


Prediction of Postoperative Creatinine Levels by Artificial Intelligence after Partial Nephrectomy
 , , ,
, , ,
Abstract
:1. Introduction
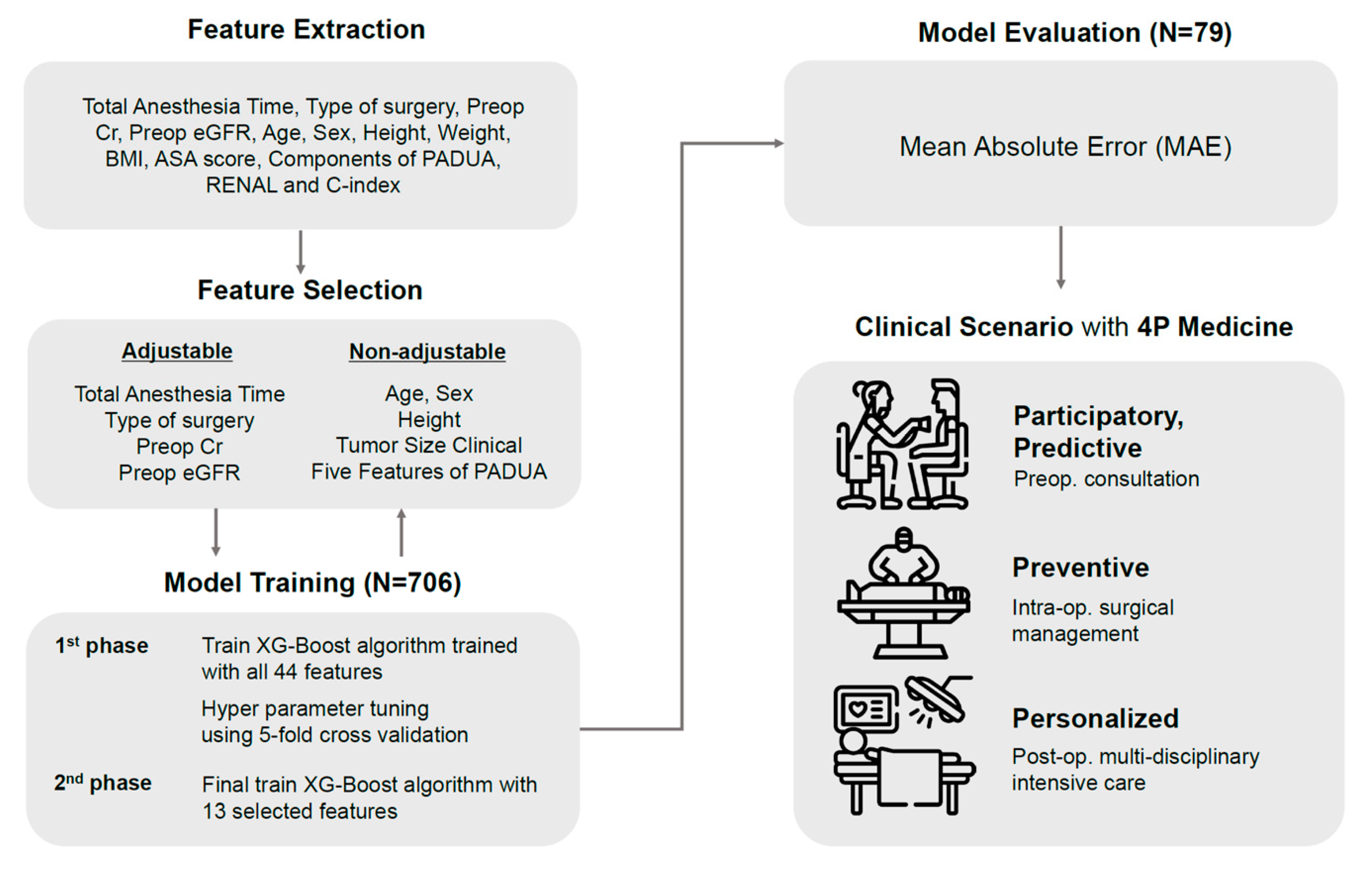
2. Methods
2.1. Study Design and Population
2.2. Data Collection
2.2.1. Preoperative Features
2.2.2. Intraoperative Features
2.3. Model Development
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
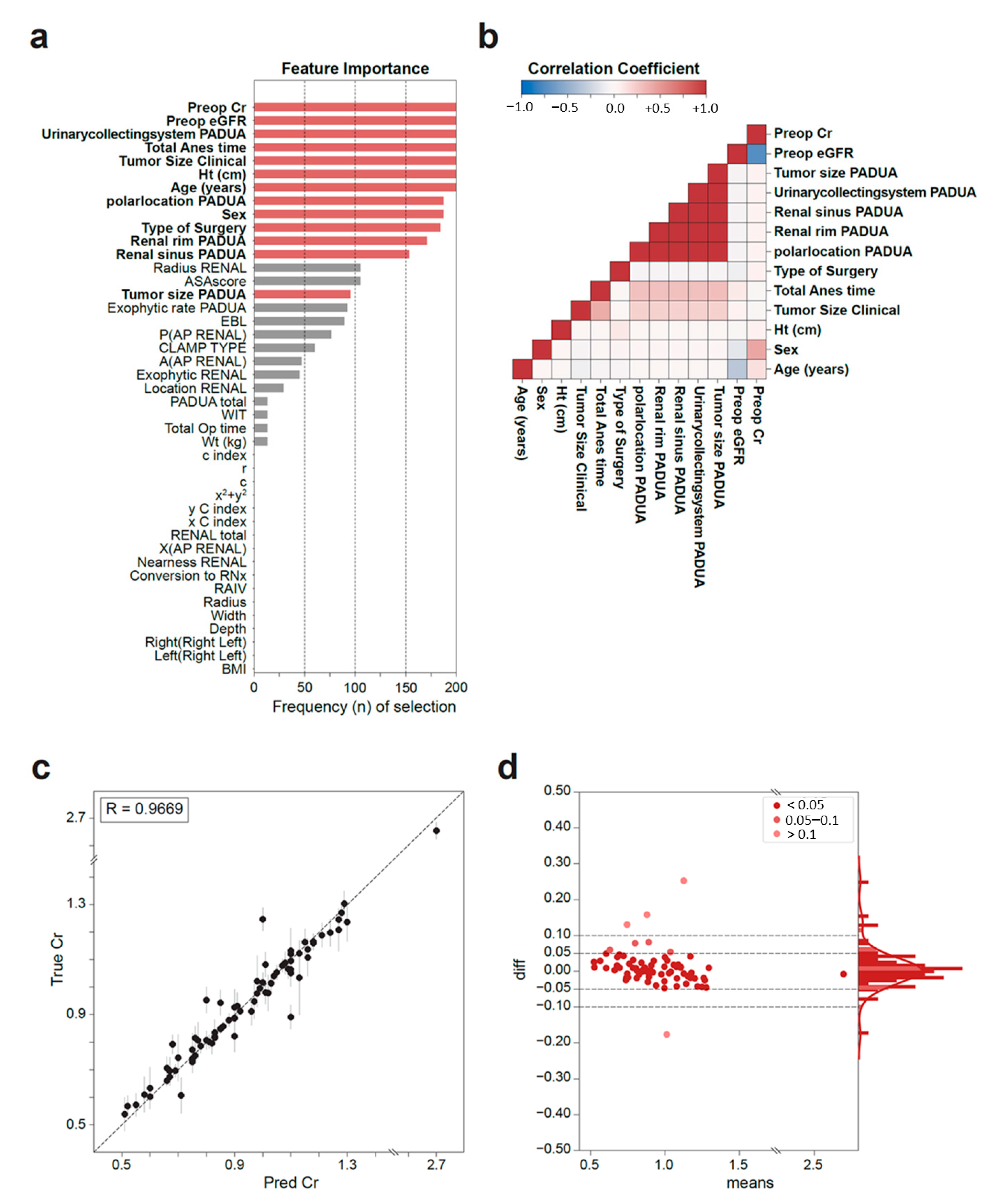
3.1. Feature Importance
3.2. Model Performance
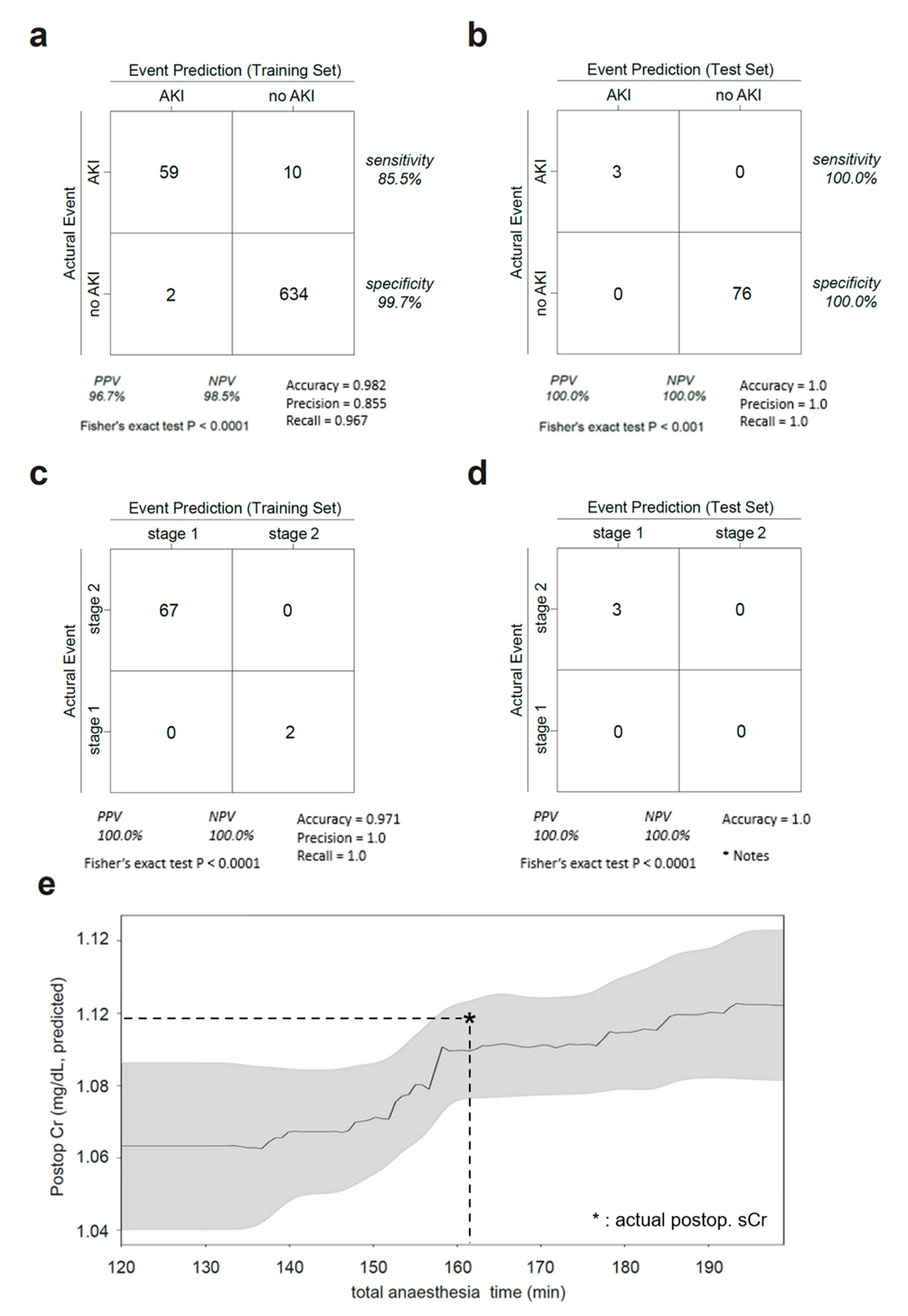
3.3. AKI Prediction
3.4. Clinical Scenario
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simone, G.; De Nunzio, C.; Ferriero, M.; Cindolo, L.; Brookman-May, S.; Papalia, R.; Sperduti, I.; Collura, D.; Leonardo, C.; Anceschi, U.; et al. Trends in the use of partial nephrectomy for cT1 renal tumors: Analysis of a 10-yr European multicenter dataset. Eur. J. Surg. Oncol. 2016, 42, 1729–1735. [Google Scholar] [PubMed]
- Bertolo, R.; Autorino, R.; Simone, G.; Derweesh, I.; Garisto, J.D.; Minervini, A.; Eun, D.; Perdona, S.; Porter, J.; Rha, K.H.; et al. Outcomes of Robot-assisted Partial Nephrectomy for Clinical T2 Renal Tumors: A Multicenter Analysis (ROSULA Collaborative Group). Eur. Urol. 2018, 74, 226–232. [Google Scholar] [PubMed] [Green Version]
- Wang, Z.; Liu, C.; Chen, R.; Liu, S.; Feng, C.; Yu, K.; Zeng, X. Will the kidney function be reduced in patients with renal cell carcinoma following laparoscopic partial nephrectomy? Baseline eGFR, warm ischemia time, and RENAL nephrometry score could tell. Urol. Oncol. 2018, 36, 498.e15–498.e24. [Google Scholar]
- Mir, M.C.; Ercole, C.; Takagi, T.; Zhang, Z.; Velet, L.; Remer, E.M.; Demirjian, S.; Campbell, S.C. Decline in renal function after partial nephrectomy: Etiology and prevention. J. Urol. 2015, 193, 1889–1898. [Google Scholar]
- Lamb, E.J.; Levey, A.S.; Stevens, P.E. The Kidney Disease Improving Global Outcomes (KDIGO) guideline update for chronic kidney disease: Evolution not revolution. Clin. Chem. 2013, 59, 462–465. [Google Scholar]
