
The Effects of Sodium-Glucose Cotransporter 2-Inhibitors on Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease or Steatohepatitis and Type 2 Diabetes: A Systematic Review of Randomized Controlled Trials

 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
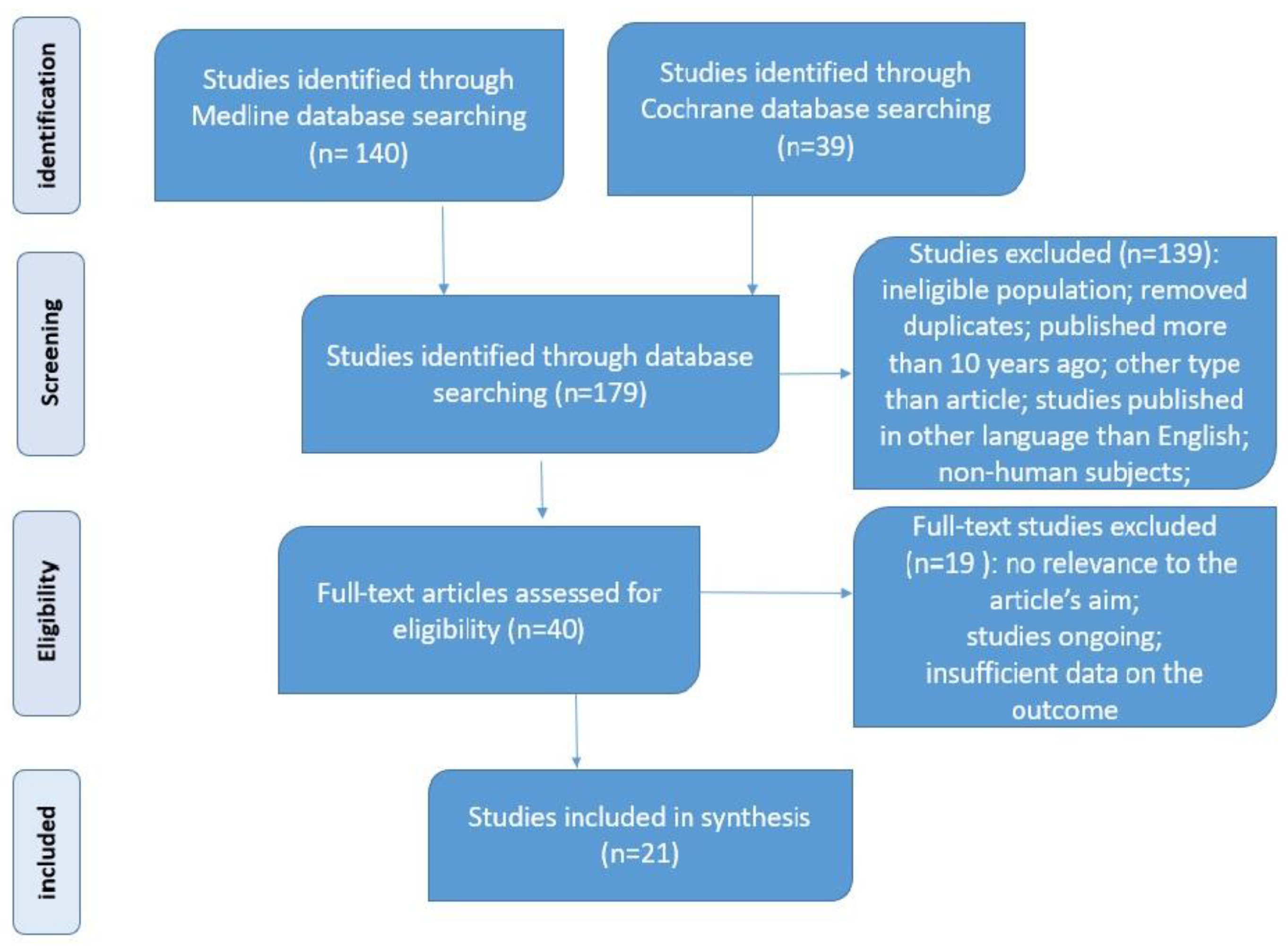
3.1. Literature Search and the Characteristics of the Included Studies
3.2. Dapagliflozin and NAFLD/NASH
3.3. Empagliflozin and NAFLD/NASH
3.4. Canagliflozin and NAFLD/NASH
3.5. Other SGLT2-i and NAFLD/NASH
3.6. New Perspectives
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.-A. The prevalence and incidence of NAFLD worldwide: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diabetes. 2022. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 2 February 2023).
