Angiogenesis Inhibitors as Anti-Cancer Therapy Following Renal Transplantation: A Case Report and Review of the Literature

 , ,
, ,
Abstract
:1. Introduction
2. Case Description
3. Discussion
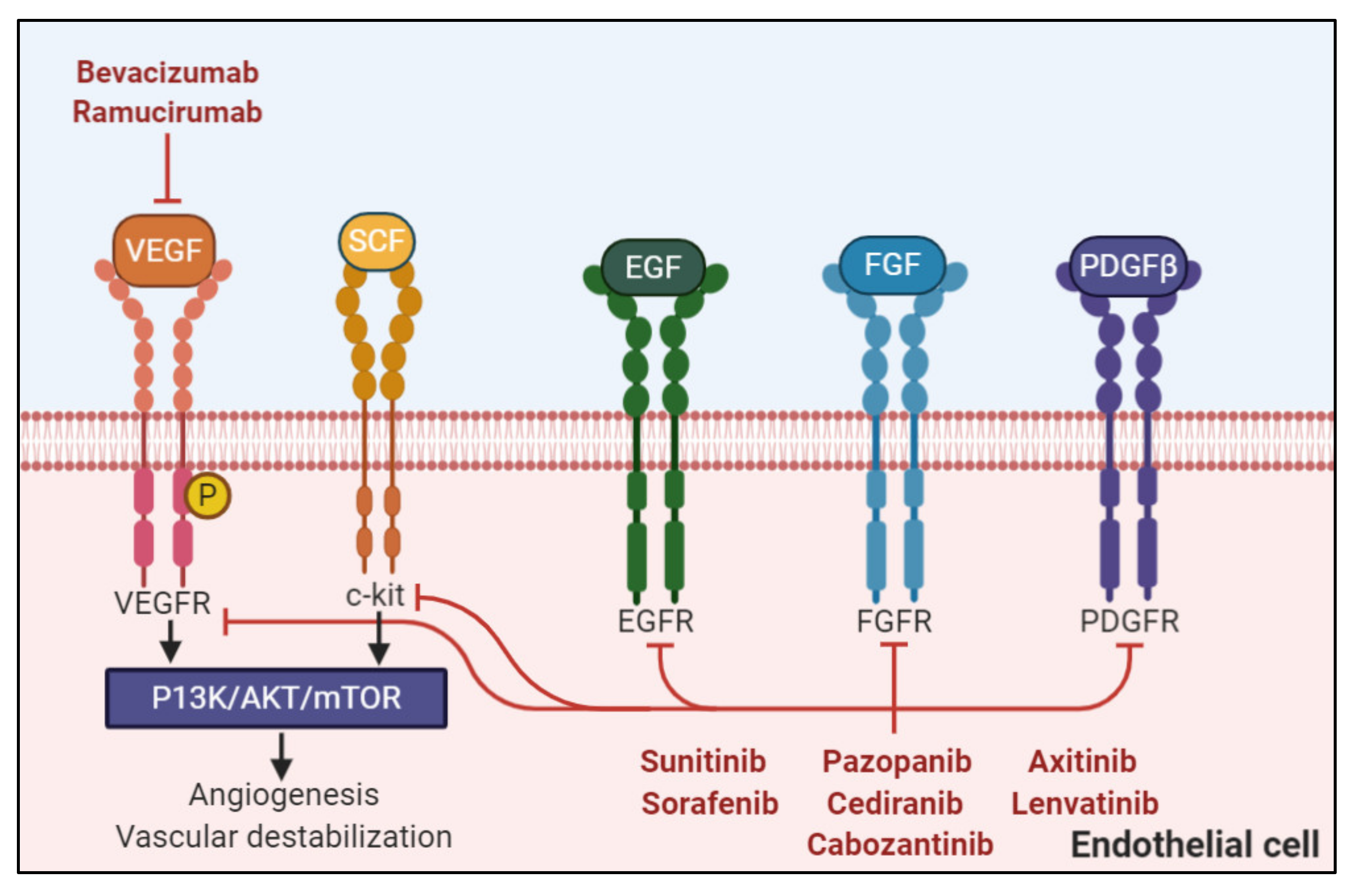
3.1. Angiogenesis Inhibitors Post-Transplant
3.2. Medication Interactions
3.3. Long-Term Adverse Events
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| VEGFR | vascular endothelial growth factor receptor |
| EGFR | epidermal growth factor receptor |
| FGFR | fibroblast growth factor receptor |
| PDGFR | platelet-derived growth factor receptor |
| SCF | stem cell factor |
| PI3K | phosphoinositide 3-kinase |
| AKT | protein kinase B |
| mTOR | mammalian target of rapamycin |
| RET | RET proto-oncogene |
| AXL | AXL receptor tyrosine kinase |
| TAH–BSO | total abdominal hysterectomy and bilateral salpingo-oophorectomy |
| Ca125 | cancer antigen 125 |
| U/ml | units per milliliter |
| AKI | acute kidney injury |
| CYP | cytochrome P450 |
| HGSOC | high-grade serous ovarian carcinoma |
| FOLFOX4 | 5-fluorouracil, leucovorin, and oxaliplatin |
| IFL | irinotecan, leucovorin, and 5-fluorouracil |
| P-gp | P-glycoprotein |
References
- National Comprehensive Cancer Network. Ovarian Cancer (Version 1.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf (accessed on 31 August 2020).
