Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns?

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Background
2.1. Colorectal Cancer in Canada
2.2. Role of Screening
2.3. Common Screening Tests
3. CRC Screening in Canada
3.1. Guidelines Published in Canada
3.2. Provincially Organized Screening Programs
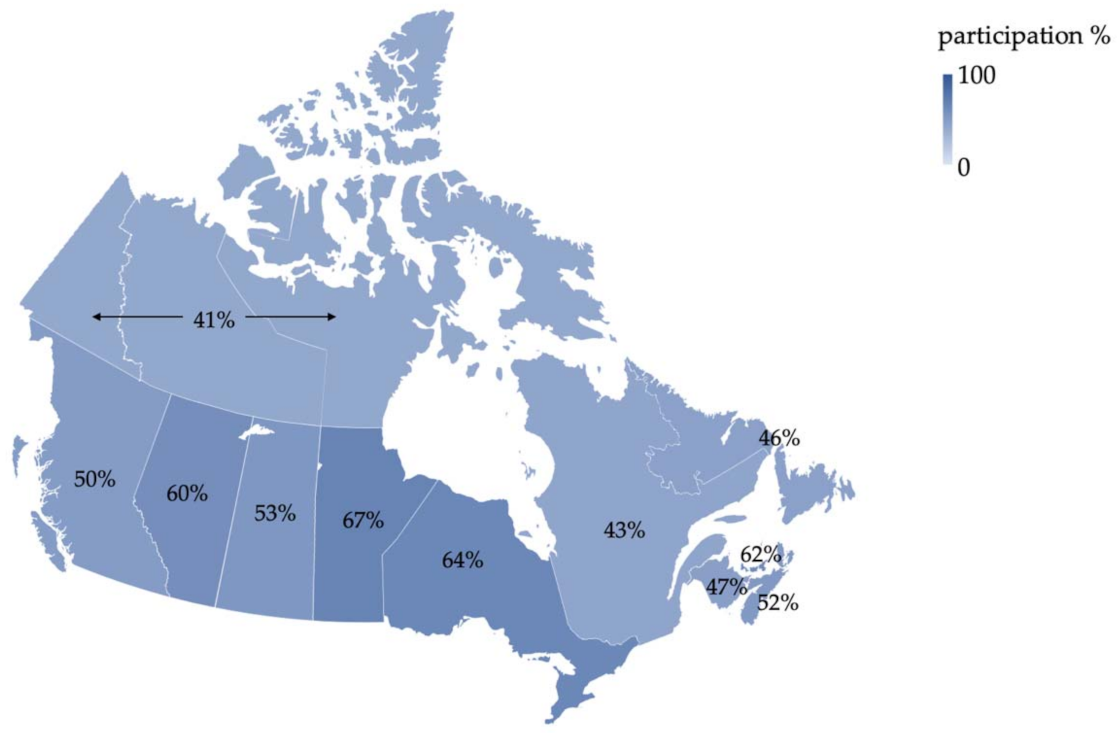
3.3. Screening Participation in Canada
4. CRC Screening in the United States
5. CRC Screening in Europe
5.1. France
5.2. The Netherlands
5.3. United Kingdom
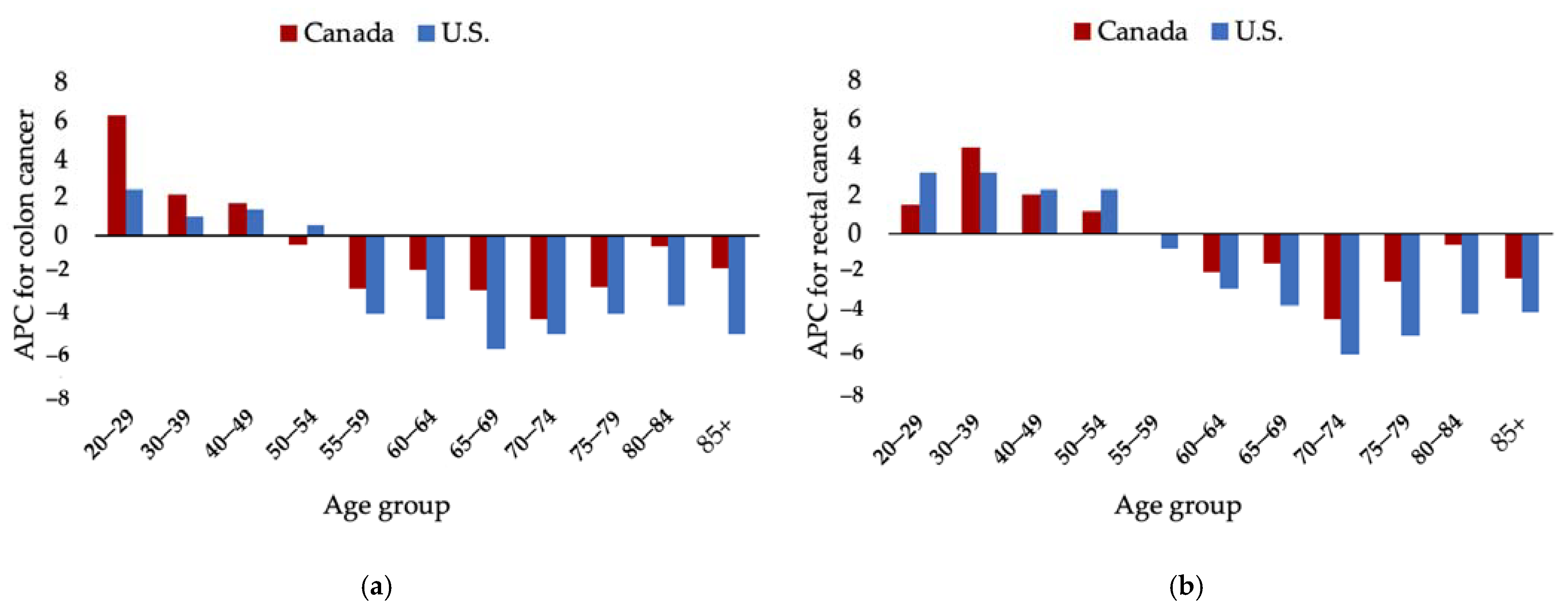
6. Early-Onset CRC in the U.S.
7. Early-Onset CRC in Canada
8. Modeling Studies—U.S.
9. Modeling Studies—Canada
10. Future Screening Strategies
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019. [Google Scholar]
- Brenner, D.R.; Weir, H.K.; Demers, A.A.; Ellison, L.F.; Louzado, C.; Shaw, A.; Turner, D.; Woods, R.R.; Smith, L.M. Projected estimates of cancer in Canada in 2020. CMAJ 2020, 192, E199–E205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Task Force on Preventive Health Care. Appendix 5: Economic implications of screening. CMAJ 2016. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Ansa, B.E.; Coughlin, S.S.; Alema-Mensah, E.; Smith, S.A. Evaluation of colorectal cancer incidence trends in the United States (2000–2014). J. Clin. Med. 2018, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Austin, H.; Henley, S.J.; King, J.; Richardson, L.C.; Eheman, C. Changes in colorectal cancer incidence rates in young and older adults in the United States: What does it tell us about screening. Cancer Causes Control 2014, 25, 191–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.-C.T.; et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef]
