
The Role of Cholangioscopy and EUS in the Evaluation of Indeterminate Biliary Strictures


1
Institute of Digestive Disease, The Chinese University of Hong Kong, Hong Kong SAR, China
2
Department of Medicine and Therapeutics, Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong SAR, China
*
Author to whom correspondence should be addressed.
Gastroenterol. Insights 2022, 13(2), 192-205; https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent13020020
Submission received: 22 April 2022
/
Revised: 18 May 2022
/
Accepted: 20 May 2022
/
Published: 14 June 2022
(This article belongs to the Special Issue Diagnostic and Therapeutic Challenges in Pancreatobiliary Diseases)
Abstract
:Bile duct stenosis continues to present a diagnostic dilemma for clinicians. It is important to establish the benign or malignant nature of the stricture early in order to avoid any unnecessary delay in medical treatment or surgery. Tissue acquisition for histological diagnosis is particularly crucial when the initial diagnostic work up is inconclusive. The diagnostic yield from the conventional endoscopic retrograde cholangiopancreatography (ERCP) with brushing and biopsy is suboptimal. Patients with indeterminate biliary strictures (IDBSs) often require a multi-disciplinary diagnostic approach and additional endoscopic evaluation, including cholangioscopy and endoscopic ultrasound, before a final diagnosis can be reached. In this article, we discuss the recent endoscopic advancements in the diagnosis of biliary stricture with a focus on the roles of cholangioscopy and endoscopic ultrasound (EUS).
1. Introduction
Despite the significant advances in pancreaticobiliary cross-sectional imaging, cholangioscopy systems and endoscopic-ultrasound-guided fine-needle aspiration (EUS-FNA), differentiating between malignant and benign biliary strictures remains a clinical challenge. In clinical practice, indeterminate biliary stricture (IDBS) refers to strictures that have no obvious mass on cross sectional imaging and without a definitive tissue diagnosis. IDBS currently represents 20% of all biliary strictures after initial evaluation, including endoscopic retrograde cholangiopancreatography (ERCP) with standard sampling, such as brush cytology and transpapillary biopsy (TPB) and laboratory testing of tumor markers [1]. However, the diagnostic yield from conventional ERCP with brushing and TPB is often disappointing. A recent meta-analysis revealed the sensitivity and specificity of brush cytology for diagnosing malignant biliary strictures (MBSs) to be 45% and 99%, respectively, while the sensitivity and specificity of TPB were 48% and 99%, respectively. The diagnostic yield using a combination of both modalities was still suboptimal and only increased the sensitivity slightly to 59% [2]. The decision whether to conservatively manage a patient or proceed with high-risk surgical resection and oncological treatment relies heavily on the confirmation of cancer during cyto- or histopathological assessment. The low negative predictive value of conventional ERCP gives clinicians with very low confidence in assuming IDBS are benign in nature [3]. In fact, previous observation studies showed two-thirds of IDBS eventually turned out to be malignant, while one-fourth of all surgical resections were actually benign [4].
2. Clinical Presentation and Common Biomarkers
The clinical presentation of patients with biliary strictures can be broad and can range from an asymptomatic incidental finding to fulminant cholangitis with right upper quadrant pain, fever and jaundice. Clinical history and symptoms are only helpful to a certain extent in differentiating between benign and malignant strictures as symptoms, such as weight loss, fever, nausea vomiting and pruritis, can be present in both [5]. Carbohydrate antigen 19-9 (CA19-9) is the most common and validated biomarker used for cholangiocarcinoma (CCA) and pancreatic adenocarcinoma. At a cut-off of 37 U/mL, CA19-9 has a sensitivity of 77% and specificity of 87% for pancreatic cancer [6]. The main limitation of CA 19-9 in its use for CCA is that it can be elevated in non-malignant obstructive jaundice. Efforts to bypass this limitation include the use of a higher cut-off value of 300 U/mL in patient with cholangitis or cholestasis or by delaying the testing of CA19-9 after patients have recovered from their acute presentation [6]. Carcinoembryonic antigen (CEA) is another widely used biomarker in the diagnosis of CCA. It is raised in up to 30% of CCA patients and its diagnostic sensitivity and specificity range from 42% to 85% and 70% to 89%, respectively [7].
3. Etiology
Biliary strictures can be caused by lesions within the biliary lumen, arising from the mural layer of the bile duct itself, or from extra-biliary compression [4]. While a mass lesion involving the bile duct may be observed on imaging such as ultrasound, computed tomography (CT), or magnetic resonance imaging of the abdomen in patient presenting with obstructive jaundice, early malignancy of the bile duct may often present with a ductal stricture without an obvious mass on cross-sectional imaging [3]. The benign causes of biliary strictures include iatrogenic bile duct injury after cholecystectomy or liver transplantation and several inflammatory conditions most notably primary sclerosing cholangitis (PSC) and IgG4-related sclerosing cholangitis (IgG4-SC) (Table 1). In contrast to the variety of the benign etiology of biliary strictures, MBS are largely caused by CCA and pancreatic adenocarcinoma (Figure 1).
IgG4-SC is an inflammatory disorder of the biliary tract and has increasingly been recognized as a biliary manifestation of IgG4-related systemic disease or in association with autoimmune pancreatitis (Figure 2). It is characterized by the elevation of the IgG4 levels and the infiltration of IgG4-plasma cells in the bile duct wall [8,9]. Nevertheless, serum IgG4 is not elevated in up to 30% of IgG4 cholangiopathy cases and it can also be elevated in 10% of PSC patients [3].
PSC is an inflammatory disorder of the intra- and extrahepatic bile ducts leading to stricture formation. The diagnosis of PSC relies on the appearance of focal biliary strictures and dilatations on imaging after excluding the secondary causes of sclerosing cholangitis [10]. In PSC patients with a dominant stricture, additional endoscopic workup to rule out CCA is warranted because up to 13% of PSC patients will eventually develop CCA. Other malignant causes of biliary strictures, such as bile duct lymphoma or intraductal papillary neoplasm of the bile duct (IPNB), can also mimic CCA. Their oncological treatment options and prognosis can be quite different, and this highlights the importance of endoscopic tissue acquisition for the diagnosis of biliary stricture [11].
