
Effects of Eccentric-Oriented Strength Training on Return to Sport Criteria in Late-Stage Anterior Cruciate Ligament (ACL)-Reconstructed Professional Team Sport Players

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
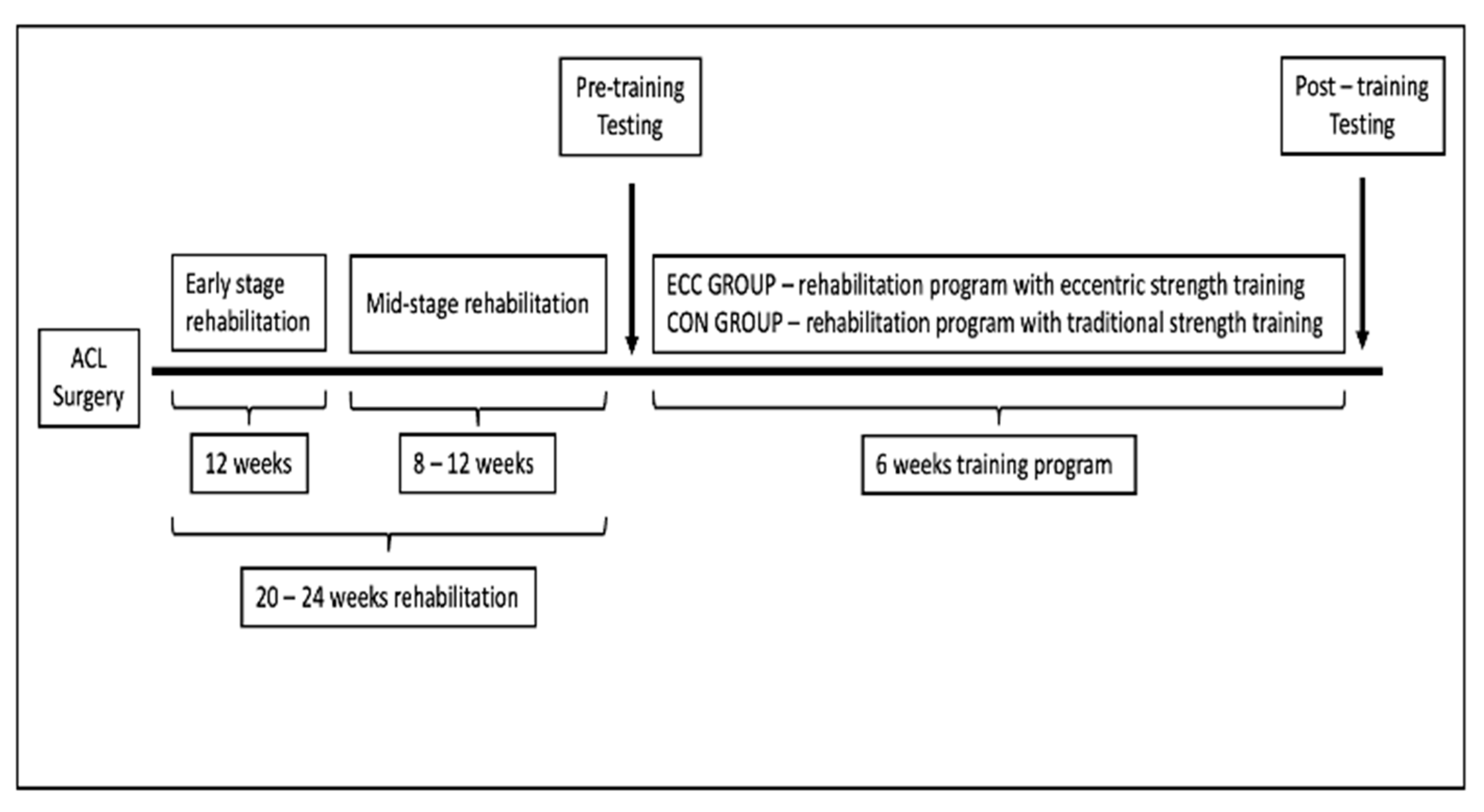
2.2. Study Design
2.3. Rehabilitation Protocols
2.4. Testing Procedures
2.4.1. Isometric Leg Strength
2.4.2. Hop Tests
2.4.3. Vertical Jump Tests
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gornitzky, A.L.; Lott, A.; Yellin, J.L.; Fabricant, P.D.; Lawrence, J.T.; Ganley, T.J. Sport-Specific Yearly Risk and Incidence of Anterior Cruciate Ligament Tears in High School Athletes. Am. J. Sport. Med. 2016, 44, 2716–2723. [Google Scholar] [CrossRef]
- Sanborn, R.M.; Badger, G.J.; Proffen, B.; Sant, N.; Barnett, S.; Fleming, B.C.; Kramer, D.E.; Micheli, L.J.; Yen, Y.-M.; Murray, M.M.; et al. Psychological Readiness to Return to Sport at 6 Months Is Higher After Bridge-Enhanced ACL Restoration Than Autograft ACL Reconstruction: Results of a Prospective Randomized Clinical Trial. Orthop. J. Sport. Med. 2022, 10, 232596712110705. [Google Scholar] [CrossRef] [PubMed]
- Davies, W.T.; Myer, G.D.; Read, P.J. Is It Time We Better Understood the Tests We Are Using for Return to Sport Decision Making Following ACL Reconstruction? A Critical Review of the Hop Tests. Sport. Med. 2020, 50, 485–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maestroni, L.; Read, P.; Bishop, C.; Turner, A. Strength and Power Training in Rehabilitation: Underpinning Principles and Practical Strategies to Return Athletes to High Performance. Sport. Med. 2019, 50, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Kyritsis, P.; Bahr, R.; Landreau, P.; Miladi, R.; Witvrouw, E. Likelihood of ACL Graft Rupture: Not Meeting Six Clinical Discharge Criteria before Return to Sport Is Associated with a Four Times Greater Risk of Rupture. Br. J. Sport. Med. 2016, 50, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Powell, C.; Jensen, J.; Johnson, S. Functional Performance Measures Used for Return-to-Sport Criteria in Youth Following Lower-Extremity Injury. J. Sport Rehabil. 2018, 27, 581–590. [Google Scholar] [CrossRef] [Green Version]
- Kotsifaki, A.; Van Rossom, S.; Whiteley, R.; Korakakis, V.; Bahr, R.; Sideris, V.; Jonkers, I. Single Leg Vertical Jump Performance Identifies Knee Function Deficits at Return to Sport after ACL Reconstruction in Male Athletes. Br. J. Sport. Med. 2022, 56, 490–498. [Google Scholar] [CrossRef]
- Greenberg, E.M.; Greenberg, E.T.; Albaugh, J.; Storey, E.; Ganley, T.J. Rehabilitation Practice Patterns Following Anterior Cruciate Ligament Reconstruction: A Survey of Physical Therapists. J. Orthop. Sport. Phys. Ther. 2018, 48, 801–811. [Google Scholar] [CrossRef]
- Korakakis, V.; Kotsifaki, A.; Korakaki, A.; Karanasios, S.; Whiteley, R. Current Perspectives and Clinical Practice of Physiotherapists on Assessment, Rehabilitation, and Return to Sport Criteria after Anterior Cruciate Ligament Injury and Reconstruction. An Online Survey of 538 Physiotherapists. Phys. Ther. Sport 2021, 52, 103–114. [Google Scholar] [CrossRef]
