

Electromyographic Evaluation of Muscle Activity in Patients Rehabilitated with Full Arch Fixed Implant-Supported Prostheses
 , ,
, ,  and
and
Abstract
:1. Introduction
- The first hypothesis was that the EMG activity would change over time due to the neuromuscular adaptation of the patients to newly inserted prostheses.
- The second hypothesis was that EMG activity in edentulous subjects is higher than in dentate ones due to the lack of periodontal mechano-receptors.
- The third hypothesis was that EMG activity in rehabilitated patients with fixed implant-supported prostheses is higher during mastication in comparison to the control (dentate) group.
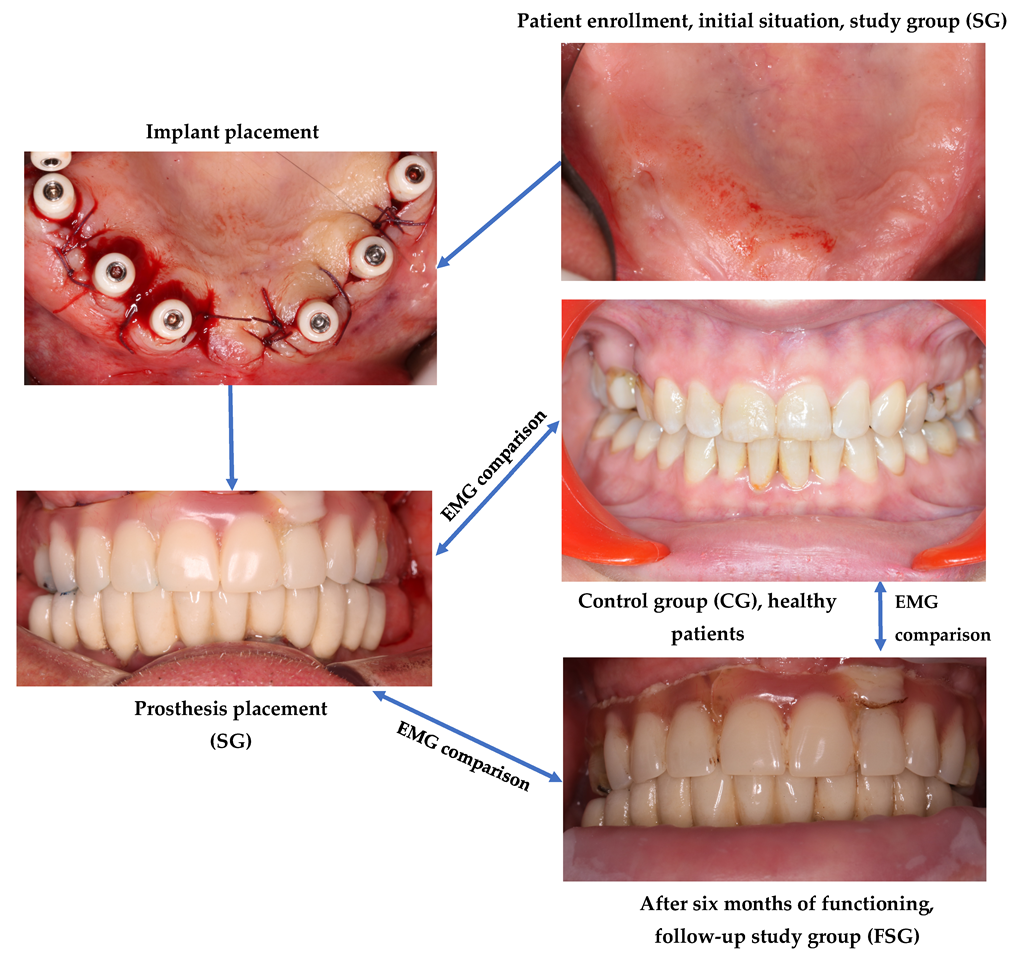
2. Materials and Methods
3. Results
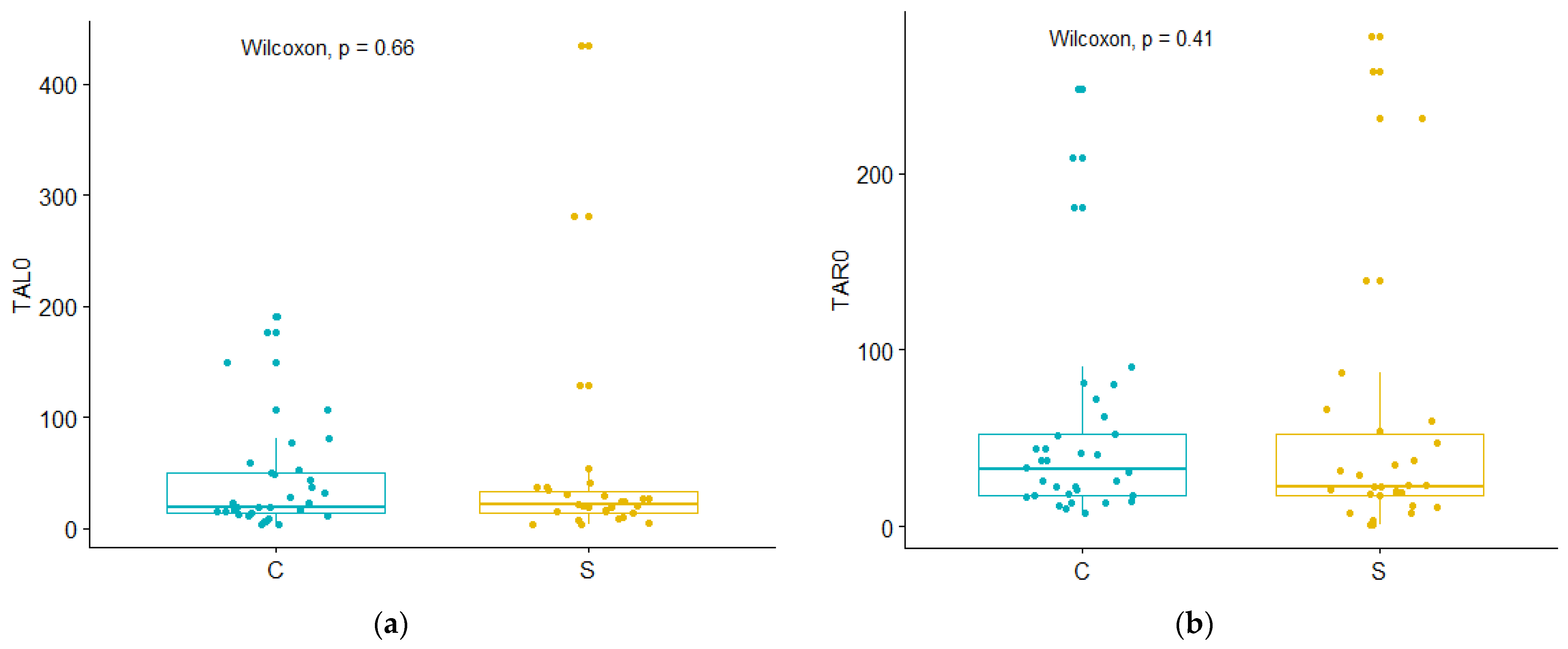
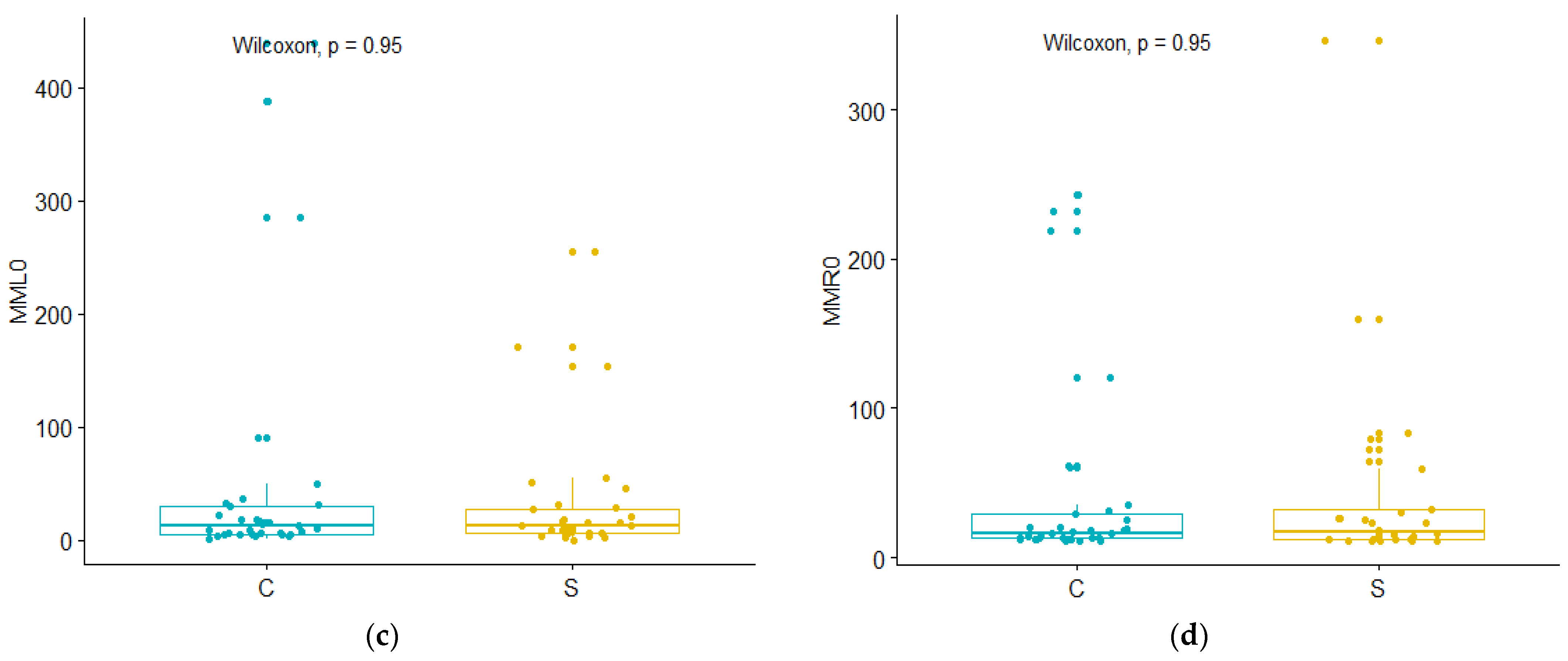
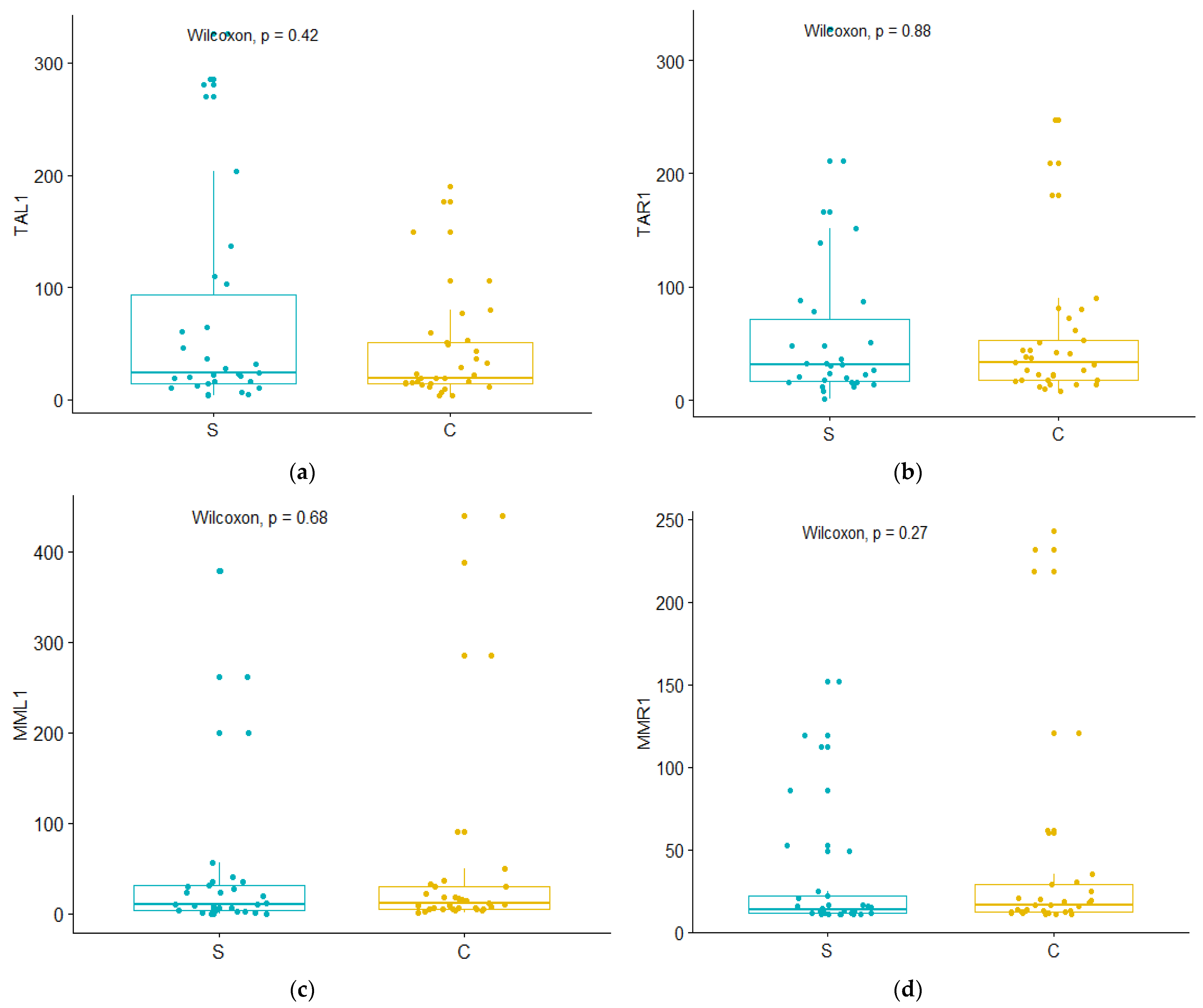
3.1. Study Group (SG) vs. Control Group (CG)
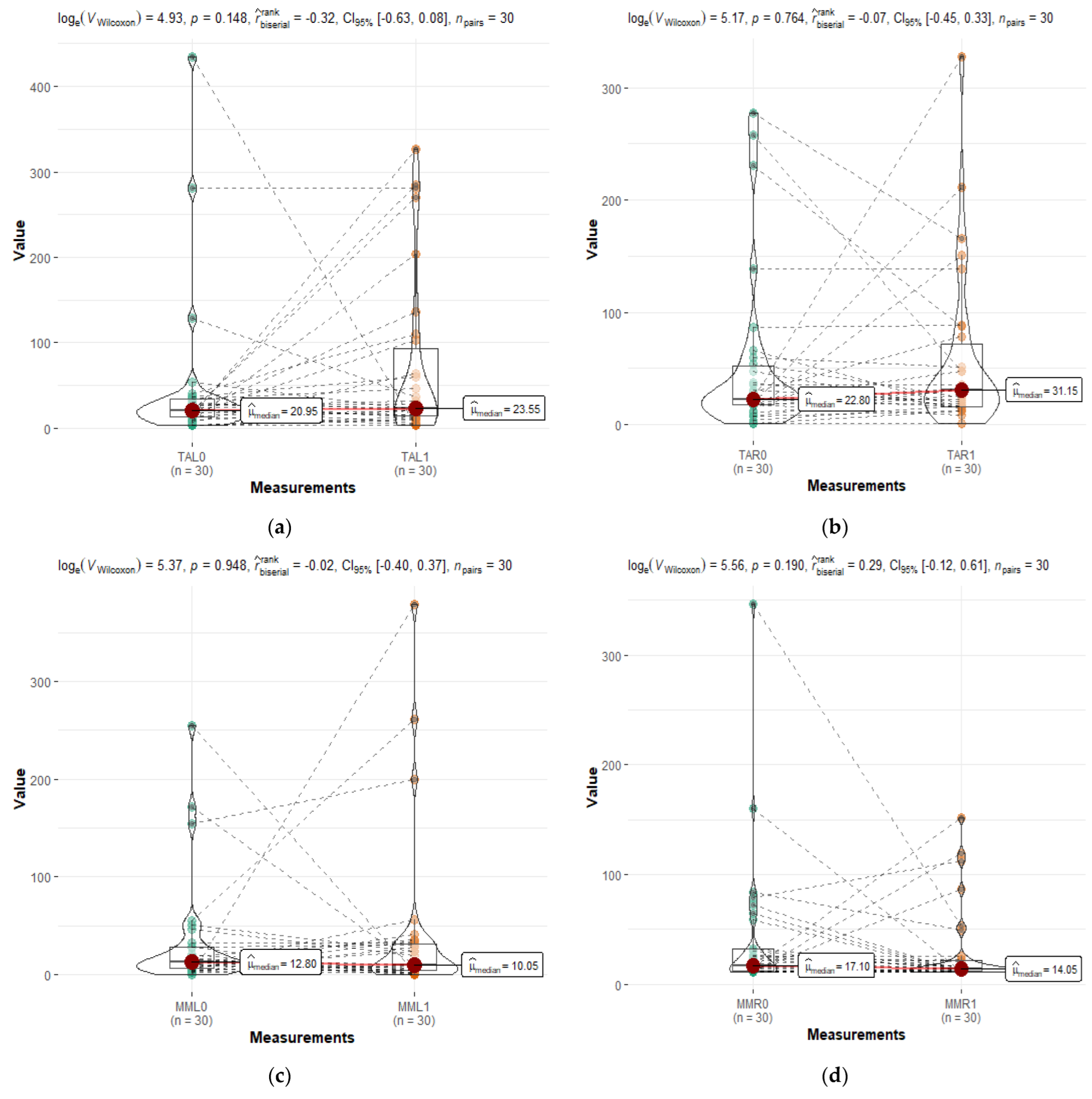
3.2. Study Group (SG) vs. Study Group after Six Months (FSG)
3.3. Study Group after Six Months (FSG) vs. Control Group (CG)
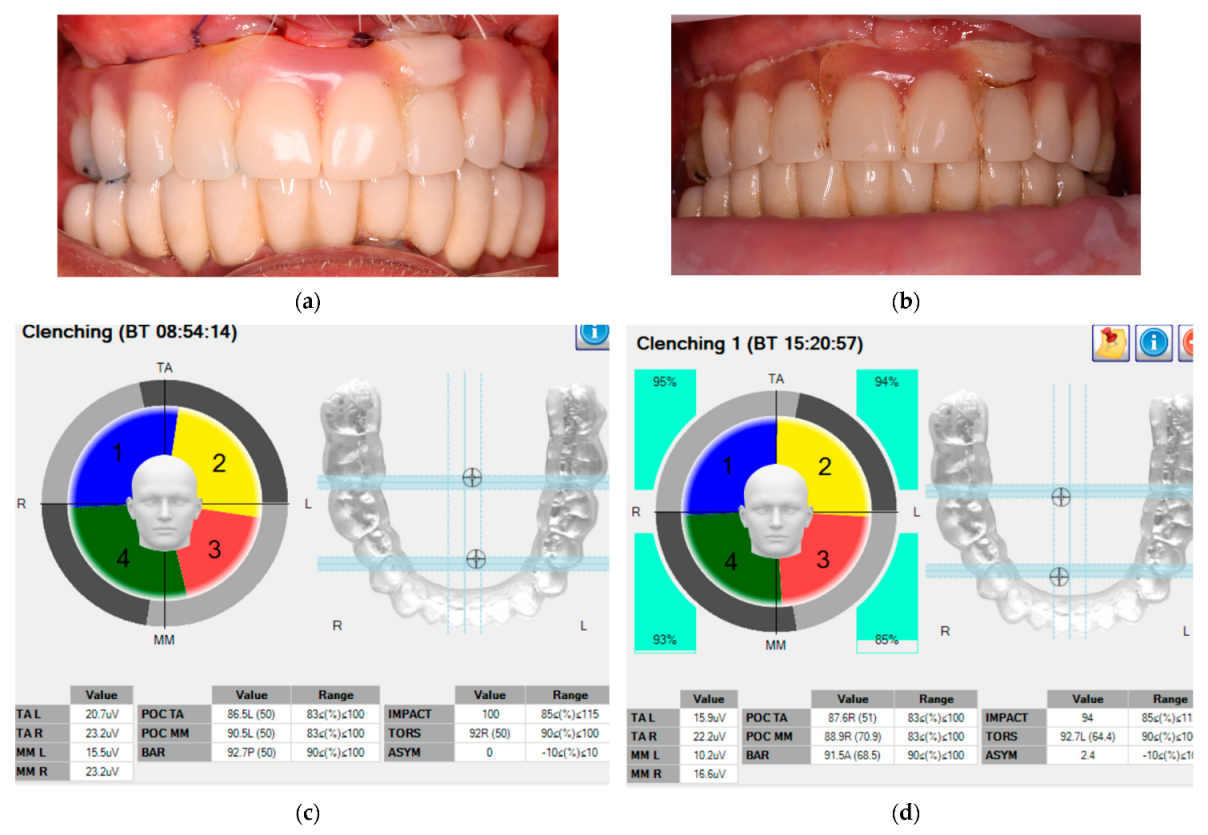
3.4. EMG Activity during Mastication
3.5. Deviation Coefficients
4. Discussion
4.1. Electromyographic Activity in MVC
4.2. Dynamic Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cunha-Cruz, J.; Hujoel, P.P.; Nadanovsky, P. Secular Trends in Socio-economic Disparities in Edentulism: USA, 1972–2001. J. Dent. Res. 2007, 86, 131–136. [Google Scholar] [CrossRef]
- Al-Rafee, M. The epidemiology of edentulism and the associated factors: A literature Review. J. Family Med. Prim Care 2020, 9, 1841. [Google Scholar] [CrossRef] [PubMed]
- Tsakos, G.; Herrick, K.; Sheiham, A.; Watt, R.G. Edentulism and Fruit and Vegetable Intake in Low-income Adults. J. Dent. Res. 2010, 89, 462–467. [Google Scholar] [CrossRef]
- Lee, J.S.; Weyant, R.J.; Corby, P.; Kritchevsky, S.B.; Harris, T.B.; Rooks, R.; Rubin, S.M.; Newman, A.B. Edentulism and nutritional status in a biracial sample of well-functioning, community-dwelling elderly: The Health, Aging, and Body Composition Study. Am. J. Clin. Nutr. 2004, 79, 295–302. [Google Scholar] [CrossRef]
- Thomason, J.M.; Kelly, S.A.M.; Bendkowski, A.; Ellis, J.S. Two implant retained overdentures––A review of the literature supporting the McGill and York consensus statements. J. Dent. 2012, 40, 22–34. [Google Scholar] [CrossRef]
- Zembic, A.; Wismeijer, D. Patient-reported outcomes of maxillary implant-supported overdentures compared with conventional dentures. Clin. Oral Impl. Res. 2014, 25, 441–450. [Google Scholar] [CrossRef]
- Ülkü, S.Z.; Acun Kaya, F.; Uysal, E.; Gulsun, B. Clinical Evaluation of Complications in Implant-Supported Dentures: A 4-Year Retrospective Study. Med. Sci. Monit. 2017, 23, 6137–6143. [Google Scholar] [CrossRef] [PubMed]