- Canadian Task Force on Preventive Health Care. Canadian colon cancer screening guidelines. CMAJ 2016, 188, 1–9. [Google Scholar] [CrossRef]
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics: A 2018 Special Report on Cancer Incidence by Stage; Canadian Cancer Society: Toronto, ON, Canada, 2018. [Google Scholar]
- Brenner, D.R.; Heer, E.; Sutherland, R.L.; Ruan, Y.; Tinmouth, J.; Heitman, S.J.; Hilsden, R.J. National trends in colorectal cancer incidence among older and younger adults in Canada. JAMA Netw. Open 2019, 2. [Google Scholar] [CrossRef] [Green Version]
- Araghi, M.; Soerjomataram, I.; Bardot, A.; Ferlay, J.; Cabasag, C.J.; Morrison, D.S.; De, P.; Tervonen, H.; Walsh, P.M.; Bucher, O.; et al. Changes in colorectal cancer incidence in seven high-income countries: A population-based study. Lancet. Gastroenterol. Hepatol. 2019, 4, 511–518. [Google Scholar] [CrossRef]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal cancer incidence patterns in the United States, 1974-2013. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [Green Version]
- Bailey, C.E.; Hu, C.Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing disparities in the age-related incidences of colon and rectal cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef]
- United States Preventive Services Task Force Draft Recommendation Statement-Colorectal Cancer: Screening. Available online: https://www.uspreventiveservicestaskforce.org/uspstf/draft-recommendation/colorectal-cancer-screening3#fullrecommendationstart (accessed on 22 November 2020).
