Pilomatrix Carcinoma: Report of Two Cases of the Head and Review of the Literature

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
3. Results
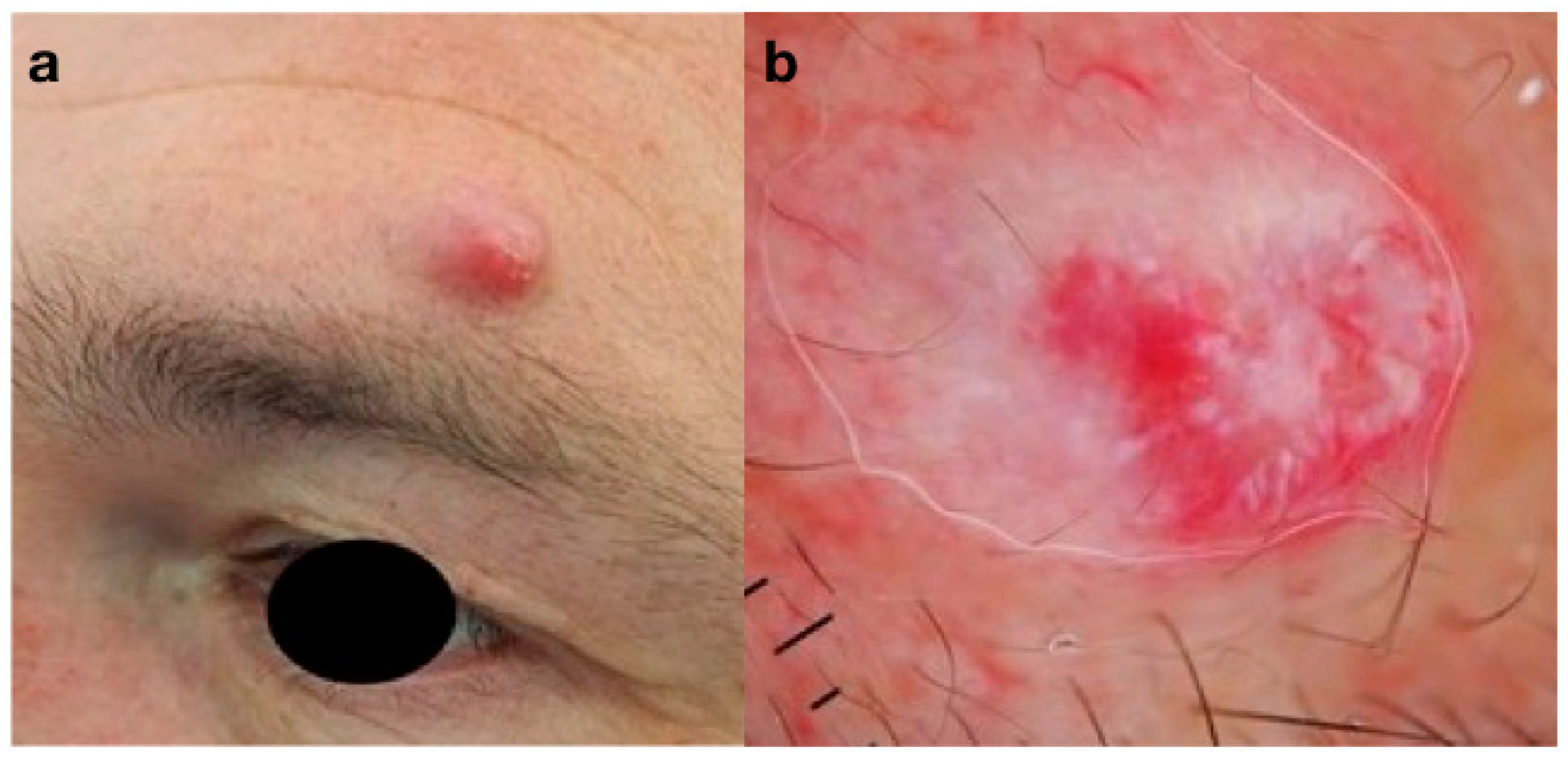
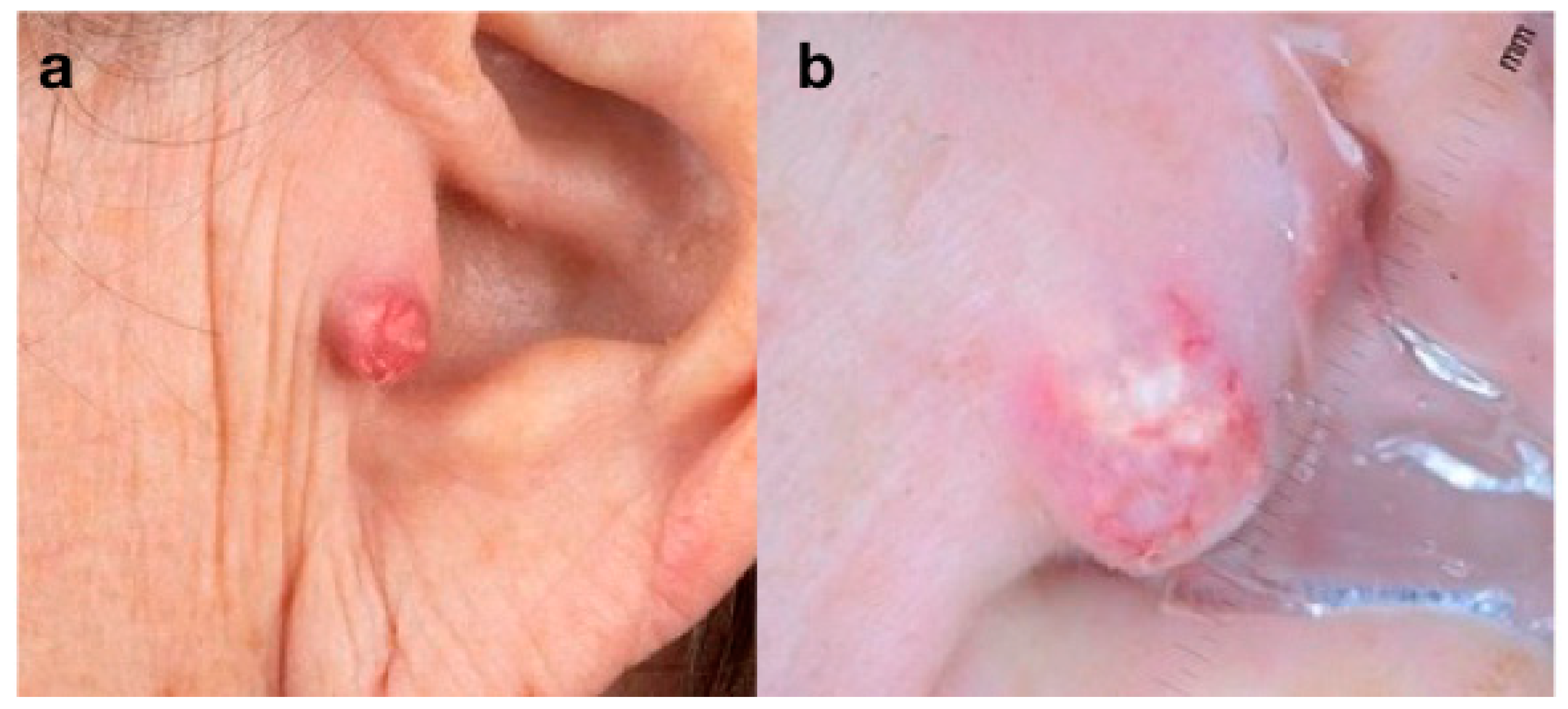
3.1. Case Reports
3.2. Review
3.2.1. Age and Sex
3.2.2. Distribution
3.2.3. Clinical Presentation and Lesion Size
3.2.4. Metastases
3.2.5. Dermoscopy
3.2.6. Method of Treatment and Recurrence
3.2.7. Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jones, C.; Twoon, M.; Ho, W.; Portelli, M.; Robertson, B.F.; Anderson, W. Pilomatrix carcinoma: 12-year experience and review of the literature. J. Cutan. Pathol. 2018, 45, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.F.; Li, B.; Fan, Z.X.; Jiao, T.; Li, C.; Qin, S.; Lang, J.Y.; Chen, J.X. Pilomatrix carcinoma on the left side of the parotid region: A case report and review of the literature. Oncol. Lett. 2015, 10, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.; DeJesus, J.; Jacob, A.; Qvavadze, T.; Guerrieri, C.; Hudacko, R.; Boucree, T. Pilomatrix carcinoma of the right postauricular region: A case report and literature review. Int. J. Surg. Case Rep. 2019, 65, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Vadrucci, M.; Gilardi, L.; Crivelli, F.; Baroli, A.; Lomuscio, G. 18F-FDG PET/CT in Metastatic Pilomatrix Carcinoma. Clin. Nucl. Med. 2016, 41, e525–e526. [Google Scholar] [CrossRef]
- Flynn, A.; Agastyaraju, A.D.; Sunitha, N.; Harrison, A. Malignant Pilomatricoma: A Report of Two Cases and Review of Literature. J. Clin. Diagn. Res. 2017, 11, ED27–ED28. [Google Scholar] [CrossRef]
- Walker, D.M.; Dowthwaite, S.; Cronin, D.; Molden-Hauer, T.; McMonagle, B. Metastatic pilomatrix carcinoma: Not so rare after all? A case report and review of the literature. Ear Nose Throat J. 2016, 95, 117–120. [Google Scholar]
- Herrmann, J.L.; Allan, A.; Trapp, K.M.; Morgan, M.B. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J. Am. Acad. Dermatol. 2014, 71, 38–43. [Google Scholar] [CrossRef]
- Pauly, M.; Subramanian, K.; Anantharaman, G.; Anthony, E. Pilomatrix carcinoma of the eyebrow. Ophthalmic Plast. Reconstr. Surg. 2015, 31, e9–e10. [Google Scholar] [CrossRef]
- Song, M.; Chekmareva, M.; Bachmann, G.; Gibbon, D. Pilomatrix carcinoma of the vulva. Gynecol. Oncol. Rep. 2015, 15, 9–11. [Google Scholar] [CrossRef] [Green Version]