- Nishi, S.E.; Basri, R.; Alam, M.K. Uses of electromyography in dentistry: An overview with meta-analysis. Eur. J. Dent. 2016, 10, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Padilla, M.; Hargens, A. Surface electromyography: Technical developments and clinical applications in sports medicine. In Adaptation Biology and Medicine; Popescu, L.M., Hargens, A.R., Singal, P.K., Eds.; Narosa Publishing House Pvt. Ltd.: New Delhi, India, 2014; Volume 7, pp. 333–351. [Google Scholar]
- Klasser, G.D.; Okeson, J.P. The clinical usefulness of surface electromyography in the diagnosis and treatment of temporomandibular disorders. J. Am. Dent. Assoc. 2006, 137, 763–771. [Google Scholar] [CrossRef]
- Marotta, N.; Ferrillo, M.; Demeco, A.; Drago Ferrante, V.; Inzitari, M.T.; Pellegrino, R.; Pino, I.; Russo, I.; de Sire, A.; Ammendolia, A. Effects of Radial Extracorporeal Shock Wave Therapy in Reducing Pain in Patients with Temporomandibular Disorders: A Pilot Randomized Controlled Trial. Appl. Sci. 2022, 12, 3821. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Sforza, C.; Colombo, A.; Ciusa, V. An electromyographic investigation of masticatory muscles symmetry in normo-occlusion subjects. J. Oral Rehabil. 2000, 27, 33–40. [Google Scholar] [CrossRef]
- Ximinis, E.; Tortopidis, D. Electromyographic activity changes of jaw-closing muscles in patients with different occlusion schemes after fixed prosthetic restoration. Balkan J. Dent. Med. 2018, 22, 157–162. [Google Scholar] [CrossRef]
- de Rossi, M.; Palinkas, M.; Lucas, B.; Santos, C.; Semprini, M.; Oliveira, L.; Regalo, I.; Bersani, E.; Migliorança, R.; Siéssere, S.; et al. Masticatory muscle activity evaluation by electromyography in subjects with zygomatic implants. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e392–e397. [Google Scholar] [CrossRef] [PubMed]
- Elsyad, M.A.; Hegazy, S.A.F.; Hammouda, N.I.; Al-Tonbary, G.Y.; Habib, A.A. Chewing efficiency and electromyographic activity of masseter muscle with three designs of implant-supported mandibular overdentures. A cross-over study. Clin. Oral Impl. Res. 2014, 25, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Al-Magaleh, W.R.; Abbas, N.A.; Amer, A.A.; Abdelkader, A.A.; Bahgat, B. Biting Force and Muscle Activity in Implant-Supported Single Mandibular Overdentures Opposing Fixed Maxillary Dentition. Implant. Dent. 2016, 25, 199–203. [Google Scholar] [CrossRef] [PubMed]
- von der Gracht, I.; Derks, A.; Haselhuhn, K.; Wolfart, S. EMG correlations of edentulous patients with implant overdentures and fixed dental prostheses compared to conventional complete dentures and dentates: A systematic review and meta-analysis. Clin. Oral Impl. Res. 2017, 28, 765–773. [Google Scholar] [CrossRef]
- Dellavia, C.; Francetti, L.; Rosati, R.; Corbella, S.; Ferrario, V.F.; Sforza, C. Electromyographic assessment of jaw muscles in patients with All-on-Four fixed implant-supported prostheses. J. Oral Rehabil. 2012, 39, 896–904. [Google Scholar] [CrossRef]
