Cost-Effectiveness Analysis of Stereotactic Ablative Body Radiotherapy for the Treatment of Oligometastatic Tumors versus Standard of Care


Abstract
:1. Introduction
2. Methods
2.1. Patient Population
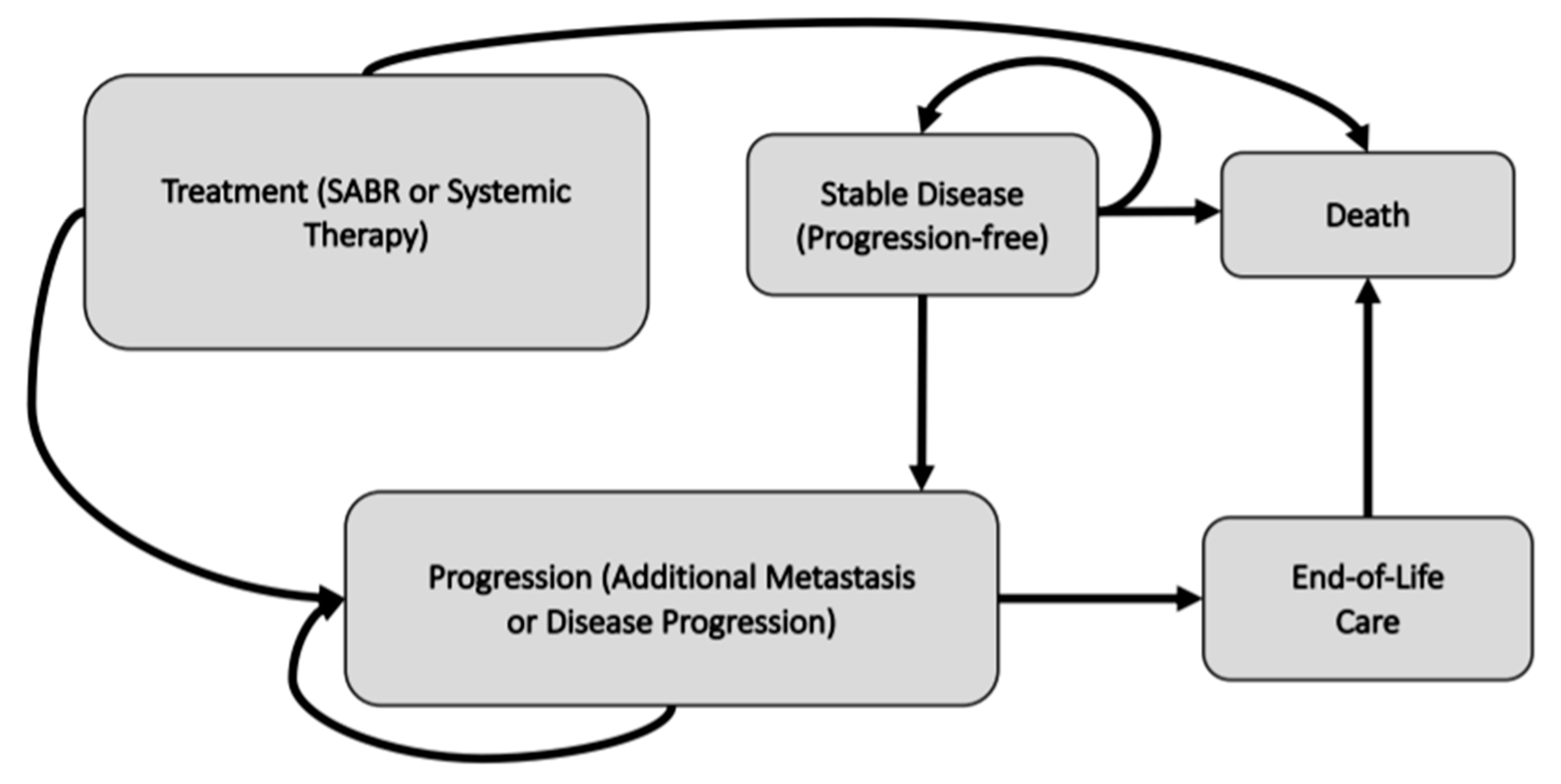
2.2. Modeling Approach
2.3. Model Data
2.4. Budget Impact Analysis
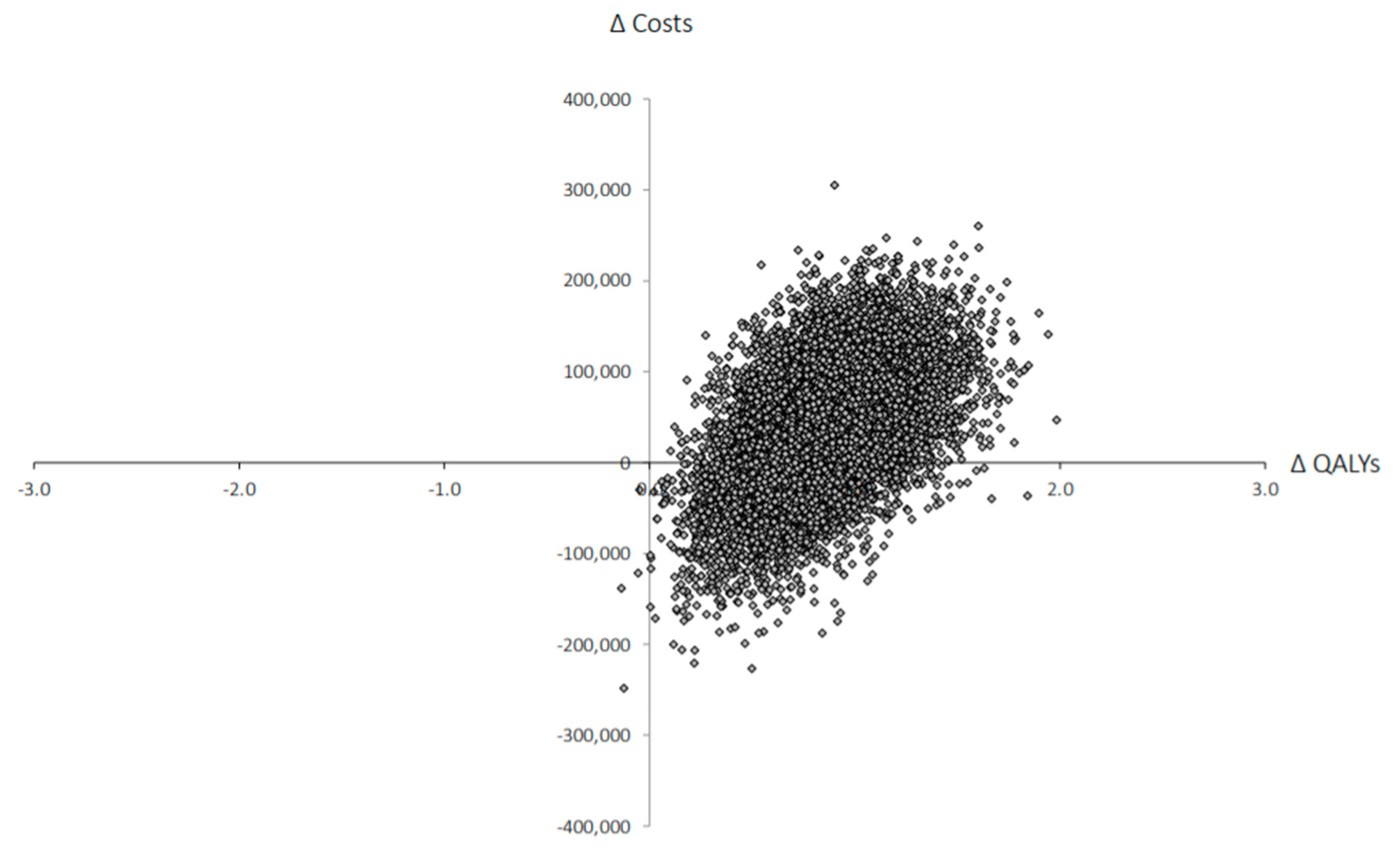
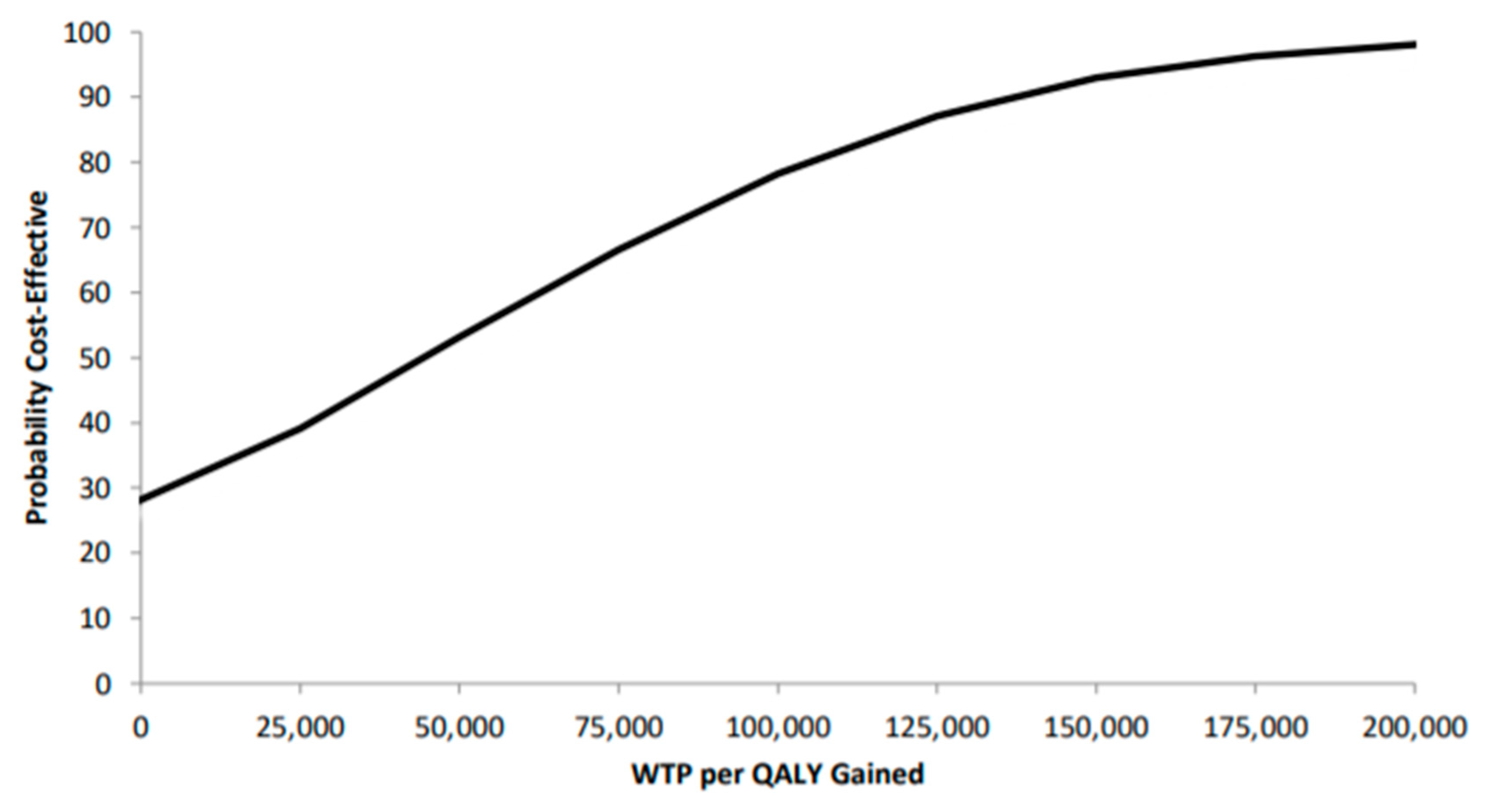
2.5. Probabilistic Analysis
2.6. Model Outcomes
3. Results
4. Discussion
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murray, P.; Franks, K.; Hanna, G.G. A systematic review of outcomes following stereotactic ablative radiotherapy in the treatment of early-stage primary lung cancer. Br. J. Radiol. 2017, 90, 20160732. [Google Scholar] [CrossRef] [Green Version]
- Simeonova, A.O.; Fleckenstein, K.; Wertz, H.; Frauenfeld, A.; Boda-Heggemann, J.; Lohr, F.; Wenz, F. Are three doses of stereotactic ablative radiotherapy (SABR) more effective than 30 doses of conventional radiotherapy? Transl. Lung Cancer Res. 2012, 1, 45–53. [Google Scholar] [PubMed]
- Potters, L.; Kavanagh, B.; Galvin, J.M.; Hevezi, J.M.; Janjan, N.A.; Larson, D.A.; Mehta, M.P.; Ryu, S.; Steinberg, M.; Timmerman, R.; et al. American society for therapeutic radiology and oncology (ASTRO) and American college of radiology (ACR) practice guideline for the performance of stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Choy, H. SABR as First Line Treatment Option. J. Thorac. Oncol. 2017, 12, S1661. [Google Scholar] [CrossRef]
- Olson, R.; Liu, M.; Bergman, A.; Lam, S.; Hsu, F.; Mou, B.; Berrang, T.; Mestrovic, A.; Chng, N.; Hyde, D.; et al. Population-based phase II trial of stereotactic ablative radiotherapy (SABR) for up to 5 oligometastases: SABR-5. BMC Cancer 2018, 18, 954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xhaferllari, I.; El-Sherif, O.; Gaede, S. Comprehensive dosimetric planning comparison for early-stage, non-small cell lung cancer with SABR: Fixed-beam IMRT versus VMAT versus TomoTherapy. J. Appl. Clin. Med. Phys. 2016, 17, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Senan, S.