- Parra, L.; Martin, M.; Garrido, M.; Pedraza, J.M.; Palazon, J.; Robustillo, M.; Grandes, D.; Lagaron, E. Concurrent Pilomatrix Carcinoma and Diffuse Large B-Cell Lymphoma. Oncol. Ther. 2016, 4, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Villada, G.; Romagosa, R.; Miteva, M.; Romanelli, P. Matrical Carcinoma With Melanocytic Proliferation and Prominent Squamoid Whorls. Am. J. Dermatopathol. 2016, 38, e11–e14. [Google Scholar] [CrossRef] [PubMed]
- Bailey, E.E.; Rushovich, A.M.; Kim, J. A growing nodule on the forearm of an 84-year-old man. J. Cutan. Pathol. 2017, 44, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lohiya, S.; Rawal, Y.B.; Dillon, J.K. Giant Pilomatrix Carcinoma of the Face. J. Oral Maxillofac Surg. 2018, 76, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Cornejo, K.M.; Deng, A. Pilomatrix carcinoma: A case report and review of the literature. Am. J. Dermatopathol. 2013, 35, 389–394. [Google Scholar] [CrossRef]
- Gupta, M.; Bansal, R.; Tiwari, G.; Sharma, S. Aggressive pilomatrixoma: A diagnostic dilemma on fine-needle aspiration cytology with review of literature. Diagn. Cytopathol. 2014, 42, 906–911. [Google Scholar] [CrossRef]
- Sorin, T.; Eluecque, H.; Gauchotte, G.; De Runz, A.; Chassagne, J.F.; Mansuy, L.; Gisquet, H.; Simon, E. Pilomatrix Carcinoma of the scalp. A case report and review of the literature. Ann. Chir. Plast. Esthet. 2015, 60, 242–246. [Google Scholar] [CrossRef] [PubMed]
- Allaoui, M.; Hubert, E.; Michels, J.J. Malignant pilomatricoma: Two new observations and review of the relevant literature. Turk Patoloji Derg. 2014, 30, 66–68. [Google Scholar] [CrossRef]
- Otero, M.N.; Trujillo, C.P.; Parra-Medina, R.; Morales, S.D. Metastatic Malignant Pilomatrixoma in an 8-Year-Old Girl Misdiagnosed as a Recurrent Pilomatrixoma. Am. J. Dermatopathol. 2017, 39, e41–e43. [Google Scholar] [CrossRef]
- Xing, L.; Marzolf, S.A.; Vandergriff, T.; Nijhawan, R.I. Facial pilomatrix carcinomas treated with Mohs micrographic surgery. JAAD Case Rep. 2018, 4, 253–255. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.S.; Na, Y.C.; Huh, W.H.; Kim, J.M. Malignant pilomatricoma of the cheek in an infant. Arch. Craniofac. Surg. 2018, 19, 283–286. [Google Scholar] [CrossRef]
- Fernandez-Flores, A.; Cassarino, D.S. Sarcomatoid pilomatrix carcinoma. J. Cutan. Pathol. 2018, 45, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Sengoz, T.; Avci, N. 18F-FDG PET/CT Findings in Metastatic Pilomatrix Carcinoma. Clin. Nucl. Med. 2020, 45, 146–147. [Google Scholar] [CrossRef]
- White, C.; Farsi, M.; Esguerra, D.; Miller, R. Not Your Average Skin Cancer: A Rare Case of Pilomatrix Carcinoma. J. Clin. Aesthet. Dermatol. 2020, 13, 40–42. [Google Scholar] [PubMed]