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology 2012, 55, 2005–2023. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1002/hep.25762 (accessed on 25 February 2023). [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1002/hep.28431 (accessed on 23 February 2023). [CrossRef] [PubMed] [Green Version]
- Tilg, H.; Moschen, A.R.; Roden, M. NAFLD and diabetes mellitus. Nat. Rev. Gastroenterol. Hepatol. 2016, 14, 32–42. Available online: https://0-www-nature-com.brum.beds.ac.uk/articles/nrgastro.2016.147 (accessed on 25 February 2023). [CrossRef] [PubMed]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. Available online: http://www.journal-of-hepatology.eu/article/S0168827819303939/fulltext (accessed on 25 February 2023). [CrossRef] [PubMed]
- Dufour, J.F.; Scherer, R.; Balp, M.M.; McKenna, S.J.; Janssens, N.; Lopez, P.; Pedrosa, M. The global epidemiology of nonalcoholic steato-hepatitis (NASH) and associated risk factors—A targeted literature review. Endocr. Metab. Sci. 2021, 3, 100089. [Google Scholar] [CrossRef]
- Mantovani, A.; Dalbeni, A.; Beatrice, G.; Cappelli, D.; Gomez-Peralta, F. Non-Alcoholic Fatty Liver Disease and Risk of Macro- and Microvascular Complications in Patients with Type 2 Diabetes. J. Clin. Med. 2022, 11, 968. [Google Scholar] [CrossRef]
- Simon, T.G.; Roelstraete, B.; Hagström, H.; Sundström, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef]
- Muzurović, E.; Peng, C.C.-H.; Belanger, M.J.; Sanoudou, D.; Mikhailidis, D.P.; Mantzoros, C.S. Nonalcoholic Fatty Liver Disease and Cardiovascular Disease: A Review of Shared Cardiometabolic Risk Factors. Hypertension 2022, 79, 1319–1326. [Google Scholar] [CrossRef]
- Przybyszewski, E.M.; Targher, G.; Roden, M.; Corey, K.E. Nonalcoholic Fatty Liver Disease and Cardiovascular Disease. Clin. Liver Dis. 2021, 17, 19–22. [Google Scholar] [CrossRef]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Wong, V.W.S.; Castellanos, M.; Aller-de la Fuente, R.; Metwally, M.; Eslam, M.; Gonzalez-Fabian, L.; Sanz, M.A.Q.; Conde-Martin, A.F.; et al. Fibrosis Se-verity as a Determinant of Cause-Specific Mortality in Patients with Advanced Nonalcoholic Fatty Liver Disease: A Multi-National Cohort Study. Gastroenterology 2018, 155, 443–457.e17. [Google Scholar] [CrossRef]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, morbidity and mortality of nonalcoholic fatty liver disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Stoian, A.P.; Rizzo, M. Dietary patterns in non-alcoholic fatty liver disease (NAFLD): Stay on the straight and narrow path! Clin. Investig. Arterioscler. 2022, 34 (Suppl. S1), S24–S31. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef] [PubMed]
- Hsia, D.S.; Grove, O.; Cefalu, W.T. An Update on SGLT2 Inhibitors for the Treatment of Diabetes Mellitus. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 73. [Google Scholar]
- Ribola, F.A.; Cançado, F.B.; Schoueri, J.H.; De Toni, V.F.; Medeiros, V.H.; Feder, D. Effects of SGLT2 inhibitors on weight loss in pa-tients with type 2 diabetes mellitus. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 199–211. [Google Scholar] [PubMed]
- Mende, C.W. Chronic Kidney Disease and SGLT2 Inhibitors: A Review of the Evolving Treatment Landscape. Adv. Ther. 2021, 39, 148–164. [Google Scholar] [CrossRef]
- View of Effects of Canagliflozin on Fatty Liver Indexes in Patients with Type 2 Diabetes: A Meta-analysis of Randomized Controlled Trials. Available online: https://journals.library.ualberta.ca/jpps/index.php/JPPS/article/view/29831/21427 (accessed on 25 February 2023).
