PD-L1 Expression in Cutaneous Angiosarcomas: A Systematic Review with Meta-Analysis


 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy, Eligibility Criteria, and Study Selection
2.2. Statistical Analysis
3. Results
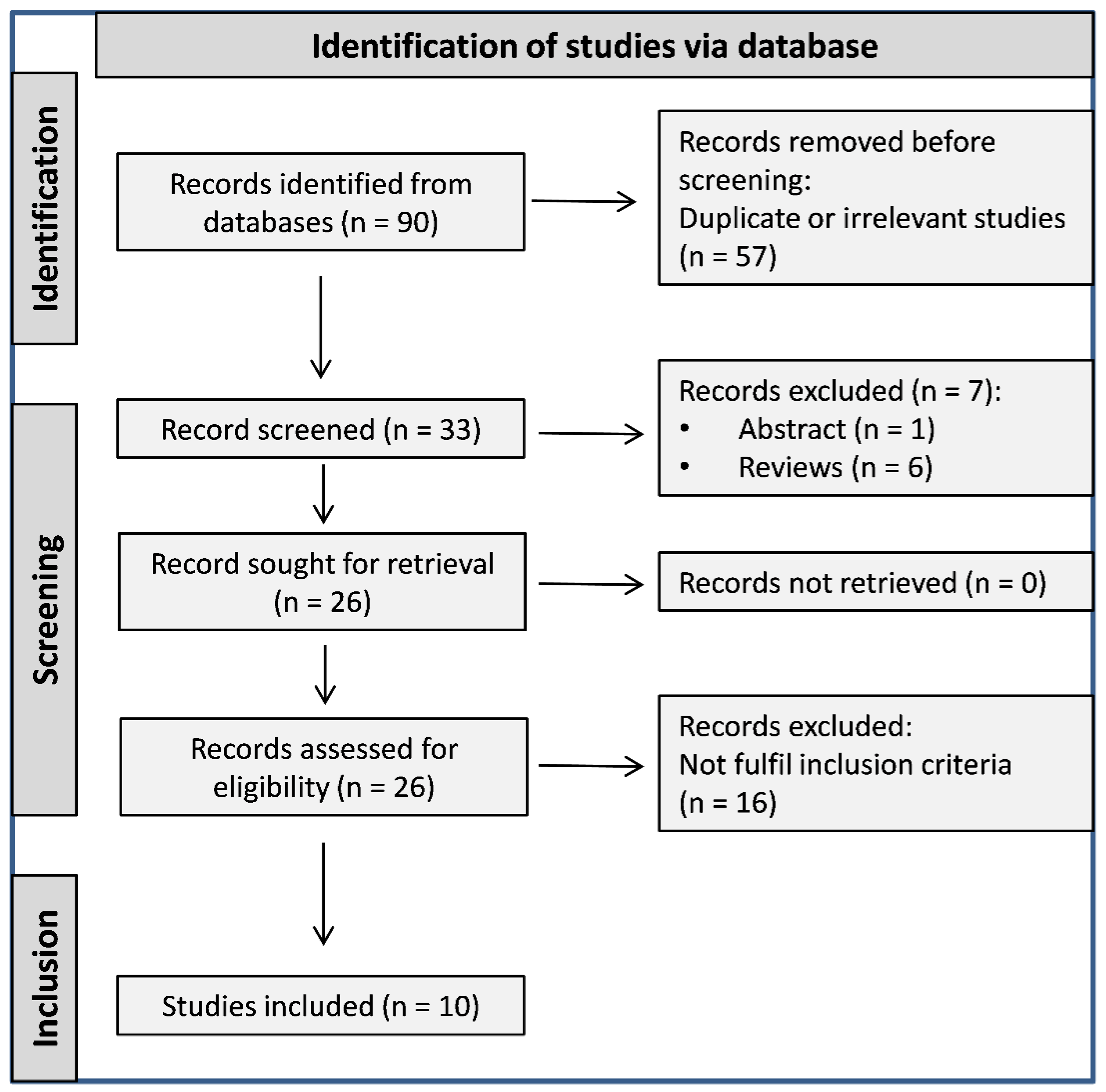
3.1. Literature Search and Study Selection
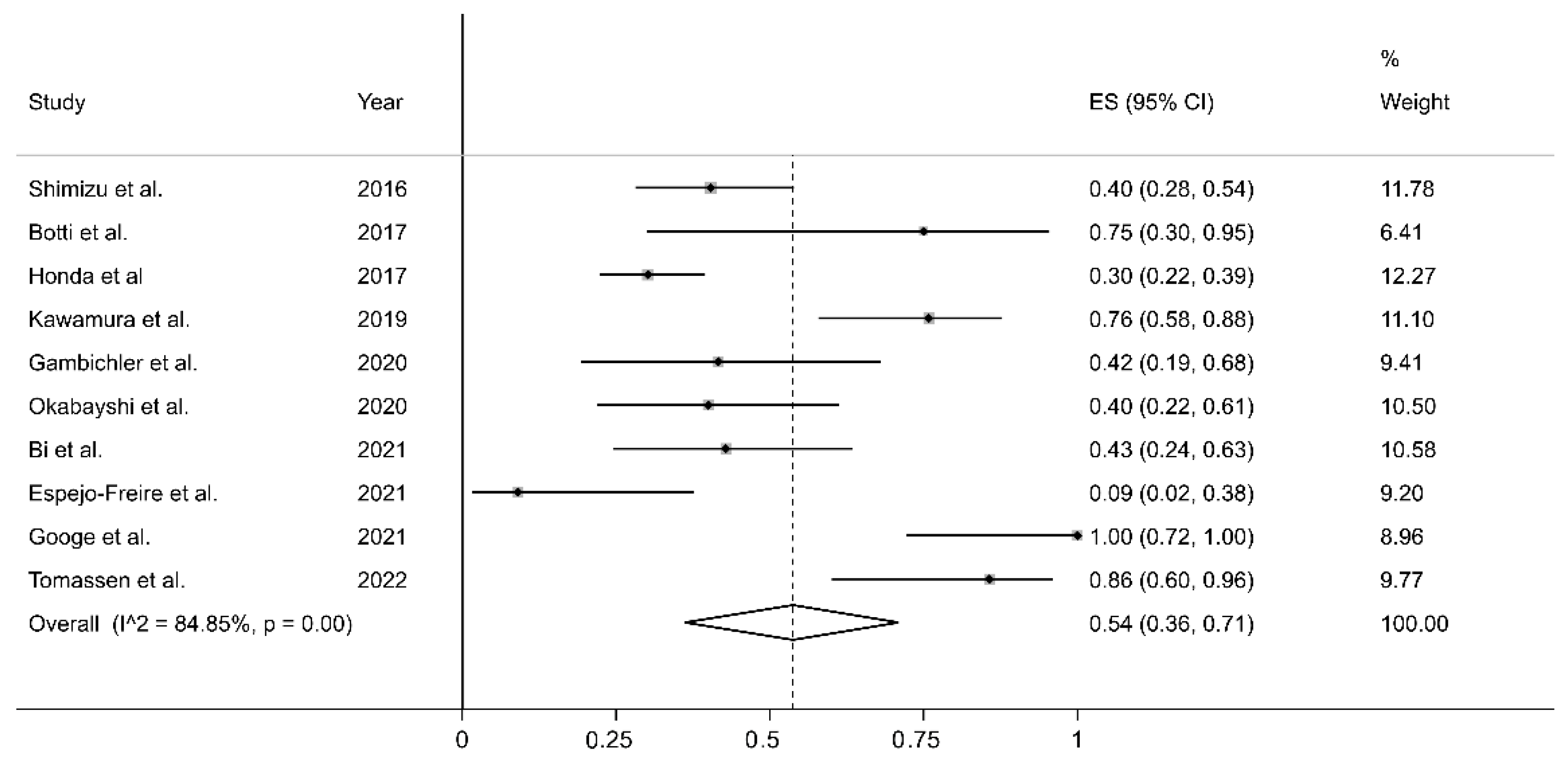
3.2. PD-L1 Expression in Cutaneous Angiosarcomas: Results of Individual Studies and Syntheses
3.3. Quality Assessment
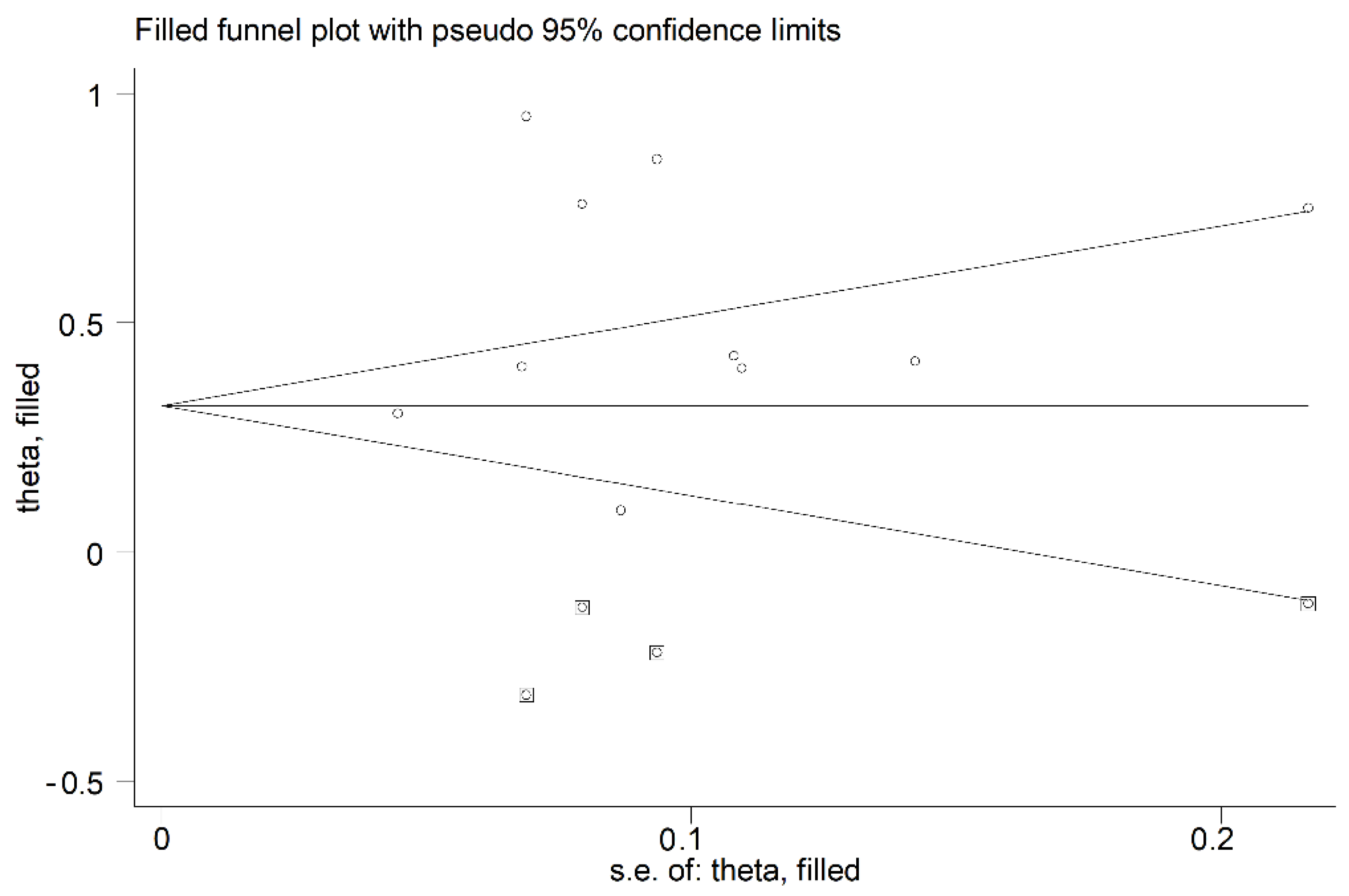
3.4. Publication Bias
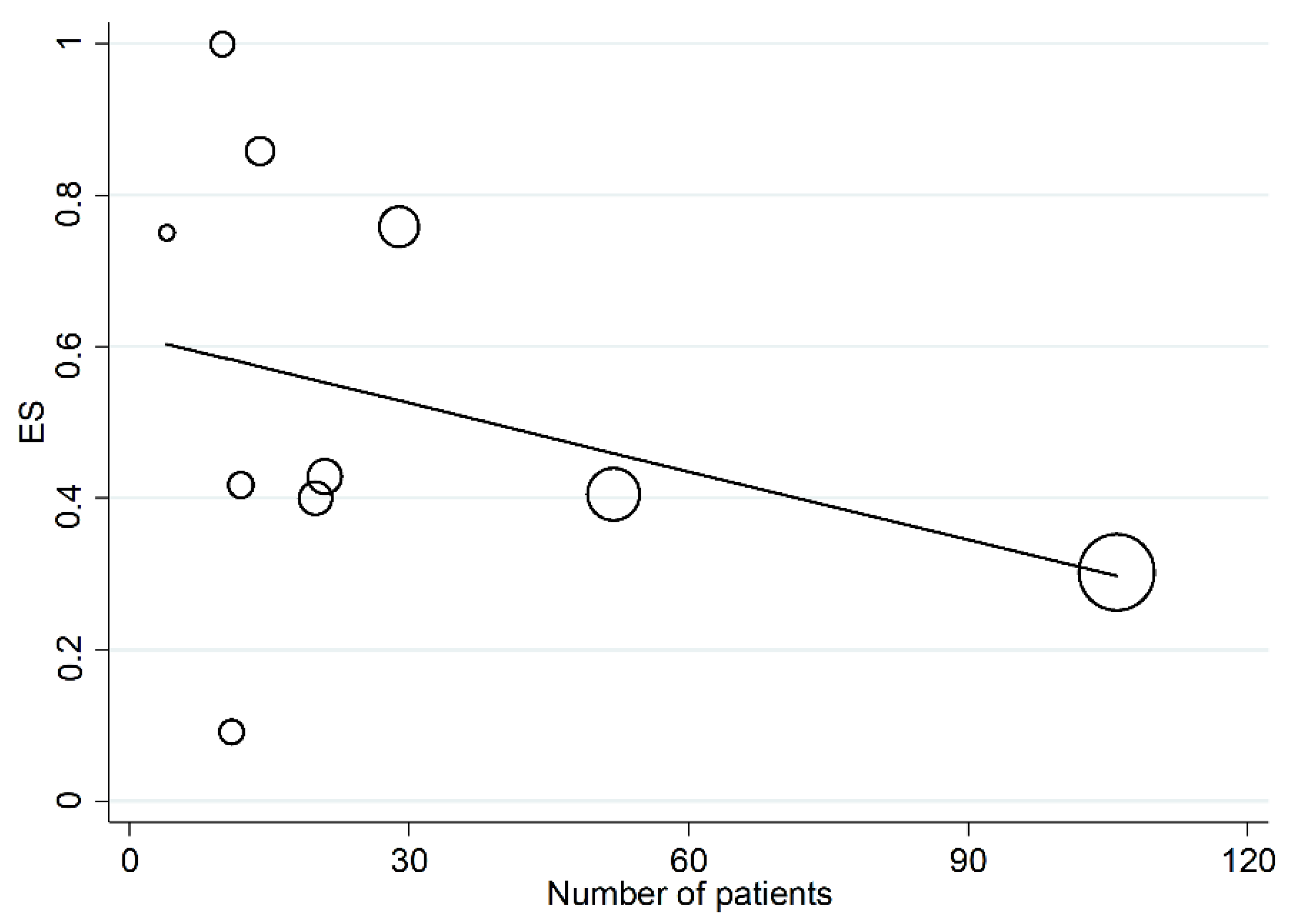
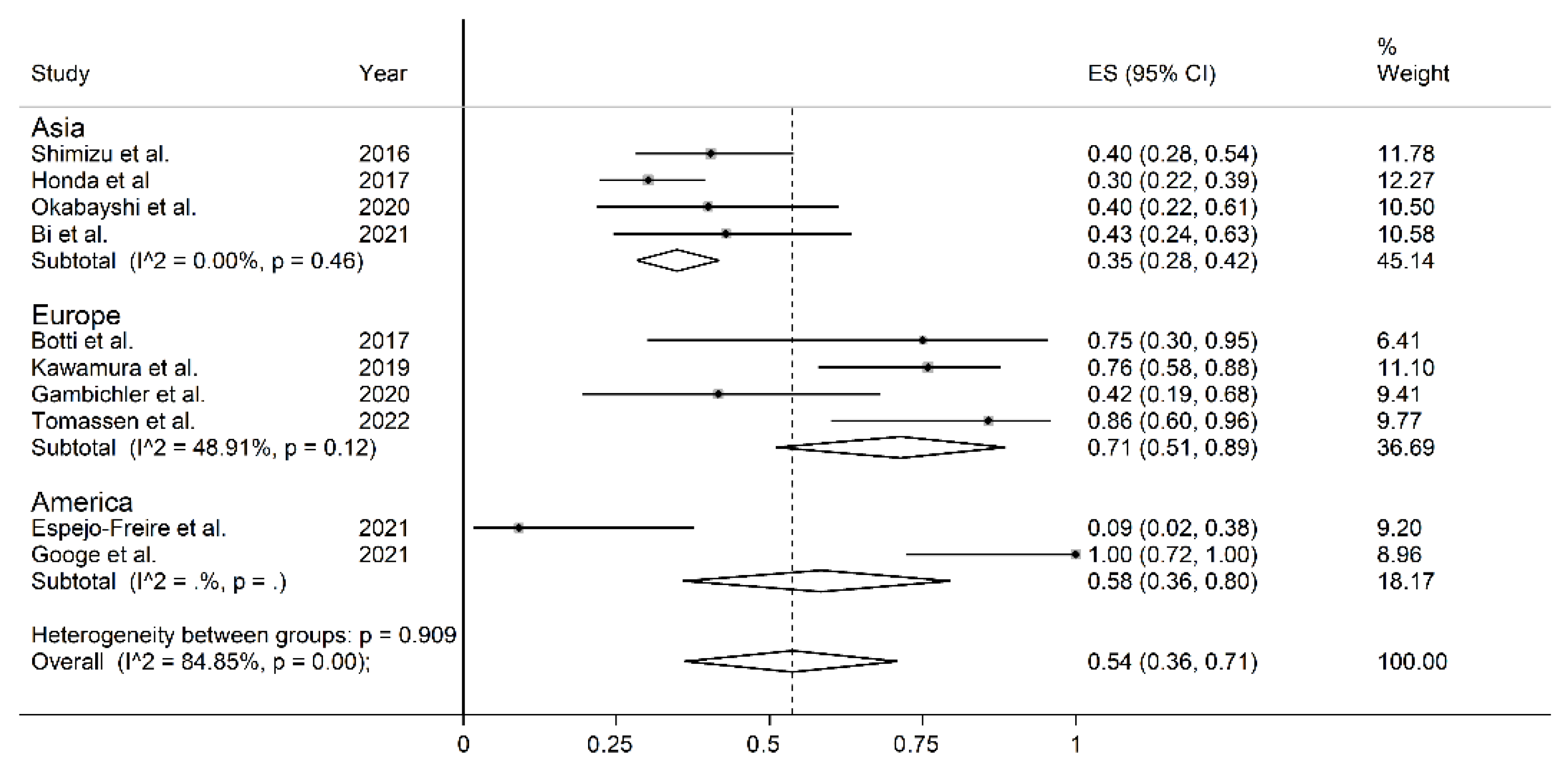
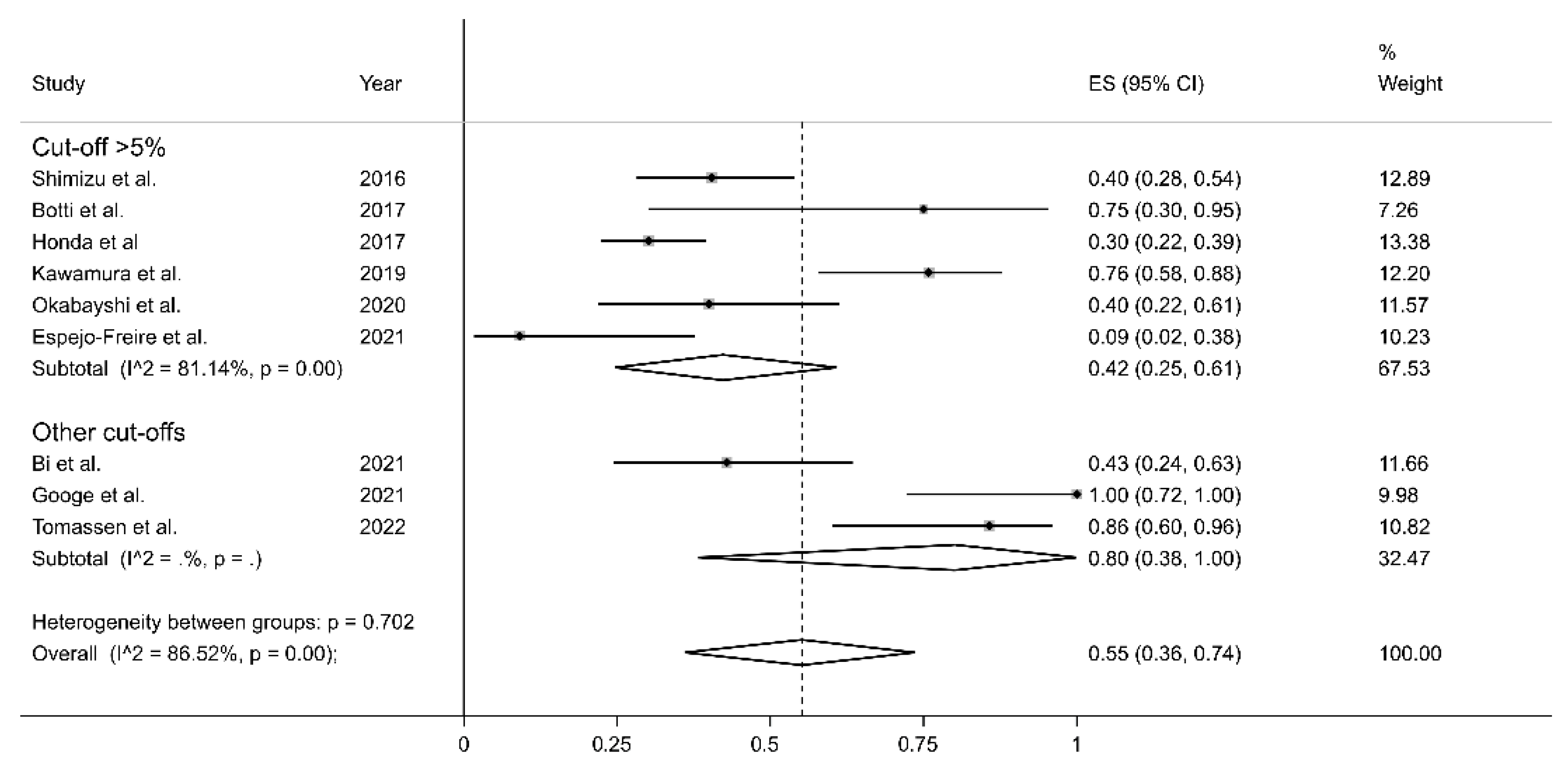
3.5. Meta-Regression and Sub-Group Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Botti, G.; Scognamiglio, G.; Marra, L.; Pizzolorusso, A.; Di Bonito, M.; De Cecio, R.; Cantile, M.; De Chiara, A. Programmed Death Ligand 1 (PD-L1) expression in primary angiosarcoma. J. Cancer 2017, 8, 3166–3172. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, Y.; Yoshino, K.; Fujimura, T.; Nakamura, Y.; Okiyama, N.; Ishitsuka, Y.; Watanabe, R.; Fujimoto, M. Cutaneous angiosarcoma: The possibility of new treatment options especially for patients with large primary tumor. Front. Oncol. 