- Kotsifaki, R.; Korakakis, V.; King, E.; Barbosa, O.; Maree, D.; Pantouveris, M.; Bjerregaard, A.; Luomajoki, J.; Wilhelmsen, J.; Whiteley, R. Aspetar Clinical Practice Guideline on Rehabilitation after Anterior Cruciate Ligament Reconstruction. Br. J. Sport. Med. 2023, 57, 500–514. [Google Scholar] [CrossRef]
- Hewett, T.E.; Di Stasi, S.L.; Myer, G.D. Current Concepts for Injury Prevention in Athletes After Anterior Cruciate Ligament Reconstruction. Am. J. Sport. Med. 2012, 41, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Paterno, M.V.; Schmitt, L.C.; Ford, K.R.; Rauh, M.J.; Myer, G.D.; Huang, B.; Hewett, T.E. Biomechanical Measures during Landing and Postural Stability Predict Second Anterior Cruciate Ligament Injury after Anterior Cruciate Ligament Reconstruction and Return to Sport. Am. J. Sport. Med. 2010, 38, 1968–1978. [Google Scholar] [CrossRef] [Green Version]
- Lepley, L.K.; Lepley, A.S.; Onate, J.A.; Grooms, D.R. Eccentric Exercise to Enhance Neuromuscular Control. Sport. Health A Multidiscip. Approach 2017, 9, 333–340. [Google Scholar] [CrossRef]
- Brockett, C.L.; Morgan, D.L.; Proske, U. Predicting Hamstring Strain Injury in Elite Athletes. Med. Sci. Sport. Exerc. 2004, 36, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Butterfield, T.A. Eccentric Exercise In Vivo. Exerc. Sport Sci. Rev. 2010, 38, 51–60. [Google Scholar] [CrossRef]
- Aagaard, P.; Andersen, J.L.; Dyhre-Poulsen, P.; Leffers, A.-M.; Wagner, A.; Magnusson, S.P.; Halkjaer-Kristensen, J.; Simonsen, E.B. A Mechanism for Increased Contractile Strength of Human Pennate Muscle in Response to Strength Training: Changes in Muscle Architecture. J. Physiol. 2001, 534, 613–623. [Google Scholar] [CrossRef]
- Douglas, J.; Pearson, S.; Ross, A.; McGuigan, M. Chronic Adaptations to Eccentric Training: A Systematic Review. Sport. Med. 2016, 47, 917–941. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Blazevich, A.J.; Haff, G.G.; Tufano, J.J.; Newton, R.U.; Häkkinen, K. Greater Strength Gains after Training with Accentuated Eccentric than Traditional Isoinertial Loads in Already Strength-Trained Men. Front. Physiol. 2016, 7, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedmann-Bette, B.; Bauer, T.; Kinscherf, R.; Vorwald, S.; Klute, K.; Bischoff, D.; Müller, H.; Weber, M.-A.; Metz, J.; Kauczor, H.-U.; et al. Effects of Strength Training with Eccentric Overload on Muscle Adaptation in Male Athletes. Eur. J. Appl. Physiol. 2009, 108, 821–836. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; González-Izal, M.; Pallarés, J.G.; Rodriguez-Falces, J.; Häkkinen, K.; Kraemer, W.J.; Pinto, R.S.; Izquierdo, M. Muscle conduction velocity, strength, neural activity, and morphological changes after eccentric and concentric training. Scand. J. Med. Sci. Sport. 2014, 24, e343–e352. [Google Scholar] [CrossRef]