- Schmid, M.; Krishna, N.; Ravi, P.; Meyer, C.P.; Becker, A.; Dalela, D.; Sood, A.; Chun, F.K.-H.; Kibel, A.S.; Menon, M.; et al. Trends of acute kidney injury after radical or partial nephrectomy for renal cell carcinoma. Urol. Oncol. 2016, 34, 293.e1–293.e10. [Google Scholar]
- Rajan, S.; Babazade, R.; Govindarajan, S.R.; Pal, R.; You, J.; Mascha, E.J.; Khanna, A.; Yang, M.; Marcano, F.; Singh, A.; et al. Perioperative factors associated with acute kidney injury after partial nephrectomy. Br. J. Anaesth. 2016, 116, 70–76. [Google Scholar]
- Bravi, C.A.; Vertosick, E.; Benfante, N.; Tin, A.; Sjoberg, D.; Hakimi, A.A.; Touijer, K.; Montorsi, F.; Eastham, J.; Russo, P.; et al. Impact of Acute Kidney Injury and Its Duration on Long-term Renal Function after Partial Nephrectomy. Eur. Urol. 2019, 76, 398–403. [Google Scholar]
- Kerr, M.; Bedford, M.; Matthews, B.; O’Donoghue, D. The economic impact of acute kidney injury in England. Nephrol. Dial. Transplant. 2014, 29, 1362–1368. [Google Scholar]
- Schrier, R.W. Early intervention in acute kidney injury. Nat. Rev. Nephrol. 2010, 6, 56–59. [Google Scholar]
- Bhindi, B.; Lohse, C.M.; Schulte, P.J.; Mason, R.J.; Cheville, J.C.; Boorjian, S.A.; Leibovich, B.C.; Thompson, R.H. Predicting Renal Function Outcomes after Partial and Radical Nephrectomy. Eur. Urol. 2019, 75, 766–772. [Google Scholar] [PubMed]
- Ficarra, V.; Novara, G.; Secco, S.; Macchi, V.; Porzionato, A.; De Caro, R.; Artibani, W. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumours in patients who are candidates for nephron-sparing surgery. Eur. Urol. 2009, 56, 786–793. [Google Scholar] [PubMed]
- Kutikov, A.; Uzzo, R.G. The R.E.N.A.L. nephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J. Urol. 2009, 182, 844–853. [Google Scholar]