2018, 8, 46. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, G.; Rozzo, C.M.; Colombino, M.; Casula, M.; Sini, M.C.; Manca, A.; Pisano, M.; Doneddu, V.; Paliogiannis, P.; Cossu, A. Are molecular alterations linked to genetic instability worth to be included as biomarkers for directing or excluding melanoma patients to immunotherapy? Front. Oncol. 2021, 11, 666624. [Google Scholar] [CrossRef] [PubMed]
- Buriolla, S.; Pelizzari, G.; Corvaja, C.; Alberti, M.; Targato, G.; Bortolot, M.; Torresan, S.; Cortiula, F.; Fasola, G.; Follador, A. Immunotherapy in NSCLC patients with brain metastases. Int. J. Mol. Sci. 2022, 23, 7068. [Google Scholar] [CrossRef] [PubMed]
- Park, J.C.; Krishnakumar, H.N.; Saladi, S.V. Current and future biomarkers for immune checkpoint inhibitors in head and neck squamous cell carcinoma. Curr. Oncol. 2022, 29, 4185–4198. [Google Scholar] [CrossRef] [PubMed]
- Franzén, A.S.; Raftery, M.J.; Pecher, G. Implications for immunotherapy of breast cancer by understanding the microenvironment of a solid tumor. Cancers 2022, 14, 3178. [Google Scholar] [CrossRef]