- Franchi, M.V.; Reeves, N.D.; Narici, M.V. Skeletal Muscle Remodeling in Response to Eccentric vs. Concentric Loading: Morphological, Molecular, and Metabolic Adaptations. Front. Physiol. 2017, 8, 447. [Google Scholar] [CrossRef] [Green Version]
- Wirth, K.; Keiner, M.; Szilvas, E.; Hartmann, H.; Sander, A. Effects of Eccentric Strength Training on Different Maximal Strength and Speed-Strength Parameters of the Lower Extremity. J. Strength Cond. Res. 2015, 29, 1837–1845. [Google Scholar] [CrossRef] [Green Version]
- Lepley, L.K.; Grooms, D.R.; Burland, J.P.; Davi, S.M.; Mosher, J.L.; Cormier, M.L.; Lepley, A.S. Eccentric cross-exercise after anterior cruciate ligament reconstruction: Novel case series to enhance neuroplasticity. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sport. Med. 2018, 34, 55–65. [Google Scholar] [CrossRef]
- Hortobágyi, T.; Lambert, N.J.; Hill, J.P. Greater Cross Education Following Training with Muscle Lengthening than Shortening. Med. Sci. Sport. Exerc. 1997, 29, 107–112. [Google Scholar] [CrossRef]
- Gabriel, D.A.; Kamen, G.; Frost, G. Neural Adaptations to Resistive Exercise. Sport. Med. 2006, 36, 133–149. [Google Scholar] [CrossRef]
- Lepley, L.K.; Wojtys, E.M.; Palmieri-Smith, R.M. Combination of Eccentric Exercise and Neuromuscular Electrical Stimulation to Improve Biomechanical Limb Symmetry after Anterior Cruciate Ligament Reconstruction. Clin. Biomech. 2015, 30, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Lepley, L.K.; Wojtys, E.M.; Palmieri-Smith, R.M. Combination of Eccentric Exercise and Neuromuscular Electrical Stimulation to Improve Quadriceps Function Post-ACL Reconstruction. Knee 2015, 22, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Friedmann-Bette, B.; Profit, F.; Gwechenberger, T.; Weiberg, N.; Parstorfer, M.; Weber, M.-A.; Streich, N.; Barié, A. Strength training effects on muscular regeneration after ACL reconstruction. Med. Sci. Sport. Exerc. 2018, 50, 1152–1161. [Google Scholar] [CrossRef]
- Kinikli, G.I. The Effect of Progressive Eccentric and Concentric Training on Functional Performance after Autogenous Hamstring Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Study. Acta Orthop. Et Traumatol. Turc. 2014, 48, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Milandri, G.; Sivarasu, S. A Randomized Controlled Trial of Eccentric Versus Concentric Cycling for Anterior Cruciate Ligament Reconstruction Rehabilitation. Am. J. Sport. Med. 2021, 49, 626–636. [Google Scholar] [CrossRef]
- Kasmi, S.; Zouhal, H.; Hammami, R.; Clark, C.C.T.; Hackney, A.C.; Hammami, A.; Chtara, M.; Chortane, S.G.; Salah, F.Z.B.; Granacher, U.; et al. The Effects of Eccentric and Plyometric Training Programs and Their Combination on Stability and the Functional Performance in the Post-ACL-Surgical Rehabilitation Period of Elite Female Athletes. Front. Physiol. 2021, 12, 688385. [Google Scholar] [CrossRef] [PubMed]
- Henderson, F.J.; Konishi, Y.; Shima, N.; Shimokochi, Y. Effects of 8-Week Exhausting Deep Knee Flexion Flywheel Training on Persistent Quadriceps Weakness in Well-Trained Athletes Following Anterior Cruciate Ligament Reconstruction. Int. J. Environ. Res. Public Health 2022, 19, 13209. [Google Scholar] [CrossRef]