4. ERCP-Based Techniques
4.1. Cholangiogram Appearance, Brush Cytology and Transpapillary Biopsy
After successful biliary cannulation in ERCP, the performance of an adequate cholangiogram is the fundamental first step in the evaluation of a suspected biliary stricture. A malignant biliary stricture usually has an irregular appearance on cholangiogram, whereas a benign biliary stricture often has a smooth contour on cholangiogram [4]. However, the cholangiographic appearance alone may not allow reliable differentiation between malignant and benign biliary strictures. While tissue sampling is the preferred technique to confirm a malignant diagnosis, the suboptimal sensitivity of ERCP-guided brush cytology and TPB remains a major limitation [4,5]. The high number of false negatives from tissue sampling during ERCP can be attributable to procedural factors and histopathological interpretation [5]. Several techniques in tissue sampling have been shown to improve the diagnostic accuracy of ERCP-based tissue sampling. Balloon dilatation of the biliary stricture prior to forcep biopsy improved the sensitivity from 40% to 71% and was not associated with a higher complication rate [12]. In a pilot study, post-brushing biliary lavage fluid cytology by injecting 5–15 mL of saline into the bile duct after brushing improved the cumulative sensitivity by 24% [13].Fluorescence in situ hybridization (FISH) has been used to measure the DNA content of potential oncogenic genes on brush cytology samples for over a decade. Nevertheless, the sensitivity of FISH and cytology alone only appears to range from 31% to 59% [14,15]. A single center retrospective study by Nanda et al. showed a sensitivity of 82% when the combination of brush cytology, forcep biopsy and FISH are used [14]. However, the cost of FISH is at least 3–4 times more expensive than conventional cytology. In a study comparing ERCP with brushings for cytology, ERCP with brushings for cytology and FISH-trisomy, ERCP with brushings for cytology and FISH-polysomy, and ERCP with TPB and single operator cholangioscopy (SOC) with targeted biopsy for the diagnosis of CCA in PSC patients, Njei et al. reported that SOC with tissue sampling is actually the most cost-effective modality for this purpose [16].
4.2. Probe-Based Confocal Laser Endomicroscopy
Probe-based confocal laser endomicroscopy (pCLE) is a novel imaging technique that provides real-time ‘optical biopsies’ during ERCP. It uses a low power beam of laser transmitted through a miniprobe, and a distal lens sequentially scans the biliary epithelium to provide in vivo architectural information at the cellular level [17]. A recent meta-analysis showed that the overall sensitivity and specificity for diagnosing MBS was 90% and 75%, respectively [18]. Inflammatory changes on the biliary epithelium from prior stenting, brushing or biopsies could affect pCLE imaging and the suboptimal specificity is likely due to the false interpretation of these inflammatory changes in biliary strictures [11].
5. Cholangioscopy
5.1. Different Types of Peroral Cholangioscopy
There has been significant technological advancement in the past decade since cholangioscopy was first introduced in 1976 [19]. Traditional peroral cholangioscopy is called the ‘mother–baby system’; the dedicated videocholangioscope is used as the baby scope and inserted through the accessory channel of the duodenoscope. It provides excellent images with narrow band imaging (NBI) capability (Figure 3) and good maneuverability for comparatively easy bile duct insertion. However, the fragility of the scope and the requirement of two skilled endoscopists to operate the system has prompted the introduction of the single operator cholangioscopy (SOC) system. There are currently two types of SOC: duodenoscopy-assisted SOC (SpyGlass, Boston scientific, Natick, MA, USA) and peroral direct cholangioscopy (DC) using an ultraslim gastroscope. DC can also be coupled with NBI to allow the clear visualization of the tumor margin for targeted biopsies. Ultraslim gastroscopes are readily available in many endoscopy units and hence the cost is significantly lower compared to the disposable SpyGlass SOC. However, sphincterotomy or balloon sphincteroplasty are required prior to scope insertion and it can be technically challenging in patients with a narrow bile duct diameter and proximal biliary stricture without an anchoring device [11]. A higher technical success rate has been reported using carbon dioxide insufflation and an anchoring balloon to facilitate the deep advancement of the ultraslim gastroscope into the bile duct through the papilla [20]. Recently, a new multibending ultra-slim endoscope has become available and was shown to have a high technical success rate with a reduced procedure time compared with a conventional ultraslim endoscope in a randomized trial [21]. The SpyGlass SOC, on the other hand, provides better maneuverability with four-way deflected steering compared to DC [21]. The imaging quality of the first generation SpyGlass SOC is traditionally poor due to its fiberoptical probe system, but the most recent digital version of the SpyGlass SOC (D-SOC) (SpyGlass DS or DS II, Boston Scientific, Natick, MA, USA) has a much-improved resolution and a wider field of view, leading to improved visualization and targeted SOC-guided biopsy or lithotripsy [22,23].
5.2. Visual Impression
Representative D-SOC images of benign and malignant biliary strictures are shown in Figure 4 and Figure 5, respectively. A meta-analysis reported the overall pooled sensitivity and specificity of D-SOC in the visual interpretation of biliary malignancy was 94% and 95%, respectively [24]. Nevertheless, the retrospective nature of the included studies and the fact that endoscopists were not blinded to the result of previous investigations allow the potential of bias [25].