- Shimizu, M.; Suzuki, K.; Kato, K.; Jojima, T.; Iijima, T.; Murohisa, T.; Iijima, M.; Takekawa, H.; Usui, I.; Hiraishi, H.; et al. Evaluation of the effects of dapagliflozin, a sodium-glucose co-transporter-2 inhibitor, on hepatic steatosis and fibrosis using transient elastography in patients with type 2 diabetes and non-alcoholic fatty liver disease. Diabetes Obes. Metab. 2018, 21, 285–292. Available online: https://pubmed.ncbi.nlm.nih.gov/30178600/ (accessed on 25 February 2023). [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients with Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. Available online: https://pubmed.ncbi.nlm.nih.gov/29895557/ (accessed on 25 February 2023). [CrossRef] [Green Version]
- Meex, R.C.R.; Watt, M.J. Hepatokines: Linking nonalcoholic fatty liver disease and insulin resistance. Nat. Rev. Endocrinol. 2017, 13, 509–520. Available online: https://pubmed.ncbi.nlm.nih.gov/28621339/ (accessed on 25 February 2023). [CrossRef]
- Rizzo, M.; Colletti, A.; Penson, P.E.; Katsiki, N.; Mikhailidis, D.P.; Toth, P.P.; Gouni-Berthold, I.; Mancini, J.; Marais, D.; Ruscica, M.; et al. Nutraceutical approaches to non-alcoholic fatty liver disease (NAFLD): A position paper from the International Lipid Expert Panel (ILEP). Pharmacol. Res. 2023, 189, 106679. [Google Scholar] [CrossRef]
- Muzurović, E.M.; Volčanšek, Š.; Tomšić, K.Z.; Janež, A.; Mikhailidis, D.P.; Rizzo, M.; Mantzoros, C.S. Glucagon-Like Peptide-1 Receptor Agonists and Dual Glucose-Dependent Insulinotropic Polypeptide/Glucagon-Like Peptide-1 Receptor Agonists in the Treatment of Obesity/Metabolic Syndrome, Prediabetes/Diabetes and Non-Alcoholic Fatty Liver Disease-Current Evidence. J. Cardiovasc. Pharmacol. Ther. 2022, 27, 10742484221146371. [Google Scholar]
- Bica, C.; Sandu, C.; Suceveanu, A.I.; Sarbu, E.; Stoica, R.A.; Gherghiceanu, F.; Bohiltea, R.E.; Stefan, S.D.; Stoian, A.P. Non-alcoholic fatty liver disease: A major challenge in type 2 diabetes mellitus (Review). Exp. Ther. Med. 2020, 20, 2387–2391. [Google Scholar] [CrossRef]
- Yaribeygi, H.; Sathyapalan, T.; Maleki, M.; Jamialahmadi, T.; Sahebkar, A. Molecular mechanisms by which SGLT2 inhibitors can induce insulin sensitivity in diabetic milieu: A mechanistic review. Life Sci. 2019, 240, 117090. Available online: https://pubmed.ncbi.nlm.nih.gov/31765648/ (accessed on 25 February 2023). [CrossRef] [PubMed]
- Nakano, D.; Akiba, J.; Tsutsumi, T.; Kawaguchi, M.; Yoshida, T.; Koga, H.; Kawaguchi, T. Hepatic expression of sodium–glucose cotransporter 2 (SGLT2) in patients with chronic liver disease. Med. Mol. Morphol. 2022, 55, 304–315. [Google Scholar] [CrossRef]
- Rizvi, A.A.; Patti, A.M.; Giglio, R.V.; Nikolic, D.; Amato, A.; Al-Busaidi, N.; Al-Rasadi, K.; Soresi, M.; Banach, M.; Montalto, G.; et al. Liraglutide improves carotid intima-media thickness in patients with type 2 diabetes and non-alcoholic fatty liver disease: An 8-month prospective pilot study. Expert Opin. Biol. Ther. 2015, 15, 1391–1397. [Google Scholar] [CrossRef]
- McCoy, R.G.; O’connor, P.J. Overcoming Therapeutic Inertia in Type 2 Diabetes Care—Timing, Context, and Appropriateness of Treatment Intensification. JAMA Netw. Open 2021, 4, e2130926. [Google Scholar] [CrossRef]
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Available online: http://www.prisma-statement.org/ (accessed on 20 February 2023).