- Sabido, R.; Hernández-Davó, J.L.; Pereyra-Gerber, G.T. Influence of Different Inertial Loads on Basic Training Variables During the Flywheel Squat Exercise. Int. J. Sport. Physiol. Perform. 2018, 13, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sport. Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Gokeler, A.; Grassi, A.; Hoogeslag, R.; van Houten, A.; Lehman, T.; Bolling, C.; Buckthorpe, M.; Norte, G.; Benjaminse, A.; Heuvelmans, P.; et al. Return to Sports after ACL Injury 5 Years from Now: 10 Things We Must Do. J. Exp. Orthop. 2022, 9, 73. [Google Scholar] [CrossRef] [PubMed]
- Vidmar, M.F.; Baroni, B.M.; Michelin, A.F.; Mezzomo, M.; Lugokenski, R.; Pimentel, G.L.; Silva, M.F. Isokinetic Eccentric Training Is More Effective than Constant Load Eccentric Training for Quadriceps Rehabilitation Following Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. Braz. J. Phys. Ther. 2020, 24, 424–432. [Google Scholar] [CrossRef]
- Gerber, J.P.; Marcus, R.L.; Dibble, L.E.; Greis, P.E.; Burks, R.T.; LaStayo, P.C. Effects of Early Progressive Eccentric Exercise on Muscle Structure After Anterior Cruciate Ligament Reconstruction. J. Bone Jt. Surg. 2007, 89, 559–570. [Google Scholar] [CrossRef]
- Matheson, G.J. We Need to Talk about Reliability: Making Better Use of Test-Retest Studies for Study Design and Interpretation. PeerJ 2019, 7, e6918. [Google Scholar] [CrossRef] [Green Version]
- Gokeler, A.; Welling, W.; Benjaminse, A.; Lemmink, K.; Seil, R.; Zaffagnini, S. A Critical Analysis of Limb Symmetry Indices of Hop Tests in Athletes after Anterior Cruciate Ligament Reconstruction: A Case Control Study. Orthop. Traumatol. Surg. Res. 2017, 103, 947–951. [Google Scholar] [CrossRef]
- Zumstein, F.; Centner, C.; Ritzmann, R. How Limb Dominance Influences Limb Symmetry in ACL Patients: Effects on Functional Performance. BMC Sport. Sci. Med. Rehabil. 2022, 14, 206. [Google Scholar] [CrossRef]
- Wellsandt, E.; Failla, M.J.; Snyder-Mackler, L. Limb Symmetry Indexes Can Overestimate Knee Function After Anterior Cruciate Ligament Injury. J. Orthop. Sport. Phys. Ther. 2017, 47, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Mallinson, J.E.; Taylor, T.; Constantin-Teodosiu, D.; Billeter-Clark, R.; Constantin, D.; Franchi, M.V.; Narici, M.V.; Auer, D.; Greenhaff, P.L. Longitudinal hypertrophic and transcriptional responses to high-load eccentric-concentric vs concentric training in males. Scand. J. Med. Sci. Sport. 2020, 30, 2101–2115. [Google Scholar] [CrossRef]
- Pietrosimone, B.G.; Lepley, A.S.; Ericksen, H.M.; Clements, A.; Sohn, D.H.; Gribble, P.A. Neural Excitability Alterations After Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2015, 50, 665–674. [Google Scholar] [CrossRef] [Green Version]