- Gurevich, F.; Perazella, M.A. Renal effects of anti-angiogenesis therapy: Update for the internist. Am. J. Med. 2009, 122, 322–328. [Google Scholar] [CrossRef]
- Touyz, R.M.; Herrmann, S.M.; Herrmann, J. Vascular toxicities with VEGF inhibitor therapies–Focus on hypertension and arterial thrombotic events. J. Am. Soc. Hypertens. 2018, 12, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-F.; Wang, T.; Liu, L.-H.; Guo, H.-Q. Risks of proteinuria associated with vascular endothelial growth factor receptor tyrosine kinase inhibitors in cancer patients: A systematic review and meta-analysis. PLoS ONE 2014, 9, e90135. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Kim, C.; Baer, L.; Zhu, X. Bevacizumab increases risk for severe proteinuria in cancer patients. J. Am. Soc. Nephrol. 2010, 21, 1381–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ollero, M.; Sahali, D. Inhibition of the VEGF signalling pathway and glomerular disorders. Nephrol. Dial. Transplant. 2015, 30, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Hanna, R.M.; López, E.; Wilson, J.; Barathan, S.; Cohen, A.H. Minimal change disease onset observed after bevacizumab administration. Clin. Kidney J. 2015, 9, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Hayman, S.R.; Leung, N.; Grande, J.P.; Garovic, V.D. VEGF inhibition, hypertension, and renal toxicity. Curr. Oncol. Rep. 2012, 14, 285–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenoglio, R.; Roccatello, D. Bevacizumab: Renal safety evaluation. J. Onco Nephrol. 2017, 1, 198–203. [Google Scholar] [CrossRef]
- Pandey, A.K.; Singhi, E.K.; Arroyo, J.P.; Ikizler, T.A.; Gould, E.R.; Brown, J.; Beckman, J.A.; Harrison, D.G.; Moslehi, J. Mechanisms of VEGF (Vascular Endothelial Growth Factor) inhibitor–Associated hypertension and vascular disease. Hypertension 2018, 71, e1–e8. [Google Scholar] [CrossRef]
- Estrada, C.C.; Maldonado, A.; Mallipattu, S.K. Therapeutic inhibition of VEGF signaling and associated nephrotoxicities. J. Am. Soc. Nephrol. 2019, 30, 187–200. [Google Scholar] [CrossRef] [Green Version]
- Izzedine, H. Anti-VEGF cancer therapy in nephrology practice. Int. J. Nephrol. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, K.P.; Seifert, M.E.; Chandraker, A.; Zurakowski, D.; Nohria, A.; Givertz, M.M.; Karumanchi, S.A.; Briscoe, D.M. VEGF-C, VEGF-A and related angiogenesis factors as biomarkers of allograft vasculopathy in cardiac transplant recipients. J. Hear. Lung Transplant. 2013, 32, 120–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rintala, S.; Savikko, J.; Rintala, J.; Von Willebrand, E. Vascular Endothelial Growth Factor (VEGF) ligand and receptor induction in rat renal allograft rejection. Transplant. Proc. 2006, 38, 3236–3238. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Abuduwufuer, A.; Lv, W.; Zhou, Z.; Yang, Y.; Zhang, C.; Hu, J. The role of HIF-1α-VEGF pathway in bronchiolitis obliterans after lung transplantation. J. Cardiothorac. Surg. 2019, 14, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Kim, R.; Quintini, C.; Hashimoto, K.; Fujiki, M.; Diago, T.; Eghtesad, B.; Miller, C.; Fung, J.F.; Tan, A.; et al. Prognostic role of plasma vascular endothelial growth factor in patients with hepatocellular carcinoma undergoing liver transplantation. Liver Transplant. 2014, 21, 101–111. [Google Scholar] [CrossRef]
- Daly, K.P.; Stack, M.; Eisenga, M.F.; Keane, J.F.; Zurakowski, D.; Blume, E.D.; Briscoe, D.M. Vascular endothelial growth factor A is associated with the subsequent development of moderate or severe cardiac allograft vasculopathy in pediatric heart transplant recipients. J. Hear. Lung Transplant. 2017, 36, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Drugs@FDA: FDA-Approved Drugs. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/125085s332lbl.pdf (accessed on 31 August 2020).