- Latva-Rasku, A.; Honka, M.-J.; Kullberg, J.; Mononen, N.; Lehtimäki, T.; Saltevo, J.; Kirjavainen, A.K.; Saunavaara, V.; Iozzo, P.; Johansson, L.; et al. The SGLT2 Inhibitor Dapagliflozin Reduces Liver Fat but Does Not Affect Tissue Insulin Sensitivity: A Randomized, Double-Blind, Placebo-Controlled Study with 8-Week Treatment in Type 2 Diabetes Patients. Diabetes Care 2019, 42, 931–937. Available online: https://pubmed.ncbi.nlm.nih.gov/30885955/ (accessed on 26 February 2023). [CrossRef] [PubMed] [Green Version]
- Frías, J.P.; Maaske, J.; Suchower, L.; Johansson, L.; Hockings, P.D.; Iqbal, N.; Dm, J.P.H.W. Long-term effects of dapagliflozin plus saxagliptin versus glimepiride on a background of metformin in patients with type 2 diabetes: Results of a 104-week extension to a 52-week randomized, phase 3 study and liver fat MRI substudy. Diabetes Obes. Metab. 2021, 24, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Gastaldelli, A.; Repetto, E.; Guja, C.; Hardy, E.; Han, J.; Jabbour, S.A.; Ferrannini, E. Exenatide and dapagliflozin combination improves markers of liver steatosis and fibrosis in patients with type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 393–403. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/dom.13907 (accessed on 26 February 2023). [CrossRef] [Green Version]
- Cho, K.Y.; Nakamura, A.; Omori, K.; Takase, T.; Miya, A.; Yamamoto, K.; Nomoto, H.; Kameda, H.; Taneda, S.; Kurihara, Y.; et al. Favorable effect of sodium–glucose cotransporter 2 inhibitor, dapagliflozin, on non-alcoholic fatty liver disease compared with pioglitazone. J. Diabetes Investig. 2020, 12, 1272–1277. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/jdi.13457 (accessed on 26 February 2023). [CrossRef] [PubMed]
- Kinoshita, T.; Shimoda, M.; Nakashima, K.; Fushimi, Y.; Hirata, Y.; Tanabe, A.; Tatsumi, F.; Hirukawa, H.; Sanada, J.; Kohara, K.; et al. Comparison of the effects of three kinds of glucose-lowering drugs on non-alcoholic fatty liver disease in patients with type 2 diabetes: A randomized, open-label, three-arm, active control study. J. Diabetes Investig. 2020, 11, 1612–1622. Available online: https://pubmed.ncbi.nlm.nih.gov/32329963/ (accessed on 26 February 2023). [CrossRef] [PubMed]
- Johansson, L.; Hockings, P.D.; Johnsson, E.; Dronamraju, N.; Maaske, J.; Garcia-Sanchez, R.; Wilding, J.P.H. Dapagliflozin plus saxagliptin add-on to metformin reduces liver fat and adipose tissue volume in patients with type 2 diabetes. Diabetes Obes. Metab. 2020, 22, 1094–1101. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/dom.14004 (accessed on 27 February 2023). [CrossRef] [PubMed]
- Taheri, H.; Malek, M.; Ismail-Beigi, F.; Zamani, F.; Sohrabi, M.; Babaei, M.R.; Khamseh, M.E. Effect of Empagliflozin on Liver Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease without Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Adv. Ther. 2020, 37, 4697–4708. Available online: https://0-link-springer-com.brum.beds.ac.uk/article/10.1007/s12325-020-01498-5 (accessed on 27 February 2023). [CrossRef] [PubMed]
- Tobita, H.; Yazaki, T.; Kataoka, M.; Kotani, S.; Oka, A.; Mishiro, T.; Oshima, N.; Kawashima, K.; Ishimura, N.; Naora, K.; et al. Comparison of dapagliflozin and teneligliptin in nonalcoholic fatty liver disease patients without type 2 diabetes mellitus: A prospective randomized study. J. Clin. Biochem. Nutr. 2021, 68, 173–180. Available online: https://www.jstage.jst.go.jp/article/jcbn/68/2/68_20-129/_article (accessed on 27 February 2023). [CrossRef] [PubMed]
- Eriksson, J.W.; Lundkvist, P.; Jansson, P.-A.; Johansson, L.; Kvarnström, M.; Moris, L.; Miliotis, T.; Forsberg, G.-B.; Risérus, U.; Lind, L.; et al. Effects of dapagliflozin and n-3 carboxylic acids on non-alcoholic fatty liver disease in people with type 2 diabetes: A double-blind randomised placebo-controlled study. Diabetologia 2018, 61, 1923–1934. Available online: https://pmc/articles/PMC6096619/ (accessed on 27 February 2023). [CrossRef] [Green Version]
- Harreiter, J.; Just, I.; Leutner, M.; Bastian, M.; Brath, H.; Schelkshorn, C.; Klepochova, R.; Krššák, M.; Kautzky-Willer, A. Combined exenatide and dapagliflozin has no additive effects on reduction of hepatocellular lipids despite better glycaemic control in patients with type 2 diabetes mellitus treated with metformin: EXENDA, a 24-week, prospective, randomized, placebo-controlled pilot trial. Diabetes Obes. Metab. 2021, 23, 1129–1139. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/dom.14319 (accessed on 28 February 2023).