- Shin, T.Y.; Komninos, C.; Kim, D.W.; So, K.S.; Bang, K.S.; Jeong, H.-J.; Han, W.K.; Hong, S.J.; Jung, B.H.; Lim, S.K.; et al. A novel mathematical model to predict the severity of postoperative functional reduction before partial nephrectomy: The importance of calculating resected and ischemic volume. J. Urol. 2015, 193, 423–429. [Google Scholar]
- Dagenais, J.; Maurice, M.J.; Mouracade, P.; Kara, O.; Nelson, R.J.; Malkoc, E.; Kaouk, J.H. The Synergistic Influence of Ischemic Time and Surgical Precision on Acute Kidney Injury after Robotic Partial Nephrectomy. Urology 2017, 107, 132–137. [Google Scholar] [PubMed]
- Tomašev, N.; Glorot, X.; Rae, J.W.; Zielinski, M.; Askham, H.; Saraiva, A.; Mottram, A.; Meyer, C.; Ravuri, S.; Protsyuk, I.; et al. A clinically applicable approach to continuous prediction of future acute kidney injury. Nature 2019, 572, 116–119. [Google Scholar] [PubMed]
- Haug, C.J.; Drazen, J.M. Artificial intelligence and machine learning in clinical medicine, 2023. N. Engl. J. Med. 2023, 388, 1201–1208. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Chen, X.; Kunasekaran, M.; Quigley, A.; Lim, S.; Stone, H.; Paik, H.-Y.; Yao, L.; Heslop, D.; Wei, W.; et al. Artificial intelligence in public health: The potential of epidemic early warning systems. J. Int. Med. Res. 2023, 51, 30000605231159335. [Google Scholar]
- Zhu, K.; Song, H.; Zhang, Z.; Ma, B.; Bao, X.; Zhang, Q.; Jin, J. Acute kidney injury in solitary kidney patients after partial nephrectomy: Incidence, risk factors and prediction. Transl. Androl. Urol. 2020, 9, 1232–1243. [Google Scholar]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar]
- Simmons, M.N.; Ching, C.B.; Samplaski, M.K.; Park, C.H.; Gill, I.S. Kidney tumor location measurement using the C index method. J. Urol. 2010, 183, 1708–1713. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, V.; Porpiglia, F.; Crestani, A.; Minervini, A.; Antonelli, A.; Longo, N.; Novara, G.; Giannarini, G.; Fiori, C.; Simeone, C.; et al. The Simplified PADUA REnal (SPARE) nephrometry system: A novel classification of parenchymal renal tumours suitable for partial nephrectomy. BJU Int. 2019, 125, 621–628. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. arXiv 2016, arXiv:1603.02754. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Development Core Team: Vienna, Austria, 2010; 3-900051-07-0. [Google Scholar]
