1. Introduction
In recent years, the advancement of knowledge of the immune system’s molecular mechanisms against cancer has allowed the clinical development of new immunological therapies for the treatment of tumors, including checkpoint inhibitor therapy (ICIs). ICIs are antibodies that increase the antitumor immunity of the host, blocking inhibitors of T cell activation and function, such as T receptors, defined immuno-checkpoints, and facilitating T-cell-mediated actions against tumors. Inhibitors of checkpoints hold the function of restoring the normal action of T lymphocytes and, therefore, their ability to kill cancer cells, blocking the signal pathway of immunosuppressants. They work not only by stimulating T cells but also by switching on other innate and adaptive arm cells.
The main targets include Cytotoxic T cells 4 (CTLA-4), receptor 1 of programmed cell death (PD-1), and its ligand (PD-L1) known as Ipilimumab, Tremelimumab, Pembrolizumab, Nivolumab, Atezolizumab, Avelumab, Durvalumab, or Cemiplimab (
Table 1). The CTLA-4 and PD-1 receptors are negative regulators of the immune function of T cells; the inhibition of these targets consequently determines the increased activation of the immune system. These drugs are used in several advanced-stage malignancies, such as melanoma, renal cell or urothelial carcinoma, lymphoma, small or non-small cell lung cancer, and colorectal cancer, often improving the patients’ survival that, nevertheless, depends also on multiple variables such as the tumor histotype, the stage of disease, and clinical status of the patient [
1,
2,
3]. At the same time, they can induce autoimmune toxicities with their mechanism of action, and it is important for the clinician to recognize their side effects, but also for the radiologist because sometimes imaging findings may precede clinical manifestation.
Immune-related adverse events (irAEs) occur mainly in the skin, gastrointestinal, hepatic, and endocrine systems, including itching, rash, nausea, diarrhea, and thyroiditis (
Table 2). The latter events are more frequently associated with treatment with anti-PD-1 antibodies (Pembrolizumab and Nivolumab), while colitis and hypophysitis with anti-CTLA-4 antibodies (Ipilimumab). The onset is typically between 3 and 6 months from initial administration; however, irAEs can occur at any time, even after cessation of treatment (“delayed effect”) [
4].
A grading system called CTCAE v5.0 (Common Terminology Criteria for Adverse Events) has been created to classify irAEs into five grades based on symptoms, signs, or test results [
5]. Grade 1 is generally asymptomatic or associated with mild symptoms without the need for intervention. Grade 2 usually requires minimal or non-invasive intervention. Whereas grade 3 is a severe medical condition in which hospitalization is indicated. Finally, grade 4 requires urgent intervention to avoid fatal consequences, and grade 5 corresponds to death determined by adverse effect to irAEs. The management of these adverse reactions can lead to a delay in the path of the patient’s oncological care. For instance, in some cases it is required to stop treatments, start steroid administration, or even hospitalize the patient.
The incidence and severity or irAEs also depend on the agent; in fact, anti-CTLA4 usually has a greater percentage of adverse effects, even up to 80%, compared to anti-PD1 (27%) and anti-PDL1 (17%) [
6].
In a review and meta-analysis, Wang et al. reported an incidence of adverse effects after PD-1 and PD-L1 inhibitors of 66%, with a grade 3 or higher in the CTCAE v5.0 of 14%. The reported incidence of serious and dangerous events is about 6% [
7].
irAEs could be completely asymptomatic or paucisymptomatic. Tirumani et al., in a study regarding Ipilimumab therapy, reported an earlier onset of irAE radiological findings compared to their clinical manifestations, in more than 33% patients. Imaging techniques, such as Computed Tomography (CT), Magnetic Resonance Imaging (MRI), Ultrasound (US), or Fluorodeoxyglucose-Positron Emission Tomography (FDG-PET), usually carried out for oncological follow-up, can also recognize immune-related adverse event radiological findings, before the onset of clinical manifestations, allowing the classification of these conditions [
8].
Hence, radiologists should be ready to identify the main imaging findings of irAEs, in order to discuss in a multidisciplinary team the more correct therapeutic management, commonly performed with ICIs suspension and corticosteroid administration.
This is a comprehensive review of the main imaging features of irAEs, involving the colon, liver, pancreas, lung, endocrine system, kidney, heart, and nervous system, that could be a useful diagnostic tool for radiologists, but also for clinicians.
Table 1.