- Aghajanian, C.; Goff, B.; Nycum, L.R.; Wang, Y.V.; Husain, A.; Blank, S.V. Final overall survival and safety analysis of OCEANS, a phase 3 trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent ovarian cancer. Gynecol. Oncol. 2015, 139, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.B.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; A Ledermann, J.; Pujade-Lauraine, E.; Kristensen, G.B.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Müsri, F.Y.; Mutlu, H.; Eryılmaz, M.K.; Salim, D.K.; Coşkun, H.Ş. Experience of bevacizumab in a patient with colorectal cancer after renal transplantation. J. Cancer Res. Ther. 2015, 11, 1018–1020. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Chebib, F.T.; Cornell, L.D.; Brodin, M.L.; Nasr, S.H.; Schinstock, C.; Stegall, M.D.; Amer, H. Intravitreal antivascular endothelial growth factor therapy may induce proteinuria and antibody mediated injury in renal allografts. Transplantation 2015, 99, 2382–2386. [Google Scholar] [CrossRef] [PubMed]
- Jonkers, I.; van Buren, M. Nephrotic-range proteinuria in a patient with a renal allograft treated with sorafenib for metastatic renal-cell carcinoma. Clin. Exp. Nephrol. 2009, 13, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Fogli, S.; Porta, C.; Del Re, M.; Crucitta, S.; Gianfilippo, G.; Danesi, R.; Rini, B.I.; Schmidinger, M. Optimizing treatment of renal cell carcinoma with VEGFR-TKIs: A comparison of clinical pharmacology and drug-drug interactions of anti-angiogenic drugs. Cancer Treat. Rev. 2020, 84, 101966. [Google Scholar] [CrossRef] [PubMed]
- Danovitch, G. Handbook of Transplantation (Immunosuppressive Medications and Protocols for Kidney Transplantation), 6th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2017. [Google Scholar]
- Gibardi, S.; Tichy, E.M. Overview of immunosuppressive therapies in renal trans-plantation. In Core Concepts in Renal Transplantation; Chandrakar, A., Sayegh, M.H., Singh, A.J., Eds.; Springer: New York, NY, USA, 2012; Available online: https://0-link-springer-com.brum.beds.ac.uk/book/10.1007%2F978-1-4614-0008-0 (accessed on 1 September 2020).
- Pfizer Products ULC. Inlyta; [Product Monograph]; Pfizer Products ULC: Kirkland, QC, Canada, 2020. [Google Scholar]
- Bayer Inc. Nexavar; [Product Monograph]; Bayer Inc.: Mississauga, ON, Canada, 2020. [Google Scholar]
- Ipsen Biopharmaceuticals Canada Inc. Cabometyx; [Product Monograph]; Ipsen Biopharmaceuticals Canada Inc.: Mississauga, ON, Canada, 2020. [Google Scholar]
- Novartis Pharmaceuticals Canada Inc. Votrient; [Product Monograph]; Novartis Pharmaceuticals Canada Inc.: Dorval, QC, Canada, 2020. [Google Scholar]
- Enderby, C.Y.; Keller, C.A. An overview of immunosuppression in solid organ transplantation. Am. J. Manag. Care 2015, 21, S12–S23. [Google Scholar]
- Ghatalia, P.; Je, Y.; Kaymakcalan, M.D.; Sonpavde, G.; Choueiri, T.K. QTc interval prolongation with vascular endothelial growth factor receptor tyrosine kinase inhibitors. Br. J. Cancer 2014, 112, 296–305. [Google Scholar] [CrossRef] [Green Version]
- Onodera, R.; Nihei, S.; Kimura, T.; Tomita, T.; Kudo, K. Severe proteinuria during the administration of bevacizumab plus mFOLFOX6 in a colorectal cancer patient after kidney transplantation: A case report. J. Pharm. Health Care Sci. 2020, 6, 1–5. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of cancer risk among US solid organ transplant recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Acuna, S.A.; Huang, J.W.; Scott, A.L.; Micic, S.; Daly, C.; Brezden-Masley, C.; Kim, S.J.; Baxter, N.N. Cancer screening recommendations for solid organ transplant recipients: A systematic review of clinical practice guidelines. Arab. Archaeol. Epigr. 2017, 17, 103–114. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Ethier, J.-L.; Lee, D.S.; Thavendiranathan, P.; Amir, E. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 53, 120–127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cancer | Stage | Usage |
|---|---|---|
| Colorectal | Metastatic, first-line | 5 mg/kg every two weeks with bolus IFL 10 mg/kg every two weeks with FOLFOX4 |
