Acute Brucellosis with a Guillain-Barre Syndrome-Like Presentation: A Case Report and Literature Review

 ,
,
Abstract
:1. Introduction
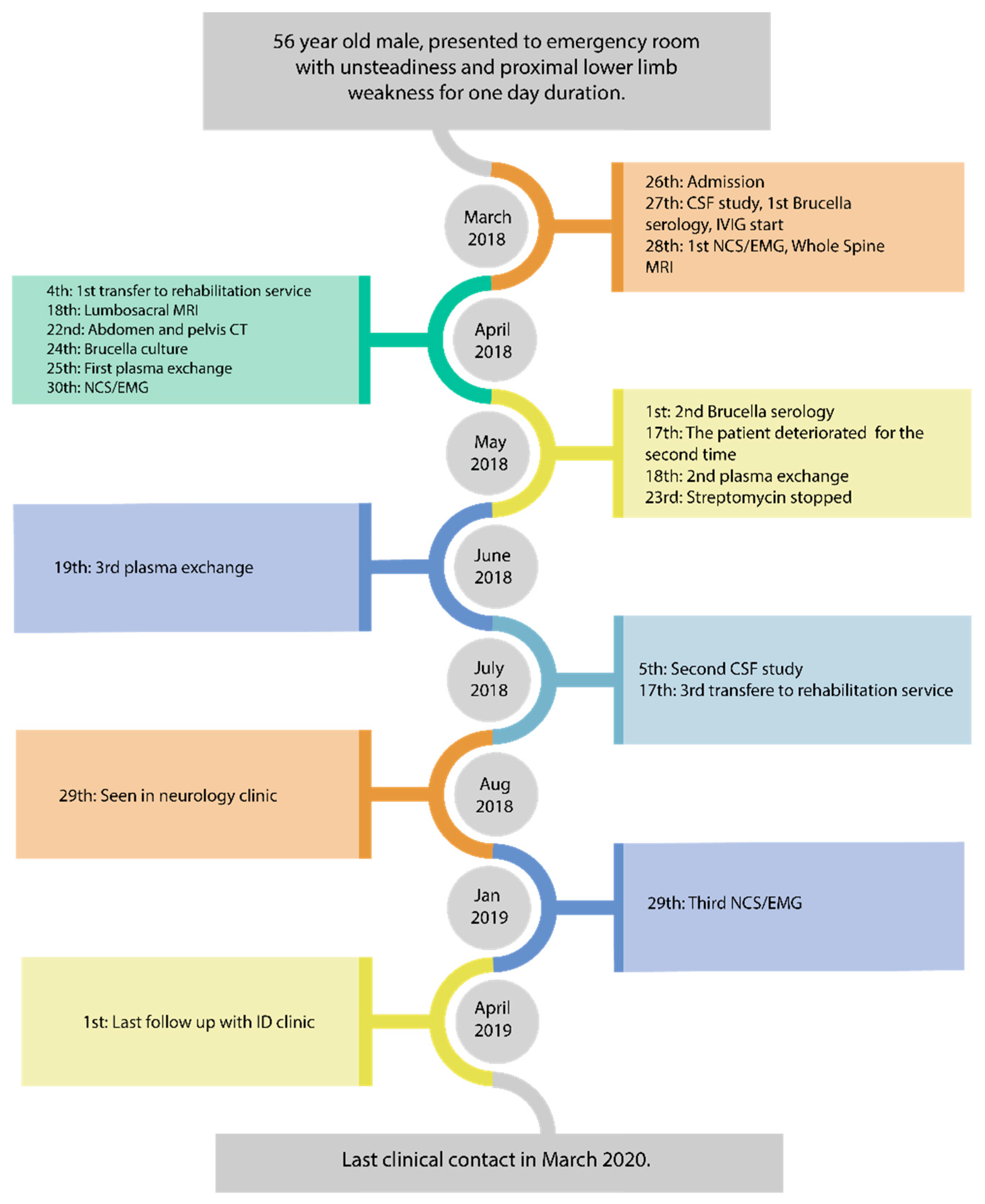
2. Case Report
2.1. Laboratory Investigations
- HgbA1c and blood sugar levels: normal.
- Vitamin B12, B6, B1 and folic acid: normal
- Vitamin E: low (11 mg/L)
- Folate: normal
- Copper: normal
- Immunofixation: normal
- Anti-GM1 ganglioside ant antibodies: negative
- IgG antibodies for EBV and CMV were positive but IgM antibodies were negative.