Mechanism of action of the most-used ICIs and their more common indications [
9,
10]. Furthermore, there are other potential targets and mechanisms of action, some still under clinical trials, such as antibody anti-BTLA, VISTA, TIM-3, and CD47, agonist of costimulatory receptors (CD137, CD134, GITR, ICOS, CD40, and CD28). Other possible mechanisms of action include Chimeric Antigen Receptor T cell, adoptive cell transfer (ACT) of ex vivo expanded tumor-infiltrating lymphocytes (TILs), or ImmTAC (Immune Mobilizing Monoclonal TCRs Against Cancer). Moreover, oncolytic viruses (OVs) are another promising class of immunotherapies for treating cancer [
11,
12].
Table 1.
Mechanism of action of the most-used ICIs and their more common indications [
9,
10]. Furthermore, there are other potential targets and mechanisms of action, some still under clinical trials, such as antibody anti-BTLA, VISTA, TIM-3, and CD47, agonist of costimulatory receptors (CD137, CD134, GITR, ICOS, CD40, and CD28). Other possible mechanisms of action include Chimeric Antigen Receptor T cell, adoptive cell transfer (ACT) of ex vivo expanded tumor-infiltrating lymphocytes (TILs), or ImmTAC (Immune Mobilizing Monoclonal TCRs Against Cancer). Moreover, oncolytic viruses (OVs) are another promising class of immunotherapies for treating cancer [
11,
12].
| ICIs | Mechanism of Action | Indication |
|---|
| Ipilimumab [13] | Anti-CTLA-4 antibody | Melanoma Lung Ovaries Prostate Kidney Colorectal cancer
|
| Tremelimumab [14] | Human IgG2 monoclonal antibody that blocks CTLA-4 | |
| Pembrolizumab [15] | Anti-PD-1 antibody | Melanoma NSCLC and SCLS SCCHN Gastric and esophageal cancer Cervical cancer HCC Merkel cell carcinoma RCC Endometrial carcinoma Classical Hodgkin lymphoma Advanced Merkel-cell carcinoma Primary mediastinal large B-cell lymphoma Urothelial carcinoma
|
| Nivolumab [13] | Anti-PD-1 antibody | |
| Atezolizumab [7] | Anti-PD-L1 antibody | |
| Avelumab [16] | Anti-PD-L1 antibody | Merkel cell carcinoma Urothelial carcinoma RCC
|
| Durvalumab [4] | Anti-PD-L1 antibody | Urothelial carcinoma NSCLC
|
| Relatlimab [17] | Anti-LAG3 antibody | |
Table 2.
Main adverse effect organized according to the organ or system involved [
18].
Table 2.
Main adverse effect organized according to the organ or system involved [
18].
| Organs | Symptoms |
|---|
| Systemic Adverse Effects | |
| Skin [19,20] | Pruritus Morbilliform or acneiform eruption Lichenoid reactions Eczema Vitiligo Psoriasis Bullous dermatoses Stevens–Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) Drug reaction with eosinophilia and systemic symptoms (DRESS)
|
| Intestinal [21,22] | |
| Hepatic [23] | |
| Pulmonary [24] | |
| Endocrine system [25] | |
| Cardiac [26] | Myocarditis Pericarditis Cardiomyopathy Cardiac fibrosis Arrhythmias
|
| Renal [27] | |
| Rheumatologic [18] | |
| Nervous system [28] | |
| Ocular [18] | Uveitis, Peripheral ulcerative keratitis Vogt–Koyanagi–Harada syndrome Choroidal neovascularization Melanoma-associated retinopathy Idiopathic orbital inflammation Episcleritis, blepharitis Optic nerve swelling
|
| Hematologic [18] | |
2. Gastrointestinal
2.1. Incidence
After dermatitis, GI tract toxicity is the most frequent irAEs in patients treated with ICIs, with a higher incidence and worst severity in cases of treatment with anti–CTLA-4 antibodies (30–40%) or a combination of different ICIs (10%) [
21,
29].
ICI-related inflammation can involve any portion of the alimentary canal, from oral mucosa to rectum; hence, inflammation of the upper GI tract can also happen with esophagitis, gastritis and, duodenitis [
22,
30,
31].
Upper GI adverse events, more commonly related to PD-1 inhibitors, are usually less frequent and poorly described in the literature. Conversely, lower GI adverse events are reported in almost 1/3 of patients treated with CTLA-4 inhibitors.
2.2. Sign and Symptoms
This kind of toxicity more commonly involves small and large bowels, presenting usually with enterocolitis, mainly because of CTLA4 therapy (Ipilimumab). Ileitis without colitis is, instead, an uncommon event.