- Ferrario, V.F.; Tartaglia, G.M.; Maglione, M.; Simion, M.; Sforza, C. Neuromuscular coordination of masticatory muscles in subjects with two types of implant-supported prostheses. Clin. Oral Implant. Res. 2004, 15, 219–225. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Bernal, G.; Rungcharassaeng, K.; Kan, J.Y.K. Clinical complications with implants and implant prostheses. J. Prosthet. Dent. 2003, 90, 121–132. [Google Scholar] [CrossRef]
- Craciunescu, E.; Sinescu, C.; Negrutiu, M.L.; Pop, D.M.; Lauer, H.-C.; Rominu, M.; Hutiu, G.; Bunoiu, M.; Duma, V.-F.; Antoniac, I. Shear Bond Strength Tests of Zirconia Veneering Ceramics after Chipping Repair. J. Adhes. Sci. Technol. 2016, 30, 666–676. [Google Scholar] [CrossRef]
- Karkazis, H.C. EMG activity of the masseter muscle in implant supported overdenture wearers during chewing of hard and soft food. J. Oral Rehabil. 2002, 29, 986–991. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Bruno, C.; Jacobs, R.; Torisu, T.; Murata, H. Short-term follow-up of masticatory adaptation after rehabilitation with an immediately loaded implant-supported prosthesis: A pilot assessment. Int. J. Implant Dent. 2017, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Bakke, M.; Holm, B.; Gotfredsen, K. Masticatory function and patient satisfaction with implant-supported mandibular overdentures: A prospective 5-year study. Int. J. Prosthodont. 2002, 15, 575–581. [Google Scholar] [PubMed]
- Saini, M. Implant biomaterials: A comprehensive review. WJCC 2015, 3, 52. [Google Scholar] [CrossRef]
- Gartner, J.L.; Mushimoto, K.; Weber, H.-P.; Nishimura, I. Effect of osseointegrated implants on the coordination of masticatory muscles: A pilot study. J. Prosthet. Dent. 2000, 84, 185–193. [Google Scholar] [CrossRef]
- Weber, H.-P.; Morton, D.; Gallucci, G.O.; Roccuzzo, M.; Cordaro, L.; Grutter, L. Consensus statements and recommended clinical procedures regarding loading protocols. Int. J. Oral Maxillofac. Implant. 2009, 24, 180–183. [Google Scholar]
- Erdelyi, R.-A.; Duma, V.-F.; Sinescu, C.; Dobre, G.M.; Bradu, A.; Podoleanu, A. Dental Diagnosis and Treatment Assessments: Between X-rays Radiography and Optical Coherence Tomography. Materials 2020, 13, 4825. [Google Scholar] [CrossRef]
- Erdelyi, R.-A.; Duma, V.-F.; Sinescu, C.; Dobre, G.M.; Bradu, A.; Podoleanu, A. Optimization of X-ray Investigations in Dentistry using Optical Coherence Tomography. Sensors 2021, 21, 4554. [Google Scholar] [CrossRef] [PubMed]
- Giannakopoulos, N.N.; Corteville, F.; Kappel, S.; Rammelsberg, P.; Schindler, H.J.; Eberhard, L. Functional adaptation of the masticatory system to implant-supported mandibular overdentures. Clin. Oral Impl. Res. 2017, 28, 529–534. [Google Scholar] [CrossRef]
- Uram-Tuculescu, S.; Cooper, L.; Foegeding, E.; Vinyard, C.; De Kok, I.; Essick, G. Electromyographic Evaluation of Masticatory Muscles in Dentate Patients Versus Conventional and Implant-Supported Fixed and Removable Denture Wearers—A Preliminary Report Comparing Model Foods. Int. J. Prosthodont. 2015, 28, 79–92. [Google Scholar] [CrossRef]