- B. melitensis titer: positive
- 3/27/18: 1/160; 5/1/2018: 1/320; 7/2/2018: 1/640; 11/19/2018: 1:320; 8/23/2019: 1/160.
- B. abortus titer: negative throughout the disease course.
- First CSF study: WBC < 1; RBC: 25152; Protein 2.52 g/L; Brucella antibody: negative; culture: negative.
2.2. Neurophysiological Studies
- First NCS/EMG: showed evidence of mixed axonal and demyelinating polyneuropathy, in keeping with GBS.
- Second NCS/EMG:
- Absent superficial peroneal, median, and ulnar sensory responses. The sural sensory response was spared.
- Abnormal tibial motor response, with prolonged distal motor latency and reduced conduction velocity in the demyelinating range.
- Absent F wave responses for the median, ulnar, tibial, and peroneal nerves.
- Needle EMG showed abnormal insertional activity in multiple muscles of the upper and lower limbs, with reduced recruitment and normal motor unit morphology.
- Third NCS/EMG:
- Normal sensory responses in the ulnar and sural nerves. Mild prolonged peak latency and reduced conduction velocity in the median sensory response.
- Normal motor responses in the tibial, ulnar, and median nerves.
- Absent left peroneal motor response.
- Normal F wave response for the median, ulnar, and tibial nerves.
- Normal needle EMG in multiple muscles of the upper and lower limbs.
2.3. Search Strategy
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Pappas, G.; Akritidis, N.; Bosilkovski, M.; Tsianos, E. Brucellosis. N. Engl. J. Med. 2005, 352, 2325–2336. [Google Scholar] [CrossRef]
- Shakir, R.A.; Al-Din, A.S.N.; Araj, G.F.; Lulu, A.R.; Mousa, A.R.; Saadah, M.A. Clinical Categories of Neurobrucellosis. Brain 1987, 110, 213–223. [Google Scholar] [CrossRef] [PubMed]
- Gul, H.C.; Erdem, H.; Bek, S. Overview of neurobrucellosis: A pooled analysis of 187 cases. Int. J. Infect. Dis. 2009, 13, e339–e343. [Google Scholar] [CrossRef] [Green Version]
- Daoud, S.; Farhat, N.; Kacem, H.H.; Hdiji, O.; Sakka, S. Guillain Barre Syndrome Associated with Brucellosis: A Case Report and Review of the Literature. J. Neuroinfect. Dis. 2018, 9, 2. [Google Scholar] [CrossRef]
- Donofrio, P.D. Guillain-Barré Syndrome. Continuum Lifelong Learn. Neurol. 2017, 23, 1295–1309. [Google Scholar] [CrossRef] [PubMed]
- Leis, A.A.; Stokic, D.S. Zika virus and Guillain-Barre syndrome: Is there sufficient evidence for causality? Front. Neurol. 2016, 7, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Brucellosis Reference Guide: Exposures, Testing and Prevention. Brucellosis 2017, 1, 1–35. [Google Scholar]
- Desai, B.T.; Toole, J.F. Polyneuropathy as a feature of brucellosis. South. Med. J. 1977, 70, 259. [Google Scholar] [CrossRef] [PubMed]
- Bahemuka, M.; Shemena, A.R.; Panayiotopoulos, C.P.; Al-Aska, A.K.; Obeid, T.A.H.I.R.; Daif, A.K. Neurological syndromes of brucellosis. J. Neurol. Neurosurg. Psychiatry 1988, 51, 1017–1021. [Google Scholar] [CrossRef] [Green Version]
- García, T.; Sánchez, J.C.; Maestre, J.F.; Guisado, F.; Vilches, R.M.; Morales, B. Brucellosis and acute inflammatory polyradiculoneuropathy. Neurologia 1989, 4, 145–147. [Google Scholar]
- Al-Eissa, Y.A.; Al-Herbish, A.S. Severe hypertension: An unusual presentation of Guillain-Barré syndrome in a child with brucellosis. Eur. J. Pediatr. 1996, 155, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Hidir Ulas, U.; Hamamcioglu, K.; Eroglu, E.; Odabasi, Z.; Alanoglu, E.; Demirkaya, S.; Gorenek, L.; Vural, O. Paraplegia associated with brucellosis involving the anterior lumbrosacral nerve roots. J. Peripher. Nerv. Syst. 2003, 8, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Namiduru, M.; Karaoglan, I.; Yilmaz, M. Guillain-Barré syndrome associated with acute neurobrucellosis. Int. J. Clin. Pract. 2003, 57, 919–920. [Google Scholar] [PubMed]