- Lui, R.N.; Tsoi, K.K.F.; Ho, J.M.W.; Lo, C.M.; Chan, F.C.H.; Kyaw, M.H.; Sung, J.J.Y. Global increasing incidence of young-onset colorectal cancer across 5 continents: A joinpoint regression analysis of 1,922,167 cases. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1275–1282. [Google Scholar] [CrossRef] [Green Version]
- Muto, T.; Bussey, H.J.R.; Morson, B.C. The evolution of cancer of the colon and rectum. Cancer 1975, 36, 2251–2270. [Google Scholar] [CrossRef]
- Leddin, D.J.; Enns, R.; Hilsden, R.; Plourde, V.; Rabeneck, L.; Sadowski, D.C.; Singh, H. Canadian Association of Gastroenterology position statement on screening individuals at average risk for developing colorectal cancer: 2010. Can. J. Gastroenterol. 2010, 24, 705–714. [Google Scholar] [CrossRef]
- Pignone, M.; Saha, S.; Hoerger, T.; Mandelblatt, J. Cost-effectiveness analyses of colorectal cancer screening: A systematic review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2002, 137, 96–104. [Google Scholar] [CrossRef]
- Lansdorp-Vogelaar, I.; Knudsen, A.B.; Brenner, H. Epidemiologic reviews cost-effectiveness of colorectal cancer screening. Epidemiol. Rev. 2011, 33, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- Miles, A.; Cockburn, J.; Smith, R.A.; Wardle, J. A perspective from countries using organized screening programs. Cancer 2004, 101, 1201–1213. [Google Scholar] [CrossRef]
- Canadian Partnership Against Cancer. Colorectal Cancer Screening in Canada: Environmental Scan; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2018. [Google Scholar]
- Rabeneck, L.; Rumble, R.B.; Thompson, F.; Mills, M.; Oleschuk, C.; Whibley, A.; Messersmith, H.; Lewis, N. Fecal immunochemical tests compared with guaiac fecal occult blood tests for population-based colorectal cancer screening. Can. J. Gastroenterol. 2012, 26, 131–147. [Google Scholar] [CrossRef]
- Young, G.P.; Symonds, E.L.; Allison, J.E.; Cole, S.R.; Fraser, C.G.; Halloran, S.P.; Kuipers, E.J.; Seaman, H.E. Advances in fecal occult blood tests: The FIT revolution. Dig. Dis. Sci. 2015, 60, 609–622. [Google Scholar] [CrossRef] [Green Version]
- Moss, S.; Mathews, C.; Day, T.J.; Smith, S.; Seaman, H.E.; Snowball, J.; Halloran, S.P. Increased uptake and improved outcomes of bowel cancer screening with a faecal immunochemical test: Results from a pilot study within the national screening programme in England. Gut 2017, 66, 1631–1644. [Google Scholar] [CrossRef]
- Van Rossum, L.G.; Van Rijn, A.F.; Laheij, R.J.; Van Oijen, M.G.; Fockens, P.; Van Krieken, H.H.; Verbeek, A.L.; Jansen, J.B.; Dekker, E. Random comparison of guaiac and immunochemical fecal occult blood tests for colorectal cancer in a screening population. Gastroenterology 2008, 135, 82–90. [Google Scholar] [CrossRef]
- Hol, L.; Wilschut, J.A.; Van Ballegooijen, M.; Van Vuuren, A.J.; Van Der Valk, H.; Reijerink, J.; Van Der Togt, A.; Kuipers, E.J.; Habbema, J.; Van Leerdam, M.E. Screening for colorectal cancer: Random comparison of guaiac and immunochemical faecal occult blood testing at different cut-off levels. Br. J. Cancer 2009, 100, 1103–1110. [Google Scholar] [CrossRef]
