
A Comparative Study on the Clinical Efficacy of Simple Transobturator Midurethal Sling and Posterior Pelvic Floor Reconstruction
 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Object
2.2. Methods
2.2.1. Preoperative Preparation
2.2.2. Method of Tension Free Sling Suspension via Obturator
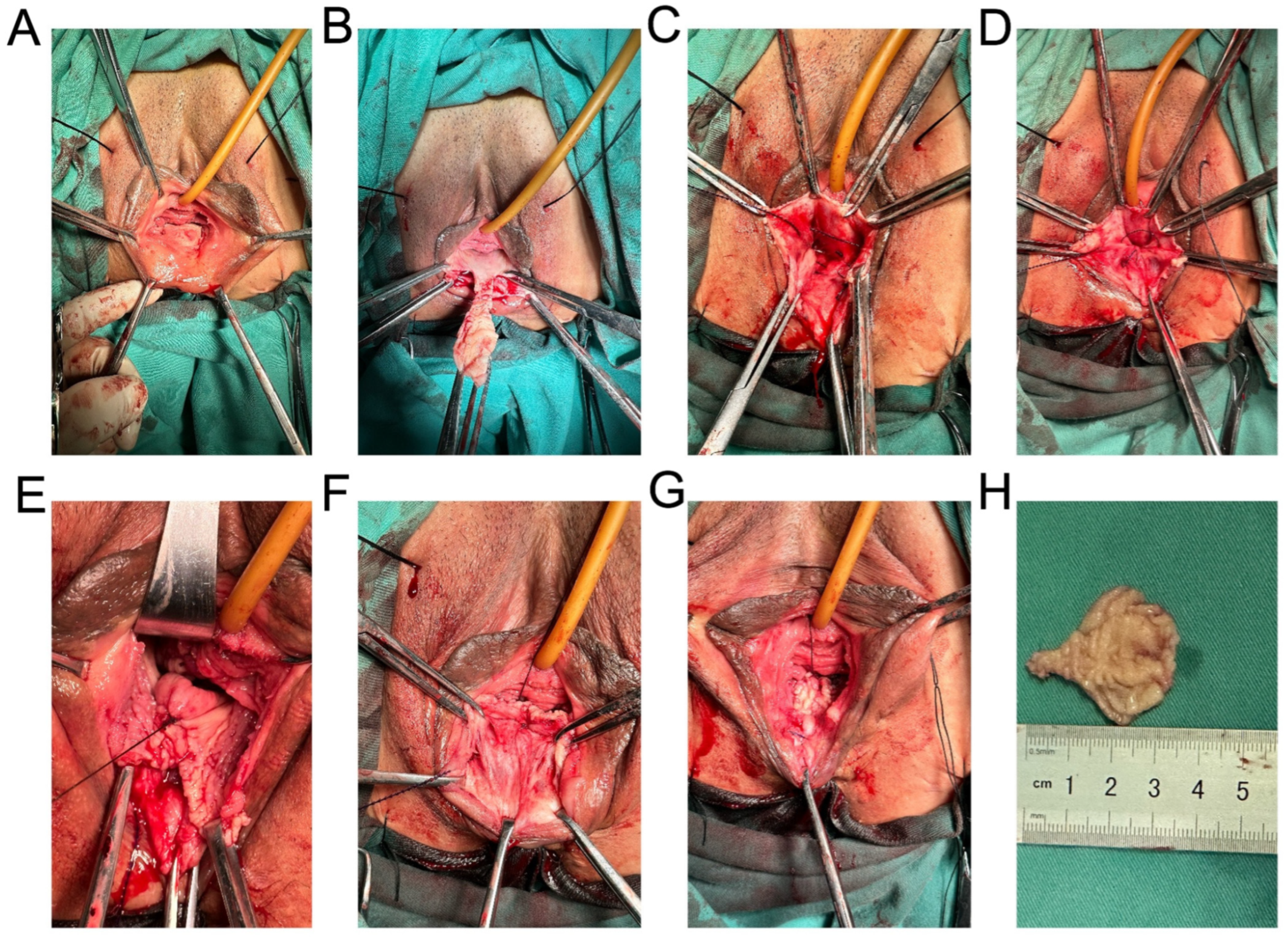
2.2.3. Methods of Posterior Pelvic Floor Reconstruction
2.2.4. Follow-Up Observation
3. Results
3.1. Perioperative Indicators
3.2. Surgical Complications
3.3. Clinical Efficacy
4. Discussion
4.1. Comparison of Therapeutic Effects of TOT and TOT Combined with Pelvic Floor Reconstruction
4.2. Comparison of Complications of TOT and TOT Combined with Pelvic Floor Reconstruction
4.3. Mechanism of Female Continence and Role of Posterior Pelvis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jaekel, A.K.; Kirschner-Hermanns, R.; Knüpfer, S.C. Diagnostic testing of female urinary incontinence: Dos and dont’s. Aktuelle Urol. 2021, 52, 237–244. [Google Scholar] [CrossRef]
- Good, M.M.; Solomon, E.R. Pelvic Floor Disorders. Obstet. Gynecol. Clin. North Am. 2019, 46, 527–540. [Google Scholar] [CrossRef]
- Chen, Z.; Wang, J.; Zhou, R.; Chen, R.; Sun, X.; Du, W.; Zhu, H. Efficacy and safety of transvaginal anterior pelvic reconstruction with mesh in treatment of cystocele with lower urinary tract symptoms. Chin. J. Urol. 2020, 41, 613–618. [Google Scholar] [CrossRef]
- Ulmsten, U.; Petros, P. Intravaginal slingplasty (IVS): An ambulatory surgical procedure for treatment of female urinary incontinence. Scand. J. Urol. Nephrol. 1995, 29, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Bandarian, M.; Ghanbari, Z.; Asgari, A. Comparison of transobturator tape (TOT) vs Burch method in treatment of stress urinary incontinence. J. Obstet. Gynaecol. 2011, 31, 518–520. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Liu, B.; Lv, T.; Wen, W.; Meng, X.; Li, X.; Xu, Z.; Chen, Y.; Pan, T. A multicenter clinical study of comparing the efficacy of two mid-urethral slings in the treatment of female stress urinary incontinence. Chin. J. Urol. 2020, 12, 368–373. [Google Scholar] [CrossRef]
- Petros, P. The Female Pelvic Floor: Function, Dysfunction and Management According to the Integral Theory; Division of Urology, PENN Medicine: Philadelphia, PA, USA, 2006. [Google Scholar]