- Goktepe, A.S.; Alaca, R.; Mohur, H.; Coskun, U. Neurobrucellosis and a demonstration of its involvement in spinal roots via magnetic resonance imaging. Spinal Cord 2003, 41, 574–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haghighi, A.B.; Sabayan, B. Acute axonal poly-radiculoneuropathy associated with partially treated brucellosis: A case report. J. Clin. Neuromuscul. Dis. 2007, 9, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Gul, H.C.; Erdem, H.; Gorenek, L.; Ozdag, M.F.; Kalpakci, Y.; Avci, I.Y.; Besirbellioglu, B.A.; Eyigun, C.P. Management of neurobrucellosis: An assessment of 11 cases. Intern. Med. 2008, 47, 995–1001. [Google Scholar] [CrossRef] [Green Version]
- Shoja, M.M.; Khosroshahi, H.T.; Tubbs, R.S.; Fervenza, F.C. Brucellosis mimicking vasculitis in a patient with renal failure and peripheral neuropathy. Am. J. Med. Sci. 2008, 336, 285–287. [Google Scholar] [CrossRef]
- Montalvo, R.; García, Y.; Ñavincopa, M.; Ticona, E.; Chávez, G.; Moore, D.A. Síndrome de Guillain Barré asociado a Brucelosis. Rev. Peru. Med. Exp. Salud Publica 2010, 27, 292–295. [Google Scholar] [CrossRef] [Green Version]
- Aygul, R.; Deniz, O.; Guzelcik, M.; Kotan, D. Guillain-Barré Syndrome during Active Brucellosis. Eurasian J. Med. 2010, 42, 157–159. [Google Scholar] [CrossRef]
- Babamahmoodi, F.; Babamahmoodi, A. Brucellosis, presenting with guillain-barré syndrome. J. Glob. Infect. Dis. 2011, 3, 390–392. [Google Scholar] [CrossRef]
- Elzein, F.E.; Mursi, M. Case report: Brucella induced Guillain-Barré syndrome. Am. J. Trop. Med. Hyg. 2014, 91, 1179–1180. [Google Scholar] [CrossRef] [Green Version]
- Paydarnia, P.; Moradi, S.; Habibi, A.; Abbasian, L.; Ghabaee, M. A case report of neurobrucellosis mimicking Guillain–Barré syndrome. Neurol. Psychiatry Brain Res. 2019, 31, 27–28. [Google Scholar] [CrossRef]
- González-Suárez, I.; Sanz-Gallego, I.; Rodríguez de Rivera, F.J.; Arpa, J. Guillain-Barré syndrome: Natural history and prognostic factors: A retrospective review of 106 cases. BMC Neurol. 2013, 13, 95. [Google Scholar] [CrossRef] [Green Version]
- Löffel, N.B.; Rossi, L.N.; Mumenthaler, M.; Lütschg, J.; Ludin, H.P. The Landry-Guillain-barré syndrome. Complications, prognosis and natural history in 123 cases. J. Neurol. Sci. 1977, 33, 71–79. [Google Scholar] [CrossRef]
- Fokke, C.; van den Berg, B.; Drenthen, J.; Walgaard, C.; van Doorn, P.A.; Jacobs, B.C. Diagnosis of Guillain-arré syndrome and validation of Brighton criteria. Brain 2014, 137, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Kim, S.; Nishiguchi, M.; Suzuki, H.; Watarai, M. Brucella melitensis infection associated with Guillain-Barré syndrome through molecular mimicry of host structures. FEMS Immunol. Med. Microbiol. 2005, 45, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuki, N. Infectious origins of, and molecular mimicry in, Guillain-Barré and Fisher syndromes. Lancet Infect. Dis. 2001, 1, 29–37. [Google Scholar] [CrossRef]
- Esposito, S.; Longo, M.R. Guillain–Barré syndrome. Autoimmun. Rev. 2017, 16, 96–101. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Brucella Culture | MRI Findings | NCS and EMG Findings | Treatment | Prognosis | |
|---|---|---|---|---|---|---|
| Brucellosis | GBS | |||||
