Efficacy and Accuracy of Using Magnetic Seed for Preoperative Non-Palpable Breast Lesions Localization: Our Experience with Magseed

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
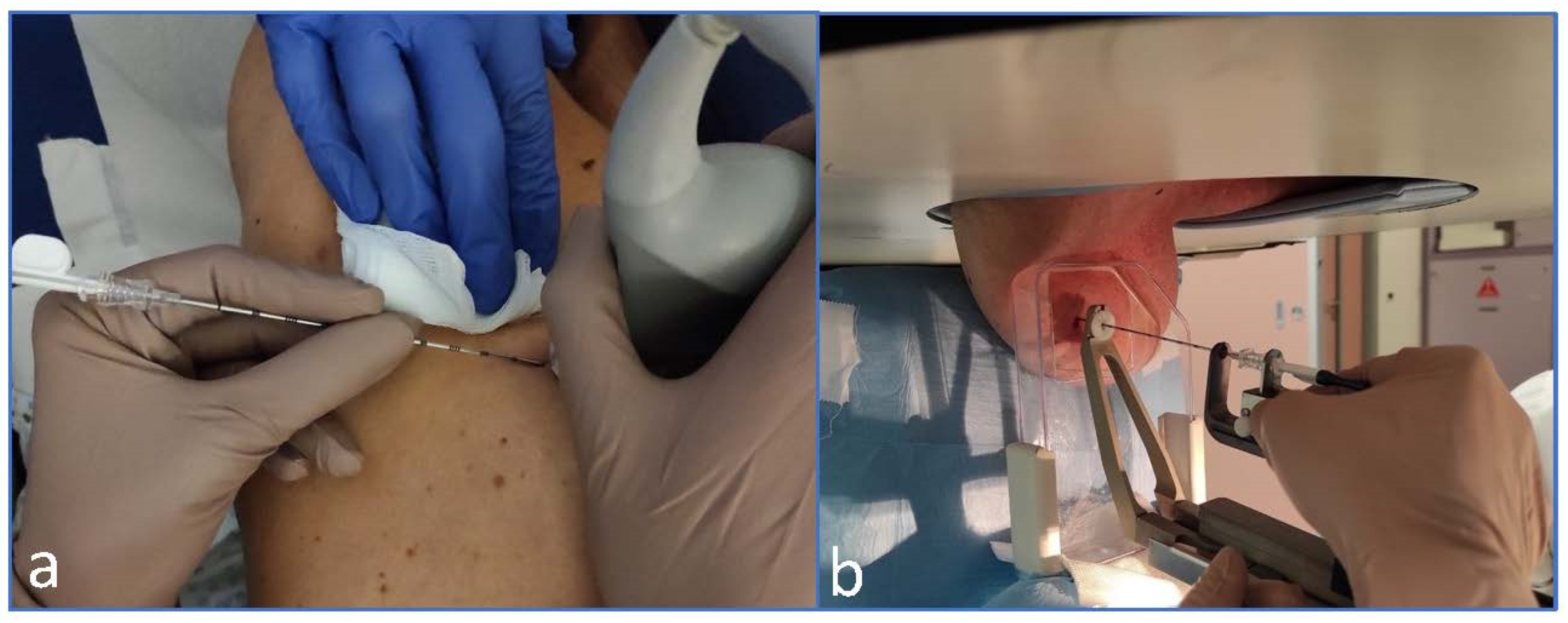
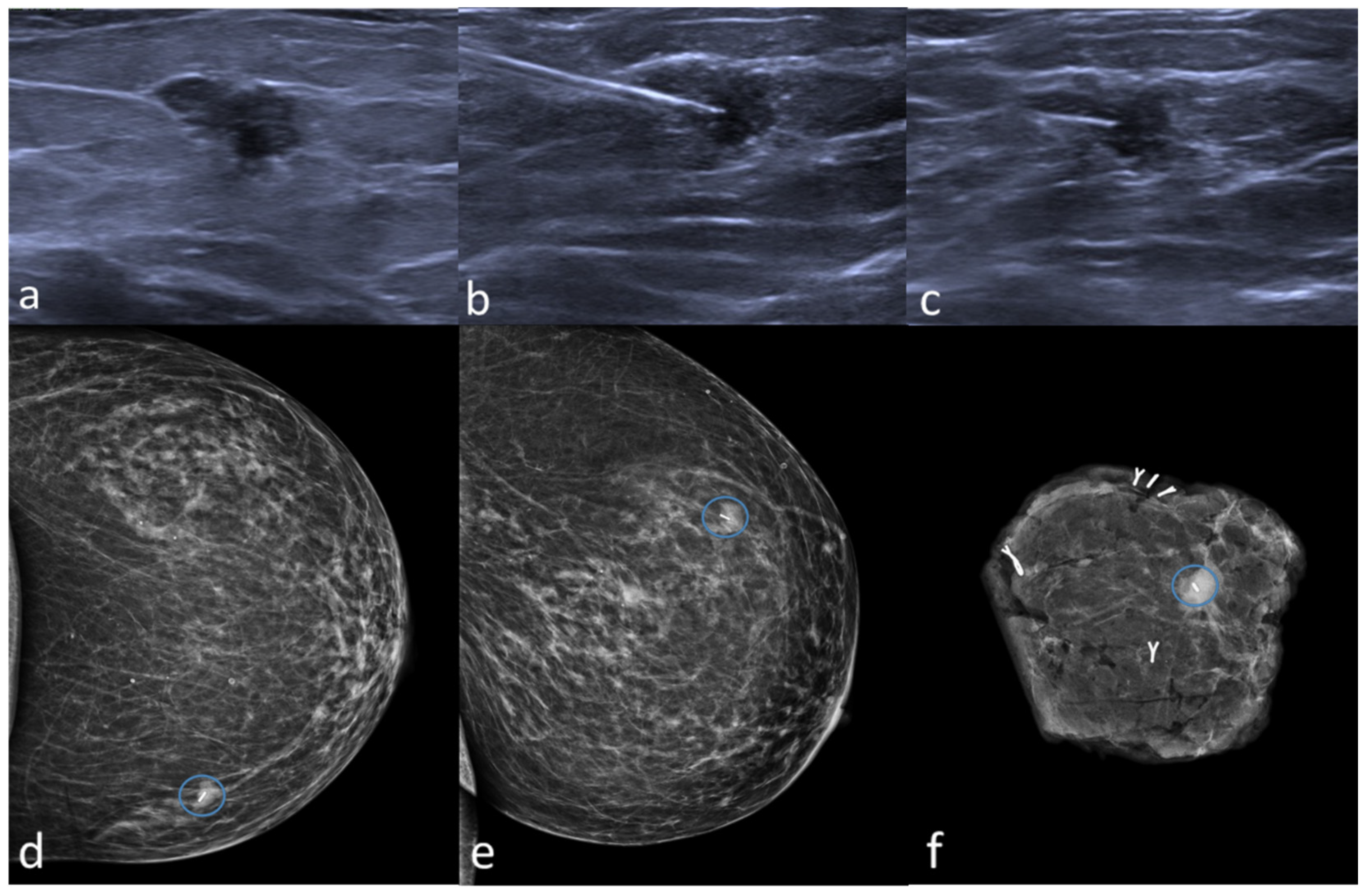
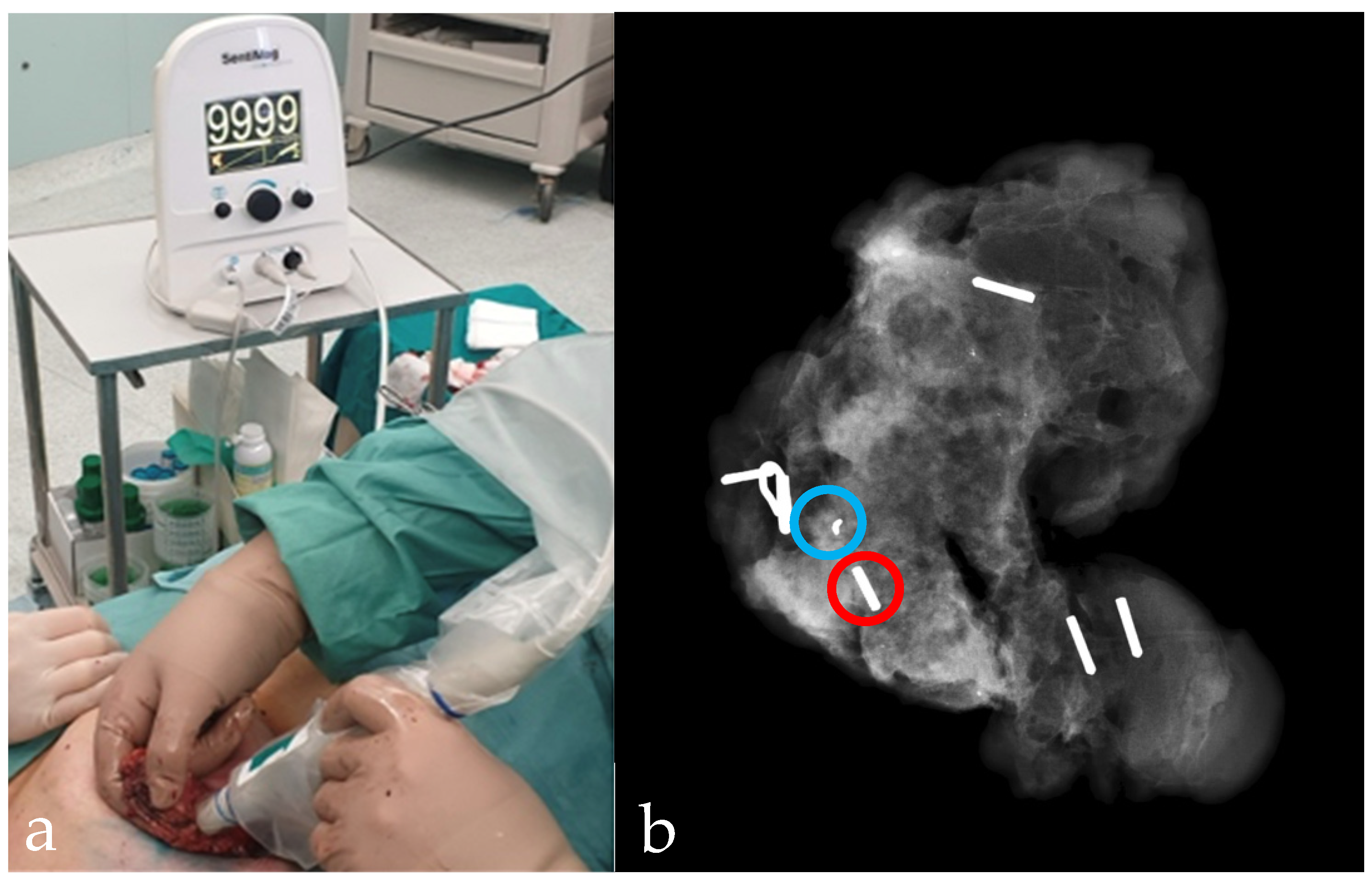
2.2. Procedure
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Benson, J.R.; Jatoi, I.; Keisch, M.; Esteva, F.J.; Makris, A.; Jordan, V.C. Early Breast Cancer. Lancet 2009, 373, 1463–1479. [Google Scholar] [CrossRef]
- Paganelli, G.; Luini, A.; Veronesi, U. Radioguided occult lesion localization (ROLL) in breast cancer: Maximizing efficacy, minimizing mutilation. Ann. Oncol. 2002, 13, 1839–1840. [Google Scholar] [CrossRef]
- Wazir, U.; Tayeh, S.; Perry, N.; Michell, M.; Malhotra, A.; Mokbel, K. Wireless Breast Localization Using Radio-frequency Identification Tags: The First Reported European Experience in Breast Cancer. In Vivo 2020, 34, 233–238. [Google Scholar] [CrossRef]
- Wazir, U.; Kasem, I.; Michell, M.J.; Suaris, T.; Evans, D.; Malhotra, A.; Mokbel, K. Reflector-Guided Localisation of Non-Palpable Breast Lesions: A Prospective Evaluation of the SAVI SCOUT® System. Cancers 2021, 13, 2409. [Google Scholar] [CrossRef] [PubMed]
- Kurita, T.; Taruno, K.; Nakamura, S.; Takei, H.; Enokido, K.; Kuwayama, T.; Kanada, Y.; Akashi-Tanaka, S.; Matsuyanagi, M.; Hankyo, M.; et al. Magnetically Guided Localization Using a Guiding-Marker System® and a Handheld Magnetic Probe for Nonpalpable Breast Lesions: A Multicenter Feasibility Study in Japan. Cancers 2021, 13, 2923. [Google Scholar] [CrossRef] [PubMed]