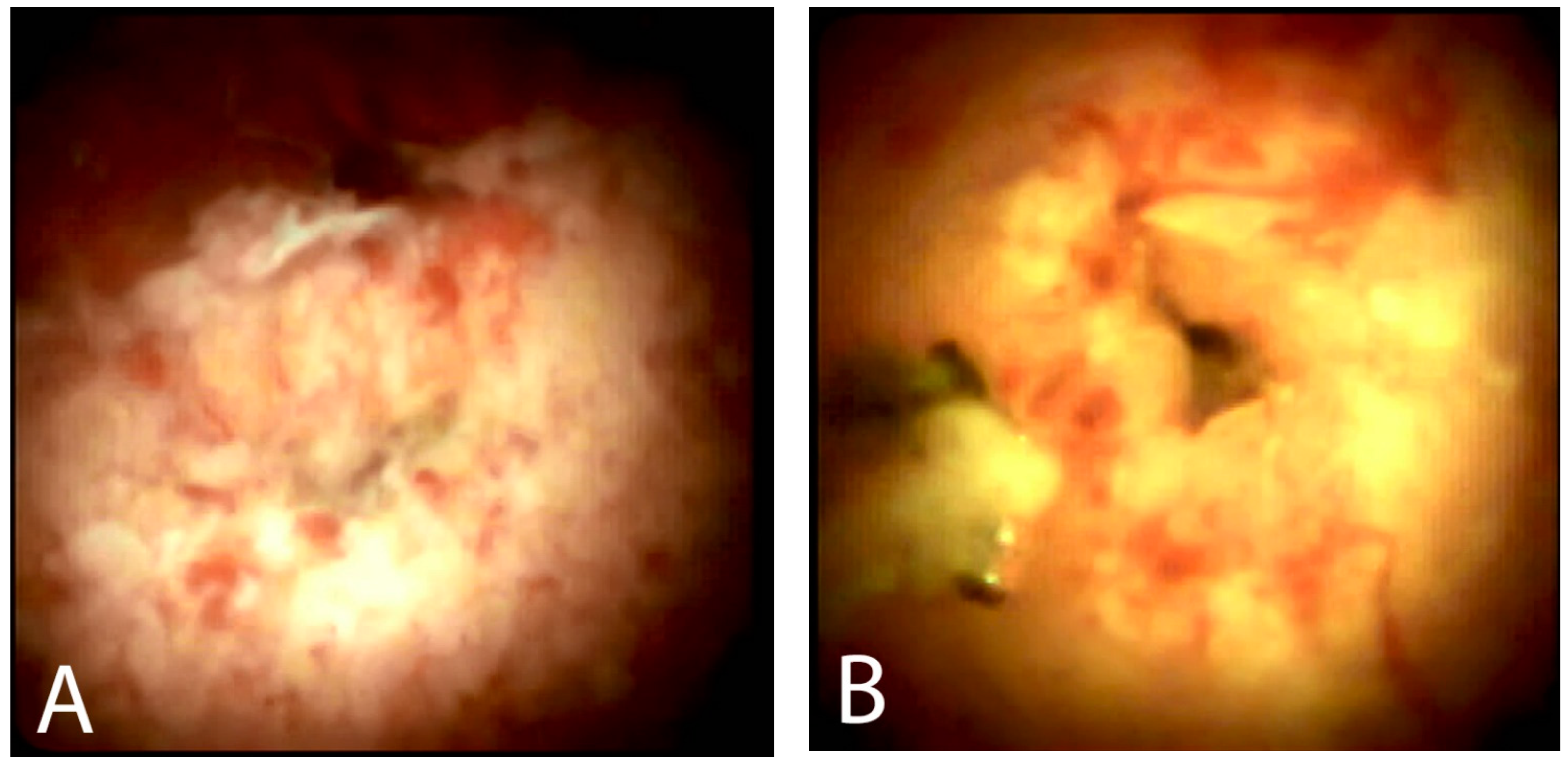
A recent prospective study enrolling 289 patients with IDBS showed that strictures were successfully visualized in 99% of patients, providing a visual diagnostic impression in 87% and obtaining adequate biopsies in 93%, while having a low complication rate of 1.7% [26]. This large, real-life prospective study has shown that D-SOC is an effective and safe intervention in guiding the management of patients with IDBS. However, these results should be interpreted with some caution as patients with PSC were not included in the study. A retrospective study including PSC patients (40% of the study population) showed the sensitivity and specificity for the D-SOC visual impression of IDBS were only 64% and 62%, respectively [27]. A recent study by Stassen et al., which also included PSC patients (25% of the study population), showed a sensitivity of 74% and specificity of 47% for the D-SOC video appraisal of IDBS when endoscopists were blinded to any clinical information. The study also showed considerable interobserver variation, despite all participating endoscopists being experts in the field with significant experience [25]. Although the D-SOC system allows for a significantly higher image resolution compared to the older generation of fibreoptic SOC (F-SOC), there is still a lack of consensus on what constitutes a malignant stricture and this might explain the high interobserver variability [5]. A new criteria-based system, the Mendoza Criteria, was developed recently to overcome this limitation. It included features that were previously shown to be statistically associated with malignancy: the presence of tortuous and dilated vessels, presence of irregular nodulations, presence of raised intraductal lesion, presence of irregular surface with or without ulcerations, and the presence of friability [28] (Figure 5). The overall diagnostic accuracy using this criteria method was 77%.
5.3. Cholangioscopy-Guided Biopsy
SOC-guided biopsy improves the diagnosis of IDBS particularly in patients with previous negative brushing and TPB. In a recent prospective randomized multicenter trial, the sensitivity of D-SOC-guided biopsy for diagnosing MBS was superior compared to conventional ERCP with standard sampling (68% vs. 21%) [23]. A meta-analysis (10 studies, 456 patients) showed that F-SOC guided biopsy had a pooled sensitivity, specificity and diagnostic odds ratio of 60%, 98% and 66 [29]. The D-SOC system allows more precise tissue sampling with improved diagnostic accuracy. In another recent meta-analysis, Wen et al. (11 studies, 356 patients) showed the pooled sensitivity, specificity and diagnostic odd ratio of D-SOC-guided biopsy to be 74%, 98% and 65%, respectively [30]. Increasing the number of biopsies taken and using a larger forceps should theoretically improve the diagnostic yield, but the optimal number of biopsies remains unclear. The mean number of biopsies performed in these studies ranged from 2 to 5 [10]. Furthermore, a recent prospective randomized trial showed no significant difference in diagnostic accuracy using the rapid on-site evaluation (ROSE) of the biopsy specimen in patients with IDBS. However, a greater number of biopsies was required to obtain a final diagnosis in the offsite cohort [31]. Adverse event rates of D-SOC were reported to be low in multiple studies, with a pooled adverse event rate of 7% in a recent meta-analysis [23,26,30,32]. On the other hand, the adverse event rate for DC was reported to be as high as 12% with air embolism being a major concern [33]. SOC-guided biopsy was shown in a cost utility analysis to be the most cost-effective diagnostic modality for CCA in PSC patients compared to conventional ERCP [16]. A cost–benefit analysis also showed that the use of D-SOC reduced the number of procedures performed by 31% and cost by 5% when compared to conventional ERCP [34]. Despite the potential benefits and cost-effectiveness, cholangioscopy is often regarded as a second-line investigation for IDBS in most endoscopy units due to cost constraints and availability.
6. Endoscopic Ultrasound
6.1. Intraductal Ultrasonography
Intraductal ultrasonography (IDUS) is performed by using a high-frequency (12–30 MHz) ultrasonic probe that can be placed in close proximity to the pancreatobiliary ductal system during ERCP. It allows real-time cross-sectional imaging of the bile duct and the surrounding structures. The sonographic features that are suggestive of malignancy include hypoechoic sessile mass, tumor size greater than 10 mm and interrupted bile duct wall echo layers [34,35]. A large retrospective study by Meister et al. showed that IDUS is highly accurate in distinguishing between benign and MBS with a sensitivity, specificity and accuracy of 93%, 90% and 91%, respectively [36]. A large retrospective study involving 234 patients with IDBS showed the superiority of IDUS in diagnostic accuracy for MBS compared to other modalities: IDUS (91%), TPB (59%) and EUS (74%) [37]. A study involving 72 patients with suspected ampullary tumor showed that IDUS has a superior diagnostic accuracy over TPB alone and can accurately stage and predict cases that can be treated endoscopically [38]. The European Society of Gastrointestinal Endoscopy suggests that a combination of IDUS and biopsies might have a role in the evaluation of ampullary tumors [17]. However, despite the strengths of IDUS, several limitations exist: (1) the tendency for under-staging of pancreatobiliary tract tumors and suboptimal staging for locoregional lymph nodes due to the limited penetration depth [37], (2) decreased diagnostic yield due to acoustic interference from previously placed biliary stents and (3) most importantly the inability to obtain a histological sample [39].