- Goede, S.L.; Rabeneck, L.; Van Ballegooijen, M.; Zauber, A.G.; Paszat, L.F.; Hoch, J.S.; Yong, J.H.E.; Kroep, S.; Tinmouth, J.; Lansdorp-Vogelaar, I. Harms, benefits and costs of fecal immunochemical testing versus guaiac fecal occult blood testing for colorectal cancer screening. PLoS ONE 2017, 12, e0172864. [Google Scholar] [CrossRef]
- Fitzpatrick-Lewis, D.; Ali, M.U.; Warren, R.; Kenny, M.; Sherifali, D.; Raina, P. Screening for colorectal cancer: A systematic review and meta-analysis. Clin. Colorectal Cancer 2016, 15, 298–313. [Google Scholar] [CrossRef]
- Cooper, M.A.; Tinmouth, J.M.; Rabeneck, L. Registered nurse-performed flexible sigmoidoscopy in Ontario: Development and implementation of the curriculum and program. Can. J. Gastroenterol. Hepatol. 2014, 28, 13–18. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.R.; Gillman, M.W.; Harper, D.M.; Kemper, A.R.; Krist, A.H.; et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA J. Am. Med. Assoc. 2016, 315, 2564–2575. [Google Scholar] [CrossRef]
- Canadian Cancer Society. How Do I Find a Colorectal Cancer Screening Program? Available online: https://www.cancer.ca/en/prevention-and-screening/reduce-cancer-risk/find-cancer-early/get-screened-for-colorectal-cancer/how-do-i-find-a-colorectal-cancer-screening-program/?region=on (accessed on 24 May 2020).
- Singh, H.; Bernstein, C.N.; Samadder, J.N.; Ahmed, R. Screening rates for colorectal cancer in Canada: A cross-sectional study. CMAJ Open 2015, 3, E149–E157. [Google Scholar] [CrossRef] [Green Version]
- Simkin, J.; Ogilvie, G.; Hanley, B.; Elliott, C. Differences in colorectal cancer screening rates across income strata by levels of urbanization: Results from the Canadian Community Health Survey (2013/2014). Can. J. Public Health 2019, 110, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Torabi, M.; Green, C.; Nugent, Z.; Mahmud, S.M.; Demers, A.A.; Griffith, J.; Singh, H. Geographical variation and factors associated with colorectal cancer mortality in a universal health care system. Can. J. Gastroenterol. Hepatol. 2014, 28, 191–197. [Google Scholar] [CrossRef] [PubMed]
- White, A.; Thompson, T.D.; White, M.C.; Sabatino, S.A.; de Moor, J.; Doria-Rose, P.V.; Geiger, A.M.; Richardson, L.C. Cancer screening test use-United States, 2015. Morb. Mortal. Wkly. Rep. 2017, 66, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calonge, N.; Petitti, D.B.; DeWitt, T.G.; Dietrich, A.J.; Gregory, K.D.; Harris, R.; Isham, G.; LeFevre, M.L.; Leipzig, R.M.; Loveland-Cherry, C.; et al. Screening for colorectal cancer: U.S: Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2008, 149, 637. [Google Scholar] [CrossRef]
- Rex, D.K.; Johnson, D.A.; Anderson, J.C.; Schoenfeld, P.S.; Burke, C.A.; Inadomi, J.M. American College of Gastroenterology guidelines for colorectal cancer screening 2008. Am. J. Gastroenterol. 2009, 104, 739–750. [Google Scholar] [CrossRef]
- The Council of the European Union. Council recommendation of 2 December 2003 on cancer screening. Off. J. Eur. Union 2003, L 327, 34–38. [Google Scholar]
- Segnan, N.; Patnick, J.; von Karsa, L. (Eds.) European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis, 1st ed.; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- Von Karsa, L.; Patnick, J.; Segnan, N. European guidelines for quality assurance in colorectal cancer screening and diagnosis. First edition executive summary. Endoscopy 2012, 44, SE1–SE8. [Google Scholar] [CrossRef] [Green Version]
