Evaluation of Five International HBV Treatment Guidelines: Recommendation for Resource-Limited Developing Countries Based on the National Study in Nepal

 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Hepatitis B Virus (HBV) Infection
1.2. HBV Diagnosis
2. HBV Epidemiology in Nepal, Compared with Other Developing Countries
2.1. The First National HBV Viral Load Study in Nepal
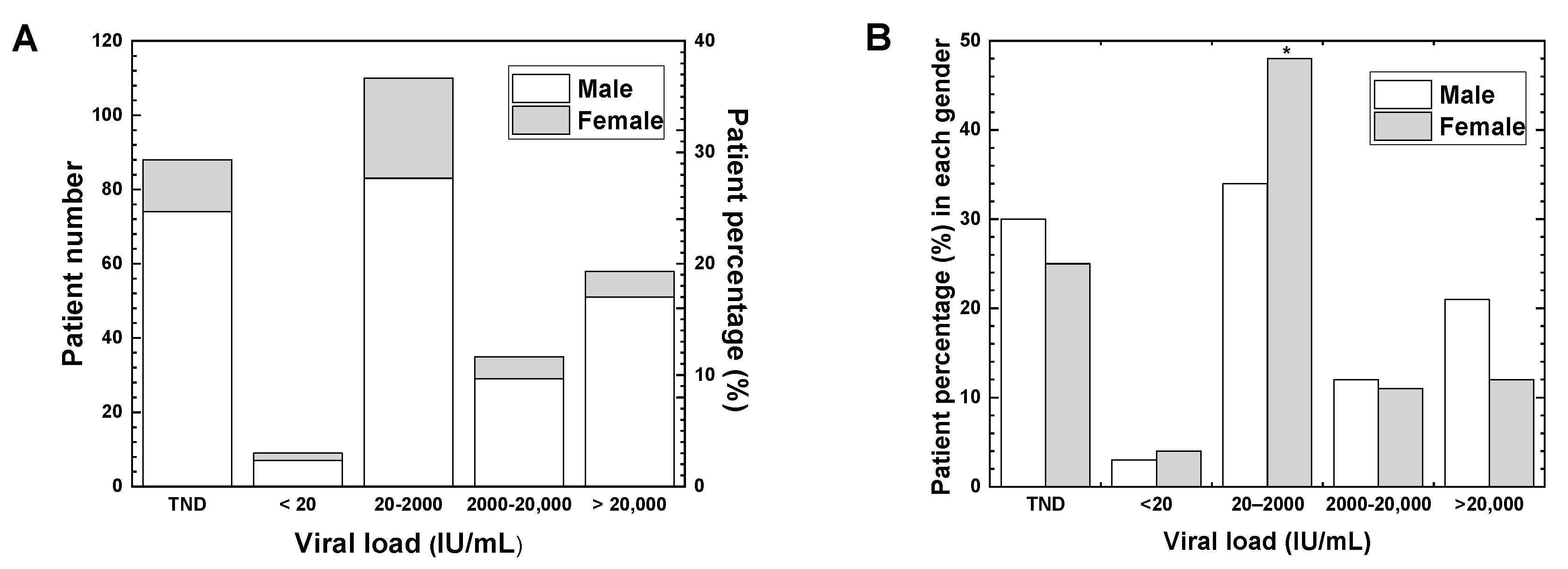
2.2. Viral Load
2.3. Gender
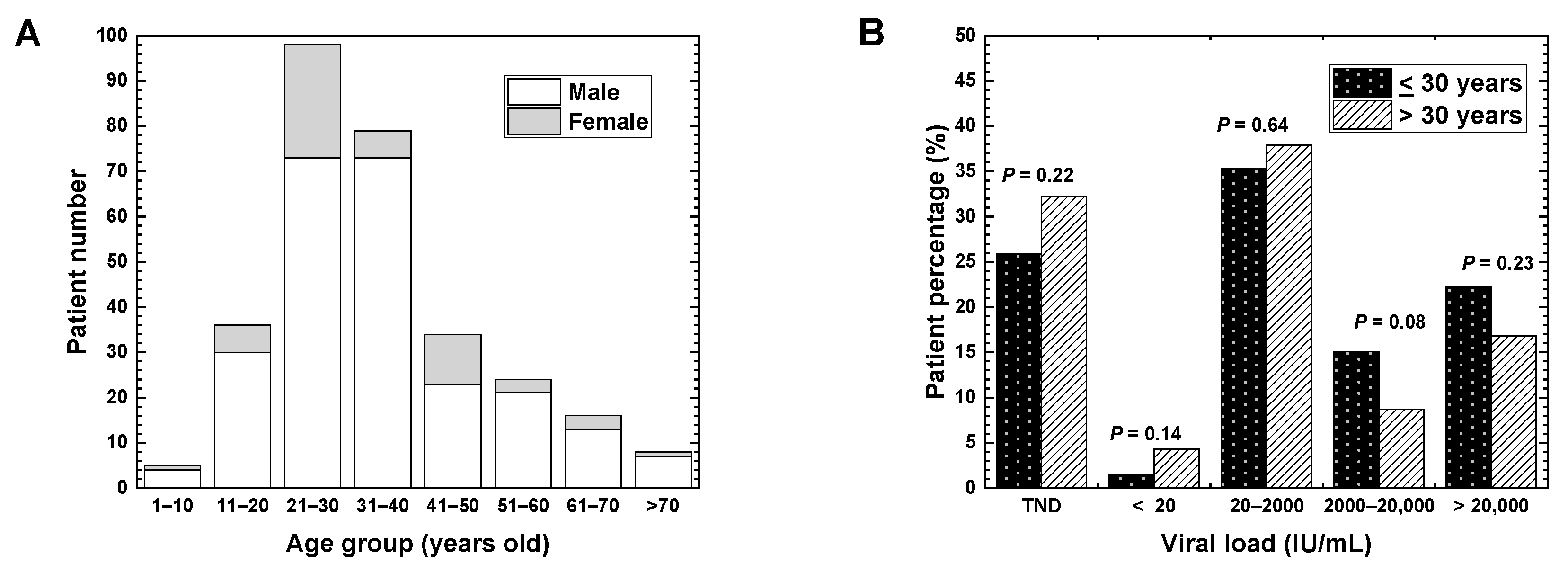
2.4. Age and Vaccination
2.5. Age and Viral Load
3. Five International HBV Treatment Guidelines
3.1. World Health Organization (WHO, 2015)
3.2. American Association for the Study of Liver Diseases (AASLD, 2018)
3.3. National Institute for Health and Care Excellence (NICE, 2013)
3.4. European Association for the Study of the Liver (EASL, 2017)
3.5. Asian Pacific Association for the Study of the Liver (APASL, 2015)
3.6. Treatment of HBV Infection Based on Five International Guidelines
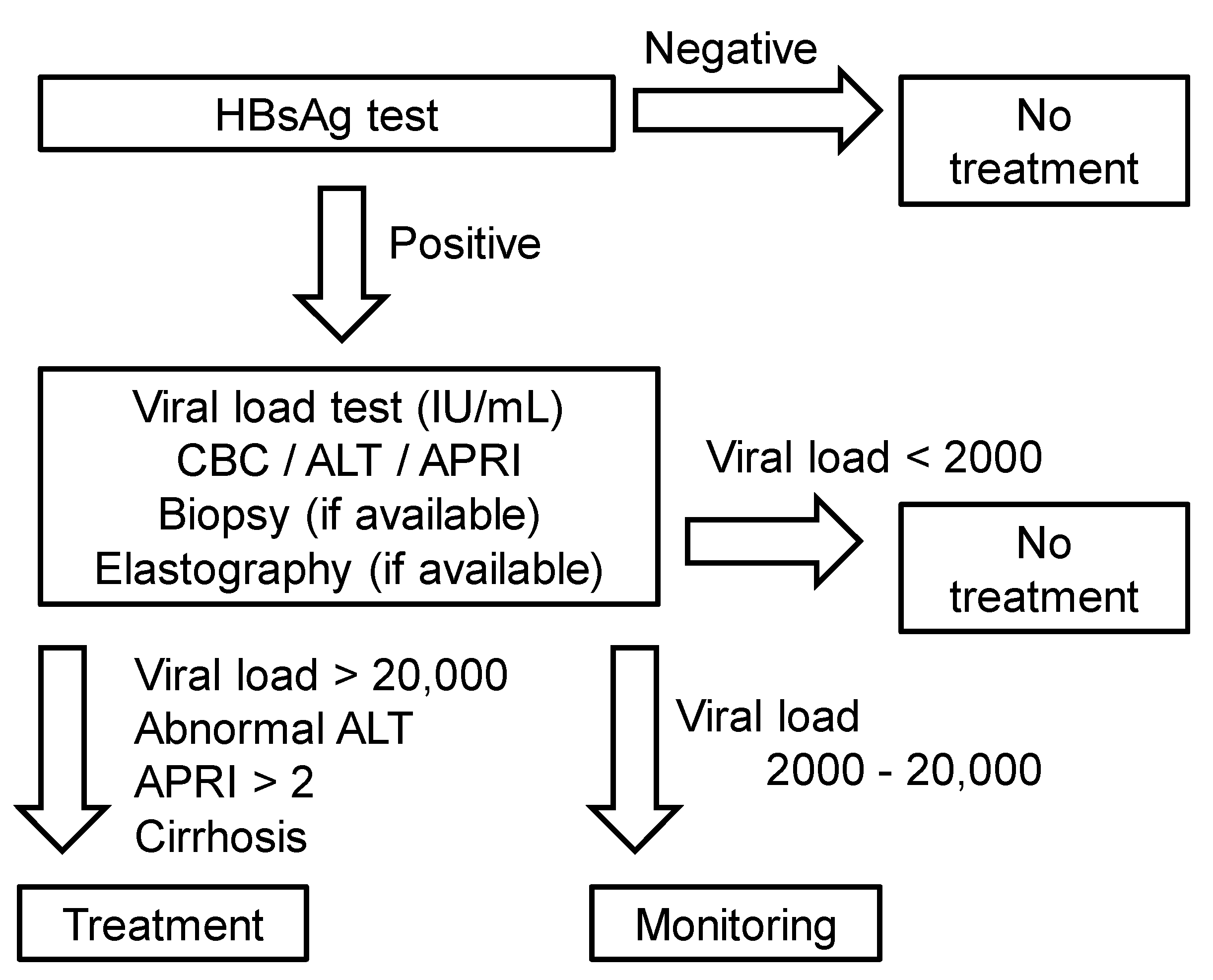
4. Guideline Proposal for Resource-Limited Developing Countries
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AASLD | American Association for the Study of Liver Diseases |
| ALT | Alanine aminotransferase |
| APASL | Asian Pacific Association for the Study of the Liver |
| APRI | Aspartate aminotransferase-to-platelet ratio index |
| EASL | European Association for the Study of the Liver |
| HBcAg | Hepatitis B core antigen |
| HBeAg | Hepatitis B envelope antigen |
| HBsAg | Hepatitis B surface antigen |
| HBV | Hepatitis B virus |
| NICE | National Institute for Health and Care Excellence |
| PCR | Polymerase chain reaction |
| TND | Target not detected |
| WHO | World Health Organization |
References