6.2. Endoscopic Ultrasound
EUS allows high resolution imaging of the pancreas parenchyma, extrahepatic bile duct and regional lymphadenopathy as well as tissue acquisition capability by FNA in the same session. The sonographic features associated with malignancy in IDBS include a pancreatic head mass and a bile duct wall thickness of >3 mm [40]. On EUS, the innermost hyperechoic layer (IHL) corresponds to the mucosal layer of the bile duct. When bile duct wall thickening is observed on EUS, efforts should be made to assess whether the IHL is preserved since cholangiocarcinoma originates from the bile duct mucosa and leads to the loss of the IHL plane. Figure 6 shows a small hypoechoic mass in the distal common bile duct (CBD) traversed by a biliary stent, which was not clearly observed in CT abdomen previously. The mass was hypoenhanced with the highlight of fine tumor vessels on contrast-enhanced EUS (CE-EUS), suggestive of CCA. A meta-analysis showed that EUS alone without FNA has a sensitivity of 78% and specificity of 84% for detecting MBS [41]. EUS-FNA has an added advantage over ERCP as it can potentially obtain a histological sample from an extraductal lesion that is not reachable with ERCP. It allows the more precise locoregional staging of the tumor, which is particularly important in guiding treatment choices in patients with CCA as the presence of malignant regional lymph nodes (RLN) often precludes curative surgical resection or liver transplantation. EUS +/− FNA was more sensitive in identifying RLN in CCA patients when compared to cross-sectional imaging (86% vs. 47%) [42]. In patients with suspected biliary strictures and failed biliary cannulation in ERCP, EUS can provide additional diagnostic information and allow rescue for biliary access by EUS rendezvous technique to facilitate the completion of ERCP [43].
6.3. Tissue Is the Real Issue
EUS-FNA is superior to conventional ERCP with brush cytology and TPB for diagnosing MBS. A recent meta-analysis showed that EUS-FNA has a higher sensitivity (75% vs. 49%) and accuracy (79% vs. 61%) compared to conventional ERCP. However, it is important to emphasize that a negative result with both techniques cannot completely exclude malignancy as both have a very low negative predictive value (47% vs. 34%) [44]. The diagnostic sensitivity of EUS-FNA is higher in a distal biliary lesion compared to a proximal lesion. This is likely due to the distal CBD being in close proximity to the duodenal wall and can be easily visualized and assessed with EUS. Furthermore, the majority of the distal lesion is caused by extrinsic compression, such as pancreatic malignancy and lymphadenopathy. EUS-FNA has a sensitivity of 76% in proximal biliary strictures compared to a sensitivity of 83% in distal stricture [45]. In a meta-analysis of 33 studies, EUS-FNA was shown to be highly accurate for the diagnosis of solid pancreatic neoplasm with a pooled sensitivity of 85% and pooled specificity of 98% [46]. When compared to conventional EUS b-mode imaging and contrast-enhanced multidetector CT, CE-EUS was shown to improve the detection of small pancreatic lesions. In a prospective study of 277 patients with pancreatic solid lesions, Kitano et al. demonstrated that CE-EUS was superior to contrast-enhanced multidetector CT in detecting small (≤2 cm) carcinoma [47]. A combination of CE-EUS and EUS-FNA increased the overall sensitivity in diagnosing pancreatic neoplasm from 92% to 100% compared to EUS-FNA alone [47]. In recent years, multiple fine-needle biopsy (FNB) needles with specialized tip designs have become available, allowing the procurement of tissue cores for histological examination [48]. A recent multicenter randomized study involving 608 patients with solid lesions demonstrated that EUS-FNB had a considerably higher histologic yield (77% vs. 44%) and diagnostic accuracy (87% vs. 78%) compared to EUS-FNA [49]. In a recent meta-analysis of 18 randomized studies comparing EUS-FNB with EUS-FNA, EUS-FNB outperformed EUS-FNA with a higher accuracy, tissue core rate and allowed diagnosis with fewer passes in both pancreatic and non-pancreatic lesions [50]. Despite the benefits of EUS-FNA/FNB, the possibility of needle tract seeding of malignant cells after EUS-FNA/FNB remains a concern in potentially operable proximal and hilar biliary malignancies. In a retrospective study of 191 hilar CCA for pre-liver transplantation laparoscopic staging, 16 pre-operative FNA were performed (3 EUS and 13 percutaneous) and 5 out of 6 (83%) patients with a positive FNA cytology for adenocarcinoma developed peritoneal metastasis [51]. In contrast, another retrospective study involving 150 CCA patients treated primarily by surgical resection with or without adjuvant chemotherapy found that pre-operative EUS-FNA did not adversely affect patients’ overall or progression-free survival [52]. Current data on the incidence and outcome of tumor seeding after the EUS-FNA of biliary malignancy is limited and conflicting. Nonetheless, given the potential detrimental risk of tumor seeding, most transplantation programs consider pre-operative EUS-FNA a contraindication to liver transplantation [3].
7. Same-Session EUS and ERCP
There are several advantages of performing EUS-FNA and conventional ERCP during the same session. This approach helps to streamline the diagnostic workup and may better triage the need for ERCP in patients with suspected biliary obstruction [53]. In a study of 418 patients with unexplained biliary obstruction, Zaheer et al. demonstrated that same-session EUS and ERCP were safe and effective and the diagnostic accuracy of EUS was 90% for malignant strictures and 92% for benign strictures [53]. In a multicenter retrospective study of 263 patients with suspected MBS who underwent same-session EUS and ERCP, the overall diagnostic sensitivity and accuracy of the EUS/ERCP combination were 85.8% and 87.1%, respectively [54]. Of note, while the sensitivity and accuracy of EUS/ERCP combination were found to be higher than those of EUS-FNA for both pancreatic and biliary lesions, there were no significant differences between the ERCP/EUS combination and EUS-FNA in patients with a large mass (≥4 cm). The superiority of same-session EUS-FNA- and ERCP-based tissue sampling when compared to either method alone was further demonstrated in a recent meta-analysis [55].
8. Biliary-Stricture-Location-Based Approach
The location of biliary strictures may affect the diagnostic efficacy of cholangioscopy and EUS for IDBS. Despite the recent improvement in the design of the SOC scopes, maintaining a stable cholangioscope position to perform adequate biopsies in tight distal CBD strictures can still be technically challenging. Proximal perihilar strictures, on the other hand, can be difficult to be visualized and biopsied with EUS as the location is closer to the liver and further away from the duodenal wall. Because there is currently no randomized controlled clinical trial data available directly comparing SOC-guided biopsy and EUS-FNA in the setting of IDBS, an approach of using SOC-guided biopsy or EUS-FNA according to the stricture location can be helpful in the endoscopic workup of IDBS after inconclusive ERCP-based tissue sampling (Figure 7). With this approach, the accuracy for diagnosing MBS using SOC-guided biopsy for proximal strictures and EUS-FNA/FNB for distal biliary strictures was 93.6% and 96.3%, respectively, in a study of 181 patients with suspected MBS [56].