- Eckhoff, M.D.; Tadlock, J.; Kafchinski, L.A. Pilomatrix Carcinoma of the Antecubitum. Cureus 2020, 12, e6821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeo, M.K.; Bae, G.E. Comparison of Benign and Malignant Pilomatricomas Using Whole-exome Sequencing. Cancer Genom. Proteom. 2020, 17, 795–802. [Google Scholar] [CrossRef]
- Harbiyeli, I.I.; Ozcan, A.A.; Acıkalin, A.; Ciloglu, E.; Shields, C.L. Pilomatrix carcinoma of the lacrimal caruncle: A case report. Arq. Bras. Oftalmol. 2020, 83, 153–156. [Google Scholar] [CrossRef]
- Dell’Antonia, M.; Ferreli, C.; Pilloni, L.; Atzori, L. Pilomatrix carcinoma: A rare cutaneous adnexal tumor. Dermatol. Online J. 2021, 27. [Google Scholar] [CrossRef]
- Subramanyam, C.; Dyrek, P.; Yao, X.; Kay, M.H. Malignant Pilomatricoma of the Lower Extremity: A Difficult and Rare Diagnosis. Cureus 2022, 14, e21957. [Google Scholar] [CrossRef]
- Papadakis, M.; de Bree, E.; Floros, N.; Giannikaki, E.; Xekalou, A.; Manios, A. Pilomatrix carcinoma: More malignant biological behavior than was considered in the past. Mol. Clin. Oncol. 2017, 6, 415–418. [Google Scholar] [CrossRef] [Green Version]
- Briley, T.; Sobiesk, J.L.; Chu, Q. Pilomatrix carcinoma: A rare hair cell tumor. Am. Surg. 2020, 86, E38–E39. [Google Scholar] [CrossRef]
- Weng, G.; Li, F.; Xu, M. Pilomatrix carcinoma of the male breast: A case report. Int. J. Clin. Exp. Pathol. 2020, 13, 2153. [Google Scholar] [PubMed]
- Ravaioli, G.M.; Lambertini, M.; Pazzaglia, M.; Corti, B.; Fanti, P.A.; Dika, E. Pilomatrix carcinoma of the nose: Clinical and dermoscopic presentation. JAAD Case Rep. 2018, 4, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, O.; Melih Can, M.; Ozlem Karatas Silistreli, A.; Kaan Bedir, Y.; Caliskan, G. Malignant pilomatrixoma arising on the previously irradiated face: Case report and literature review. J. Cutan. Med. Surg. 2012, 16, 341–343. [Google Scholar] [CrossRef]
- Arslan, D.; Gündüz, S.; Avci, F.; Merdin, A.; Tatli, A.M.; Uysal, M.; Tural, D.; Başsorgun, C.I.; Savaş, B. Pilomatrix carcinoma of the scalp with pulmonary metastasis: A case report of a complete response to oral endoxan and etoposide. Oncol. Lett. 2014, 7, 1959–1961. [Google Scholar] [CrossRef] [PubMed]
- Tvrdi, A.B.; Elabjer, K.; Elabjer, B.K.; Miletić, D.; Bušić, M.; Bosnar, D.; Petrović, Z. Periocular pilomatrixoma: Case report. Acta Clin. Croat 2014, 53, 362–364. [Google Scholar]
- Mukherjee, B.; Roy, P.; Adulkar, N.; Krishnakumar, S.; Biswas, J. Pilomatrix carcinoma of the eyelid. Indian J. Cancer 2014, 51, 569–570. [Google Scholar] [CrossRef]