| Metastatic, recurrent after first-line bevacizumab-containing regimen | 5 mg/kg every two weeks, or 7.5 mg/kg every three weeks with fluoropyrimidine–irinotecan, or fluoropyrimidine–oxaliplatin-based chemotherapy | |
| Non-squamous, non-small-cell lung | Unresectable, locally advanced, recurrent, or metastatic | 15 mg/kg every three weeks with carboplatin and paclitaxel |
| Glioblastoma | Recurrent | 10 mg/kg every two weeks |
| Renal cell | Metastatic | 10 mg/kg every two weeks with interferon-alfa |
| Cervical | Persistent, recurrent, or metastatic | 15 mg/kg every three weeks with paclitaxel and cisplatin, or paclitaxel and topotecan |
| Epithelial ovarian, fallopian tube, or primary peritoneal | III or IV, following surgical resection | 15 mg/kg every three weeks with carboplatin and paclitaxel for up to six cycles, followed by 15 mg/kg every three weeks as a single agent for up to 22 cycles |
| Recurrent, platinum-sensitive | 15 mg/kg every three weeks with carboplatin and either paclitaxel (6–8 cycles) or gemcitabine (6–10 cycles) followed by 15 mg/kg every 3 weeks as a single agent | |
| Recurrent, platinum-resistant | 10 mg/kg every two weeks with paclitaxel, pegylated liposomal doxorubicin, or topotecan given weekly 15 mg/kg every three weeks with topotecan every three weeks | |
| Hepatocellular | Unresectable or metastatic, first-line | 15 mg/kg with atezolizumab every three weeks |
| Transplant Medication | Potential Interactions with Anti-Angiogenesis Agents [26,27,28,29,30,31,32,33,34] |
|---|---|
| Cyclosporine | Increased cyclosporine levels and subsequent toxicity due to CYP3A4 and P-gp-mediated drug interactions (e.g., cabozatinib, axitinib, pazopanib, sorafenib, sunitinib) |
| Tacrolimus | Increased tacrolimus levels and subsequent toxicity due to inhibition of or competition with CYP3A4 metabolism and P-gp-mediated transport (e.g., cabozatinib, axitinib, pazopanib, sorafenib, sunitinib) Additive impairment of the renal function (e.g., cediranib, axitinib, pazopanib) Increased risk of QT prolongation with other agents that prolong the QT interval (e.g., cabozantinib, pazopanib, sorafenib, sunitinib) |
| Mycophenolate mofetil | Exaggerated leukopenia (e.g., ramucirumab, bevacizumab, sunitinib) |
| Azathioprine | Exaggerated leukopenia (e.g., ramucirumab, bevacizumab, sunitinib) |
| Sirolimus | Increased tacrolimus levels and subsequent toxicity due to inhibition of or competition with CYP3A4 metabolism and P-gp-mediated transport (e.g., cabozatinib, axitinib, pazopanib, sorafenib, sunitinib) Additive impairment of the renal function (e.g., cediranib, axitinib, pazopanib) Additive impairment of wound healing |
| Everolimus | Increased everolimus levels and subsequent toxicity due to inhibition of CYP3A4 metabolism and P-gp-mediated transport (e.g., cabozantinib, pazopanib) Additive impairment of the renal function (e.g., cediranib, axitinib, pazopanib) Additive impairment of wound healing |
| Corticosteroids | Competitive CYP3A4 metabolism (e.g., prednisone) with other CYP3A4 substrates (e.g., cabozantinib, axitinib, pazopanib, sorafenib, sunitinib) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasherman, L.; Doi, J.; Karakasis, K.; Schiff, J.; Kitchlu, A.; Lheureux, S.; Oza, A.M. Angiogenesis Inhibitors as Anti-Cancer Therapy Following Renal Transplantation: A Case Report and Review of the Literature. Curr. Oncol. 2021, 28, 661-670. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010064
Kasherman L, Doi J, Karakasis K, Schiff J, Kitchlu A, Lheureux S, Oza AM. Angiogenesis Inhibitors as Anti-Cancer Therapy Following Renal Transplantation: A Case Report and Review of the Literature. Current Oncology. 2021; 28(1):661-670. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010064
Chicago/Turabian StyleKasherman, Lawrence, Jeffrey Doi, Katherine Karakasis, Jeffrey Schiff, Abhijat Kitchlu, Stephanie Lheureux, and Amit M. Oza. 2021. "Angiogenesis Inhibitors as Anti-Cancer Therapy Following Renal Transplantation: A Case Report and Review of the Literature" Current Oncology 28, no. 1: 661-670. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28010064