| Desai [8] | B. abortus | NA | NA | DOXY, Streptomycin and TMP/SMX | NA | Complete recovery, after 3 months |
| Bahemuka Case # 8 [9] | NA | NA | EMG showed denervation and NCS was normal | RIF and DOXY | NA | Walk with Zimmer frame after 6 weeks |
| Garcia [10] (3 cases) from abstract and Daoud et al. | NA | NA | 1 case: Pure M axonal PRN 2 cases: M DEM PRN in the remaining 2 patients | RIF and DOXY (4) | PLEX (4) | Unfavorable outcome in one case of axonal GBS (died), partial recovery in the remaining 2 cases of DEM GBS |
| Al-Eissa [11] | NA | NA | DEM PRN | RIF, DOXY, Streptomycin and TMP/SMX | NA | Completely cured during a 1 year follow up |
| Hidir [12] | B. melitensis | Selective enhancement of ventral lumbosacral nerve roots and cauda equina | DEM PRN with secondary axonal loss | RIF, DOXY, and CFXN | NA | Complete recovery and able to walk unaided after 6 months |
| Namiduru [13] from abstract and Daoud et al. | B. melitensis | NA | NA | RIF and TMP/SMX | PLEX (4) | Complete recovery within 1 month |
| Goktepe [14] | B. melitensis | Thickening of the spinal nerve roots and diffuse enhancement along the distal cord and cauda equina | Pure motor PRN with normal sensory NCS | RIF, DOXY, and CFXN | PLEX and IVIG | Able to walk with minimal help after 3 months |
| Haghighi [15] | NA | Unremarkable | Acute M-S axonal PRN | RIF, DOXY, and CFXN | PLEX and IVIG | Full strength after 1 year |
| Gul [16] Case # 8 | B. melitensis | Contrast enhancement of lumbar roots | PRN (axonal degeneration) | RIF, DOXY, and CFXN | NA | Barely able to walk unassisted after 6 months. |
| Shoja [17] | NA | NA | Symmetrical distal axonal S-M PN | RIF and DOXY | N/A “MP 1 g/day for suspected systemic vasculitis” | Weakness resolved after 1 month |
| Montalvo [18] From abstract | NA | NA | Pure M PRN with axonal pattern | RIF and DOXY | PLEX | Complete recovery after 3 months |
| Aygul [19] | B. melitensis (from bone marrow) | Unremarkable | Acute DEM PRN | RIF, DOXY, Streptomycin and TMP/SMX | IVIG | Able to walk unaided after 3 months aside from mild facial diplegia |
| Babamahmood [20] | NA | Unremarkable | DEM PN | RIF, DOXY, Gentamycin, Streptomycin and TMP/SMX | IVIG | Able to walk normally after 4 weeks |
| Elzein [21] | NA | NA | DEM S-M PN | RIF, DOXY and Streptomycin | IVIG | Able to mobilize after 3 weeks |
| Daoud [4] | NA | NA | DEM PRN | RIF and DOXY | PLEX | Partial recovery, and able to walk unaided after 4 weeks |
| Paydarnia [22] | NA | Mild enhancement of thoracic region | Generalized axonal PN | RIF, DOXY and Ciprofloxacin | PLEX | Walking normally after 6 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alanazi, A.; Al Najjar, S.; Madkhali, J.; Al Malik, Y.; Al-Khalaf, A.; Alharbi, A. Acute Brucellosis with a Guillain-Barre Syndrome-Like Presentation: A Case Report and Literature Review. Infect. Dis. Rep. 2021, 13, 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010001
Alanazi A, Al Najjar S, Madkhali J, Al Malik Y, Al-Khalaf A, Alharbi A. Acute Brucellosis with a Guillain-Barre Syndrome-Like Presentation: A Case Report and Literature Review. Infectious Disease Reports. 2021; 13(1):1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010001
Chicago/Turabian StyleAlanazi, Ali, Sara Al Najjar, Jnadi Madkhali, Yaser Al Malik, Athal Al-Khalaf, and Ahmad Alharbi. 2021. "Acute Brucellosis with a Guillain-Barre Syndrome-Like Presentation: A Case Report and Literature Review" Infectious Disease Reports 13, no. 1: 1-10. https://0-doi-org.brum.beds.ac.uk/10.3390/idr13010001