- Alcántara-González, J.; Sánchez-Largo, M.E.; Caminoa, A.; Erana, I.; Calzado-Villarreal, L. Pilomatrix carcinoma: A rare cause of facial tumor. Dermatol. Online J. 2014, 20. [Google Scholar] [CrossRef]
- Sato, S.; Nakamura, Y.; Shimizu, M.; Yamada, K.; Teramoto, Y.; Yamazaki, N.; Yamamoto, A. Giant pedunculated pilomatrix carcinoma on the upper limb: A rare clinical appearance. Eur. J. Dermatol. 2015, 25, 91–92. [Google Scholar] [CrossRef]
- Lan, M.Y.; Lan, M.C.; Ho, C.Y.; Li, W.Y.; Lin, C.Z. Pilomatricoma of the Head and Neck: A Retrospective Review of 179 Cases. Arch. Otolaryngol. Head Neck Surg. 2003, 129, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Sia, P.I.; Figueira, E.; Allende, A.; Selva, D. Malignant hair follicle tumors of the periorbital region: A review of literature and suggestion of a management guideline. Orbit 2016, 35, 144–156. [Google Scholar] [CrossRef]
- Goodwin, C.R.; Sankey, E.W.; Liu, A.; Elder, B.D.; Kosztowski, T.; Lo, S.F.; Fisher, C.G.; Clarke, M.J.; Gokaslan, Z.L.; Sciubba, D.M. A systematic review of clinical outcomes for patients diagnosed with skin cancer spinal metastases. J. Neurosurg. Spine 2016, 24, 837–849. [Google Scholar] [CrossRef] [Green Version]
- Melancon, J.M.; Tom, W.L.; Lee, R.A.; Jackson, M.; Jiang, S.I. Management of pilomatrix carcinoma: A case report of successful treatment with mohs micrographic surgery and review of the literature. Dermatologic. Surg. 2011, 37, 1798–1805. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.; Hurwitz, H.I.; Sandler, A.B.; Miles, D.; Coleman, R.L.; Deurloo, R.; Chinot, O.L. Bevacizumab (Avastin®) in cancer treatment: A review of 15 years of clinical experience and future outlook. Cancer Treat. Rev. 2020, 86, 102017. [Google Scholar] [CrossRef] [PubMed]
- Özcan, A.A.; Çiloğlu, E.; Esen, E.; Şimdivar, G.H. Use of topical bevacizumab for conjunctival intraepithelial neoplasia. Cornea 2014, 33, 1205–1209. [Google Scholar] [CrossRef] [PubMed]
- Asena, L.; Dursun Altınörs, D. Topical Bevacizumab for the Treatment of Ocular Surface Squamous Neoplasia. J. Ocul. Pharmacol. Ther. 2015, 31, 487–490. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex (n, %) | |
| Male | 29 (55.8%) |
| Female | 23 (44.2%) |
| Mean age (years, range) | 57 (8 months-87) |
| Distribution (n, %) | |
| Head | 32 (62%) |
| Trunk | 6 (11%) |
| Upper extremity | 6 (11%) |
| Lower extremity | 4 (8%) |
| Neck | 3 (6%) |
| Genitalia | 1 (2%) |
| * Mean size (cm, range) | 2.5 (0.5–15) |