- Kuenze, C.M.; Hertel, J.; Weltman, A.; Diduch, D.; Saliba, S.A.; Hart, J.M. Persistent Neuromuscular and Corticomotor Quadriceps Asymmetry After Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2015, 50, 303–312. [Google Scholar] [CrossRef] [Green Version]
- Hurley, M.V.; Jones, D.W.; Newham, D.J. Arthrogenic Quadriceps Inhibition and Rehabilitation of Patients with Extensive Traumatic Knee Injuries. Clin. Sci. 1994, 86, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Duchateau, J.; Enoka, R.M. Neural Control of Lengthening Contractions. J. Exp. Biol. 2016, 219, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.-H.; Park, J.-W. Different Cortical Activation Patterns during Voluntary Eccentric and Concentric Muscle Contractions: An fMRI Study. NeuroRehabilitation 2011, 29, 253–259. [Google Scholar] [CrossRef]


{kind=link}
| Group | Exercises | First Week | Second Week | Third Week | Fourth Week | Fifth Week | Sixth Week |
|---|---|---|---|---|---|---|---|
| ECC eccentric oriented | Half squat on an isoinertial device | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 |
| Copenhagen eccentric | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Romanian deadlifts on isoinertial device | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Eccentric Swiss ball curl | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Hip thrust on an isoinertial device | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Bulgarian squats on an isoinertial device | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| CON traditional | Spanish squat | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 |
| Copenhagen | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Romanian deadlift with free weights | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Leg curl | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Hip thrust | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 | |
| Bulgarian squat | 2 × 6 | 2 × 8 | 2 × 10 | 3 × 8 | 3 × 9 | 3 × 10 |
| Title 1 | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday | Sunday |
|---|---|---|---|---|---|---|---|
| Weeks 1, 2, and 3 | Upper body strength; Agility/decelerations/landing skills; Aerobic endurance | Lower body strength | Recovery core; flexibility stretching | Upper body strength; Agility/decelerations/landing skills; Aerobic endurance | Lower body strength | Recovery core; flexibility stretching | Off |
| Weeks 4, 5, and 6 | Upper body strength; Agility/decelerations/landing skills; Aerobic endurance | Lower body strength | Recovery core; flexibility stretching | Lower body strength | Upper body strength; Agility/decelerations/landing skills; Aerobic endurance | Lower body strength | Off |
| Variables | Group | Pre-Test | Post-Test | Main Effect F (Sign) | Interaction F (Sign) | Effect Size |
|---|---|---|---|---|---|---|
| Strength (uninjured) | ECC | 82.54 ± 23.16 | 105.72 ± 26.98 *† | 192.81 (0.000) | 31.62 (0.000) | 2.51, very large |
| CON | 64.81 ± 11.46 | 74.63± 11.76 * | ||||
| Strength (injured) | ECC | 77.09 ± 16.94 | 98.00 ± 20.58 *† | 144.72 (0.000) | 16.08 (0.001) | 1.78, large |