- Lee, E.; Nitti, V.W.; Brucker, B.M. Midurethral slings for all stress incontinence: A urology perspective. Urol. Clin. North Am. 2012, 39, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Manonai, J.; Mouritsen, L.; Palma, P.; Contreras-Ortiz, O.; Korte, J.E.; Swift, S. The inter-system association between the simplified pelvic organ prolapse quantification system (S-POP) and the standard pelvic organ prolapse quantification system (POPQ) in describing pelvic organ prolapse. Int. Urogynecol. J. 2011, 22, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Kim, J.H.; Chae, H.D.; Chung, J.H.; Kim, H.J.; Lee, S.R.; Kim, S.H. Surgical outcomes of tension-free vaginal tape (TVT)- abbrevo® and TVT-obturator® for the treatment of stress urinary incontinence: A retrospective study. Obstet. Gynecol. Sci. 2021, 64, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Natale, F.; Illiano, E.; Marchesi, A.; La Penna, C.; Costantini, E. Transobturator Tape: Over 10 Years Follow-up. Urology 2019, 129, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Costantini, E.; Kocjancic, E.; Lazzeri, M.; Giannantoni, A.; Zucchi, A.; Carbone, A.; Bini, V.; Palleschi, G.; Pastore, A.L.; Porena, M. Long-term efficacy of the trans-obturator and retropubic mid-urethral slings for stress urinary incontinence: Update from a randomized clinical trial. World J. Urol. 2016, 34, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Jun, T.; Yoon, H.S.; Kim, H.S.; Lee, J.W.; Bae, J.; Lee, H.W. Recurrence rate of stress urinary incontinence in females with initial cure after transobturator tape procedure at 3-year follow-up. Investig. Clin. Urol. 2017, 58, 54. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Keji, X.; Shaolin, Z. Meta analysis of the short-term effect of Ajust single incision micro sling versus TVT-O/TOT in the stress urinary incontinence. Chin. J. Urol. 2015, 30, 927–933. [Google Scholar] [CrossRef]
- Athanasopoulos, A.; Perimenis, P.; Giannitsas, K.; Markou, S.; Gyftopoulos, K.; Fisfis, J.; Liatsikos, E.; Barbalias, G. The relationship between the perineal length measurements and the urodynamic stress incontinence. Int. Urol. Nephrol. 2005, 37, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Ogah, J.; Cody, J.D.; Rogerson, L. Minimally invasive synthetic suburethral sling operations for stress urinary incontinence in women. Cochrane Database Syst. Rev. 2009, 4, CD006375. [Google Scholar] [CrossRef]
- Durnea, C.M.; Khashan, A.S.; Kenny, L.C.; Tabirca, S.S.; O’Reilly, B.A. The role of prepregnancy pelvic floor dysfunction in postnatal pelvic morbidity in primiparous women. Int. Urogynecol. J. 2014, 25, 1363–1374. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | TOT | TOT Combined with Pelvic Floor Reconstruction | p Value |