- Žatecký, J.; Kubala, O.; Jelínek, P.; Lerch, M.; Ihnát, P.; Peteja, M.; Brát, R. Magnetic marker localisation in breast cancer surgery. Arch. Med. Sci. 2020, 16, 383–388. [Google Scholar] [CrossRef]
- Gray, R.J.; Salud, C.; Nguyen, K.; Dauway, E.; Friedland, J.; Berman, C.; Peltz, E.; Whitehead, G.; Cox, C.E. Randomized Prospective Evaluation of a Novel Technique for Biopsy or Lumpectomy of Nonpalpable Breast Lesions: Radioactive Seed Versus Wire Localization. Ann. Surg. Oncol. 2001, 8, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Gera, R.; Tayeh, S.; Al-Reefy, S.; Mokbel, K. Evolving Role of Magseed in Wireless Localization of Breast Lesions: Systematic Review and Pooled Analysis of 1,559 Procedures. Anticancer Res. 2020, 40, 1809–1815. [Google Scholar] [CrossRef] [PubMed]
- Fleming, F.; Hill, A.; Mc Dermott, E.; O’Doherty, A.; O’Higgins, N.; Quinn, C. Intraoperative margin assessment and re-excision rate in breast conserving surgery. Eur. J. Surg. Oncol. 2004, 30, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.A.; Feneis, J.; LaLonde, C.; Ojeda-Fournier, H. A Pictorial Review of Changes in the BI-RADS Fifth Edition. RadioGraphics 2016, 36, 623–639. [Google Scholar] [CrossRef] [PubMed]
- Žatecký, J.; Kubala, O.; Coufal, O.; Kepičová, M.; Faridová, A.; Rauš, K.; Lerch, M.; Peteja, M.; Brát, R. Magnetic Seed (Magseed) Localisation in Breast Cancer Surgery: A Multicentre Clinical Trial. Breast Care 2020, 16, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Harvey, J.R.; Lim, Y.; Murphy, J.; Howe, M.; Morris, J.; Goyal, A.; Maxwell, A.J. Safety and feasibility of breast lesion localization using magnetic seeds (Magseed): A multi-centre, open-label cohort study. Breast Cancer Res. Treat. 2018, 169, 531–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hersi, A.-F.; Eriksson, S.; Ramos, J.; Abdsaleh, S.; Wärnberg, F.; Karakatsanis, A. A combined, totally magnetic technique with a magnetic marker for non-palpable tumour localization and superparamagnetic iron oxide nanoparticles for sentinel lymph node detection in breast cancer surgery. Eur. J. Surg. Oncol. 2019, 45, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Price, E.R.; Khoury, A.L.; Esserman, L.J.; Joe, B.N.; Alvarado, M.D. Initial Clinical Experience With an Inducible Magnetic Seed System for Preoperative Breast Lesion Localization. Am. J Roentgenol. 2018, 210, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Tayeh, S.; Gera, R.; Perry, N.; Michell, M.; Malhotra, A.; Mokbel, K. The Use of Magnetic Seeds and Radiofrequency Identifier Tags in Breast Surgery for Non-palpable Lesions. Anticancer Res. 2020, 40, 315–321. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients Age (Years) | 57.58 (range 31–80) |
| Breast lesions dimension (mm) | 8.8 (range 3–18) |
| Type of surgery: | |
| Lumpectomy | 3 |
| Quadrantectomy | 43 |
| Re-excision rate | 0% |
| Intraoperative widening | 0% |
| Post-operative histology: | |
| DCIS | 4 (8.8%) |
| IDC | 35 (77.8%) |
| B3 | 6 (13.4%) |
| Total Magseed Placed | 45 |