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.; Yaremko, B.; et al. Stereotactic ablative radiotherapy for oligometastatic cancers: Efficacy and toxicity results from the randomized SABR-COMET Trial. Ann. Oncol. 2018, 29, ix170. [Google Scholar] [CrossRef]
- Canadian Agency for Drugs and Technologies in Health. Guidelines for the Economic Evaluation of Health Technologies in Canada; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2017. [Google Scholar]
- Bank of Canada Bank of Canada Inflation Calculator. Available online: https://www.bankofcanada.ca/rates/related/inflation-calculator/ (accessed on 12 August 2020).
- USD Historical Exchange Rates (US Dollar)—X-Rates. Available online: https://www.x-rates.com/historical/?from=USD&amount=1&date=2014-07-29 (accessed on 12 August 2020).
- Newcombe, P.J.; Raza Ali, H.; Blows, F.M.; Provenzano, E.; Pharoah, P.D.; Caldas, C.; Richardson, S. Weibull regression with Bayesian variable selection to identify prognostic tumour markers of breast cancer survival. Stat. Methods Med. Res. 2017, 26, 414–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, C. Flexsurv: A platform for parametric survival modeling in R. J. Stat. Softw. 2016, 70, i08. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendenhall, W.; Sincich, T. A Second Course in Statistics: Regression Analysis, 7th ed.; Prentice Hall: Boston, MA, USA, 2012; ISBN 978-0-321-69169-9. [Google Scholar]