- William, F.; Nauschuetz, S.L.L. Clinical virology. In Textbook of Diagnostics Microbiology, 5th ed.; Connie, R., Mahon, D.C.L., Manuselis, G., Eds.; Elsevier: Missouri, MO, USA, 2015; pp. 688–726. [Google Scholar]
- O’Hara, G.A.; McNaughton, A.L.; Maponga, T.; Jooste, P.; Ocama, P.; Chilengi, R.; Mokaya, J.; Liyayi, M.I.; Wachira, T.; Gikungi, D.M.; et al. Hepatitis B virus infection as a neglected tropical disease. PLoS Negl. Trop. Dis. 2017, 11, e0005842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.Y.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global epidemiology of hepatitis B virus infection: New estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef] [Green Version]
- WHO. Guideline for the Prevention Care and Treatment of Persons with Chronic Hepatitis B Infection; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Krajden, M.; McNabb, G.; Petric, M. The laboratory diagnosis of hepatitis B virus. Can J. Infect Dis. Med. Microbiol. 2005, 16, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.M. Hepatitis B virus infection. N. Engl. J. Med. 1997, 337, 1733–1745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayoub, W.S.; Keeffe, E.B. Review article: Current antiviral therapy of chronic hepatitis B. Aliment. Pharmacol. Ther. 2011, 34, 1145–1158. [Google Scholar] [CrossRef]
- Bárcena Marugán, R.; García Garzón, S. DNA-guided hepatitis B treatment, viral load is essential, but not sufficient. World J. Gastroenterol. 2009, 15, 423–430. [Google Scholar] [CrossRef]
- Shrestha, A. Viral hepatitis in Nepal: Past, present, and future. Euroasian J. Hepatogastroenterol. 2016, 6, 59–61. [Google Scholar]