Colitis may present with a wide spectrum of manifestations; it could also be asymptomatic. However, the most frequent symptoms are abdominal pain and diarrhea, that reach a reported incidence of almost 45% in cases of combined ICI therapy [
13,
32].
Fever, hematochezia, or mucus in stool and endoscopic evidence of colon inflammation could be present [
13]. Upper GI toxicity can be an isolated event, but it frequently coexists with lower GI toxicity, usually presenting with decreased appetite, abdominal pain, and nausea and/or vomit, which are non-specific symptoms often encountered in cancer patients [
33].
Severe cases that implicate life-threatening complications, such as bowel perforation, sepsis, bleedings, and dehydration, are rare.
The symptoms usually occur after the second or third dose of ICI, within 6–8 weeks from the beginning of treatment; nevertheless, they could manifest with various onset timings even several months after the end of therapy (“delayed toxicity”) [
32].
2.3. Diagnosis and Imaging
Diagnosis of upper or lower GI involvement is achieved with endoscopy, which can demonstrate inflammation, erythema, ulceration, and mucosal friability. Sometimes a histological sampling is performed, showing neutrophilic, lymphocytic, or eosinophilic intra-epithelial infiltrates and crypt invasion.
Nevertheless, CT could offer a less invasive, though less accurate, diagnostic alternative; moreover, in some cases, imaging features could precede the onset of symptoms [
34].
In two studies, Garcia-Neur et al. and Tirumani et al. have reported a good correlation between CT findings and evidence of ICIs-related colitis. In a study aimed at recognizing colitis, involving 53 patients, Wang et al. reported a sensitivity of CT of 53% and a specificity of 78% [
35].
Furthermore, CT should always be considered if severe complications are suspected, for instance toxic megacolon, bleedings, or intestinal perforation [
34].
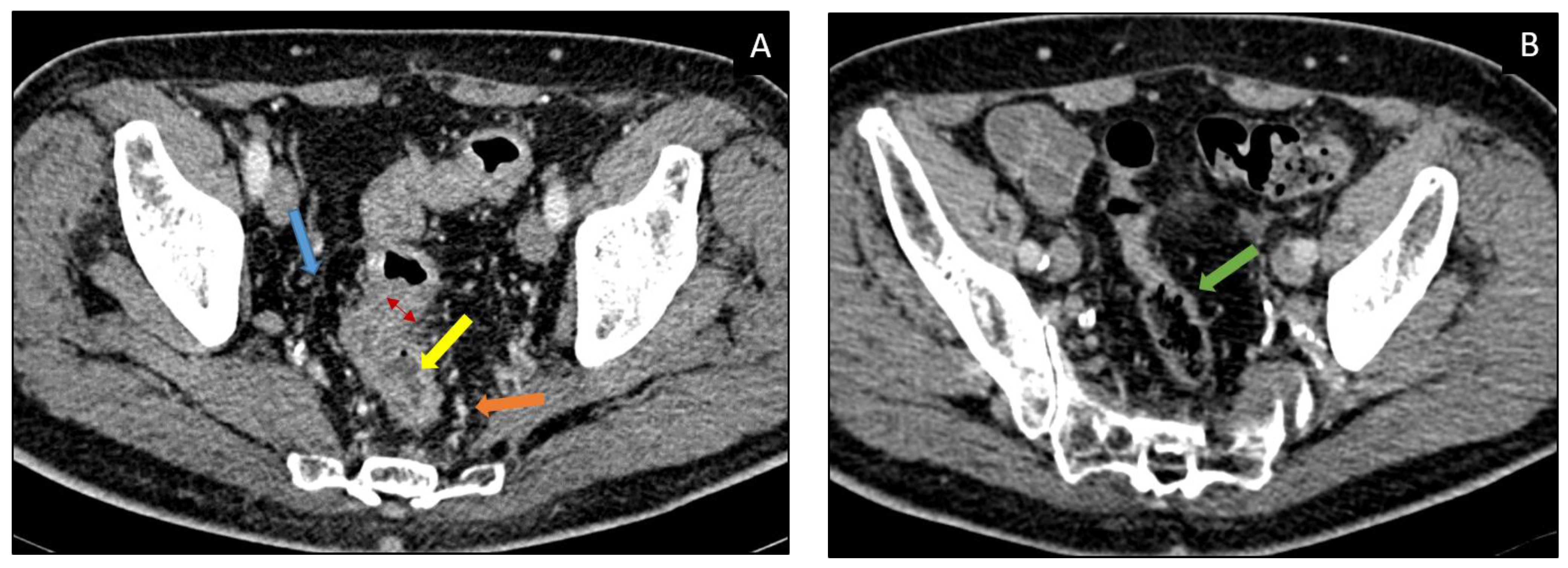
There are two main CT patterns of immune-related colitis described in the literature, diffuse colitis or segmental colitis associated with diverticulosis (SCAD) which is usually confined to the sigmoid (
Figure 1). A less frequent pattern has been described by Barina et al. which corresponds to isolated recto-sigmoid colitis without diverticulosis (
Table 3) [
36].