- Trulsson, M. Sensory and motor function of teeth and dental implants: A basis for osseoperception. Clin. Exp. Pharmacol. Physiol. 2005, 32, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, V.F.; Sforza, C. Coordinated electromyographic activity of the human masseter and temporalis anterior muscles during mastication. Eur. J. Oral Sci. 1996, 104, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Alqutaibi, A.Y.; Kaddah, A.F.; Farouk, M. Randomized study on the effect of single-implant versus two-implant retained overdentures on implant loss and muscle activity: A 12-month follow-up report. Int. J. Oral Maxillofac. Surg. 2017, 46, 789–797. [Google Scholar] [CrossRef]
- Fontijn-Tekampl, E.; Slagter, A.P.; van’t Hof, M.A.; Geertman, M.E.; Kalk, W. Bite Forces with Mandibular Implant-retained Overdentures. J. Dent. Res. 1998, 77, 1832–1839. [Google Scholar] [CrossRef]
- Uçankale, M.; Akoğlu, B.; Özkan, Y.; Ozkan, Y.K. The effect of different attachment systems with implant-retained overdentures on maximum bite force and EMG: EMG activity of different overdenture system. Gerodontology 2012, 29, 24–29. [Google Scholar] [CrossRef]
- Elsyad, M.A.; El-asfahani, I.A.; Kortam, S.A.; Mourad, S.I. Masseter muscle activity of conventional denture, fixed prosthesis, and milled bar overdenture used for All-on-4 implant rehabilitation: A within-subject study. Clin. Implant. Dent. Relat. Res. 2021, 23, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Misch, C. Dental Implant Prosthetics, 3rd ed.; Mosby Elsevier: St. Louis, MI, USA, 2005. [Google Scholar]
- Jacobs, R.; van Steenberghe, D. Masseter muscle fatigue during sustained clenching in subjects with complete dentures, implant-supported prostheses, and natural teeth. J. Prosthet. Dent. 1993, 69, 305–313. [Google Scholar] [CrossRef]
- De Rossi, M.; Santos, C.M.; Miglioranca, R.; Regalo, S.C.H. All on Four® Fixed Implant Support Rehabilitation: A Masticatory Function Study: All on Four® and Masticatory Function. Clin. Implant. Dent. Relat. Res. 2014, 16, 594–600. [Google Scholar] [CrossRef]
- Mostovei, M.; Mostovei, A.; Tiutiucă, C.; Dimofte, A.R.; Oleg, A.; Oleg, S. Determination of masticatory efficiency in patients with fixed full implant-supported prostheses: Dynamic study. Rom. J. Oral Rehabil. 2022, 14, 174–183. [Google Scholar]
- Sinescu, C.; Duma, V.-F.; Dodenciu, D.; Stratul, S.; Manole, M.; Draganescu, G.E. Mechanical properties of the periodontal system and of dental constructs deduced from the free response of the tooth. J. Healthc. Eng. 2018, 2018, 4609264. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CG (N = 33) | SG (N = 30) | FSG (N = 30) | Wilcoxon Test (CG vs. SG) | Wilcoxon Test (CG vs. FSG) | Wilcoxon Paired Test (SG vs. FSG) | ||
|---|---|---|---|---|---|---|---|
| TAL (µV) | Mean (SD) | 42.0 (48.5) | 46.9 (89.8) | 73.6 (97.6) | W = 527, p = 0.6646 | W = 554, p = 0.4207 | V = 267, p = 0.1482 |
| Median (IQR) | 18.8 (36.3) | 21.0 (20.3) | 23.6 (79.1) | ||||