- Lee, J.B.; Ahn, B.C.; Kim, S.H.; Lee, Y.H.; Han, J.W.; Jeon, M.K.; Kim, S.H.; Kim, H.S. Prognostic implications of PD-L1 expression in patients with angiosarcoma. Future Sci. OA 2021, 7, FSO691. [Google Scholar] [CrossRef]
- Shimizu, A.; Kaira, K.; Okubo, Y.; Utsumi, D.; Yasuda, M.; Asao, T.; Nishiyama, M.; Takahashi, K.; Ishikawa, O. Positive PD-L1 Expression Predicts Worse Outcome in Cutaneous Angiosarcoma. J. Glob. Oncol. 2017, 3, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Orth, M.F.; Buecklein, V.L.; Kampmann, E.; Subklewe, M.; Noessner, E.; Cidre-Aranaz, F.; Romero-Pérez, L.; Wehweck, F.S.; Lindner, L.; Issels, R.; et al. A comparative view on the expression patterns of PD-L1 and PD-1 in soft tissue sarcomas. Cancer Immunol. Immunother. 2020, 69, 1353–1362. [Google Scholar] [CrossRef]
- Honda, Y.; Otsuka, A.; Ono, S.; Yamamoto, Y.; Seidel, J.; Morita, S.; Hirata, M.; Kataoka, T.R.; Takenouchi, T.; Fujii, K.; et al. Infiltration of PD-1-positive cells in combination with tumor site PD-L1 