |
| Germ spectrum n (%) | |||
| Fungi | 57 (34.3) | 101 (37.4) | 0.539 |
| Germ with enhanced resistence potential (%) | 31 (18.7) | 51 (18.9) | >0.999 |
| Gramnegative germ (%) | 58 (34.9) | 123 (45.6) | 0.035 |
| Variable | Female | Male | p-Value |
|---|---|---|---|
| n = 166 | n = 270 | ||
| Adherence to SOP a | 63.5 ± 34.6 | 67.2 ± 30.1 | 0.531 |
| Median b | 70 (40–100) | 71 (47–100) | |
| Daily dose of antibiotics in substances per day a | 1.1 ± 0.7 | 1.3 ± 0.7 | 0.028 |
| Median b | 1 (0.6–1.5) | 1.2 (0.8–1.8) | |
| Antibiotic-free days a | 33.7 ± 28.7 | 28.5 ± 25.0 | 0.104 |
| Median b | 30.6 (9.1–50.0) | 25.0 (7.3–44.5) | |
| Operated microbiologic diagnostic (sum) a | 6 ± 7.3 | 6.9 ± 8.3 | 0.197 |
| Median b | 4 (1–9) | 4 (1–11) | |
| Operated radiologic diagnostic (sum) a | 7.4 ± 6.7 | 8.4 ± 7.1 | 0.077 |
| Median b | 5 (3–9) | 6 (3–11) | |
| Calculated antibiotic/LOS g in d a, h | 0.5 ± 0.3 | 0.5 ± 0.3 | 0.146 |
| Medianb | 0.5 (0.3–0.8) | 0.4 (0.2–0.7) | |
| Targeted antibiotic therapy LOS g in d a, h | 0.2 ± 0.3 | 0.3 ± 0.3 | 0.016 |
| Median b | 0 (0–0.3) | 0.1(0–0.5) | |
| ICU mortality (%) | 34 (20.5) | 39 (14.4) | 0.113 |
| ICU LOS g in d a | 17.9 ± 14.4 | 18.4 ± 15.6 | 0.891 |
| Median b | 13 (8–25) | 14 (7–24) | |
| Mechanical ventilation (%) | 142 (85.5) | 252 (93.3) | 0.011 |
| Durance of mechanical ventilation in h a | 295 ± 349 | 306 ± 489 | 0.919 |
| Median b | 161 (30–466) | 157 (36–392) | |
| ICU mortality (%) | 34 (20.5) | 39 (14.4) | 0.113 |
| Univariate Analysis c | Multivariate Analysis d | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Sex (♀ Female vs. ♂ Male) | 0.655 (0.395–1.088) | 0.103 | 1.775 (1.029–3.062) | 0.039 |
| Age | 1.018 (0.0996–1037) | 0.055 | 1.025 (1.006–1.046) | 0.014 |
| Scores at Hospital Admittance | ||||
| Initial SAPS | 1.033 (1.017–1.049) | <0.001 | ||
| Initial SOFA | 1.128 (1.061–1.200) | <0.001 | 1.139 (1.063–1.220) | <0.001 |
| Initial TISS | 1.060 (1.034–1.086) | <0.001 | ||
| Comorbidities | ||||
| Immune suppression | 1.097 (0.464–2.591) | 0.833 | ||
| Cardiovascular comorbidities | 0.968 (0.585–1.602) | 0.900 | ||
| Pulmonary comorbidities | 1.946 (1.121–3.378) | 0.018 | 1.598 (0.886–2.883) | 0.119 |
| Type of Pneumonia | ||||
| Early and late onset HAP | 0.580 (0.350–0.963) | 0.0354 | 0.799 (0.390–1.633) | 0.538 |
| SCAP | 0.860 (0.403–1.836) | 0.697 | ||
| VAP | 1.974 (1.182–3.297) | 0.009 | 1.431 (0.672–3.048) | 0.353 |
| Coinfections | ||||
| Abdominal infections | 1.750 (0.786–3.896) | 0.171 | ||
| Urogenital infections | 0.994 (0.423–2.334) | 0.989 | ||
| Bone-/joint infections | 1.513 (0.406–5.638) | 0.537 | ||
| Endocarditis | 0.994 (0.213–4.636) | 0.994 | ||
| Wound/ soft tissue infections (%) | 1.864 (0.956–3.632) | 0.067 | 1.816 (0.850–3.878) | 0.123 |
| Meningitis | 0.702 (0.156–3.158) | 0.645 | ||
| Focus not identified | 0.896 (0.361–2.222) | 0.812 | ||
| Catheter infection | 1.644 (0.675–4.005) | 0.274 | ||
| Pseudomembranousus Colitis | 1.250 (0.260–6.010) | 0.781 | ||
| Germ Spectrum | ||||
| Fungi | 1.680 (1.011–2.794) | 0.045 | 1.130 (0.643–1.986) | 0.671 |
| Germ with enhanced resistance potential (%) | 1.675 (0.930–3.020) | 0.086 | 1.145 (0.581–2.258) | 0.696 |
| Gramnegative germ (%) | 1.369 (0.826–2.268) | 0.223 | ||
| SOP-Adherence | ||||
| SOP adherence > 70 (%) | 0.768 (0.464–1.272) | 0.305 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koerber, M.K.; Agaoglu, S.; Bichmann, A.; Tafelski, S.; Nachtigall, I. Female Patients with Pneumonia on Intensive Care Unit Are under Risk of Fatal Outcome. Medicina 2022, 58, 827. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060827
Koerber MK, Agaoglu S, Bichmann A, Tafelski S, Nachtigall I. Female Patients with Pneumonia on Intensive Care Unit Are under Risk of Fatal Outcome. Medicina. 2022; 58(6):827. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060827
Chicago/Turabian StyleKoerber, Mareike Kristina, Sarah Agaoglu, Anna Bichmann, Sascha Tafelski, and Irit Nachtigall. 2022. "Female Patients with Pneumonia on Intensive Care Unit Are under Risk of Fatal Outcome" Medicina 58, no. 6: 827. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina58060827