| [Min., Max.] | [3.80, 190] | [3.80, 434] | [3.80, 326] | ||||
| Shapiro-Wilk normality test | W = 0.72061, p = 1.361 × 10−6 | W = 0.72061, p = 1.361 × 10−6 | W = 0.6981, p = 1.464 × 10−6 | ||||
| TAR (µV) | Mean (SD) | 51.4 (56.8) | 53.5 (74.4) | 59.4 (72.9) | W = 556, p = 0.4051 | W = 483.5, p = 0.8797 | V = 202, p = 0.7639 |
| Median (IQR) | 32.9 (35.2) | 22.8 (34.6) | 31.2 (55.2) | ||||
| [Min., Max.] | [7.90, 248] | [1.30, 278] | [1.30, 328] | ||||
| Shapiro-Wilk normality test | W = 0.67751, p = 3.031 × 10−7 | W = 0.67751, p = 3.031 × 10−7 | W = 0.69981, p = 1.551 × 10−6 | ||||
| MML (µV) | Mean (SD) | 48.7 (107) | 33.8 (57.7) | 41.7 (85.4) | W = 490, p = 0.9506 | W = 464.5, p = 0.6797 | V = 221, p = 0.9483 |
| Median (IQR) | 12.3 (24.8) | 12.8 (21.2) | 10.1 (27.6) | ||||
| [Min., Max.] | [1.50, 439] | [0.200, 255] | [0.300, 379] | ||||
| Shapiro-Wilk normality test | W = 0.45479, p = 5.957 × 10−10 | W = 0.45479, p = 5.957 × 10−10 | W = 0.50205, p = 5.634 × 10−9 | ||||
| MMR (µV) | Mean (SD) | 42.1 (64.4) | 41.9 (66.1) | 30.5 (37.1) | W = 500.5, p = 0.945 | W = 415, p = 0.2734 | V = 145, p = 0.1904 |
| Median (IQR) | 16.3 (16.7) | 17.1 (20.3) | 14.1 (10.1) | ||||
| [Min., Max.] | [11.4, 243] | [11.4, 346] | [11.3, 152] | ||||
| Shapiro-Wilk normality test | W = 0.51507, p = 2.646 × 10−9 | W = 0.51507, p = 2.646 × 10−9 | W = 0.5765, p = 3.816 × 10−8 |
| CGch (N = 33) | SGch (N = 30) | FSGch (N = 30) | CG vs. CGch | SG vs. SGch | FSG vs. FSGch | SGch vs. FSGch | CGch vs. SGch and FSGch | ||
|---|---|---|---|---|---|---|---|---|---|
| TAL (µV) | Mean (SD) | 41.4 (60.9) | 46.7 (73.1) | 74.9 (106) | Wilcoxon paired test, V (p) | Wilcoxon test | |||
| Median (IQR) | 25.9 (18.1) | 20.3 (13.5) | 21.4 (72.6) | ||||||
| [Min, Max] | [3.80, 301] | [3.80, 291] | [3.80, 442] | V = 263, p = 0.9925 | V = 187, p = 0.9713 | V = 249, p = 0.5027 | V = 137, p = 0.1358 | W = 534.5, p = 0.5914; W = 463, p = 0.6646 | |
| Shapiro-Wilk normality test | W = 0.52469, p = 3.395 × 10−9 | W = 0.54318, p = 1.581 × 10−8 | W = 0.67237, p = 6.334 × 10−7 | ||||||
| TAR (µV) | Mean (SD) | 49.0 (59.1) | 66.6 (88.7) | 68.5 (109) | V = 221, p = 0.4268 | V = 291, p = 0.1144 | V = 232, p = 1.000 | V = 264.5, p = 0.517 | W = 516, p = 0.7778; W = 547.5, p = 0.4742 |
| Median (IQR) | 27.4 (26.1) | 27.3 (50.2) | 24.7 (21.7) | ||||||
| [Min, Max] | [5.60, 255] | [1.90, 305] | [2.90, 421] | ||||||
| Shapiro-Wilk normality test | W = 0.60284, p = 2.94 × 10−8 | W = 0.68422, p = 9.27 × 10−7 | W = 0.57884, p = 4.067 × 10−8 | ||||||
| MML (µV) | Mean (SD) | 41.7 (96.0) | 58.6 (85.3) | 53.3 (111) | V = 186, p = 0.1473 | V = 271, p = 0.1243 | V = 228, p = 0.9344 | V = 247, p = 0.5306 | W = 394, p = 0.1666; W = 496, p = 0.9945 |
| Median (IQR) | 10.1 (11.9) | 14.6 (64.7) | 10.5 (17.2) | ||||||
| [Min, Max] | [2.60, 439] | [0.600, 321] | [1.70, 458] | ||||||
| Shapiro-Wilk normality test | W = 0.42774, p = 3.163 × 10−10 | W = 0.69698, p = 1.41 × 10−6 | W = 0.50761, p = 6.454 × 10−9 | ||||||
