
Impact of the COVID-19 Pandemic Surveillance of Visceral Leishmaniasis in Brazil: An Ecological Study
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
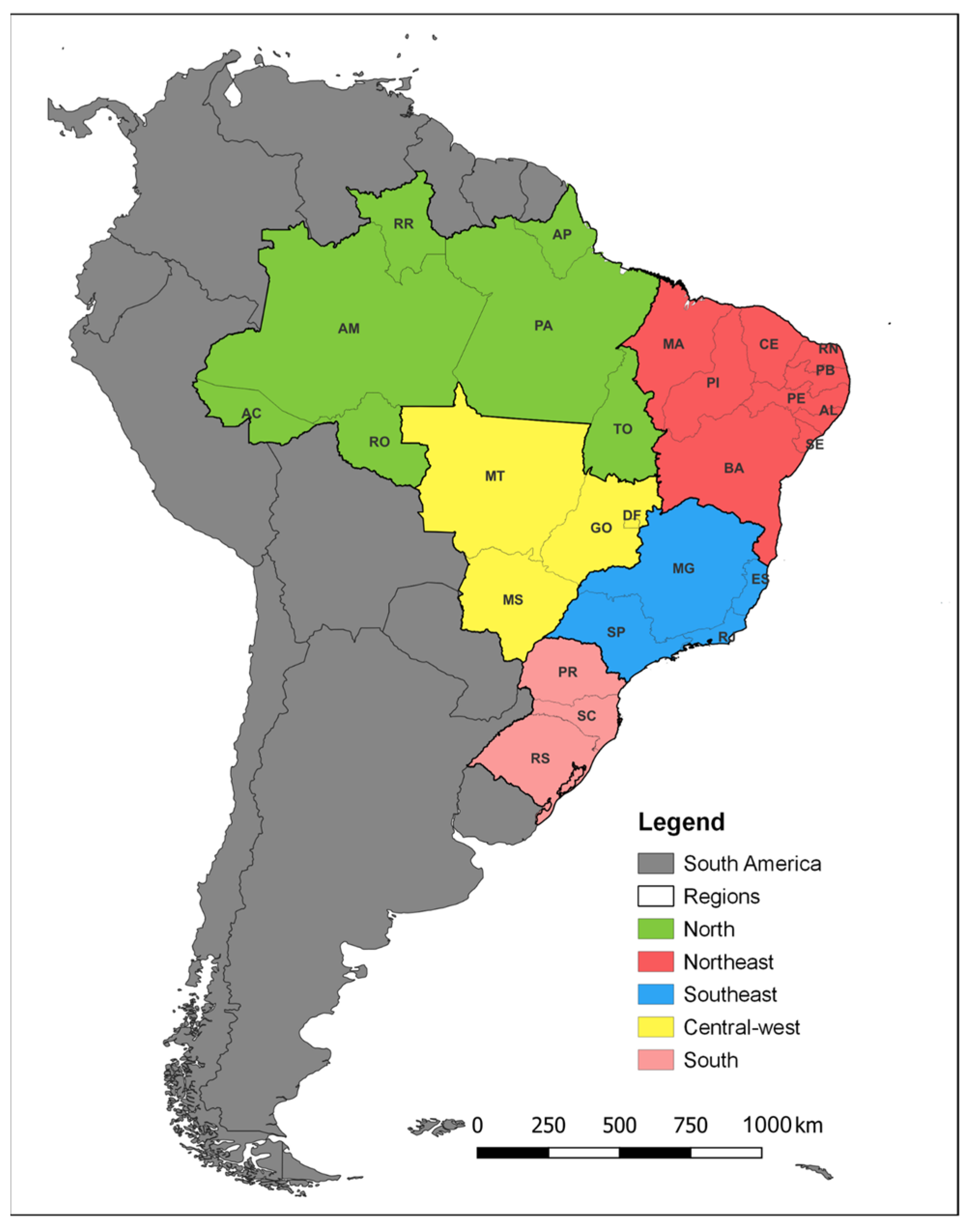
2.2. Study Area
2.3. Study Population and Data Source
2.4. Study Variables
2.5. Descriptive Analysis
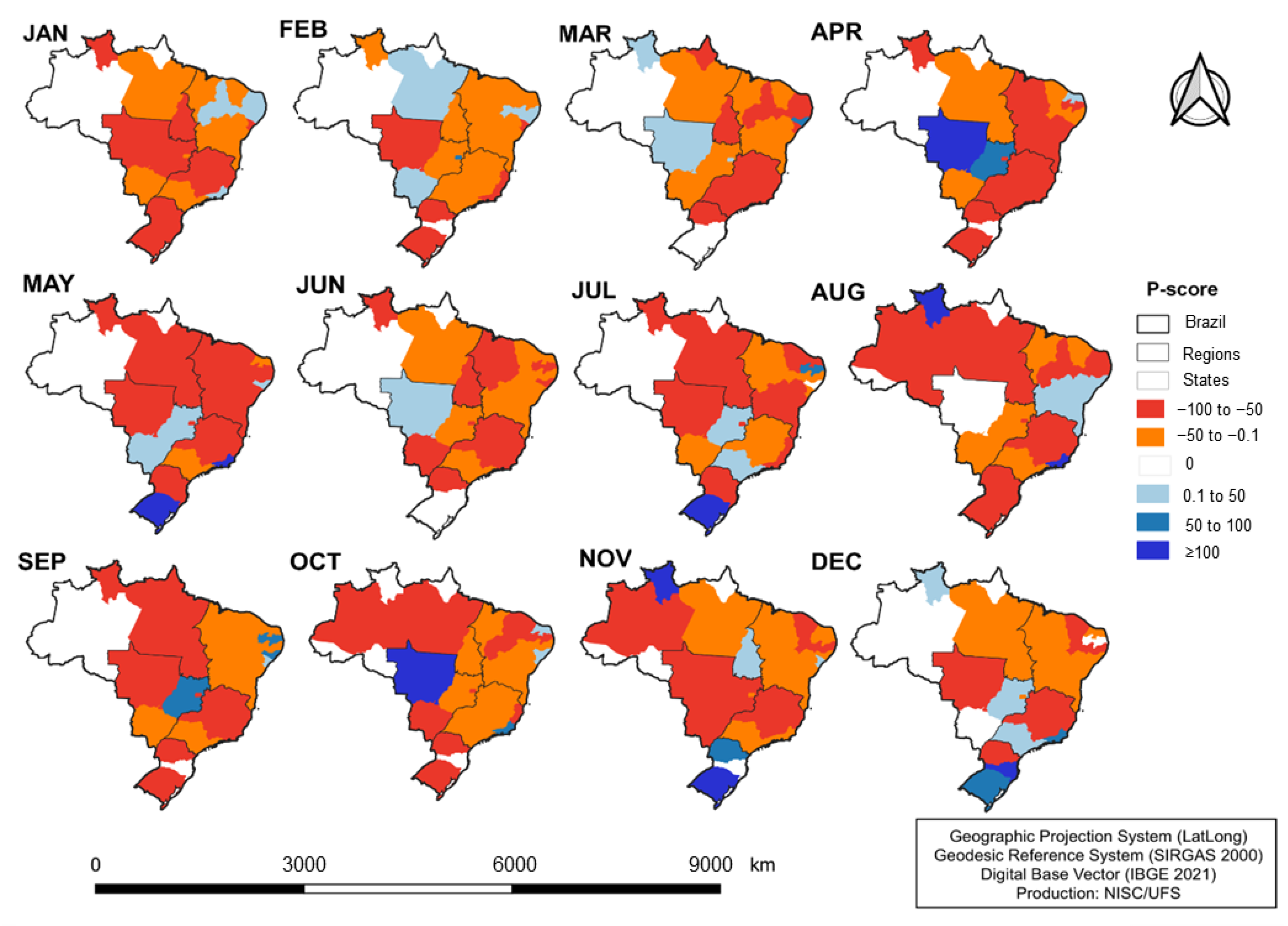