|---|---|---|---|
| Age (mean ± SD, y) | 52.92 ± 11.52 | 50.43 ± 10.24 | <0.05 |
| BMI (mean ± SD, kg/m2) | 23.55 ± 2.93 | 23.92 ± 3.04 | >0.05 |
| Number of pregnancies (mean ± SD, times) | 3.11 ± 1.40 | 3.47 ± 1.47 | <0.05 |
| Hospital stay (mean ± SD, d) | 2.06 ± 0.74 | 3.93 ± 1.05 | <0.05 |
| Operation time (mean ± SD, min) | 20.5 ± 11.4 | 61.04 ± 7.64 | <0.05 |
| Blood loss (mean ± SD, mL) | 21.5 ± 12.9 | 20.77 ± 10.65 | >0.05 |
| Characteristics | TOT | TOT Combined with Pelvic Floor Reconstruction | p Value |
|---|---|---|---|
| Bladder injury | 1/191 (0.52%) | 0/151 (0%) | >0.05 |
| Injury of vaginal wall | 2/191 (1.05%) | 0/151 (0%) | >0.05 |
| Retropubic hematoma | 0/191 (0%) | 0/151 (0%) | >0.05 |
| Incision infection | 0/191 (0%) | 0/151 (0%) | >0.05 |
| Urinary tract infection | 1/191 (0.52%) | 1/151 (0.66%) | >0.05 |
| Dysuria | 12/191 (6.28%) | 3/151 (0.66%) | >0.05 |
| Leg pain | 2/191 (1.05%) | 0/151 (0%) | >0.05 |
| Postoperative constipation | 2/191 (1.05%) | 0/151 (0%) | >0.05 |
| Exposed sling | 0/191 (0%) | 0/151 (0%) | >0.05 |
| Characteristics | TOT | TOT Combined with Pelvic Floor Reconstruction | p Value |
|---|---|---|---|
| Cure rate | 165/191 (86.39%) | 137/151 (90.73%) | >0.05 |
| Effective rate | 173/191 (90.58%) | 143/151 (94.79%) | >0.05 |
| Reoperation rate | 4/191 (2.09%) | 3/151 (1.99%) | >0.05 |
| Patient satisfaction rate | 187/191 (97.90%) | 148/151 (98.01%) | >0.05 |
| Complete success rate | 153/191 (80.10%) | 139/151 (92.05%) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, D.; Gao, Z.; Zhou, H.; Lin, H.; Wang, X.; Li, L.; Yang, X.; Wen, Y.; Zhang, Q.; Shen, J. A Comparative Study on the Clinical Efficacy of Simple Transobturator Midurethal Sling and Posterior Pelvic Floor Reconstruction. Medicina 2023, 59, 155. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59010155
Tian D, Gao Z, Zhou H, Lin H, Wang X, Li L, Yang X, Wen Y, Zhang Q, Shen J. A Comparative Study on the Clinical Efficacy of Simple Transobturator Midurethal Sling and Posterior Pelvic Floor Reconstruction. Medicina. 2023; 59(1):155. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59010155
Chicago/Turabian StyleTian, Daoming, Zhenhua Gao, Hang Zhou, Han Lin, Xingqi Wang, Ling Li, Xunguo Yang, Yubin Wen, Quan Zhang, and Jihong Shen. 2023. "A Comparative Study on the Clinical Efficacy of Simple Transobturator Midurethal Sling and Posterior Pelvic Floor Reconstruction" Medicina 59, no. 1: 155. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59010155