- Guest, J.F.; Ruiz, F.J.; Greener, M.J.; Trotman, I.F. Palliative care treatment patterns and associated costs of healthcare resource use for specific advanced cancer patients in the UK. Eur. J. Cancer Care 2006, 15, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Hahn, S.M.; Stetson, R.L.; Friedberg, J.S.; Pechet, T.T.V.; Sher, D.J. Cost-effectiveness of stereotactic body radiation therapy versus surgical resection for stage I non-small cell lung cancer. Cancer 2013, 119, 3123–3132. [Google Scholar] [CrossRef]
- Minion, L.E.; Bai, J.; Monk, B.J.; Robin Keller, L.; Ramez, E.N.; Forde, G.K.; Chan, J.K.; Tewari, K.S. A Markov model to evaluate cost-effectiveness of antiangiogenesis therapy using bevacizumab in advanced cervical cancer. Gynecol. Oncol. 2015, 137, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Fox, K.M.; Brooks, J.M.; Kim, J. Metastatic non–small cell lung cancer: Costs associated with disease progression. Am. J. Manag. Care 2008, 14, 7. [Google Scholar]
- Louie, A.V.; Rodrigues, G.B.; Palma, D.A.; Senan, S. Measuring the population impact of introducing stereotactic ablative radiotherapy for stage i non-small cell lung cancer in canada. Oncologist 2014, 19, 880–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemplényi, A.T.; Kaló, Z.; Kovács, G.; Farkas, R.; Beöthe, T.; Bányai, D.; Sebestyén, Z.; Endrei, D.; Boncz, I.; Mangel, L. Cost-effectiveness analysis of intensity-modulated radiation therapy with normal and hypofractionated schemes for the treatment of localised prostate cancer. Eur. J. Cancer Care 2018, 27, e12430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, S.T.; Lenert, L.; Bhatnagar, V.; Kaplan, R.M. Utilities for prostate cancer health states in men aged 60 and older. Med. Care 2005, 43, 347–355. [Google Scholar] [CrossRef]
- Grutters, J.P.C.; Pijls-Johannesma, M.; Ruysscher, D.D.; Peeters, A.; Reimoser, S.; Severens, J.L.; Lambin, P.; Joore, M.A. The cost-effectiveness of particle therapy in non-small cell lung cancer: Exploring decision uncertainty and areas for future research. Cancer Treat. Rev. 2010, 36, 468–476. [Google Scholar] [CrossRef] [PubMed]