- Labianca, R.; Nordlinger, B.; Beretta, G.D.; Mosconi, S.; Mandalà, M.; Cervantes, A.; Arnold, D. Early colon cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi64–vi72. [Google Scholar] [CrossRef]
- European Colorectal Cancer Screening Guidelines Working Group. European guidelines for quality assurance in colorectal cancer screening and diagnosis: Overview and introduction to the full supplement publication. Endoscopy 2013, 45, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Altobelli, E.; Lattanzi, A.; Paduano, R.; Varassi, G.; Di Orio, F. Colorectal cancer prevention in Europe: Burden of disease and status of screening programs. Prev Med. 2014, 62, 132–141. [Google Scholar] [CrossRef]
- Bowel Cancer Screening | about Bowel Cancer | Bowel Cancer UK. Available online: https://www.bowelcanceruk.org.uk/about-bowel-cancer/screening/ (accessed on 19 May 2020).
- Koo, S.; Neilson, L.J.; Wagner, C.V.; Rees, C.J. The NHS bowel cancer screening program: Current perspectives on strategies for improvement. Risk Manag. Healthc. Policy 2017, 10, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Cancer Research UK. Bowel Cancer Screening Coverage and Uptake UK, FY2012-2015. Available online: https://www.cancerresearchuk.org/sites/default/files/cstream-node/screen_bowel_cov_upt.pdf (accessed on 20 May 2020).
- Pellat, A.; Deyra, J.; Coriat, R.; Chaussade, S. Results of the national organised colorectal cancer screening program with FIT in Paris. Sci. Rep. 2018, 8, 1–4. [Google Scholar] [CrossRef]
- Leuraud, K.; Jezewski-Serra, D.; Rôme Viguier, J.; Salines, E. Colorectal cancer screening by guaiac faecal occult blood test in France: Evaluation of the programme two years after launching. Cancer Epidemiol. 2013, 37, 959–967. [Google Scholar] [CrossRef]
- Toes-Zoutendijk, E.; Van Leerdam, M.E.; Dekker, E.; Van Hees, F.; Penning, C.; Nagtegaal, I.; Van Der Meulen, M.P.; Van Vuuren, A.J.; Kuipers, E.J.; Bonfrer, J.M.G.; et al. Real-time monitoring of results during first year of dutch colorectal cancer screening program and optimization by altering fecal immunochemical test cut-off levels. Gastroenterology 2017, 152, 767–775. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Public Health and the Environment (Netherlands). Colorectal Cancer Screening Programme. Available online: https://www.rivm.nl/en/colorectal-cancer-screening-programme (accessed on 19 May 2020).
- Bowel Cancer Screening: Programme Overview-GOV.UK. Available online: https://www.gov.uk/guidance/bowel-cancer-screening-programme-overview (accessed on 19 May 2020).
- Mcgregor, L.M.; Bonello, B.; Kerrison, R.S.; Nickerson, C.; Baio, G.; Berkman, L.; Rees, C.J.; Atkin, W.; Wardle, J.; von Wagner, C. Uptake of bowel scope (flexible sigmoidoscopy) screening in the English National Programme: The first 14 months. J. Med. Screen. 2016, 23, 77–82. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Available online: https://gco.iarc.fr/today/online-analysis-map?v=2018&mode=population&mode_population=continents&population=900&popultions=900&key=asr&sex=0&cancer=41&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=9&nb_items=10&gro (accessed on 3 August 2020).