- Orth, M.; Averina, M.; Chatzipanagiotou, S.; Faure, G.; Haushofer, A.; Kusec, V.; Machado, A.; Misbah, S.A.; Oosterhuis, W.; Pulkki, K.; et al. Opinion: Redefining the role of the physician in laboratory medicine in the context of emerging technologies, personalised medicine and patient autonomy (‘4P medicine’). J. Clin. Pathol. 2019, 72, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chadaga, K.; Prabhu, S.; Bhat, V.; Sampathila, N.; Umakanth, S.; Chadaga, R. A Decision Support System for Diagnosis of COVID-19 from Non-COVID-19 Influenza-like Illness Using Explainable Artificial Intelligence. Bioengineering 2023, 10, 439. [Google Scholar] [CrossRef] [PubMed]
- Khanna, V.V.; Chadaga, K.; Sampathila, N.; Prabhu, S.; Bhandage, V.; Hegde, G.K. A distinctive explainable machine learning framework for detection of polycystic ovary syndrome. Applied System Innovation. Appl. Syst. Innov. 2023, 6, 32. [Google Scholar] [CrossRef]
- Chadaga, K.; Prabhu, S.; Sampathila, N.; Nireshwalya, S.; Katta, S.S.; Tan, R.-S.; Acharya, U.R. Application of artificial intelligence techniques for monkeypox: A systematic review. Diagnostics 2023, 13, 824. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Rajkomar, A.; Oren, E.; Chen, K.; Dai, A.M.; Hajaj, N.; Hardt, M.; Liu, P.J.; Liu, X.; Marcus, J.; Sun, M.; et al. Scalable and accurate deep learning with electronic health records. NPJ Digit. Med. 2018, 1, 18. [Google Scholar] [CrossRef]
- Choi, E.; Bahadori, M.T.; Schuetz, A.; Stewart, W.F.; Sun, J. Doctor AI: Predicting clinical events via recurrent neural networks. JMLR Work. Conf. Proc. 2016, 56, 301–318. [Google Scholar]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Ibarrola, R.; Hein, S.; Reis, G.; Gratzke, C.; Miernik, A. Current and future applications of machine and deep learning in urology: A review of the literature on urolithiasis, renal cell carcinoma, and bladder and prostate cancer. World J. Urol. 2020, 38, 2329–2347. [Google Scholar] [PubMed]