- Wen, F.; Yao, K.; Du, Z.-D.; He, X.-F.; Zhang, P.-F.; Tang, R.-L.; Li, Q. Cost-effectiveness analysis of colon cancer treatments from MOSIAC and No. 16968 trials. World J. Gastroenterol. WJG 2014, 20, 17976–17984. [Google Scholar] [CrossRef]
- Lester-Coll, N.H.; Rutter, C.E.; Bledsoe, T.J.; Goldberg, S.B.; Decker, R.H.; Yu, J.B. Cost-effectiveness of surgery, stereotactic body radiation therapy, and systemic therapy for pulmonary oligometastases. Int. J. Radiat. Oncol. 2016, 95, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Doyle, S.; Lloyd, A.; Walker, M. Health state utility scores in advanced non-small cell lung cancer. Lung Cancer Amst. Neth. 2008, 62, 374–380. [Google Scholar] [CrossRef] [PubMed]
- de Kok, I.M.C.M.; van Ballegooijen, M.; Habbema, J.D.F. Cost-effectiveness analysis of human papillomavirus vaccination in the netherlands. JNCI J. Natl. Cancer Inst. 2009, 101, 1083–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, R.; Mathews, L.; Liu, M.; Schellenberg, D.; Mou, B.; Berrang, T.; Harrow, S.; Correa, R.J.M.; Bhat, V.; Pai, H.; et al. Stereotactic ablative radiotherapy for the comprehensive treatment of 1–3 Oligometastatic tumors (SABR-COMET-3): Study protocol for a randomized phase III trial. BMC Cancer 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tarricone, R.; Torbica, A.; Drummond, M. Challenges in the assessment of medical devices: The medtecHTA project. Health Econ. 2017, 26, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, B.D.; Jiang, J.; Chang, J.Y.; Welsh, J.; Likhacheva, A.; Buchholz, T.A.; Swisher, S.G.; Shirvani, S.M. Cost-effectiveness of stereotactic radiation, sublobar resection, and lobectomy for early non-small cell lung cancers in older adults. J. Geriatr. Oncol. 