- Brenner, D.R.; Ruan, Y.; Shaw, E.; De, P.; Heitman, S.J.; Hilsden, R.J. Increasing colorectal cancer incidence trends among younger adults in Canada. Prev. Med. 2017, 105, 345–349. [Google Scholar] [CrossRef]
- Abualkhair, W.H.; Zhou, M.; Ahnen, D.; Yu, Q.; Wu, X.C.; Karlitz, J.J. Trends in incidence of early-onset colorectal cancer in the United States among those approaching screening age. JAMA Netw. Open 2020, 3. [Google Scholar] [CrossRef] [Green Version]
- Patel, P.; De, P. Trends in colorectal cancer incidence and related lifestyle risk factors in 15–49-year-olds in Canada, 1969–2010. Cancer Epidemiol. 2016, 42, 90–100. [Google Scholar] [CrossRef]
- Leddin, D.; Hunt, R.; Champion, M.; Cockeram, A.; Flook, N.; Gould, M.; Kim, Y.-I.; Love, J.; Morgan, D.; Natsheh, S.; et al. Canadian Association of Gastroenterology and the Canadian Digestive Health Foundation: Guidelines on colon cancer screening. Can. J. Gastroenterol. 2004, 18, 93–99. [Google Scholar] [CrossRef]
- Peterse, E.F.P.; Meester, R.G.S.; Siegel, R.L.; Chen, J.C.; Dwyer, A.; Dennis, J.; Ahnen, J.; Smith, R.A.; Zauber, A.G. The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline. Cancer 2018, 124, 2964–2973. [Google Scholar] [CrossRef]
- Meester, R.G.S.; Peterse, E.F.P.; Knudsen, A.B.; de Weerdt, A.C.; Chen, J.C.; Lietz, A.P.; Dwyer, A.; Ahnen, D.J.; Siegel, R.L.; Smith, R.A.; et al. Optimizing colorectal cancer screening by race and sex: Microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline. Cancer 2018, 124, 2974–2985. [Google Scholar] [CrossRef]
- Ladabaum, U.; Mannalithara, A.; Meester, R.G.S.; Gupta, S.; Schoen, R.E. Cost-effectiveness and national effects of initiating colorectal cancer screening for average-risk persons at age 45 years instead of 50 years. Gastroenterology 2019, 157, 137–148. [Google Scholar] [CrossRef]
- Telford, J.J.; Levy, A.R.; Sambrook, J.C.; Zou, D.; Enns, R.A. The cost-effectiveness of screening for colorectal cancer. CMAJ 2010, 182, 1307–1313. [Google Scholar] [CrossRef] [Green Version]
- Heitman, S.J.; Hilsden, R.J.; Au, F.; Dowden, S.; Manns, B.J. Colorectal cancer screening for average-risk north americans: An economic evaluation. PLoS Med. 2010, 7. [Google Scholar] [CrossRef] [Green Version]
- Coldman, A.J.; Phillips, N.; Brisson, J.; Flanagan, W.; Wolfson, M.; Nadeau, C.; Fitzgerald, N.; Miller, A.B. Using the cancer risk management model to evaluate colorectal cancer screening options for Canada. Curr. Oncol. 2015, 22, e41–e50. [Google Scholar] [CrossRef] [Green Version]
- Lofton-Day, C.; Model, F.; DeVos, T.; Tetzner, R.; Distler, J.; Schuster, M.; Song, X.; Lesche, R.; Liebenberg, V.; Ebert, M.; et al. DNA methylation biomarkers for blood-based colorectal cancer screening. Clin. Chem. 2008, 54, 414–423. [Google Scholar] [CrossRef]
- Vacante, M.; Ciuni, R.; Basile, F.; Biondi, A. The liquid biopsy in the management of colorectal cancer: An overview. Biomedicines 2020, 8, 308. [Google Scholar] [CrossRef]
- Ofman, J.J.; Hall, M.P.; Aravanis, A.M. GRAIL and the Quest for Earlier Multi-Cancer Detection. Available online: https://media-nature-com.ezproxy.library.ubc.ca/original/magazine-assets/d42473-020-00079-y/d42473-020-00079-y.pdf (accessed on 5 July 2020).