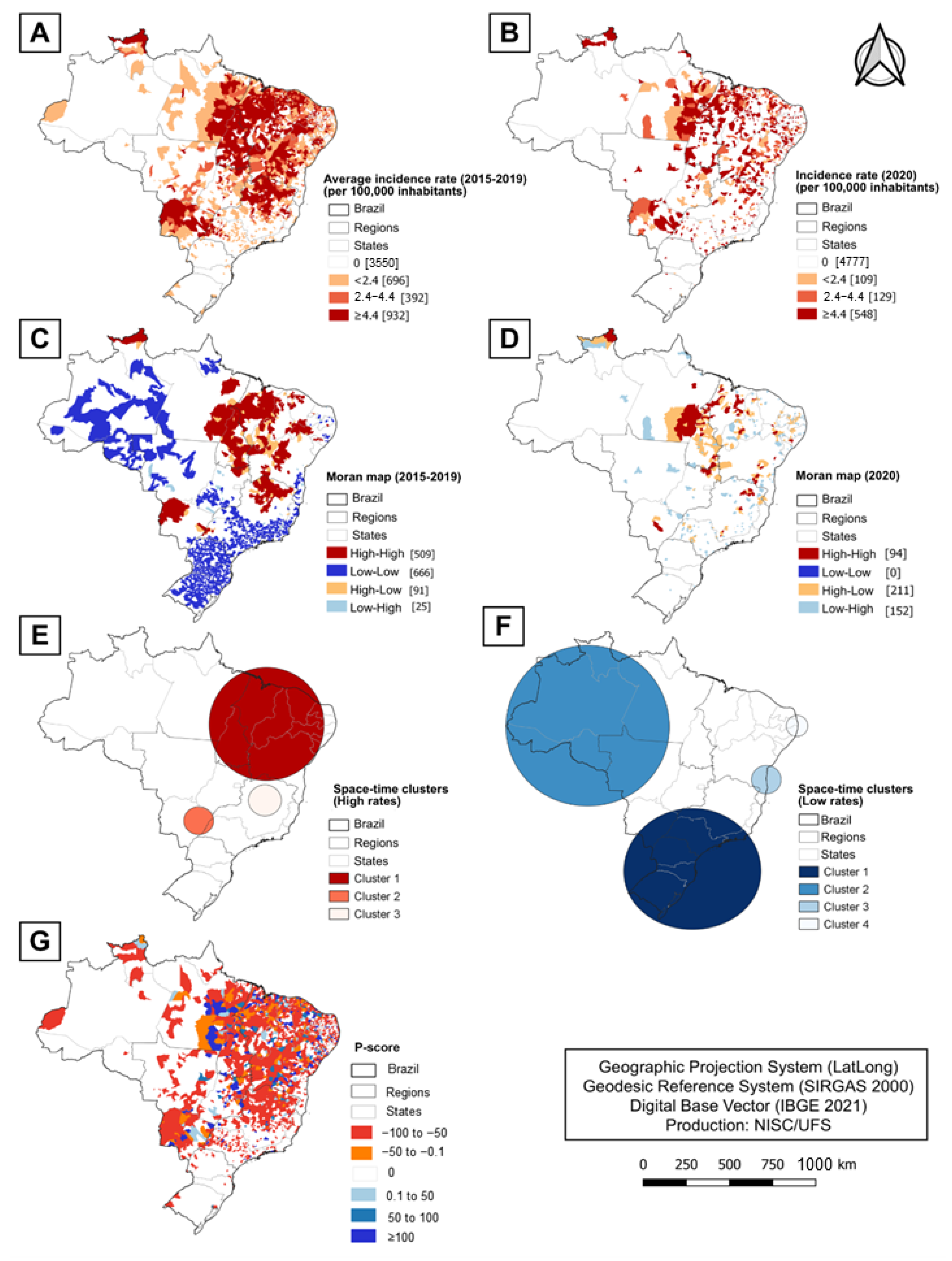
2.6. Spatial Analysis
2.7. Spatiotemporal Analysis
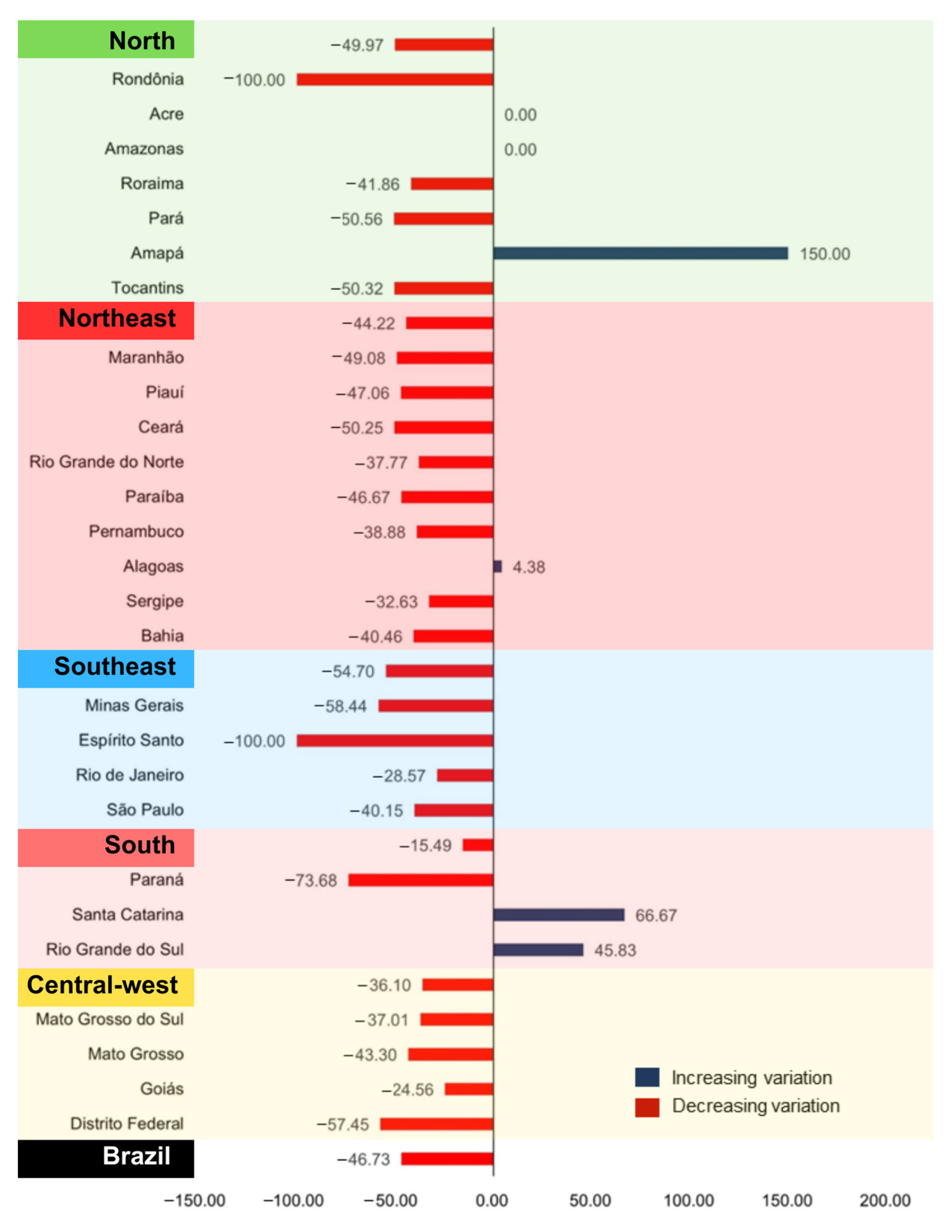
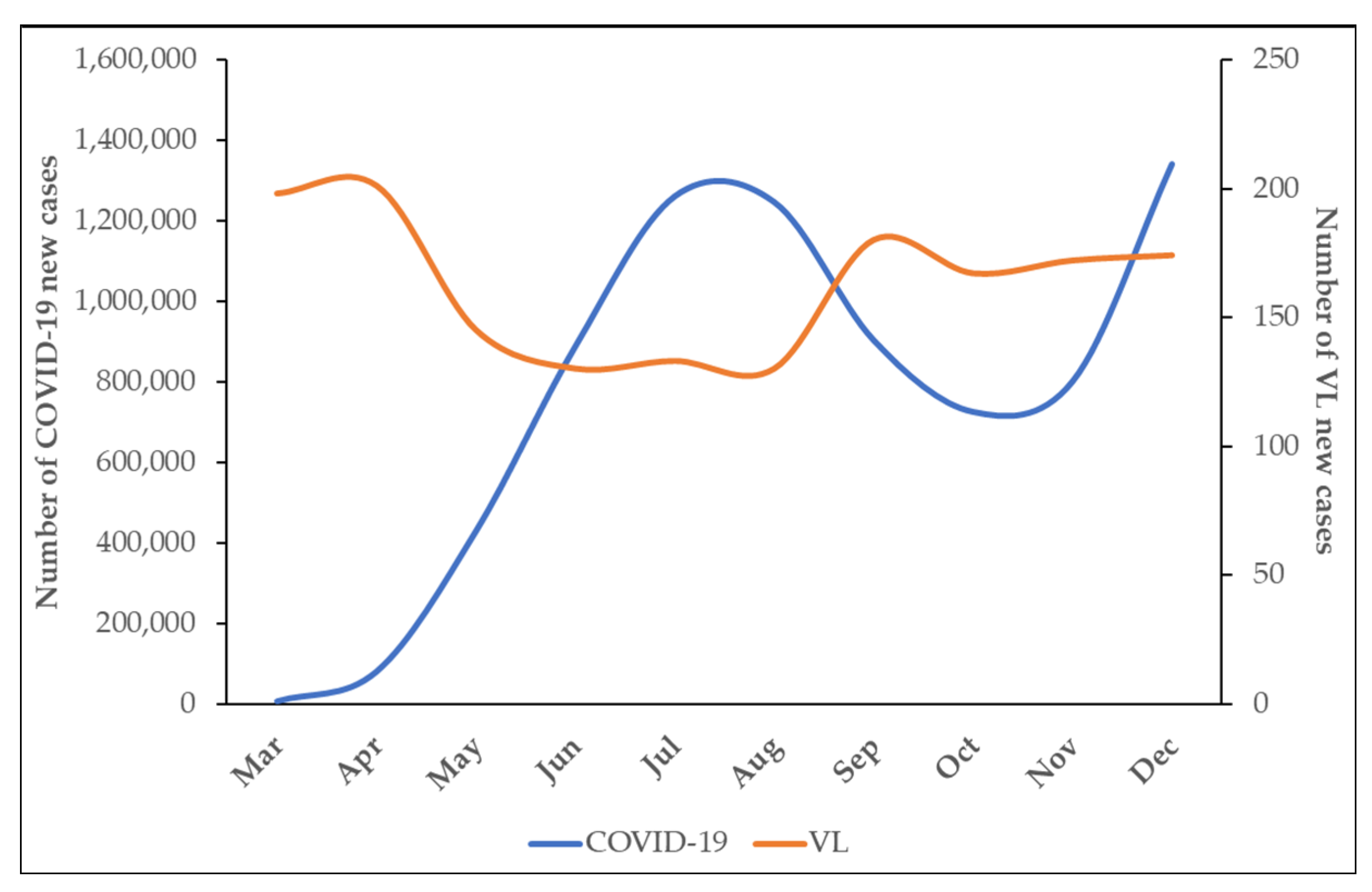
3. Results
4. Discussion
4.1. Global Health Implications
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khedar, R.S.; Gupta, R.; Sharma, K.; Mittal, K.; Ambaliya, H.C.; Gupta, J.B.; Singh, S.; Sharma, S.; Singh, Y.; Mathur, A. Biomarkers and outcomes in hospitalised patients with COVID-19: A prospective registry. BMJ Open 2022, 12, e067430. [Google Scholar] [CrossRef]
- Brito, P.d.S.; Pascoal, L.M.; Costa, M.V.T.; da Silva, L.F.M.; de Melo, L.P.L.; Neto, M.S.; Lima, F.E.T.; Santos, F.S. Primary Health Care assessment in the COVID-19 pandemic from physicians’ and nurses’ perspective. Rev. Bras. Enferm. 2023, 76, e20220475. [Google Scholar] [CrossRef]
- Prado, E.; Camparoto, C.W.; Takemoto, A.Y.; Ichisato, S.M.T.; Miguel, M.E.G.B.; Marcon, S.S. Palliative care strategies in the management of people with severe cases of COVID-19. Rev. Bras. Enferm. 2023, 76 (Suppl. S1), e20220308. [Google Scholar] [CrossRef]
- World Health Organization. Impact of the COVID-19 Pandemic on Seven Neglected Tropical Diseases: A Model-Based Analysis. Whoint [Internet]. 2021. Available online: https://apps.who.int/iris/handle/10665/343993 (accessed on 1 February 2024).