| MMR (µV) | Mean (SD) | 51.0 (89.3) | 47.7 (82.1) | 49.6 (78.7) | V = 293, p = 0.594 | V = 270.5, p = 0.1271 | V = 340, p = 0.008331 | V = 211, p = 0.8644 | W = 509, p = 0.8526; W = 552.5, p = 0.4327 |
| Median (IQR) | 16.4 (16.9) | 16.1 (15.2) | 15.3 (15.0) | ||||||
| [Min, Max] | [11.4, 401] | [11.5, 397] | [11.4, 303] | ||||||
| Shapiro-Wilk normality test | W = 0.48789, p = 1.332 × 10−9 | W = 0.49244, p = 4.462 × 10−9 | W = 0.53966, p = 1.444 × 10−8 | ||||||
| CG (N = 33) | SG (N = 30) | FSG (N = 30) | CGch (N = 33) | SGch (N = 30) | FSGch (N = 30) | ||
|---|---|---|---|---|---|---|---|
| POCTA | Mean (SD) | 74.7 (17.2) | 74.9 (17.6) | 67.0 (17.8) | 62.3 (14.1) | 63.1 (21.5) | 56.9 (16.2) |
| Median (IQR) | 81.0 (18.9) | 82.9 (20.7) | 70.1 (22.3) | 66.4 (22.2) | 71.6 (29.7) | 59.1 (19.6) | |
| [Min, Max] | [29.0, 90.9] | [29.8, 95.1] | [26.8, 88.8] | [34.8, 83.3] | [15.3, 89.6] | [16.8, 86.8] | |
| CD_POCTA% | Mean (SD) | 12.5 (18.8) | 12.1 (19.4) | 20.2 (20.5) | 25.0 (17.0) | 24.5 (25.4) | 29.0 (20.0) |
| Median (IQR) | 2.41 (17.5) | 0.0602 (20.2) | 15.6 (26.8) | 20.0 (26.7) | 13.7 (35.8) | 26.1 (28.0) | |
| [Min, Max] | [0, 65.1] | [0, 64.1] | [0, 67.7] | [0, 58.1] | [0, 81.6] | [0, 79.8] | |
| POCMM | Mean (SD) | 73.6 (17.2) | 63.5 (24.5) | 58.0 (25.9) | 52.3 (15.5) | 51.7 (21.5) | 41.1 (23.2) |
| Median (IQR) | 76.2 (18.1) | 68.4 (26.0) | 58.1 (39.3) | 52.7 (14.7) | 54.6 (26.3) | 40.8 (28.9) | |
| [Min, Max] | [14.5, 98.7] | [10.5, 90.5] | [7.20, 97.8] | [10.4, 85.1] | [8.30, 90.2] | [1.70, 94.9] | |
| CD_POCMM% | Mean (SD) | 13.8 (18.3) | 21.9 (25.9) | 31.7 (29.2) | 37.0 (18.5) | 38.1 (25.2) | 50.1 (27.8) |
| Median (IQR) | 8.19 (18.9) | 14.8 (30.5) | 30.1 (47.3) | 36.5 (17.7) | 34.3 (31.7) | 50.8 (36.1) | |
| [Min, Max] | [0, 82.5] | [0, 79.4] | [0, 91.3] | [0, 87.5] | [0, 90.0] | [0, 98.0] | |
| BAR | Mean (SD) | 76.4 (14.7) | 73.6 (16.2) | 72.6 (15.1) | 71.4 (11.1) | 65.3 (19.8) | 59.1 (19.9) |
| Median (IQR) | 80.1 (21.4) | 79.7 (23.5) | 77.3 (19.2) | 72.4 (16.8) | 70.8 (24.2) | 64.6 (25.9) | |
| [Min, Max] | [23.4, 93.1] | [39.8, 92.7] | [34.3, 91.5] | [48.5, 90.1] | [14.3, 91.2] | [8.40, 84.3] | |
| CD_BAR% | Mean (SD) | 15.4 (16.0) | 18.4 (17.7) | 19.3 (16.7) | 20.7 (12.3) | 27.5 (22.0) | 34.3 (22.2) |
| Median (IQR) | 11.0 (23.8) | 11.5 (26.1) | 14.2 (21.3) | 19.6 (18.7) | 21.3 (26.9) | 28.3 (28.8) | |
| [Min, Max] | [0, 74.0] | [0, 55.8] | [0, 61.9] | [0, 46.1] | [0, 84.1] | [6.33, 90.7] | |
| IMPACT0 | Mean (SD) | 95.0 (28.2) | 105 (22.8) | 105 (63.9) | 94.2 (24.8) | 168 (177) | 160 (149) |
| Median (IQR) | 95.0 (31.0) | 100 (30.0) | 97.5 (28.3) | 91.0 (33.0) | 103 (33.5) | 117 (51.0) | |
| [Min, Max] | [0, 150] | [66.0, 164] | [0, 399] | [46.0, 146] | [55.0, 824] | [29.0, 724] | |
| CD_IMPACT0% | Mean (SD) | 9.87 (19.5) | 6.46 (10.4) | 16.9 (46.3) | 9.30 (12.7) | 60.9 (147) | 57.6 (116) |
| Median (IQR) | 0 (11.3) | 0.865 (7.74) | 0 (10.2) | 3.40 (16.0) | 2.60 (14.9) | 12.2 (46.7) | |