- Sheridan, C. Grail to pour $1 billion into blood test to detect early cancer. Nat. Biotechnol. 2017, 35, 101–102. [Google Scholar] [CrossRef] [PubMed]
- Farshidfar, F.; Weljie, A.M.; Kopciuk, K.A.; Hilsden, R.; Mcgregor, E.; Buie, D.; Maclean, A.; Vogel, H.J.; Bathe, O.F. A validated metabolomic signature for colorectal cancer: Exploration of the clinical value of metabolomics. Br. J. Cancer 2016, 115, 848–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Publishing Organization | Last Updated | Ages Targeted | Recommended Screening Test Options | Recommended Follow-Up for Positive Screen |
|---|---|---|---|---|
| Canadian Task Force on Preventive Health [9] | 2016 | 60–74 (strong recommendation; screening should be offered to all), 50–59 (weak recommendation; screening to be offered after discussing harms and benefits), no screening at 75+ | FIT or HS-gFOBT q2 yrs, FS q10 yrs | Colonoscopy |
| Canadian Association of Gastroenterology [18] | 2010 | 50–75, 76–85 case-by-case | FIT (preferred) or HS-gFOBT q1–2 yrs, FS q10 yrs | Colonoscopy |
| U.S. Preventive Services Task Force (draft posted October 2020) [15] | 2020 | 45–75, 76–85 case-by-case | FIT or HS-gFOBT q1 yr, DNA-FIT q1–3 yrs, FIT q1 yr, plus FS q10 yrs, FS q5 yrs, colonoscopy q10 yrs, CTC q5 yrs | Colonoscopy |
| American Cancer Society [8] | 2018 | 45–75 (qualified recommendation), 50–75 (strong recommendation), 76–85 case-by-case | FIT or HS-gFOBT q1 yr, DNA-FIT q3 yrs, FS q5 yrs colonoscopy q10 yrs, CTC q5 yrs, | Colonoscopy |
| U.S. Preventive Services Task Force [32] | 2016 | 50–75, 76–85 case-by-case | FIT or gFOBT q1 yr, FIT-DNA q1–3 yrs, FIT q1 yr plus FS q10 yrs, FS q5 yrs, colonoscopy q10 yrs, CTC q5 yrs | Colonoscopy |
| Province | Program Name [23,33] | Organization Responsible | Program Start | Ages Targeted | Screening Tests Offered | Enrolment in Program | Cut-off for Positive FIT (ng/mL) [23] |
|---|---|---|---|---|---|---|---|
| Alberta | Alberta Colorectal Cancer Screening Program | Alberta Health Services | 2009 | 50–74 | FIT q1 yr | Referral by clinician | 75 |
| British Columbia | Colon Screening Program | BC Cancer | 2013 | 50–74 | FIT q2 yrs | Referral by clinician, Northern Health Authority does not participate | 50 |
| Manitoba | ColonCheck | CancerCare Manitoba | 2007 | 50–74 | gFOBT q2 yrs (requires 3 different samples) | Referral by clinician or individual requests online/by phone | N/A |
| New Brunswick | New Brunswick Colon Cancer Screening Program | New Brunswick Cancer Network | 2014 | 50–74 | FIT q2 yrs | Invitations mailed q2 yrs once individual turns 50 | 100 |
| Newfoundland and Labrador | Newfoundland and Labrador Colon Cancer Screening Program | Eastern Health | 2012 | 50–74 | FIT q2 yrs | Referral by clinician or individual requests online/by phone | 100 |
| Northwest Territories | Organized screening program in planning stages | Northwest Territories Health and Social Services Authority | N/A | 50–74 | FIT q1–2 yrs | Referral by clinician | 75 |
| Nova Scotia | Colon Cancer Prevention Program | Nova Scotia Health Authority | 2009 | 50–74 | FIT q2 yrs | Kits mailed q2 yrs once individuals turn 50 | 100 |