| Location of Metastasis | References | No. of Patients | Location of PC | Time of Onset (months) |
|---|---|---|---|---|
| Lung, lymph nodes | Vadrucci et al. [4] Arslan et al. [34] | 2 | Head | At time of diagnosis |
| Bone | Walker et al. [6] | 1 | Neck | 3 |
| Lung, bone | Sorin et al. [16] | 1 | Head | 8 |
| Parotid gland | Liu et al. [2] | 1 | Head | 12 |
| Brain, bone | Flynn et al. [5] | 1 | Head | 16 |
| Lymph nodes | Otero et al. [18] | 1 | Head | 6 |
| Lung-pleura, liver, bone | Sengoz et al. [22] | 1 | Head | 10 |
| Lymph nodes | Errmann et al. [7] | 1 | Head | 6 |
| Treatment N = 52 | |
|---|---|
| Surgery | |
| Wide local excision | 30 |
| Simple/incisional excision | 15 |
| MMS [19,20,21,23] | 4 |
| Excision + LND [2,3,13] | 3 |
| Adjuvant therapy (after surgery) | |
| RT [2,7,13,29] | 4 |
| CT [34] | 1 |
| CT + RT [16] | 1 |
| Bevacizumab (eye drops) [26] | 1 |
| References | Patients (n°) | Age (years) | Gender | Site | Presentation | Size (cm) | Dermoscopy | Metastasis (Time of Onset) | Follow-Up (Duration) | Therapy (Margins) | Other Therapy | Local Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Karaaslan O et al. [33] | 1 | 65 | M | Head | Ulcerated nodule | 1.5 | NR | - | Periodically (6 months) | Wide local excision (1 cm) | - | - |
| Arslan D et al. [34] | 1 | 76 | M | Head | Asymptomatic nodule | NR | NR | Lymph nodes, lung (at time of diagnosis) | Periodically (6 months) | Excision | CT | - |
| Tvrdi AB et al. [35] | 1 | 10 | F | Head | Firm, asymptomatic nodule | 0.9 | NR | - | NR | Wide local excision | - | - |
| Mukherjee B et al. [36] | 1 | 65 | F | Head | Asymptomatic nodule | 1.2 | NR | - | Periodically (NR) | Excision | - | - |
| Alcántara-González J et al. [37] | 1 | 87 | M | Head | Firm, ulcerated nodule | 1.5 | NR | - | Periodically (12 months) | Incisional biopsy, Wide local excision | Re-excision | - |
| Sato S et al. [38] | 1 | 36 | M | Upper extremity | Ucerated nodule | 1 | NR | - | Periodically (6 months) | Incisional biopsy, Wide local excision (5 mm) | - | - |
| Pauli M et al. [8] | 1 | 68 | F | Head | Firm, asymptomatic nodule | 2 | NR | - | Periodically (12 months) | Incisional biopsy, wide local excision (4 mm) | - | |
| Song M et al. [9] | 1 | 30 | F | Genitalia | Firm asymptomatic nodule | 3 | NR | - | Periodically (8 years) | Excision | Wide local excision (1 cm) | - |
| Walker DM et al. [6] | 1 | 43 | F | Neck | Firm mobile symptomatic nodule | 3 | NR | Vertebral bone (after 3 months) | Exitus | Excision | Metastasis excision, re-excision (CT not initiated) | 1 (after 3 months) |