| [Min, Max] | [0, 100] | [0, 42.0] | [0, 246] | [0, 45.9] | [0, 616] | [0, 530] | |
| TORS | Mean (SD) | 80.5 (12.4) | 76.1 (16.2) | 72.8 (13.9) | 69.3 (10.9) | 68.7 (19.3) | 55.7 (18.4) |
| Median (IQR) | 83.5 (15.8) | 82.9 (24.8) | 72.1 (15.9) | 71.5 (11.4) | 73.5 (25.2) | 56.5 (36.6) | |
| [Min, Max] | [40.2, 93.9] | [40.7, 92.6] | [40.6, 92.7] | [37.6, 86.5] | [19.1, 89.1] | [27.2, 80.8] | |
| CD_TORS0 % | Mean (SD) | 11.2 (13.1) | 15.8 (17.6) | 19.3 (15.3) | 23.0 (12.1) | 23.6 (21.5) | 36.3 (21.4) |
| Median (IQR) | 7.22 (17.3) | 7.94 (27.5) | 19.9 (17.7) | 20.6 (12.7) | 18.4 (27.9) | 35.5 (41.1) | |
| [Min, Max] | [0, 55.3] | [0, 54.8] | [0, 54.9] | [3.89, 58.2] | [1.00, 78.8] | [0, 69.8] | |
| ASYM | Mean (SD) | 12.7 (13.5) | 12.0 (12.4) | 19.2 (16.3) | 16.7 (16.1) | 25.0 (24.8) | 29.1 (23.6) |
| Median (IQR) | 6.60 (11.3) | 8.30 (13.7) | 17.2 (16.8) | 9.30 (16.3) | 12.8 (22.8) | 25.4 (35.4) | |
| [Min, Max] | [0, 56.4] | [4.00, 53.8] | [0.300, 68.4] | [0.300, 54.3] | [0.400, 83.0] | [0.400, 80.1] | |
| CD_Asym % | Mean (SD) | 60.0 (114) | 53.9 (99.5) | 109 (147) | 92.8 (141) | 166 (235) | 207 (219) |
| Median (IQR) | 0 (58.0) | 0 (72.0) | 71.5 (149) | 0 (112) | 28.0 (228) | 154 (344) | |
| [Min, Max] | [0, 464] | [0, 438] | [0, 584] | [0, 443] | [0, 730] | [0, 701] |
| Value | Value | Range | Value | Range | |||
|---|---|---|---|---|---|---|---|
| TAL (µV) | 434.2 | POC TA | 80.6 L (98.6) | 83 < (%) < 100 | IMPACT | 125 | 83 < (%) < 100 |
| TAR (µV) | 257.9 | POC MM | 80.7 R (77) | 83 < (%) < 100 | TORS | 83.2 L (95.6) | 90 < (%) < 100 |
| MM L | 10.4 | BAR | 80.7 A (93.5) | 90 < (%) < 100 | ASYM | −6.7 | −10 < (%) < −10 |
| MM R | 11.4 | ||||||
| CG | SG | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | n/N (%) | 95% CI | n/N (%) | 95% CI | n/N (%) | 95% CI | Fisher’s test | McNemar’s test | Characteristic |
| L0/R1_POCTA | p-value = 0.3173, OR = 0.58 (95% CI 0.19, 1.73) | p-value = 0.6164, OR = 0.75 (95% CI 0.24, 2.27) | ꭓ2 = 0.071429, df = 1, p-value = 0.7893 | ||||||
| 0 | 13/33 (39) | 23, 58 | 16/30 (53) | 35, 71 | 14/30 (47) | 29, 65 | |||
| 1 | 20/33 (61) | 42, 77 | 14/30 (47) | 29, 65 | 16/30 (53) | 35, 71 | |||
| L0/R1_POCTAch | p-value = 0.8014, OR = 0.82 (95% CI 0.27, 2.45) | p-value = 0.8025, OR = 1.21 (95% CI 0.40, 3.67) | ꭓ2 = 0.30769, df = 1, p-value = 0.5791 | ||||||
| 0 | 17/33 (52) | 34, 69 | 17/30 (57) | 38, 74 | 14/30 (47) | 29, 65 | |||
| 1 | 16/33 (48) | 31, 66 | 13/30 (43) | 26, 62 | 16/30 (53) | 35, 71 | |||
| POCTA vs. POCTAch (McNemar’s) | ꭓ2 = 0.75, df = 1, p-value = 0.3865 | ꭓ2 = 0, df = 1, p-value = 1 | ꭓ2 = 0, df = 1, p-value = 1 | ||||||
| L0/R1_POCMM | p-value = 0.4502, OR = 1.58 (95% CI 0.52, 4.88) | p-value = 0.2034, OR = 2.10 (95% CI 0.68, 6.71) | ꭓ2 = 0.083333, df = 1, p-value = 0.7728 | ||||||
| 0 | 17/33 (52) | 34, 69 | 12/30 (40) | 23, 59 | 10/30 (33) | 18, 53 | |||
| 1 | 16/33 (48) | 31, 66 | 18/30 (60) | 41, 77 | 20/30 (67) | 47, 82 | |||