expression is a positive prognostic factor in cutaneous angiosarcoma. Oncoimmunology 2016, 6, e1253657. [Google Scholar] [CrossRef]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Tobias, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, A.; Kawamura, T.; Riddell, M.; Hikita, T.; Yanagi, T.; Umemura, H.; Nakayama, M. Regulation of programmed cell death ligand 1 expression by atypical protein kinase C lambda/iota in cutaneous angiosarcoma. Cancer Sci. 2019, 110, 1780–1789. [Google Scholar] [CrossRef] [PubMed]
- Gambichler, T.; Koim, S.; Wrobel, M.; Käfferlein, H.U.; Brüning, T.; Stockfleth, E.; Becker, J.C.; Lang, K. Expression of programmed cell death proteins in Kaposi sarcoma and cutaneous angiosarcoma. J. Immunother. 2020, 43, 169–174. [Google Scholar] [CrossRef]
- Okabayshi, M.; Kataoka, T.R.; Oji, M.; Mibayashi, S.; Odani, K.; Otsuka, A.; Haga, H. IGF2BP3 (IMP3) expression in angiosarcoma, epithelioid hemangioendothelioma, and benign vascular lesions. Diagn. Pathol. 2020, 15, 26. [Google Scholar] [CrossRef]
- Bi, Y.; Ge, L.; Ren, X.; Pang, J.; Zhao, Y.; Liang, Z. Tumor microenvironment and its clinicopathological and prognostic associations in surgically resected cutaneous angiosarcoma. Clin. Transl. Oncol. 2022, 24, 941–949. [Google Scholar] [CrossRef]
- Espejo-Freire, A.P.; Elliott, A.; Rosenberg, A.; Costa, P.A.; Barreto-Coelho, P.; Jonczak, E.; D’amato, G.; Subhawong, T.; Arshad, J.; Diaz-Perez, J.A.; et al. Genomic Landscape of Angiosarcoma: A Targeted and Immunotherapy Biomarker Analysis. Cancers 2021, 13, 4816. [Google Scholar] [CrossRef]
- Googe, P.B.; Flores, K.; Jenkins, F.; Merritt, B.; Moschos, S.J.; Grilley-Olson, J.E. Immune checkpoint markers in superficial angiosarcomas: PD-L1, PD-1, CD8, LAG-3, and tumor-infiltrating lymphocytes. Am. J. Dermatopathol. 2021, 43, 556–559. [Google Scholar] [CrossRef]
- Tomassen, T.; Weidema, M.E.; Hillebrandt-Roeffen, M.H.S.; van der Horst, C.; PALGA Group; Desar, I.M.E.; Flucke, U.E.; Versleijen-Jonkers, Y.M.H. Analysis of PD-1, PD-L1, and T-cell infiltration in angiosarcoma pathogenetic subgroups. Immunol. Res. 2022, 70, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, M.; Rashid, S.; Al-Bozom, I.A. PD-L1 immunostaining: What pathologists need to know. Diagn. Pathol. 