9. Conclusions
The evaluation of IDBS remains a complex and challenging task despite the advancement of new technologies over the past two decades. A multidisciplinary approach is necessary in order to choose the right diagnostic modality and to achieve early diagnosis. While both cholangioscopy and EUS are reasonable next steps in workup after inconclusive ERCP-guided tissue sampling, each modality has its own strengths and weaknesses. Apart from procedure cost consideration, the selection of cholangioscopy and EUS is best guided by the stricture location and availability of local expertise.
Author Contributions
Conceptualization, W.S. and R.S.Y.T.; methodology, W.S. and R.S.Y.T.; resources, R.S.Y.T.; writing—original draft preparation, W.S.; writing—review and editing, R.S.Y.T. and W.S.; visualization, W.S.; supervision, R.S.Y.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this publication because this is not a clinical study, but a review paper of a topic that does not include any new human research data by the authors.
Informed Consent Statement
Permission for the use of endoscopic and radiologic images for publication was obtained from patients.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviation
| ERCP | endoscopic retrograde cholangiopancreatography |
| IDBS | indeterminate biliary stricture |
| EUS | endoscopic ultrasound |
| EUS-FNA | endoscopic-ultrasound-guided fine-needle aspiration |
| TPB | trans-papillary biopsy |
| MBS | malignant biliary stricture |
| CA19-9 | carbohydrate antigen 19-9 |
| CCA | cholangiocarcinoma |
| CEA | carcinoembryonic antigen |
| CT | computed tomography |
| PSC | primary sclerosing cholangitis |
| IgG4-SC | IgG4-related sclerosing cholangitis |
| IPNB | intraductal papillary neoplasm of the bile duct |
| FISH | fluorescence in situ hybridization |
| SOC | single-operator cholangioscopy |
| pCLE | probe-based confocal laser endomicroscopy |
| NBI | narrow band imaging |
| DC | direct cholangioscopy |
| D-SOC | digital-single-operator cholangioscopy |
| F-SOC | fibreoptic-single-operator cholangioscopy |
| ROSE | rapid on-site evaluation |
| IDUS | intraductal ultrasonography |
| CBD | common bile duct |
| CE-EUS | contrast-enhanced endoscopic ultrasound |
| RLN | regional lymph nodes |
| FNB | fine-needle biopsy |
References
- Martinez, N.S.; Trindade, A.J.; Sejpal, D.V. Determining the Indeterminate Biliary Stricture: Cholangioscopy and Beyond. Curr. Gastroenterol. Rep. 2020, 22, 58. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, U.; Njei, B.; Lourdusamy, V.; Konjeti, R.; Vargo, J.J.; Parsi, M.A. Comparative effectiveness of biliary brush cytology and intraductal biopsy for detection of malignant biliary strictures: A systematic review and meta-analysis. Gastrointest. Endosc. 2015, 81, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowlus, C.L.; Olson, K.A.; Gershwin, M.E. Evaluation of indeterminate biliary strictures. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Novikov, A.; Kowalski, T.E.; Loren, D.E. Practical Management of Indeterminate Biliary Strictures. Gastrointest. Endosc. Clin. N. Am. 2019, 29, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio Blanco, G.; Mossa, M.; Troncone, E.; Argirò, R.; Anderloni, A.; Repici, A.; Paoluzi, O.A.; Monteleone, G. Tips and tricks for the diagnosis and management of biliary stenosis-state of the art review. World J. Gastrointest. Endosc. 2021, 13, 473–490. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, M.H.; Myung, S.J.; Lim, B.C.; Park, E.T.; Yoo, K.S.; Seo, D.W.; Lee, S.K.; Min, Y.I. A new strategy for the application of CA19-9 in the differentiation of pancreaticobiliary cancer: Analysis using a receiver operating characteristic curve. Am. J. Gastroenterol. 1999, 94, 1941–1946. [Google Scholar] [CrossRef]
- Macias, R.I.R.; Kornek, M.; Rodrigues, P.M.; Paiva, N.A.; Castro, R.E.; Urban, S.; Pereira, S.P.; Cadamuro, M.; Rupp, C.; Loosen, S.H.; et al. Diagnostic and prognostic biomarkers in cholangiocarcinoma. Liver Int. 2019, 39 (Suppl. 1), 108–122. [Google Scholar] [CrossRef] [Green Version]
- Kamisawa, T.; Nakazawa, T.; Tazuma, S.; Zen, Y.; Tanaka, A.; Ohara, H.; Muraki, T.; Inui, K.; Inoue, D.; Nishino, T.; et al. Clinical practice guidelines for IgG4-related sclerosing cholangitis. J. Hepatobiliary Pancreat. Sci. 2019, 26, 9–42. [Google Scholar] [CrossRef] [Green Version]
- Nour, E.; Hammami, A.; Missaoui, N.; Bdioui, A.; Dahmani, W.; Ben Ameur, W.; Braham, A.; Ajmi, S.; Ben Slama, A.; Ksiaa, M.; et al. Multi-Organ Involvement of Immunoglobulin G4-Related Disease. Gastroenterol. Insights 2021, 12, 350–357. [Google Scholar] [CrossRef]
- Gupta, A.; Bowlus, C.L. Primary sclerosing cholangitis: Etiopathogenesis and clinical management. Front. Biosci. 2012, 4, 1683–1705. [Google Scholar] [CrossRef]
- Sun, B.; Moon, J.H.; Cai, Q.; Rerknimitr, R.; Ma, S.; Lakhtakia, S.; Ryozawa, S.; Kutsumi, H.; Yasuda, I.; Shiomi, H.; et al. Review article: Asia-Pacific consensus recommendations on endoscopic tissue acquisition for biliary strictures. Aliment. Pharmacol. Ther. 2018, 48, 138–151. [Google Scholar] [CrossRef] [PubMed]
- Porner, D.; Kaczmarek, D.J.; Heling, D.; Hausen, A.; Mohr, R.; Huneburg, R.; Matthaei, H.; Glowka, T.R.; Manekeller, S.; Fischer, H.P.; et al. Transpapillary tissue sampling of biliary strictures: Balloon dilatation prior to forceps biopsy improves sensitivity and accuracy. Sci. Rep. 2020, 10, 17423. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, S.; Matsubayashi, H.; Kimura, H.; Sasaki, K.; Nagata, K.; Ohno, S.; Uesaka, K.; Mori, K.; Imai, K.; Hotta, K.; et al. Diagnosis of bile duct cancer by bile cytology: Usefulness of post-brushing biliary lavage fluid. Endosc. Int. Open 2015, 3, E323–E328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, A.; Brown, J.M.; Berger, S.H.; Lewis, M.M.; Barr Fritcher, E.G.; Gores, G.J.; Keilin, S.A.; Woods, K.E.; Cai, Q.; Willingham, F.F. Triple modality testing by endoscopic retrograde cholangiopancreatography for the diagnosis of cholangiocarcinoma. Ther. Adv. Gastroenterol. 2015, 8, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Liew, Z.H.; Loh, T.J.; Lim, T.K.H.; Lim, T.H.; Khor, C.J.L.; Mesenas, S.J.; Kong, C.S.C.; Ong, W.C.; Tan, D.M.Y. Role of fluorescence in situ hybridization in diagnosing cholangiocarcinoma in indeterminate biliary strictures. J. Gastroenterol. Hepatol. 2018, 33, 315–319. [Google Scholar] [CrossRef]