| Vadrucci M et al. [4] | 1 | 76 | M | Head | Soft-tissue nodule | NR | NR | Lymph nodes, lung (at time of diagnosis) | Exitus after 3 months | Incisional biopsy | - | - |
| Parra L et al. [10] | 1 | 58 | M | Lower extremity | Firm, asymptomatic, ulcerated nodule | 6.5 | NR | - | every 6 months (12 months) | Wide local excision (1 cm) | - | - |
| Villada G et al. [11] | 1 | 79 | F | Lower extremity | Ulcerated, aymptomatic nodule | 2.2 | NR | - | NR | Excision | - | - |
| Bailey EE et al. [12] | 1 | 84 | M | Upper extremity | Nodule | NR | NR | - | NR | Excision | - | - |
| Lohiya S et al. [13] | 1 | 60 | M | Head | Firm, asymptomatic ulcerated nodule | 9 | NR | - | Lost | Wide local excision (5 mm) + lymph node dissection | Adiuvant RT (close margin) | - |
| Cornejo KM et al. [14] | 1 | 44 | M | Trunk | Asymptomatic nodule | NR | NR | - | NR | Excision | Wide local excision, re-excision | - |
| Gupta M et al. [15] | 1 | 25 | M | Neck | Firm, mobile, asymptomatic nodule | 2 | NR | - | Periodically (1 year) | Excision (after FNAC) | Recurrance wide local excision | 1 (after 3 months) |
| Sorin T et al. [16] | 1 | 15 | F | Head | Nodule | 2 | NR | Parietal bone, superior sagittal sinus, lung metastases (after 8 months) | Periodically (4 years) | Excision | Recurrence wide local excision (2 cm), RT, CT | 3 (after 5, 3, 4 months) |
| Alloui M et al. [17] | 2 | 63 | F | Lower extremity | Multinodular lesion | 5 | NR | - | Periodically (2 years) | Incisional biopsy, wide local excision (1 cm) | - | - |
| 66 | F | Head | Nodule | 1.5 | NR | - | Periodically (NR) | Wide local excision | - | - | ||
| Liu JF et al. [2] | 1 | 46 | F | Head | Firm, asymptomatic nodule | 1 | NR | Parotid gland (after 12 months) | Periodically follow-up + imaging (2 years) | Excision | Recurrence excision + lymph node dissection, RT | 2 (after 1 year, 3) |
| Flynn et al. [5] | 2 | 24 | F | Head | Lobulated nodule | 12 | NR | Skull bones, brain (after 16 months) | Exitus | Excision | RT refused (involvement of base and margins) | 1 (after 16 months) |
| 14 | F | Upper extremity | Firm, nontender nodule | 2 | NR | - | Yearly follow-up + chest X-Ray (12 months) | Excision | Wide local excision (ose margin) | - | ||
| Otero MN et al. [18] | 1 | 8 | F | Head | Asynnetric nodule | 9 | NR | Lymph nodes (after 6 months) | Periodically follow-up + ultrasound (6 months) | Wide local excision | Re-excision | - |
| Xing L [19] | 2 | 68 | F | Head | Nodule | 1.9 | NR | - | Periodically (7.5 months) | Mohs surgery (5 mm) | - | - |