| Ontario | ColonCancerCheck | Cancer Care Ontario | 2008 | 50–74 | FIT q2 yrs or FS q10 yrs (can be done by registered nurse) | Referral by clinician or individual requests by phone | Not reported |
| Prince Edward Island (PEI) | Colorectal Cancer Screening Program | Health PEI | 2011 | 50–74 | FIT q2 yrs (requires 2 different samples) | Individual requests online/by phone | 100 |
| Quebec | Colorectal Cancer Screening Program (still in pilot phase) | Ministère de la Santé et des Services Sociaux | Pilot started in 2011 | 50–74 | FIT q2 yrs | Referral by clinician | 175 |
| Saskatchewan | Screening Program for Colorectal Cancer | Saskatchewan Cancer Agency | 2009 | 50–74 | FIT q2 yrs | Kits mailed q2 yrs once individuals turn 50 | 100 |
| Yukon | ColonCheck Yukon | Government of Yukon Health and Social Services | 2017 | 50–74 | FIT q2 yrs | Referral by clinician or individual requests by phone | 100 |
| Nunavut | Organized program implementation is in-progress | Nunavut Department of Health | 2018 | 50–74 | FIT q2 yrs | Opportunistic screening available | Not reported |
| Country | Organization Responsible | Program Start/Updates | Ages Targeted | Screening Tests Offered | Follow-Up Test for Positive Screen | Participant Recruitment |
|---|---|---|---|---|---|---|
| United Kingdom [46,47,48] | National Health Service | Started in 2006, updated in 2018 | 60–74 in England, Wales and Northern Ireland, 50–74 in Scotland. A 2018 decision to start at 50 U.K.-wide has not yet been implemented. | FIT q2 yrs (gFOBT in Northern Ireland), Bowelscope program offers one-time FS at age 55 in England only | Colonoscopy | Kits mailed to eligible individuals |
| France [49,50] | French Ministry of Health and National Cancer Institute | 2008, switched to FIT in 2015 | 50–74 | FIT q2 yrs | Colonoscopy | Invitations mailed to eligible individuals; kits obtained from family doctor |
| Netherlands [51,52] | National Institute for Public Health and the Environment | 2014 | 55–75 | FIT q2 yrs | Colonoscopy | Kits mailed to eligible individuals |
| Country | Age Group | Incidence (ASIR per 100,000) [1,55] | Mortality (ASMR per 100,000) [1,55] |
|---|---|---|---|
| Canada | All ages | 31.5 | 10.1 |
| Over 50 | 135.6 | 47.0 | |
| Under 50 | 5.4 | 0.91 | |
| U.S. | All ages | 25.6 | 8.2 |
| Over 50 | 105.0 | 35.0 | |
| Under 50 | 5.7 | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kalyta, A.; De Vera, M.A.; Peacock, S.; Telford, J.J.; Brown, C.J.; Donnellan, F.; Gill, S.; Loree, J.M. Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns? Curr. Oncol. 2021, 28, 1558-1570. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030147
Kalyta A, De Vera MA, Peacock S, Telford JJ, Brown CJ, Donnellan F, Gill S, Loree JM. Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns? Current Oncology. 2021; 28(3):1558-1570. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030147
Chicago/Turabian StyleKalyta, Anastasia, Mary A. De Vera, Stuart Peacock, Jennifer J. Telford, Carl J. Brown, Fergal Donnellan, Sharlene Gill, and Jonathan M. Loree. 2021. "Canadian Colorectal Cancer Screening Guidelines: Do They Need an Update Given Changing Incidence and Global Practice Patterns?" Current Oncology 28, no. 3: 1558-1570. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030147