- Spradling, P.R.; Hu, D.J.; McMahon, B.J. Epidemiology and prevention. In Viral Hepatitis, 4th ed.; Thomas, H.C., Lok, A.S.F., Locarnini, S.A., Zuckerman, A.J., Eds.; John Wiley & Sons: Chichester, West Sussex, UK, 2014; pp. 81–95. [Google Scholar]
- Khadka, S.; Tsunoda, I.; Omura, S.; Sato, F.; Park, A.-M.; Fujita, M.; Sakiyama, N.; Nakamura, Y.; Katsuki, A.; Pandit, R.; et al. First national hepatitis B viral load testing in Nepal: Laboratory perspective for Nepalese national treatment guideline. In Proceedings of the 67th Annual Meeting of the Japanese Society for Virology, Tokyo, Japan, 29–31 October 2019. [Google Scholar]
- Naing, L.; Winn, T.; Rusli, B.N. Practical issues in calculating the sample size for prevalence studies. Arch. Orofacial. Sci. 2006, 1, 9–14. [Google Scholar]
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed. Bench. 2013, 6, 14–17. [Google Scholar]
- Iregbu, K.C.; Nwajiobi-Princewill, P.I. Viral load pattern among hepatitis B surface antigen-positive patients: Laboratory perspective and implications for therapy. Ann. Med. Health Sci. Res. 2016, 6, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerlich, W.H. Medical virology of hepatitis B: How it began and where we are now. Virol. J. 2013, 10, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, B.P.; Adhikari, A.; Chaudhary, S. Hepatitis viruses in Kathmandu, Nepal: Hospital-based study. BMC Res. Notes. 2018, 11, 627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, S.M.; Shrestha, S. Chronic hepatitis B in Nepal: An Asian country with low prevalence of HBV infection. Trop. Gastroenterol. 2012, 33, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Bhatta, B.; Thapa, R.; Pant, P.; Pandeya, D.R. A retrospective hospital based study in Kathmandu to assess the seroprevalence of hepatitis B virus. JMMIHS 2016, 2, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Amidu, N.; Alhassan, A.; Obirikorang, C.; Feglo, P.; Majeed, S.F.; Timmy-Donkoh, E.; Afful, D. Sero-prevalence of hepatitis B surface (HBsAg) antigen in three densely populated communities in Kumasi, Ghana. J. Med. Biomed. Sci. 2012, 1, 59–65. [Google Scholar]
- Wang, S.; Tao, Y.; Tao, Y.; Jiang, J.; Yan, L.; Wang, C.; Ding, Y.; Yu, J.; Zhao, D.; Chi, X.; et al. Epidemiological study of hepatitis B and hepatitis C infections in northeastern China and the beneficial effect of the vaccination strategy for hepatitis B: A cross-sectional study. BMC Public Health 2018, 18, 1088. [Google Scholar] [CrossRef]
- Khan, F.; Shams, S.; Qureshi, I.D.; Israr, M.; Khan, H.; Sarwar, M.T.; Ilyas, M. Hepatitis B virus infection among different sex and age groups in Pakistani Punjab. Virol. J. 2011, 8, 225. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, S.T.; Alter, M.J.; Williams, I.T.; Moyer, L.A.; Judson, F.N.; Mottram, K.; Fleenor, M.; Ryder, P.L.; Margolis, H.S. Incidence and risk factors for acute hepatitis B in the United States, 1982–1998, Implications for vaccination programs. J. Infect. Dis. 2002, 185, 713–719. [Google Scholar] [CrossRef]
- Kolou, M.; Katawa, G.; Salou, M.; Gozo-Akakpo, K.S.; Dossim, S.; Kwarteng, A.; Prince-David, M. High prevalence of hepatitis B virus infection in the age range of 20-39 years old individuals in Lome. Open Virol. J. 2017, 11, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Okwuraiwe, A.P.; Salu, O.B.; Onwuamah, C.K.; Amoo, O.S.; Odunukwe, N.N.; Audu, R.A. Experience with hepatitis B viral load testing in Nigeria. Afr. J. Clin. Exp. Microbiol. 2011, 12. [Google Scholar] [CrossRef] [Green Version]