- Phrueksotsai, S.; Pinyopornpanish, K.; Euathrongchit, J.; Leerapun, A.; Phrommintikul, A.; Buranapin, S.; Chattipakorn, N.; Thongsawat, S. The effects of dapagliflozin on hepatic and visceral fat in type 2 diabetes patients with non-alcoholic fatty liver disease. J. Gastroenterol. Hepatol. 2021, 36, 2952–2959. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/jgh.15580 (accessed on 28 February 2023). [CrossRef]
- Kahl, S.; Gancheva, S.; Straßburger, K.; Herder, C.; Machann, J.; Katsuyama, H.; Kabisch, S.; Henkel, E.; Kopf, S.; Lagerpusch, M.; et al. Empagliflozin Effectively Lowers Liver Fat Content in Well-Controlled Type 2 Diabetes: A Randomized, Double-Blind, Phase 4, Placebo-Controlled Trial. Diabetes Care 2019, 43, 298–305. Available online: https://diabetesjournals.org/care/article/43/2/298/36104/Empagliflozin-Effectively-Lowers-Liver-Fat-Content (accessed on 28 February 2023). [CrossRef] [Green Version]
- Gaborit, B.; Ancel, P.; Abdullah, A.E.; Maurice, F.; Abdesselam, I.; Calen, A.; Soghomonian, A.; Houssays, M.; Varlet, I.; Eisinger, M.; et al. Effect of empagliflozin on ectopic fat stores and myocardial energetics in type 2 diabetes: The EMPACEF study. Cardiovasc. Diabetol. 2021, 20, 57. Available online: https://0-cardiab-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/s12933-021-01237-2 (accessed on 1 March 2023). [CrossRef]
- Chehrehgosha, H.; Sohrabi, M.R.; Ismail-Beigi, F.; Malek, M.; Babaei, M.R.; Zamani, F.; Ajdarkosh, H.; Khoonsari, M.; Fallah, A.E.; Khamseh, M.E. Empagliflozin Improves Liver Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease and Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Diabetes Ther. 2021, 12, 843–861. [Google Scholar] [CrossRef]
- Elhini, S.H.; Wahsh, E.A.; Elberry, A.A.; El Ameen, N.F.; Saedii, A.A.; Refaie, S.M.; Elsayed, A.A.; Rabea, H.M. The Impact of an SGLT2 Inhibitor versus Ursodeoxycholic Acid on Liver Steatosis in Diabetic Patients. Pharmaceuticals 2022, 15, 1516. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K.; Bril, F.; Barb, D.; Polidori, D.; Sha, S.; Ghosh, A.; Bs, K.F.; Sunny, N.E.; Kalavalapalli, S.; Pettus, J.; et al. Effect of canagliflozin treatment on hepatic triglyceride content and glucose metabolism in patients with type 2 diabetes. Diabetes Obes. Metab. 2018, 21, 812–821. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/full/10.1111/dom.13584 (accessed on 1 March 2023). [CrossRef] [PubMed]
- Bando, Y.; Ogawa, A.; Ishikura, K.; Kanehara, H.; Hisada, A.; Notumata, K.; Okafuji, K.; Toya, D. The effects of ipragliflozin on the liver-to-spleen attenuation ratio as assessed by computed tomography and on alanine transaminase levels in Japanese patients with type 2 diabetes mellitus. Diabetol. Int. 2017, 8, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Ito, D.; Shimizu, S.; Inoue, K.; Saito, D.; Yanagisawa, M.; Inukai, K.; Akiyama, Y.; Morimoto, Y.; Noda, M.; Shimada, A. Comparison of Ipragliflozin and Pioglitazone Effects on Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes: A Randomized, 24-Week, Open-Label, Active-Controlled Trial. Diabetes Care 2017, 40, 1364–1372. Available online: https://pubmed.ncbi.nlm.nih.gov/28751548/ (accessed on 1 March 2023). [CrossRef] [PubMed] [Green Version]
- Shibuya, T.; Fushimi, N.; Kawai, M.; Yoshida, Y.; Hachiya, H.; Ito, S.; Kawai, H.; Ohashi, N.; Mori, A. Luseogliflozin improves liver fat deposition compared to metformin in type 2 diabetes patients with non-alcoholic fatty liver disease: A prospective randomized controlled pilot study. Diabetes Obes. Metab. 2018, 20, 438–442. Available online: https://pubmed.ncbi.nlm.nih.gov/28719078/ (accessed on 1 March 2023). [CrossRef]