2021, 16, 94. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, Y.; Guo, G.; Cai, X.; Yu, H.; Cai, Y.; Zhang, B.; Hong, S.; Zhang, L. Nivolumab plus ipilimumab versus pembrolizumab as chemotherapy-free, first-line treatment for PD-L1-positive non-small cell lung cancer. Clin. Transl. Med. 2020, 10, 107–115. [Google Scholar] [CrossRef]
- Mouritzen, M.T.; Carus, A.; Ladekarl, M.; Meldgaard, P.; Nielsen, A.W.M.; Livbjerg, A.; Larsen, J.W.; Skuladottir, H.; Kristiansen, C.; Wedervang, K.; et al. Nationwide Survival Benefit after Implementation of First-Line Immunotherapy for Patients with Advanced NSCLC—Real World Efficacy. Cancers 2021, 13, 4846. [Google Scholar] [CrossRef] [PubMed]
- Putzu, C.; Canova, S.; Paliogiannis, P.; Lobrano, R.; Sala, L.; Cortinovis, D.L.; Colonese, F. Duration of immunotherapy in non-small cell lung cancer survivors: A lifelong commitment? Cancers 2023, 15, 689. [Google Scholar] [CrossRef] [PubMed]
- Mastracci, L.; Grillo, F.; Parente, P.; Gullo, I.; Campora, M.; Angerilli, V.; Rossi, C.; Sacramento, M.L.; Pennelli, G.; Vanoli, A.; et al. PD-L1 evaluation in the gastrointestinal tract: From biological rationale to its clinical application. Pathologica 2022, 114, 352–364. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author Year, Country | n | Age Mean ± SD | Sex (M/F) | PD-L1 Antibody Clone | Cut-Off | Cut-Off < 1% | Cut-Off 1–49% | Cut-Off > 50% | PD-L1 Positive |
|---|---|---|---|---|---|---|---|---|---|
| Shimizu et al., 2016, Japan [8] | 52 | 76 | 33/19 | NR | >5% | NR | NR | NR | 21 |
| Botti et al., 2017, Italy [1] | 4 | NR | NR | SP142 | >5% | NR | NR | NR | 3 |
| Honda et al., [10] 2017, Japan | 106 | 74,5 | 75/31 | SP142 | >5% | NR | NR | NR | 32 |
| Kawamura et al., 2019, Germany [18] | 29 | 76 | 18/11 | NR | >5% | NR | NR | NR | 22 |
| Gambichler et al., 2020, Germany [19] | 12 | 72 | 8/4 | ab205921 | NR | NR | NR | NR | 5 |
| Okabayshi et al., 2020, Japan [20] | 20 | NR | NR | E1L3N | >5% | NR | NR | NR | 8 |
| Bi et al., 2021, China [21] | 21 | 67 | 14/7 | 22C3 | >1, 1–5, 5–10, 10–50, >50 | 12 | 4 | 5 | 9 |
| Espejo-Freire et al., 2021, USA [22] | 11 | NR | NR | SP142 | >5% | NR | NR | NR | 1 |