2.4. Differential Diagnosis
Possible differential diagnoses are Crohn’s disease and ulcerative colitis, infectious colitis, and pseudomembranous colitis.
2.5. Management
GI adverse effects management is performed by discontinuing ICI administration and starting methylprednisolone; Infliximab or Vedolizumab may be considered as a second-line therapy. In grade 4, the permanent withdrawal of all ICIS is strongly recommended.
6. Endocrine System
Immune-related endocrine adverse events are among the most common toxicities in patients treated with ICIs, happening in almost 40% of cases [
61,
62].
In a meta-analysis by Abdel-Rahman et al., patients treated with these therapies reported a greater risk of hypophysitis, hypo- and hyperthyroidism, and adrenal insufficiency, but without a specific association with incidence, severity, and distinct tumors or drugs (CTLA-4 vs. PD-1) [
63].
Other studies demonstrated a greater prevalence of thyroid disorders in the case of anti-PD-1 treatments and a higher rate of pituitary disorders in patients treated with anti CTLA-4 [
63].
In descending order, the most common organs involved are thyroid, pituitary, adrenal, and beta cells of pancreatic islets.
Even though symptoms usually present within 6 months of ICI initiation, the onset can be variable and unpredictable [
64].
Severity is widely variable. Typically, these endocrinopathies are manageable with prompt recognition and treatment; however, they are rarely fatal, but rather these conditions can alter the patients’ quality of life. In fact, most other systems are affected by transient inflammation that resolves with the restoration of normal organ function, whereas ICI-related endocrinopathies can result in permanent, irreversible endocrine dysfunction [
65]. Some cases of diabetes mellitus (DM) have proven fatal when presenting in diabetic ketoacidosis.
Manifestations are usually subtle and non-specific, often overlapping with cancer-related or other therapy-related complications (e.g., fatigue, nausea); hence, hormone level monitoring is critical.
12. Cardiac Toxicity
12.1. Incidence
Cardiotoxicity represents an uncommon irAE (incidence < 1%). Nevertheless, the mortality rate is high (50%); therefore, clinicians and radiologists need to be aware of these complications and to recognize the main signs, symptoms, and imaging findings, to promptly achieve the diagnosis and appropriately guide patient management.
Cardiovascular irAEs are more common in patients treated with ICI in combinations than in those undergoing monotherapy. Moreover, they are more likely in cases of co-administration of another cardiotoxic drug or in cases of previous cardiovascular disease or pre-existing risk factors.
The most reported complications are myocarditis, with a higher incidence in the case of combined treatment with Nivolumab and Ipilimumab [
81].
12.2. Sign and Symptoms
Clinical symptoms and signs of ICI-related myocarditis are heterogeneous; hence, diagnosis is often challenging. In addition, pathophysiology is still not completely understood. Studies suggest that a tumor-activated T cell population may cross-react with cardiac antigens exposed on cardiomyocytes. It can occur from 2 days to 15 months after the start of ICIs and is potentially fatal [
26].
12.3. Diagnosis and Imaging
The gold standard for the diagnosis of myocarditis is the endomyocardial biopsy, which, however, as an invasive approach is accomplished in rare cases. On the other side, cardiac biomarkers and ECGs are non-specific although easy to use. Therefore, the diagnostic challenges have opened the door to different imaging techniques in assessing ICI-induced cardiotoxicity (
Table 12).
12.4. Differential Diagnosis
Myocarditis has many different etiologies, such as infectious (viral, bacterial, fungal, or parasites) or non-infectious. Non-infectious etiologies include radiation, transplant rejection, giant cell myocarditis, autoimmune disease, and also drugs (for instance antibiotics, anticonvulsants, anti-inflammatories, or diuretics).
12.5. Management
According to CTCAE v5.0 after grade 1, permanent withdrawal of ICIs is necessary. In some refractory cases, corticosteroids and Infliximab are recommended.

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