- Xu, L.; Li, C.; Zhao, L.; Zhou, B.; Luo, C.; Man, X.; Luan, H.; Che, L.; Wang, Y.; Xu, Y. Acute kidney injury after nephrectomy: A new nomogram to predict postoperative renal function. BMC Nephrol. 2020, 21, 181. [Google Scholar]
- Sykes, L.; Nipah, R.; Kalra, P.; Green, D. A narrative review of the impact of interventions in acute kidney injury. J. Nephrol. 2018, 31, 523–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colli, J.; Martin, B.; Purcell, M.; Kim, Y.I.; Busby, E.J. Surgical factors affecting return of renal function after partial nephrectomy. Int. Urol. Nephrol. 2011, 43, 131–137. [Google Scholar] [CrossRef]
- Mavuduru, R.S.; Sharma, A.P.; Bora, G.S.; Devana, S.K.; Palani, K.; Lal, A.; Kakkar, N.; Singh, S.K.; Mandal, A.K. Comparison of RENAL, PADUA, and C-index scoring systems in predicting perioperative outcomes after nephron sparing surgery. Indian. J. Urol. 2018, 34, 51–55. [Google Scholar]
- Hew, M.N.; Baseskioglu, B.; Barwari, K.; Axwijk, P.H.; Can, C.; Horenblas, S.; Bex, A.; de la Rosette, J.; Pes, M.L. Critical appraisal of the PADUA classification and assessment of the R.E.N.A.L. nephrometry score in patients undergoing partial nephrectomy. J. Urol. 2011, 186, 42–46. [Google Scholar] [CrossRef]
- Mutasa, S.; Sun, S.; Ha, R. Understanding artificial intelligence based radiology studies: What is overfitting? Clin. Imaging 2020, 65, 96–99. [Google Scholar]
- Corradi, R.; Kabra, A.; Suarez, M.; Oppenheimer, J.; Okhunov, Z.; White, H.; Nougaret, S.; Vargas, H.A.; Landman, J.; Coleman, J.; et al. Validation of 3D volumetric-based renal function prediction calculator for nephron sparing surgery. Int. Urol. Nephrol. 2017, 49, 615–621. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Data Type | Training Set | Test Set | p-Value | ||