| L0/R1_POCMMch | p-value = 0.1292, OR = 0.44 (95% CI 0.14, 1.37) | p-value = 0.2045, OR = 0.50 (95% CI 0.16, 1.57) | ꭓ2 = 0, df = 1, p-value = 1 | ||||||
| 0 | 10/33 (30) | 16, 49 | 15/30 (50) | 33, 67 | 14/30 (47) | 29, 65 | |||
| 1 | 23/33 (70) | 51, 84 | 15/30 (50) | 33, 67 | 16/30 (53) | 35, 71 | |||
| POCMM vs. POCMMch (McNemar’s) | ꭓ2 = 2.4, df = 1, p-value = 0.1213 | ꭓ2 = 0.30769, df = 1, p-value = 0.5791 | ꭓ2 = 0.75, df = 1, p-value = 0.3865 | ||||||
| A0/P1_BAR | |||||||||
| 0 | 22/33 (67) | 48, 81 | 16/30 (53) | 35, 71 | 19/30 (63) | 44, 79 | p-value = 0.3127, OR = 1.73 (95% CI 0.56, 5.49) | p-value = 0.7978, OR = 1.16 (95% CI 0.36, 3.70) | ꭓ2 = 0.30769, df = 1, p-value = 0.5791 |
| 1 | 11/33 (33) | 19, 52 | 14/30 (47) | 29, 65 | 11/30 (37) | 21, 56 | |||
| A0/P1_BARch | |||||||||
| 0 | 22/33 (67) | 48, 81 | 17/30 (57) | 38, 74 | 16/30 (53) | 35, 71 | p-value = 0.4472, OR = 1.52 (95% CI 0.49, 4.82) | p-value = 0.3127, OR = 1.73 (95% CI 0.56, 5.49) | ꭓ2 = 0, df = 1, p-value = 1 |
| 1 | 11/33 (33) | 19, 52 | 13/30 (43) | 26, 62 | 14/30 (47) | 29, 65 | |||
| BAR vs. BARch (McNemar’s) | ꭓ2 = 0, df = 1, p-value = 1 | ꭓ2 = 0, df = 1, p-value = 1 | ꭓ2 = 0.36364, df = 1, p-value = 0.5465 | ||||||
| L0/R1_TORS | p-value = 0.8025, OR = 0.83 (95% CI 0.27, 2.48) | p-value = 0.616, OR = 0.72 (95% CI 0.24, 2.17) | ꭓ2 = 0, df = 1, p-value = 1 | ||||||
| 0 | 16/33 (48) | 31, 66 | 16/30 (53) | 35, 71 | 17/30 (57) | 38, 74 | |||
| 1 | 17/33 (52) | 34, 69 | 14/30 (47) | 29, 65 | 13/30 (43) | 26, 62 | |||
| L0/R1_TORSch | p-value = 0.6164, OR = 1.34 (95% CI 0.44, 4.12) | p-value = 0.3137, OR = 1.74 (95% CI 0.58, 5.39) | ꭓ2 = 0, df = 1, p-value = 1 | ||||||
| 0 | 20/33 (61) | 42, 77 | 14/30 (47) | 29, 65 | 14/30 (47) | 29, 65 | |||
| 1 | 13/33 (39) | 23, 58 | 16/30 (53) | 35, 71 | 16/30 (53) | 35, 71 | |||
| TORS vs. TORSch (McNemar’s) | ꭓ2 = 0.5625, df = 1, p-value = 0.4533 | ꭓ2 = 0.16667, df = 1, p-value = 0.6831 | ꭓ2 = 0.36364, df = 1, p-value = 0.5465 | TORS vs. TORSch (McNemar’s) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mostovei, M.; Solomon, O.; Chele, N.; Sinescu, C.; Duma, V.-F.; Mostovei, A. Electromyographic Evaluation of Muscle Activity in Patients Rehabilitated with Full Arch Fixed Implant-Supported Prostheses. Medicina 2023, 59, 299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59020299
Mostovei M, Solomon O, Chele N, Sinescu C, Duma V-F, Mostovei A. Electromyographic Evaluation of Muscle Activity in Patients Rehabilitated with Full Arch Fixed Implant-Supported Prostheses. Medicina. 2023; 59(2):299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59020299
Chicago/Turabian StyleMostovei, Mihail, Oleg Solomon, Nicolae Chele, Cosmin Sinescu, Virgil-Florin Duma, and Andrei Mostovei. 2023. "Electromyographic Evaluation of Muscle Activity in Patients Rehabilitated with Full Arch Fixed Implant-Supported Prostheses" Medicina 59, no. 2: 299. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59020299