| 68 | M | Head | Rapidly growing nodule | 1.1 | NR | - | Periodically follow-up + CT imaging (6 months) | Mohs surgery (5 mm) | Mohs surgery (depth) | - | ||
| Xim JS et al. [20] | 1 | 8-month | M | Head | Nodule | 0.7 | NR | - | Periodically (12 months) | Excision | Wide local excision (1 cm) | - |
| Fernandez-Florez A et al. [21] | 1 | 78 | M | Upper extramity | Ulcerated plaque | 0.6 | NR | - | Periodically (8 months) | Mohs surgery | - | - |
| Martin S et al. [3] | 1 | 74 | M | Head | Nodule with associated regional lymphadenopathy | 4 | NR | - | Exitus | Wide local excision + level II and III neck dissection | - | - |
| Sengoz T et al. [22] | 1 | 37 | F | Head | Nodule | NR | NR | Lung, pleura, liver, bone (after 10 months) | Periodically follow-up with 18F-FDG PET/CT (10 months) | Excision | - | 1 (after 10 months) |
| White C et al. [23] | 1 | 62 | M | Head | Nodule | 3 | Focal ulceration, irregularly telangiectasias | - | 6-monthly follow-up (14 months) | Excision | Mohs surgery | - |
| Eckhoff MD et al. [24] | 1 | 46 | M | Upper extremity | Nodule | 15 | NR | - | Periodically(24 months) | Excision margin-controlled | Recurrence excision | 1 (after 4 months) |
| Yeo MK et al. [25] | 1 | 43 | F | Head | Nodule | 2.1 | NR | - | NR | Excision | no | - |
| Harbiyeli II et al. [26] | 1 | 45 | F | Head | Nontender nodule | 1.5 | NR | - | Periodically 12 months) | Excision | Re-excision (2 mm safety margin) + bevacizumab eye drops | - |
| Dell’Antonia M et al. [27] | 1 | 80 | M | Head | Rapidly growing, ulcerated nodule | 3.5 | Telangiectasias, white structureless areas, yellowish hues, erythematous background | - | 6-monthly follow-up + imaging (5 years) | Wide local excision | - | - |
| Subramanyam et al. [28] | 1 | 51 | M | Lower extremity | Slow-growing nodule | 6 | NR | - | 3-monthly follow-up for the first 2 years (MRI and PET-CT scans) | Partial excision, wide local excision | - | - |
| Papadakis M et al. [29] | 1 | 79 | F | Head | Slow growing nontender nodule | NR | NR | - | Periodically (4 years) | Wide local excision | Recurrence excision + adjuvant RT | 1 (after 2 months) |
| Briley T et al. [30] | 1 | 51 | M | Trunk | Rapidly growing nontender nodule | 4 | NR | - | 1 month | Wide local excision (1 cm) | - | - |
| Herrmann JL et al. [7] | 13 | 72 | M | Neck | Rapidly growing nodule | 1 | NR | - | Periodically (>6 months) | Wide local excision | - | - |
| 68 | M | Head | Rapidly growing nodule | 0.8 | NR | - | Periodically (>6 months) | Wide local excision | - | 1 (NR) | ||