|---|---|
| Localization modality: | |
| Ultrasound localization | 40 (88.9%) |
| Stereotactic localization | 5 (11.1 %) |
| Seed migration/malpositioning | 1 (2.2%) |
| Successful detection and retrieval | 45 (100%) |
| Time between Magseed placement and surgery (d) | 3.46 |
| Time for Magseed placement (min) | 5.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Angelo, A.; Trombadori, C.M.L.; Caprini, F.; Lo Cicero, S.; Longo, V.; Ferrara, F.; Palma, S.; Conti, M.; Franco, A.; Scardina, L.; et al. Efficacy and Accuracy of Using Magnetic Seed for Preoperative Non-Palpable Breast Lesions Localization: Our Experience with Magseed. Curr. Oncol. 2022, 29, 8468-8474. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29110667
D’Angelo A, Trombadori CML, Caprini F, Lo Cicero S, Longo V, Ferrara F, Palma S, Conti M, Franco A, Scardina L, et al. Efficacy and Accuracy of Using Magnetic Seed for Preoperative Non-Palpable Breast Lesions Localization: Our Experience with Magseed. Current Oncology. 2022; 29(11):8468-8474. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29110667
Chicago/Turabian StyleD’Angelo, Anna, Charlotte Marguerite Lucille Trombadori, Flavia Caprini, Stefano Lo Cicero, Valentina Longo, Francesca Ferrara, Simone Palma, Marco Conti, Antonio Franco, Lorenzo Scardina, and et al. 2022. "Efficacy and Accuracy of Using Magnetic Seed for Preoperative Non-Palpable Breast Lesions Localization: Our Experience with Magseed" Current Oncology 29, no. 11: 8468-8474. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol29110667