- Han, E.; Lee, Y.-H.; Lee, B.-W.; Kang, E.S.; Cha, B.-S. Ipragliflozin Additively Ameliorates Non-Alcoholic Fatty Liver Disease in Patients with Type 2 Diabetes Controlled with Metformin and Pioglitazone: A 24-Week Randomized Controlled Trial. J. Clin. Med. 2020, 9, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, H.; Kessoku, T.; Kawanaka, M.; Nonaka, M.; Hyogo, H.; Fujii, H.; Nakajima, T.; Imajo, K.; Tanaka, K.; Kubotsu, Y.; et al. Ipragliflozin Improves the Hepatic Outcomes of Patients with Diabetes with NAFLD. Hepatol. Commun. 2021, 6, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, M.; Honda, Y.; Ogawa, Y.; Kessoku, T.; Kobayashi, T.; Imajo, K.; Ozaki, A.; Nogami, A.; Taguri, M.; Yamanaka, T.; et al. Comparing the effects of tofogliflozin and pioglitazone in non-alcoholic fatty liver disease patients with type 2 diabetes mellitus (ToPiND study): A randomized prospective open-label controlled trial. BMJ Open Diabetes Res. Care 2021, 9, e001990. Available online: https://0-drc-bmj-com.brum.beds.ac.uk/content/9/1/e001990 (accessed on 1 March 2023). [CrossRef] [PubMed]
- Takeshita, Y.; Honda, M.; Harada, K.; Kita, Y.; Takata, N.; Tsujiguchi, H.; Tanaka, T.; Goto, H.; Nakano, Y.; Iida, N.; et al. Comparison of Tofogliflozin and Glimepiride Effects on Nonalcoholic Fatty Liver Disease in Participants with Type 2 Diabetes: A Randomized, 48-Week, Open-Label, Active-Controlled Trial. Diabetes Care 2022, 45, 2064–2075. [Google Scholar] [CrossRef]
- Harrison, S.A.; Manghi, F.P.; Smith, W.B.; Alpenidze, D.; Aizenberg, D.; Klarenbeek, N.; Chen, C.-Y.; Zuckerman, E.; Ravussin, E.; Charatcharoenwitthaya, P.; et al. Licogliflozin for nonalcoholic steatohepatitis: A randomized, double-blind, placebo-controlled, phase 2a study. Nat. Med. 2022, 28, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, L.; Li, S.; Jia, P.; Deng, K.; Chen, W.; Sun, X. Effects of SGLT2 inhibitors on UTIs and genital infections in type 2 diabetes mellitus: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 2824. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Choi, E.; Park, E.; Na, E.; Chung, S.Y.; Kim, B.; Han, S.Y. Risk of genital and urinary tract infections associated with SGLT-2 inhibitors as an add-on therapy to metformin in patients with type 2 diabetes mellitus: A retrospective cohort study in Korea. Pharmacol. Res. Perspect. 2022, 10, e00910. [Google Scholar] [CrossRef]
- Hahn, K.; Ejaz, A.A.; Kanbay, M.; Lanaspa, M.A.; Johnson, R.J. Acute kidney injury from SGLT2 inhibitors: Potential mechanisms. Nat. Rev. Nephrol. 2016, 12, 711–712. [Google Scholar] [CrossRef]
- Sridhar, V.S.; Tuttle, K.R.; Cherney, D.Z. We Can Finally Stop Worrying about SGLT2 Inhibitors and Acute Kidney Injury. Am. J. Kidney Dis. 2020, 76, 454–456. [Google Scholar] [CrossRef] [PubMed]
- Nadkarni, G.N.; Ferrandino, R.; Chang, A.; Surapaneni, A.; Chauhan, K.; Poojary, P.; Saha, A.; Ferket, B.; Grams, M.E.; Coca, S.G. Acute Kidney Injury in Patients on SGLT2 Inhibitors: A Propensity-Matched Analysis. Diabetes Care 2017, 40, 1479–1485. [Google Scholar] [CrossRef] [Green Version]
- Rong, X.; Zhu, Y.; Wen, B.; Liu, K.; Li, X.; Gou, Q.; Chen, X. Risk of hypovolemia associated with sodium–glucose cotransporter-2 inhibitors treatment: A meta-analysis of randomized controlled trials. Front. Cardiovasc. Med. 2022, 9, 973129. [Google Scholar] [CrossRef] [PubMed]