|---|---|---|---|---|---|
| Number of Patients | 706 | 79 | |||
| Patient Physical Status | Age (years) | n | 53.4 ± 12.7 | 50.2 ± 12.0 | 0.478 |
| Sex (Male: Female) | n | 461:244 | 46:32 | ||
| BMI (kg/m2) | n | 24.6 ± 3.6 | 25.2 ± 4.35 | 0.345 | |
| DM (Diabetes Mellitus) | c | 136 | 15 | ||
| HTN (Hypertension) | c | 356 | 36 | ||
| ASA score (1:2:3) | n | 1.52 0.77 | 1.56 0.64 | 0.642 | |
| Tumor Radiology | Location (Left/Right) | c | 335/367 | 38/40 | |
| Depth (cm) | n | 1.74 1.17 | 1.51 0.94 | 0.124 | |
| Width (cm) | n | 1.09 0.23 | 1.13 0.24 | 0.246 | |
| Radius (cm) | n | 1.55 0.87 | 1.34 0.64 | 0.091 | |
| RAIV, resected volume (cm3) | n | 35.9 38.5 | 28.7 20.9 | 0.062 | |
| RAIV, ischemized volume (cm3) | n | 58.8 75.9 | 42.2 38.0 | 0.059 | |
| Surgery | Clamp Type (zero ischemia: selective: full) | c | 110: 117: 440 | 11: 20: 44 | |
| Total Operation Time (TOT, min) | n | 177.0 78.2 | 164.5 75.6 | 0.134 | |
| Total Anesthesia Time (TAT, min) | n | 245.2 86.3 | 237.6 72.4 | 0.541 | |
| Warm Ischemia Time (WIT, min) | n | 21.3 12.7 | 20.3 11.7 | 0.633 | |
| Type of Surgery (Robot: Open) | n | 620: 38 | 73: 1 | ||
| Estimated Blood Loss (EBL, mL) | n | 498.6 715.4 | 376.3 355.6 | 0.111 | |
| Conversion to Radical Nephrectomy (True/False) | n | 10:427 | 0:37 | ||
| Sliding clip renorrhapy (n) | c | 625 | 65 | ||
| Use of reno-protective agents | c | 34 | 6 | ||
| PADUA Score * | Polar location (upper/lower: medium) | c | 407:270 | 38:39 | |
| Exophytic rate (≥50%:<50%: endophytic) | c | 224:330:123 | 21:41:15 | ||
| Rim location (lateral: medial) | c | 454:223 | 46:31 | ||
| Renal sinus involvement (absent not: present) | c | 400:277 | 39:38 | ||
| Sinus/UCS involvement (absent: sinus only: UCS only: both) | c | 392:277:7:1 | 38:38:1:0 | ||
| Tumor size (cm) (≤4:4.1–7:>7) | c | 516:135:26 | 60:16:1 | ||
| PADUA total (score) | n | 8.70 1.77 | 9.06 1.78 | 0.125 | |