| CON | 57.54 ± 14.48 | 68.00 ± 13.74 * | ||||
| Strength (LSI) | ECC | 86.45 ± 6.02 | 92.45 ± 7.31 * | 22.86 (.000) | 0.122 (0.730) | 0.156, trivial |
| CON | 82.81 ± 5.19 | 88.00 ± 4.25 * | ||||
| CMJ | ECC | 45.92 ± 8.19 | 51.86 ± 8.11 *† | 156.01 (0.000) | 25.36 (0.000) | 2.23, very large |
| CON | 37.60 ± 7.29 | 40.12 ± 7.47 * | ||||
| Single-leg jump (uninjured) | ECC | 27.40 ± 4.88 | 30.91 ± 4.74 * | 14.79 (0.001) | 3.33 (0.08) | 0.82, moderate |
| CON | 21.99 ± 4.77 | 23.18 ± 4.49 * | ||||
| Single-leg jump (injured) | ECC | 22.73 ± 5.20 | 28.14 ± 5.01 *† | 95.24 (0.000) | 11.51 (0.003) | 1.48, large |
| CON | 19.06 ± 3.47 | 21.68 ± 4.53 * | ||||
| Single-leg jump (LSI) | ECC | 80.36 ± 5.29 | 90.27 ± 5.53 * | 27.39 (0.000) | 0.872 (0.362) | 0.48, small |
| CON | 82.36 ± 11.35 | 89.97 ± 8.84 * | ||||
| Single-leg hop (uninjured) | ECC | 159.54 ± 30.68 | 181.81 ± 21.52 * | 48.33 (0.000) | 2.33 (0.133) | 0.69, moderate |
| CON | 139.54 ± 14.90 | 153.64 ± 13.61 * | ||||
| Single-leg hop (injured) | ECC | 138.63 ± 23.56 | 171.81 ± 19.40 *† | 70.00 (0.000) | 16.79 (0.001) | 1.83, large |
| CON | 139.54 ± 23.71 | 150.90 ± 17.00 * | ||||
| Single-leg hop (LSI) | ECC | 87.54 ± 7.44 | 93.90 ± 5.14 * | 8.21 (0.010) | 2.09 (0.163) | 0.64, moderate |
| CON | 91.09 ± 6.23 | 93.18 ± 5.60 * | ||||
| Triple-leg hop (uninjured) | ECC | 550.00 ± 93.91 | 593.63 ± 77.72 * | 47.26 (0.000) | 0.965 (0.338) | 0.43, small |
| CON | 455.90 ± 43.11 | 488.63 ± 35.82 * | ||||
| Triple-leg hop (injured) | ECC | 494.54 ± 89.95 | 565.45 ± 80.82 *† | 64.28 (0.000) | 16.07 (0.001) | 1.78, large |
| CON | 450.45 ± 56.32 | 474.09 ± 45.78 * | ||||
| Triple-leg hop (LSI) | ECC | 90.00 ± 6.66 | 95.09 ± 4.61 * | 23.01 (0.000) | 1.53 (0.229) | 0.55, moderate |
| CON | 92.81 ± 3.25 | 95.81 ± 3.54 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojanović, M.D.M.; Andrić, N.; Mikić, M.; Vukosav, N.; Vukosav, B.; Zolog-Șchiopea, D.-N.; Tăbăcar, M.; Melinte, R.M. Effects of Eccentric-Oriented Strength Training on Return to Sport Criteria in Late-Stage Anterior Cruciate Ligament (ACL)-Reconstructed Professional Team Sport Players. Medicina 2023, 59, 1111. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061111
Stojanović MDM, Andrić N, Mikić M, Vukosav N, Vukosav B, Zolog-Șchiopea D-N, Tăbăcar M, Melinte RM. Effects of Eccentric-Oriented Strength Training on Return to Sport Criteria in Late-Stage Anterior Cruciate Ligament (ACL)-Reconstructed Professional Team Sport Players. Medicina. 2023; 59(6):1111. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061111
Chicago/Turabian StyleStojanović, Marko D. M., Nikola Andrić, Mladen Mikić, Nikola Vukosav, Borko Vukosav, Dan-Nicolae Zolog-Șchiopea, Mircea Tăbăcar, and Răzvan Marian Melinte. 2023. "Effects of Eccentric-Oriented Strength Training on Return to Sport Criteria in Late-Stage Anterior Cruciate Ligament (ACL)-Reconstructed Professional Team Sport Players" Medicina 59, no. 6: 1111. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061111