| Googe et al., 2021, USA [23] | 10 | 73 | 5/5 | ZR3 | <1, 1–49, >50 | 0 | 3 | 7 | 10 |
| Tomassen et al., 2022, Netherlands [24] | 14 | NR | NR | E1L3N | <1, 1–10, 10–49, >50 | 2 | 11 | 1 | 12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobrano, R.; Paliogiannis, P.; Zinellu, A.; Palmieri, G.; Persico, I.; Mangoni, A.A.; Cossu, A. PD-L1 Expression in Cutaneous Angiosarcomas: A Systematic Review with Meta-Analysis. Curr. Oncol. 2023, 30, 5135-5144. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30050388
Lobrano R, Paliogiannis P, Zinellu A, Palmieri G, Persico I, Mangoni AA, Cossu A. PD-L1 Expression in Cutaneous Angiosarcomas: A Systematic Review with Meta-Analysis. Current Oncology. 2023; 30(5):5135-5144. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30050388
Chicago/Turabian StyleLobrano, Renato, Panagiotis Paliogiannis, Angelo Zinellu, Giuseppe Palmieri, Ivana Persico, Arduino A. Mangoni, and Antonio Cossu. 2023. "PD-L1 Expression in Cutaneous Angiosarcomas: A Systematic Review with Meta-Analysis" Current Oncology 30, no. 5: 5135-5144. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol30050388