- Carithers, R.L. Epidemiology of hepatitis B and hepatitis C. In Chronic Viral Hepatitis: Diagnosis and Therapeutics, 1st ed.; Koff, R.S., Wu, G.Y., Eds.; Humana Press: Totowa, NJ, USA, 2001; pp. 25–40. [Google Scholar]
- Butt, A.S.; Sharif, F. Viral hepatitis in Pakistan: Past, present, and future. Euroasian J. Hepatogastroenterol. 2016, 6, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Naveira, M.C.M.; Badal, K.; Dhakal, J.; Mayer, N.A.; Pokharel, B.; Del Prado, R.F. Seroprevalence of hepatitis B and C in Nepal: A systematic review (1973–2017). Hepatol. Med. Policy 2018, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.H.; Chan, H.L.; Chen, P.J.; Cheng, J.; Goenka, M.K.; Hou, J.; Lim, S.G.; Omata, M.; Piratvisuth, T.; Xie, Q.; et al. Chronic hepatitis B: Whom to treat and for how long? Propositions, challenges, and future directions. Hepatol. Int. 2010, 4, 386–395. [Google Scholar] [CrossRef] [Green Version]
- Vittal, A.; Ghany, M.G. WHO Guidelines for Prevention, Care and Treatment of Individuals Infected with HBV: A US Perspective. Clin. Liver Dis. 2019, 23, 417–432. [Google Scholar] [CrossRef]
- Huang, D.Q.; Lim, S.G.; Hepatitis, B. Who to treat? A critical review of international guidelines. Liver Int. 2020, 40, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Terrault, N.A.; Lok, A.S.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Health NIF EC. Hepatitis B (Chronic): Diagnosis and Management of Chronic Hepatitis B in Children, Young People, and Adults; National Institute for Health and Care Excellence: London, UK, 2013. [Google Scholar]
- Liver EAftSot. EASL 2017 Clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- National centre for AIDS and STD control, Nepal. National HIV Testing and Treatment Guidelines 2017; National centre for AIDS and STD control, Nepal: Kathmandu, Nepal, 2017.