| RENAL Score | Radius (≤4:>4 but 7:>7) | c | 510:136:31 | 60:16:1 | |
| Exophytic properties (≥50%:<50%: endophytic) | c | 228:326:122 | 24:39:14 | ||
| Nearness to Sinus or UCS (mm) (≥7:>4 but <7:≤4) | c | 249:108:320 | 22:15:40 | ||
| Location to coronal plane Anterior (A): Posterior (P): Neither (X) | c | 328:329:18 | 38:38:1 | ||
| Location to polar line (upper/lower: cross: across or midline) | c | 277:206:194 | 37:16:24 | ||
| RENAL total (score) | n | 6.11 2.11 | 6.60 2.00 | 0.411 | |
| Centrality Index (C-index) | (cm) | n | 2.04 2.20 | 2.84 4.65 | 0.365 |
| (cm) | n | 2.90 4.96 | 4.30 7.01 | <0.05 | |
| n | 41.8 232.8 | 94.6 239.1 | <0.05 | ||
| c | n | 3.87 5.19 | 5.78 7.97 | <0.05 | |
| r | n | 1.53 0.86 | 1.36 0.61 | 0.123 | |
| C-index (score) | n | 2.72 3.27 | 3.20 4.06 | 0.241 | |
| Renal Function | Preop eGFR (mL/min/1.73 m2) | n | 87.1 26.2 | 91.8 22.8 | 0.289 |
| Preoperative serum Cr (mg/dL) | n | 0.90 0.28 | 0.85 0.25 | 0.124 | |
| Postoperative day 0 serum Cr (mg/dL) | n | 1.01 0.33 | 0.94 0.28 | 0.223 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, T.Y.; Han, H.; Min, H.-S.; Cho, H.; Kim, S.; Park, S.Y.; Kim, H.J.; Kim, J.H.; Lee, Y.S. Prediction of Postoperative Creatinine Levels by Artificial Intelligence after Partial Nephrectomy. Medicina 2023, 59, 1402. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59081402
Shin TY, Han H, Min H-S, Cho H, Kim S, Park SY, Kim HJ, Kim JH, Lee YS. Prediction of Postoperative Creatinine Levels by Artificial Intelligence after Partial Nephrectomy. Medicina. 2023; 59(8):1402. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59081402
Chicago/Turabian StyleShin, Tae Young, Hyunho Han, Hyun-Seok Min, Hyungjoo Cho, Seonggyun Kim, Sung Yul Park, Hyung Joon Kim, Jung Hoon Kim, and Yong Seong Lee. 2023. "Prediction of Postoperative Creatinine Levels by Artificial Intelligence after Partial Nephrectomy" Medicina 59, no. 8: 1402. https://0-doi-org.brum.beds.ac.uk/10.3390/medicina59081402