2015, 6, 324–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, M.X.; Chen, Y.; Zaric, G.; Senan, S.; Olson, R.A.; Harrow, S.; John-Baptiste, A.; Gaede, S.; Mulroy, L.; Schellenberg, D.; et al. Is SABR cost-effective in oligometastatic cancer? An economic analysis of SABR-comet. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, S100–S101. [Google Scholar] [CrossRef]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: Long-term results of the SABR-COMET phase II randomized trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Health States | Value | Distribution | Source |
|---|---|---|---|
| Costs | |||
| SABR Time-Zero Costs | $89,696.22 | Gamma | BC Cancer internal estimate |
| SABR No Toxicity | $3563.38 | Gamma | BC Cancer internal estimate |
| SABR Minor Toxicity | $3646.89 | Gamma | Shah et al. (2013) [16] |
| SABR Major Toxicity | $4800.10 | Gamma | Minion et al. (2015) [17] |
| Stable Disease No Toxicity | $12,737.47 | Gamma | Fox et al. (2008) [18] |
| Stable Disease Minor Toxicity | $12,820.98 | Gamma | Fox et al. (2008) [18] |
| Stable Disease Major Toxicity | $14,063.44 | Gamma | Shah et al. (2013) [16] |
| Progression | $43,397.98 | Gamma | Calculated |
| Systemic Therapy | $43,397.98 | Gamma | Calculated |
| Stable Disease | $12,820.97 | Gamma | Fox et al. (2008) [18] |
| Supportive Care | $3959.91 | Gamma | Louie et al. (2014) [19] |
| Utilities | |||
| SABR No Toxicity | 0.73 | Beta | Zemplenyi et al. (2019) [20]; Stewart et al. (2005) [21] |
| SABR Minor Toxicity | 0.60 | Beta | Zemplenyi et al. (2019) [20]; Stewart et al. (2005) [21] |
| SABR Major Toxicity | 0.46 | Beta | Grutters et al. (2019) [22] |
| Stable Disease No Toxicity | 0.78 | Beta | Zemplenyi et al. (2019) [20] ; Stewart et al. (2005) [21] |