- Njei, B.; McCarty, T.R.; Varadarajulu, S.; Navaneethan, U. Cost utility of ERCP-based modalities for the diagnosis of cholangiocarcinoma in primary sclerosing cholangitis. Gastrointest. Endosc. 2017, 85, 773–781.e710. [Google Scholar] [CrossRef]
- Tringali, A.; Lemmers, A.; Meves, V.; Terheggen, G.; Pohl, J.; Manfredi, G.; Häfner, M.; Costamagna, G.; Devière, J.; Neuhaus, H.; et al. Intraductal biliopancreatic imaging: European Society of Gastrointestinal Endoscopy (ESGE) technology review. Endoscopy 2015, 47, 739–753. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Lu, Y.; Sun, B.; Zhang, W.M.; Zhang, Z.Z.; He, Y.P.; Yang, X.J. Probe-based confocal laser endomicroscopy for the diagnosis of undetermined biliary stenoses: A meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 666–673. [Google Scholar] [CrossRef]
- Turowski, F.; Hügle, U.; Dormann, A.; Bechtler, M.; Jakobs, R.; Gottschalk, U.; Nötzel, E.; Hartmann, D.; Lorenz, A.; Kolligs, F.; et al. Diagnostic and therapeutic single-operator cholangiopancreatoscopy with SpyGlassDS™: Results of a multicenter retrospective cohort study. Surg. Endosc. 2018, 32, 3981–3988. [Google Scholar] [CrossRef]
- Farnik, H.; Weigt, J.; Malfertheiner, P.; Grutzmann, A.; Gossner, L.; Friedrich-Rust, M.; Zeuzem, S.; Sarrazin, C.; Albert, J.G. A multicenter study on the role of direct retrograde cholangioscopy in patients with inconclusive endoscopic retrograde cholangiography. Endoscopy 2014, 46, 16–21. [Google Scholar] [CrossRef]
- Lee, Y.N.; Moon, J.H.; Lee, T.H.; Choi, H.J.; Itoi, T.; Beyna, T.; Neuhaus, H. Prospective randomized trial of a new multibending versus conventional ultra-slim endoscope for peroral cholangioscopy without device or endoscope assistance (with video). Gastrointest. Endosc. 2020, 91, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Itoi, T.; Okabe, Y. Types of Peroral Cholangioscopy: How to Choose the Most Suitable Type of Cholangioscopy. Curr. Treat. Options Gastroenterol. 2016, 14, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Gerges, C.; Beyna, T.; Tang, R.S.Y.; Bahin, F.; Lau, J.Y.W.; van Geenen, E.; Neuhaus, H.; Nageshwar Reddy, D.; Ramchandani, M. Digital single-operator peroral cholangioscopy-guided biopsy sampling versus ERCP-guided brushing for indeterminate biliary strictures: A prospective, randomized, multicenter trial (with video). Gastrointest. Endosc. 2020, 91, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, P.; de Moura, D.T.H.; Ribeiro, I.B.; Bazarbashi, A.N.; Franzini, T.A.P.; Dos Santos, M.E.L.; Bernardo, W.M.; de Moura, E.G.H. Efficacy of digital single-operator cholangioscopy in the visual interpretation of indeterminate biliary strictures: A systematic review and meta-analysis. Surg. Endosc. 2020, 34, 3321–3329. [Google Scholar] [CrossRef] [PubMed]
- Stassen, P.M.C.; Goodchild, G.; de Jonge, P.J.F.; Erler, N.S.; Anderloni, A.; Cennamo, V.; Church, N.I.; Fernandez-Urien Sainz, I.; Huggett, M.T.; James, M.W.; et al. Diagnostic accuracy and interobserver agreement of digital single-operator cholangioscopy for indeterminate biliary strictures. Gastrointest. Endosc. 2021, 94, 1059–1068. [Google Scholar] [CrossRef]
- Almadi, M.A.; Itoi, T.; Moon, J.H.; Goenka, M.K.; Seo, D.W.; Rerknimitr, R.; Lau, J.Y.; Maydeo, A.P.; Lee, J.K.; Nguyen, N.Q.; et al. Using single-operator cholangioscopy for endoscopic evaluation of indeterminate biliary strictures: Results from a large multinational registry. Endoscopy 2020, 52, 574–582. [Google Scholar] [CrossRef]
- de Vries, A.B.; van der Heide, F.; Ter Steege, R.W.F.; Koornstra, J.J.; Buddingh, K.T.; Gouw, A.S.H.; Weersma, R.K. Limited diagnostic accuracy and clinical impact of single-operator peroral cholangioscopy for indeterminate biliary strictures. Endoscopy 2020, 52, 107–114. [Google Scholar] [CrossRef]
- Kahaleh, M.; Gaidhane, M.; Shahid, H.M.; Tyberg, A.; Sarkar, A.; Ardengh, J.C.; Kedia, P.; Andalib, I.; Gress, F.; Sethi, A.; et al. Digital single-operator cholangioscopy interobserver study using a new classification: The Mendoza Classification (with video). Gastrointest. Endosc. 2022, 95, 319–326. [Google Scholar] [CrossRef]
- Navaneethan, U.; Hasan, M.K.; Lourdusamy, V.; Njei, B.; Varadarajulu, S.; Hawes, R.H. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: A systematic review. Gastrointest. Endosc. 2015, 82, 608–614.e602. [Google Scholar] [CrossRef] [Green Version]
- Wen, L.J.; Chen, J.H.; Xu, H.J.; Yu, Q.; Liu, K. Efficacy and Safety of Digital Single-Operator Cholangioscopy in the Diagnosis of Indeterminate Biliary Strictures by Targeted Biopsies: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 666. [Google Scholar] [CrossRef]
- Bang, J.Y.; Navaneethan, U.; Hasan, M.; Sutton, B.; Hawes, R.; Varadarajulu, S. Optimizing Outcomes of Single-Operator Cholangioscopy-Guided Biopsies Based on a Randomized Trial. Clin. Gastroenterol. Hepatol. 2020, 18, 441–448.e441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navaneethan, U.; Hasan, M.K.; Kommaraju, K.; Zhu, X.; Hebert-Magee, S.; Hawes, R.H.; Vargo, J.J.; Varadarajulu, S.; Parsi, M.A. Digital, single-operator cholangiopancreatoscopy in the diagnosis and management of pancreatobiliary disorders: A multicenter clinical experience (with video). Gastrointest. Endosc. 2016, 84, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Meves, V.; Ell, C.; Pohl, J. Efficacy and safety of direct transnasal cholangioscopy with standard ultraslim endoscopes: Results of a large cohort study. Gastrointest. Endosc. 2014, 79, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Deprez, P.H.; Garces Duran, R.; Moreels, T.; Furneri, G.; Demma, F.; Verbeke, L.; Van der Merwe, S.W.; Laleman, W. The economic impact of using single-operator cholangioscopy for the treatment of difficult bile duct stones and diagnosis of indeterminate bile duct strictures. Endoscopy 2018, 50, 109–118. [Google Scholar] [CrossRef]