- Girerd, N. Low Blood Pressure and Managing Drugs in HF. J. Am. Coll. Cardiol. 2021, 78, 1349–1351. [Google Scholar] [CrossRef]
- Monami, M.; Nreu, B.; Zannoni, S.; Lualdi, C.; Mannucci, E. Effects of SGLT-2 inhibitors on diabetic ketoacidosis: A meta-analysis of randomised controlled trials. Diabetes Res. Clin. Pract. 2017, 130, 53–60. [Google Scholar] [CrossRef]
- Watts, N.B.; Bilezikian, J.P.; Usiskin, K.; Edwards, R.; Desai, M.; Law, G.; Meininger, G. Effects of Canagliflozin on Fracture Risk in Patients with Type 2 Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2016, 101, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- The Nuffield Department of Population Health Renal Studies Group and and theSGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists’ Consortium. Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: Collaborative meta-analysis of large placebo-controlled trials. Lancet 2022, 400, 1788–1801. [Google Scholar] [CrossRef] [PubMed]
- Ercin, C.N.; Dogru, T.; Genç, H.; Celebi, G.; Aslan, F.; Gurel, H.; Kara, M.; Sertoglu, E.; Tapan, S.; Bagci, S.; et al. Insulin Resistance but Not Visceral Adiposity Index Is Associated with Liver Fibrosis in Nondiabetic Subjects with Nonalcoholic Fatty Liver Disease. Metab. Syndr. Relat. Disord. 2015, 13, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Kahl, S.; Ofstad, A.P.; Zinman, B.; Wanner, C.; Schüler, E.; Sattar, N.; Inzucchi, S.E.; Roden, M. Effects of empagliflozin on markers of liver steatosis and fibrosis and their relationship to cardiorenal outcomes. Diabetes Obes. Metab. 2022, 24, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Riazi, K.; Raman, M.; Taylor, L.; Swain, M.G.; Shaheen, A.A. Dietary Patterns and Components in Nonalcoholic Fatty Liver Disease (NAFLD): What Key Messages Can Health Care Providers Offer? Nutrients 2019, 11, 2878. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author | Design/Comparator | Number of Patients | Study Duration | Method of Diagnosis | Outcome | Measure Method |
|---|---|---|---|---|---|---|
| Shimizu et al., 2019 [20] | RCT/placebo | 57 | 24 weeks | FibroScan | Improvement of hepatic steatosis and fibrosis | CAP and LSM |
| Kinoshita et al., 2020 [35] | RCT/pioglitazone or glimepiride | 98 | 28 weeks | CT | Improvement of NAFLD | Liver-to-spleen ratio |
| Johansson et al., 2020 [36] | RCT/glimepiride plus placebo | 444/59 in the MRI substudy | 52 weeks | MRI-PDFF | Improvement of NAFLD | Liver fat percentage and adipose tissue volumes |
| EFFECT-II/Eriksson et al., 2018 [39] | RCT/omega-3 carboxylic acids/ placebo | 83 | 12 weeks | MRI-PDFF + PNPLA3 polymorphism | Improvement of NAFLD | Liver fat content |
| Rasku et al., 2019 [31] | RCT/placebo | 32 | 8 weeks | MRI-PDFF | Improvement of NAFLD | Liver fat content |
| Gastaldelli et al., 2020 [33] | RCT/exenatide combination/placebo combination | 695 | 52 weeks | FLI, FIB-4, NAFLD fibrosis score | Improvement in non-invasive steatosis and fibrosis score | Non-invasive scores |
| EXENDA/Harreiter et al., 2021 [40] | RCT/exenatide combination/placebo | 30 | 24 weeks | MRS + FLI + FIB-4 | Improvement in intrahepatic lipid content | HCL |
| Phrueksotsai et al., 2021 [41] | RCT/placebo | 38 | 12 weeks | CT | Changes in intrahepatic lipid contents | Liver attenuation index |
| Frias et al., 2022 [32] | RCT | 338 | 105 weeks | MRI | Changes in adipose tissue and liver fat | MRI |
| Author | Design/Comparator | Number of Patients | Study Duration | Method of Diagnosis | Outcome | Measure Method |
|---|---|---|---|---|---|---|