| Stable Disease Minor Toxicity | 0.73 | Beta | Wen et al. (2014) [23] |
| Stable Disease Major Toxicity | 0.59 | Beta | Wen et al. (2014) [23] |
| Progression | 0.62 | Beta | Lester-Coll et al. (2016) [24] |
| Stable Disease | 0.78 | Beta | Zemplenyi et al. (2019) [20] |
| Systemic Therapy | 0.62 | Beta | Lester-Coll et al. (2016) [24] ; Doyle et al. (2008) [25] |
| Supportive Care | 0.29 | Beta | de Kok et al. (2009) [26] |
| Costs | QALYs | Incremental Costs | Incremental QALYs | ICER | |
|---|---|---|---|---|---|
| SABR | $495,853 (410,330–577,745) | 1.88 (1.44–2.35) | 38,488 | 0.85 | $45,279 |
| SoC | $457,365 (385,331–536,483) | 1.03 (0.88–1.21) |
| Costs | QALYs | Incremental Costs | Incremental QALYs | ICER | |
|---|---|---|---|---|---|
| SABR | $756,622 (507,713–1,069,635) | 2.26 (1.94–2.65) | $291,544 | 1.21 | $240,945 |
| SoC | $465,078 (389,160–559,224) | 1.05 (0.88–1.21) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raymakers, A.J.N.; Cameron, D.; Tyldesley, S.; Regier, D.A. Cost-Effectiveness Analysis of Stereotactic Ablative Body Radiotherapy for the Treatment of Oligometastatic Tumors versus Standard of Care. Curr. Oncol. 2021, 28, 1857-1866. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030172
Raymakers AJN, Cameron D, Tyldesley S, Regier DA. Cost-Effectiveness Analysis of Stereotactic Ablative Body Radiotherapy for the Treatment of Oligometastatic Tumors versus Standard of Care. Current Oncology. 2021; 28(3):1857-1866. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030172
Chicago/Turabian StyleRaymakers, Adam J. N., David Cameron, Scott Tyldesley, and Dean A. Regier. 2021. "Cost-Effectiveness Analysis of Stereotactic Ablative Body Radiotherapy for the Treatment of Oligometastatic Tumors versus Standard of Care" Current Oncology 28, no. 3: 1857-1866. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28030172