- Sun, B.; Hu, B. The role of intraductal ultrasonography in pancreatobiliary diseases. Endosc. Ultrasound 2016, 5, 291–299. [Google Scholar] [CrossRef]
- Meister, T.; Heinzow, H.S.; Woestmeyer, C.; Lenz, P.; Menzel, J.; Kucharzik, T.; Domschke, W.; Domagk, D. Intraductal ultrasound substantiates diagnostics of bile duct strictures of uncertain etiology. World J. Gastroenterol. 2013, 19, 874–881. [Google Scholar] [CrossRef]
- Heinzow, H.S.; Kammerer, S.; Rammes, C.; Wessling, J.; Domagk, D.; Meister, T. Comparative analysis of ERCP, IDUS, EUS and CT in predicting malignant bile duct strictures. World J. Gastroenterol. 2014, 20, 10495–10503. [Google Scholar] [CrossRef]
- Heinzow, H.S.; Lenz, P.; Lallier, S.; Lenze, F.; Domagk, D.; Domschke, W.; Meister, T. Ampulla of Vater tumors: Impact of intraductal ultrasound and transpapillary endoscopic biopsies on diagnostic accuracy and therapy. Acta Gastroenterol. Belg. 2011, 74, 509–515. [Google Scholar]
- Cha, S.-W. Recent advances of diagnostic approaches for indeterminate biliary tract obstruction. Int. J. Gastrointest. Interv. 2021, 10, 114–119. [Google Scholar] [CrossRef]
- Lee, J.H.; Salem, R.; Aslanian, H.; Chacho, M.; Topazian, M. Endoscopic ultrasound and fine-needle aspiration of unexplained bile duct strictures. Am. J. Gastroenterol. 2004, 99, 1069–1073. [Google Scholar] [CrossRef]
- Garrow, D.; Miller, S.; Sinha, D.; Conway, J.; Hoffman, B.J.; Hawes, R.H.; Romagnuolo, J. Endoscopic ultrasound: A meta-analysis of test performance in suspected biliary obstruction. Clin. Gastroenterol. Hepatol. 2007, 5, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Malikowski, T.; Levy, M.J.; Gleeson, F.C.; Storm, A.C.; Vargas, E.J.; Topazian, M.D.; Abu Dayyeh, B.K.; Iyer, P.G.; Rajan, E.; Gores, G.J.; et al. Endoscopic Ultrasound/Fine Needle Aspiration Is Effective for Lymph Node Staging in Patients With Cholangiocarcinoma. Hepatology 2020, 72, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.T.; Chew, M.C.H.; Tang, R.S.Y. Troubleshooting Difficult Bile Duct Access: Advanced ERCP Cannulation Techniques, Percutaneous Biliary Drainage, or EUS-Guided Rendezvous Technique? Gastroenterol. Insights 2021, 12, 405–422. [Google Scholar] [CrossRef]
- De Moura, D.T.H.; Moura, E.G.H.; Bernardo, W.M.; De Moura, E.T.H.; Baraca, F.I.; Kondo, A.; Matuguma, S.E.; Almeida Artifon, E.L. Endoscopic retrograde cholangiopancreatography versus endoscopic ultrasound for tissue diagnosis of malignant biliary stricture: Systematic review and meta-analysis. Endosc. Ultrasound 2018, 7, 10–19. [Google Scholar] [CrossRef]
- Sadeghi, A.; Mohamadnejad, M.; Islami, F.; Keshtkar, A.; Biglari, M.; Malekzadeh, R.; Eloubeidi, M.A. Diagnostic yield of EUS-guided FNA for malignant biliary stricture: A systematic review and meta-analysis. Gastrointest. Endosc. 2016, 83, 290–298.e291. [Google Scholar] [CrossRef]
- Hewitt, M.J.; McPhail, M.J.; Possamai, L.; Dhar, A.; Vlavianos, P.; Monahan, K.J. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: A meta-analysis. Gastrointest. Endosc. 2012, 75, 319–331. [Google Scholar] [CrossRef]
- Kitano, M.; Kudo, M.; Yamao, K.; Takagi, T.; Sakamoto, H.; Komaki, T.; Kamata, K.; Imai, H.; Chiba, Y.; Okada, M.; et al. Characterization of small solid tumors in the pancreas: The value of contrast-enhanced harmonic endoscopic ultrasonography. Am. J. Gastroenterol. 2012, 107, 303–310. [Google Scholar] [CrossRef]
- Kovacevic, B.; Vilmann, P. EUS tissue acquisition: From A to B. Endosc. Ultrasound 2020, 9, 225–231. [Google Scholar] [CrossRef]
- van Riet, P.A.; Larghi, A.; Attili, F.; Rindi, G.; Nguyen, N.Q.; Ruszkiewicz, A.; Kitano, M.; Chikugo, T.; Aslanian, H.; Farrell, J.; et al. A multicenter randomized trial comparing a 25-gauge EUS fine-needle aspiration device with a 20-gauge EUS fine-needle biopsy device. Gastrointest. Endosc. 2019, 89, 329–339. [Google Scholar] [CrossRef]
- van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2021, 53, 411–423. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Sanchez, W.; Rosen, C.B.; Gores, G.J. Trans-peritoneal fine needle aspiration biopsy of hilar cholangiocarcinoma is associated with disease dissemination. HPB 2011, 13, 356–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Chafic, A.H.; Dewitt, J.; Leblanc, J.K.; El Hajj, I.I.; Cote, G.; House, M.G.; Sherman, S.; McHenry, L.; Pitt, H.A.; Johnson, C.; et al. Impact of preoperative endoscopic ultrasound-guided fine needle aspiration on postoperative recurrence and survival in cholangiocarcinoma patients. Endoscopy 2013, 45, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Zaheer, A.; Anwar, M.M.; Donohoe, C.; O’Keeffe, S.; Mushtaq, H.; Kelleher, B.; Clarke, E.; Kirca, M.; McKiernan, S.; Mahmud, N.; et al. The diagnostic accuracy of endoscopic ultrasound in suspected biliary obstruction and its impact on endoscopic retrograde cholangiopancreatography burden in real clinical practice: A consecutive analysis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Jo, J.H.; Cho, C.M.; Jun, J.H.; Chung, M.J.; Kim, T.H.; Seo, D.W.; Kim, J.; Park, D.H. Same-session endoscopic ultrasound-guided fine needle aspiration and endoscopic retrograde cholangiopancreatography-based tissue sampling in suspected malignant biliary obstruction: A multicenter experience. J. Gastroenterol. Hepatol. 2019, 34, 799–805. [Google Scholar] [CrossRef] [PubMed]
- de Moura, D.T.H.; Ryou, M.; de Moura, E.G.H.; Ribeiro, I.B.; Bernardo, W.M.; Thompson, C.C. Endoscopic Ultrasound-Guided Fine Needle Aspiration and Endoscopic Retrograde Cholangiopancreatography-Based Tissue Sampling in Suspected Malignant Biliary Strictures: A Meta-Analysis of Same-Session Procedures. Clin. Endosc. 2020, 53, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.N.; Moon, J.H.; Choi, H.J.; Kim, H.K.; Lee, H.W.; Lee, T.H.; Choi, M.H.; Cha, S.W.; Cho, Y.D.; Park, S.H. Tissue acquisition for diagnosis of biliary strictures using peroral cholangioscopy or endoscopic ultrasound-guided fine-needle aspiration. Endoscopy 2019, 51, 50–59. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
CT showing a dilated bile duct and pancreatic duct (double duct sign) caused by a pancreatic head mass.