| E-LIFT trial (Kuchay et al., 2018) [21] | RCT/Standard treatment | 50 | 20 weeks | MRI-PDFF | Liver fat content < 6% | Liver fat content |
| Kahl et al., 2020 [42] | RCT/placebo | 84 | 24 weeks | 1H-MRS | Change in liver fat content | Liver fat content |
| EMPACEF(Gaborit et al., 2021) [43] | RCT/placebo | 56 | 12 weeks | 1H-MRS | Changes in liver, pancreatic, and myocardial trygliceride content | Epicardial fat volume; intrahepatic and pancreatic fat content |
| Chehrehgosha et al., (2021) [44] | RCT/placebo | 78 | 24 weeks | FibroScan | Improvement of hepatic steatosis and fibrosis | CAP and LSM |
| Elhini et al., (25 mg/day 2022) [45] | RCT/UDCA | 240 | 24 weeks | MRI-PDFF | Change in liver fat content | Liver fat content |
| Author | Design/Comparator | Number of Patients | Study Duration | Method of Diagnosis | Outcome | Measure Method |
|---|---|---|---|---|---|---|
| Cusi et al., 2019 [46] | RCT/placebo | 56 | 24 weeks | 1H-MRS | Reduction in intrahepatic TG | Intrahepatic TG accumulation |
| Author | Design/Comparator | Number of Patients | Study Duration | Method of Diagnosis | Outcome | Measure Method |
|---|---|---|---|---|---|---|
| Takahashi et al., 2022 [51] | RCT/standard treatment | 55 | 72 weeks | Liver biopsy | Reduction in intrahepatic ballooning and fibrosis | Ballooning and fibrosis |
| Ito et al., 2017 [48] | RCT/pioglitazone | 66 | 24 weeks | CT | Change in L/S ratio | L/S ratio |
| Han et al., 2020 [50] | RCT/metformin + pioglitazone | 45 | 24 weeks | FibroScan CT | Improvement in CAP; reduction in VFA | CAP, VFA |
| Author | Design/Comparator | Number of Patients | Study Duration | Method of Diagnosis | Outcome | Measure Method |
|---|---|---|---|---|---|---|
| ToPiND study (tofogliflozin 20 mg/day, 2021) [52] | RCT/pioglitazone | 40 | 24 weeks | MRI-PDFF | Change in MRI-PDFF | Hepatic fat fraction on MRI-PDFF |
| Takeshita et al., (tofogliflozin 20 mg/day, 2022) [53] | RCT/glimepiride | 40 | 48 weeks | Liver biopsy; FibroScan | Change in hepatocellular ballooning, inflammation, and lobular fibrosis | CAP; LSM; hepatocellular ballooning, inflammation, and lobular fibrosis |
| Shibuya et al., (luseogliflozin 2.5 mg/day, 2017) [49] | RCT/metformin | 32 | 6 months | CT | Change in L/S ratio | L/S ratio |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bica, I.-C.; Stoica, R.A.; Salmen, T.; Janež, A.; Volčanšek, Š.; Popovic, D.; Muzurovic, E.; Rizzo, M.; Stoian, A.P. The Effects of Sodium-Glucose Cotransporter 2-Inhibitors on Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease or Steatohepatitis and Type 2 Diabetes: A Systematic Review of Randomized Controlled Trials. Medicina 2023, 59, 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061136
Bica I-C, Stoica RA, Salmen T, Janež A, Volčanšek Š, Popovic D, Muzurovic E, Rizzo M, Stoian AP. The Effects of Sodium-Glucose Cotransporter 2-Inhibitors on Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease or Steatohepatitis and Type 2 Diabetes: A Systematic Review of Randomized Controlled Trials. Medicina. 2023; 59(6):1136. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061136
Chicago/Turabian StyleBica, Ioana-Cristina, Roxana Adriana Stoica, Teodor Salmen, Andrej Janež, Špela Volčanšek, Djordje Popovic, Emir Muzurovic, Manfredi Rizzo, and Anca Pantea Stoian. 2023. "The Effects of Sodium-Glucose Cotransporter 2-Inhibitors on Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease or Steatohepatitis and Type 2 Diabetes: A Systematic Review of Randomized Controlled Trials" Medicina 59, no. 6: 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59061136