- Masaki, N.; Shrestha, P.K.; Nishimura, S.; Ito, K.; Sugiyama, M.; Mizokami, M. Use of nucleoside analogs in patients with chronic hepatitis B in Nepal: A prospective cohort study in a single hospital. Hepatol. Res. 2015, 45, 1163–1169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Viral Load (IU/mL) | ALT Level | Age (Years) | Recommendation |
|---|---|---|---|
| >20,000 | Abnormal | >30 (in particular) | Treatment |
| Normal | ≤30 | Monitoring | |
| 2000–20,000 | Abnormal | >30 | Monitoring |
| <2000 | Normal | All | No treatment |
| Viral Load (IU/mL) | ALT Level | HBeAg | Recommendation |
|---|---|---|---|
| >20,000 | >2 × ULN | Positive | Treatment |
| Increased | Positive | Treatment (if age > 40 years) | |
| Normal | Positive | Monitoring | |
| 2000–20,000 | Increased | Both | Treatment (if age > 40 years) |
| <2000 | Normal | Negative | No treatment |
| Viral Load (IU/mL) | ALT Level | Age (Years) | Recommendation |
|---|---|---|---|
| >20,000 | Abnormal | All | Treatment |
| 2000–20,000 | Abnormal | >30 | Treatment |
| Abnormal | ≤30 | Treatment (if severe hepatitis or fibrosis) | |
| <2000 | Normal | All | No treatment |
| Viral Load (IU/mL) | ALT Level | Liver Biopsy | Recommendation |
|---|---|---|---|
| >20,000 | >2 × ULN | Not required | Treatment |
| Normal | Not required | Monitoring (if age < 30 years) | |
| 2000–20,000 | Increased | Active necrosis/liver inflammation | Treatment |
| <2000 | Normal | Not required | No treatment |
| Viral Load (IU/mL) | ALT Level | Liver Disease | Recommendation |
|---|---|---|---|
| >20,000 | >2 × ULN | Pre-cirrhotic chronic hepatitis | Treatment (if HBeAg-positive) |
| 2000–20,000 | Increased | Cirrhosis/inflammation | Treatment (if age > 35 years) |
| >2000 | >2 × ULN | Pre-cirrhotic chronic hepatitis | Treatment (if HBeAg negative) |
| <2000 | Normal | Compensated cirrhosis | Treatment |
| Normal | − | Monitoring |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khadka, S.; Pandit, R.; Dhital, S.; Baniya, J.B.; Tiwari, S.; Shrestha, B.; Pandit, S.; Sato, F.; Fujita, M.; Sharma, M.; et al. Evaluation of Five International HBV Treatment Guidelines: Recommendation for Resource-Limited Developing Countries Based on the National Study in Nepal. Pathophysiology 2020, 27, 3-13. https://0-doi-org.brum.beds.ac.uk/10.3390/pathophysiology27010002
Khadka S, Pandit R, Dhital S, Baniya JB, Tiwari S, Shrestha B, Pandit S, Sato F, Fujita M, Sharma M, et al. Evaluation of Five International HBV Treatment Guidelines: Recommendation for Resource-Limited Developing Countries Based on the National Study in Nepal. Pathophysiology. 2020; 27(1):3-13. https://0-doi-org.brum.beds.ac.uk/10.3390/pathophysiology27010002
Chicago/Turabian StyleKhadka, Sundar, Roshan Pandit, Subhash Dhital, Jagat Bahadur Baniya, Surendra Tiwari, Bimal Shrestha, Sanjeet Pandit, Fumitaka Sato, Mitsugu Fujita, Mukunda Sharma, and et al. 2020. "Evaluation of Five International HBV Treatment Guidelines: Recommendation for Resource-Limited Developing Countries Based on the National Study in Nepal" Pathophysiology 27, no. 1: 3-13. https://0-doi-org.brum.beds.ac.uk/10.3390/pathophysiology27010002