Figure 1.
CT showing a dilated bile duct and pancreatic duct (double duct sign) caused by a pancreatic head mass.

Figure 2.
EUS images of a benign distal biliary stricture: (A) Diffuse inflammatory thickening of the bile duct wall with a focal nodular area causing a short biliary stricture in a patient with IgG4-SC; (B) Contrast-enhanced EUS showing isoenhancement of the nodular area inside the biliary tract and the thickened bile duct wall, suggestive of an inflammatory stricture.
Figure 2.
EUS images of a benign distal biliary stricture: (A) Diffuse inflammatory thickening of the bile duct wall with a focal nodular area causing a short biliary stricture in a patient with IgG4-SC; (B) Contrast-enhanced EUS showing isoenhancement of the nodular area inside the biliary tract and the thickened bile duct wall, suggestive of an inflammatory stricture.

Figure 3.
Cholangioscopy images of an MBS by mother–baby cholangioscopy with NBI capability. (A) Irregular, nodular bile duct mucosa seen in the region of narrowing upon white light examination. (B) Irregular, dilated and tortuous ‘tumor’ vessels seen on NBI examination.
Figure 3.
Cholangioscopy images of an MBS by mother–baby cholangioscopy with NBI capability. (A) Irregular, nodular bile duct mucosa seen in the region of narrowing upon white light examination. (B) Irregular, dilated and tortuous ‘tumor’ vessels seen on NBI examination.

Figure 4.
D-SOC image of benign biliary strictures. (A) Benign hilar stricture seen in a patient with recurrent pyogenic cholangitis and intrahepatic duct stones. (B)Benign stricture due to focal bile duct wall thickening from inflammation in a patient with IgG4-SC (white arrow).
Figure 4.
D-SOC image of benign biliary strictures. (A) Benign hilar stricture seen in a patient with recurrent pyogenic cholangitis and intrahepatic duct stones. (B)Benign stricture due to focal bile duct wall thickening from inflammation in a patient with IgG4-SC (white arrow).

Figure 5.
D-SOC image of a malignant biliary stricture (cholangiocarcinoma). (A) Tight malignant stricture caused by an irregular polypoid mass. (B) Tortuous, dilated ‘tumor’ vessels.
Figure 5.
D-SOC image of a malignant biliary stricture (cholangiocarcinoma). (A) Tight malignant stricture caused by an irregular polypoid mass. (B) Tortuous, dilated ‘tumor’ vessels.

Figure 6.
EUS images of a distal malignant biliary stricture. (A) A small 1 cm hypoechoic mass was noted in the distal CBD traversed by a plastic biliary stent on EUS. This lesion was not clearly observed in CT abdomen before EUS examination. (B) CE-EUS showed a hypoenhanced mass with fine tumor vessels.
Figure 6.
EUS images of a distal malignant biliary stricture. (A) A small 1 cm hypoechoic mass was noted in the distal CBD traversed by a plastic biliary stent on EUS. This lesion was not clearly observed in CT abdomen before EUS examination. (B) CE-EUS showed a hypoenhanced mass with fine tumor vessels.

Figure 7.
Algorithm for the evaluation of indeterminate biliary strictures. * Consider pCLE or IDUS if available. +EUS-guided tissue sampling may not be necessary if the lesion is potentially operable.
Figure 7.
Algorithm for the evaluation of indeterminate biliary strictures. * Consider pCLE or IDUS if available. +EUS-guided tissue sampling may not be necessary if the lesion is potentially operable.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Etiology of indeterminate biliary strictures (IDBSs).
| Benign | Malignant |
|---|---|
| Iatrogenic bile duct injury Post-endoscopic sphincterotomy, cholecystectomy, liver transplantation | Cholangiocarcinoma Sporadic, PSC-associated |
| Autoinflammatory Primary sclerosing cholangitis (PSC), IgG4-SC, chronic pancreatitis | Pancreatic and ampullary adenocarcinoma |
| Vascular Ischemic cholangiopathy, vasculitis, portal hypertensive biliopathy | Hepatocellular and gallbladder carcinoma |
| Infectious Recurrent pyogenic cholangitis, tuberculosis, human immunodeficiency virus cholangiopathy | Intrahepatic metastasis Lymphoma |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Siu, W.; Tang, R.S.Y. The Role of Cholangioscopy and EUS in the Evaluation of Indeterminate Biliary Strictures. Gastroenterol. Insights 2022, 13, 192-205. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent13020020
AMA Style
Siu W, Tang RSY. The Role of Cholangioscopy and EUS in the Evaluation of Indeterminate Biliary Strictures. Gastroenterology Insights. 2022; 13(2):192-205. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent13020020
Chicago/Turabian StyleSiu, Wilson, and Raymond S. Y. Tang. 2022. "The Role of Cholangioscopy and EUS in the Evaluation of Indeterminate Biliary Strictures" Gastroenterology Insights 13, no. 2: 192-205. https://0-doi-org.brum.beds.ac.uk/10.3390/gastroent13020020