| 67 | M | Head | Ulcerated papule | 0.8 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 78 | M | Head | Rapidly growing nodule | 2 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 62 | M | Head | Rapidly growing nodule | 1 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 67 | M | Head | Ulcerated nodule | 3 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 78 | M | Trunk | Rapidly growing nodule | 0.8 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 76 | M | Trunk | Rapidly growing nodule | 0.9 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 59 | F | Head | Rapidly growing nodule | 0.5 | NR | Lymph nodes (after 6 months) | Periodically (>6 months) | Wide local excision | Adjuvant RT (lymph nodes) | - | ||
| 51 | F | Head | Rapidly growing nodule | 1.5 | NR | - | Periodically (>6 months) | Wide local excision | - | 1 (NR) | ||
| 63 | F | Upper extremity | Rapidly growing nodule | 2 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 71 | F | Trunk | Rapidly growing nodule | 3 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| 69 | F | Trunk | Rapidly growing nodule | 3.5 | NR | - | Periodically (>6 months) | Wide local excision | - | - | ||
| Weng G et al. [31] | 1 | 53 | F | Trunk | Tenacious subcutaneous nodule | 2 | NR | - | Periocally follow-up + ultrasound (4 years) | Excision | Recurrence excision (RT refused) | 1 (after 7 months) |
| Ravaioli GM [32] | 1 | 69 | M | Head | Rapidly growing reddish nodule | 1.4 | Arborized vessels, purple/blue areas, white/yellowish blotches | - | NR | Excision | - | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toffoli, L.; Bazzacco, G.; Conforti, C.; Guarneri, C.; Giuffrida, R.; Zelin, E.; di Meo, N.; Zalaudek, I. Pilomatrix Carcinoma: Report of Two Cases of the Head and Review of the Literature. Curr. Oncol. 2023, 30, 1426-1438. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30020109
Toffoli L, Bazzacco G, Conforti C, Guarneri C, Giuffrida R, Zelin E, di Meo N, Zalaudek I. Pilomatrix Carcinoma: Report of Two Cases of the Head and Review of the Literature. Current Oncology. 2023; 30(2):1426-1438. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30020109
Chicago/Turabian StyleToffoli, Ludovica, Giulia Bazzacco, Claudio Conforti, Claudio Guarneri, Roberta Giuffrida, Enrico Zelin, Nicola di Meo, and Iris Zalaudek. 2023. "Pilomatrix Carcinoma: Report of Two Cases of the Head and Review of the Literature" Current Oncology 30, no. 2: 1426-1438. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30020109