- de Toledo, C.R.S.; de Almeida, A.S.; Chaves, S.A.d.M.; Sabroza, P.C.; Toledo, L.M.; Caldas, J.P. Vulnerability to the transmission of human visceral leishmaniasis in a Brazilian urban area. Rev. Saude Publica 2017, 51, 49. [Google Scholar] [CrossRef]
- Ribeiro, C.J.N.; dos Santos, A.D.; Lima, S.V.M.A.; da Silva, E.R.; Ribeiro, B.V.S.; Duque, A.M.; Peixoto, M.V.S.; dos Santos, P.L.; de Oliveira, I.M.; Lipscomb, M.W.; et al. Space-time risk cluster of visceral leishmaniasis in Brazilian endemic region with high social vulnerability: An ecological time series study. PLoS Neglected Trop. Dis. 2021, 15, e0009006. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, L.C.; Moreira, N.M. Epidemiological aspects of visceral leishmaniasis in Brazil and in international border regions. Res. Soc. Dev. 2021, 10, e549101220684. [Google Scholar] [CrossRef]
- Ávila, I.R.; de Araújo, G.R.; Barbosa, D.S.; Bezerra, J.M.T. Occurrence of human visceral leishmaniasis in the Central-West region of Brazil: A systematic review. Acta Trop. 2023, 237, 106707. [Google Scholar] [CrossRef]
- Leishmaniasis [Internet]. WHO|Regional Office for Africa. Available online: https://www.afro.who.int/health-topics/Leishmaniasis (accessed on 1 February 2024).
- Miguel, D.C.; Brioschi, M.B.; Rosa, L.B.; Minori, K.; Grazzia, N. The impact of COVID-19 on neglected parasitic diseases: What to expect? Trends Parasitol. 2021, 37, 694–697. [Google Scholar] [CrossRef] [PubMed]
- Toor, J.; Adams, E.R.; Aliee, M.; Amoah, B.; Anderson, R.M.; Ayabina, D.; Bailey, R.; Basáñez, M.-G.; Blok, D.J.; Blumberg, S.; et al. Predicted Impact of COVID-19 on Neglected Tropical Disease Programs and the Opportunity for Innovation. Clin. Infect. Dis. 2020, 72, 1463–1466. [Google Scholar] [CrossRef]
- IBGE|Portal Do IBGE|IBGE [Internet]. Ibge.gov.br. 2022. Available online: http://www.ibge.gov.br/home (accessed on 1 February 2024).
- Excess Mortality during the Coronavirus Pandemic (COVID-19) [Internet]. Our World in Data. Available online: https://ourworldindata.org/excess-mortality-covid (accessed on 1 February 2024).
- Anselin, L. Local Indicators of Spatial Association-LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- da Paz, W.S.; Souza, M.D.R.; Tavares, D.d.S.; de Jesus, A.R.; dos Santos, A.D.; Carmo, R.F.D.; de Souza, C.D.F.; Bezerra-Santos, M. Impact of the COVID-19 pandemic on the diagnosis of leprosy in Brazil: An ecological and population-based study. Lancet Reg. Health Am. 2022, 9, 100181. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.D.R.; da Paz, W.S.; Sales, V.B.d.S.; de Jesus, G.F.H.; Tavares, D.d.S.; Lima, S.V.M.A.; Sousa, F.L.; de Melo, E.V.; Carmo, R.F.D.; de Souza, C.D.F.; et al. Impact of the COVID-19 Pandemic on the Diagnosis of Tuberculosis in Brazil: Is the WHO End TB Strategy at Risk? Front. Pharmacol. 2022, 13, 891711. [Google Scholar] [CrossRef] [PubMed]
- do Carmo, R.F.; de Souza, C.D.F. Impact of the COVID-19 pandemic on hepatitis C diagnosis in Brazil: Is the global hepatitis C elimination strategy at risk? J. Hepatol. 2021, 76, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Dantas, N.M.; Andrade, L.A.; da Paz, W.S.; Borges, W.N.; Barbosa, V.G.B.; da Hora, D.P.G.; da Silva, C.E.; Carmo, R.F.D.; de Souza, C.D.F.; dos Santos, A.D.; et al. Impact of the COVID-19 pandemic on the actions of the Schistosomiasis Control Program in an endemic area in Northeastern Brazil. Acta Trop. 2023, 240, 106859. [Google Scholar] [CrossRef] [PubMed]
- Abreu, M.d.S.; de Siqueira, J.M.M.T.; Maia, J.C.d.S.; Nepomuceno, D.B.; Luz, E.B.A.L.; Mendes-Sousa, A.F. Aspectos epidemiológicos e distribuição espacial da leishmaniose visceral em Picos, Piauí, Brasil. Saúde Coletiva 2021, 11, 5846–5857. [Google Scholar] [CrossRef]
- Da Silva, A.S.; da Silva, M.V.S.; dos Reis, D.S.T.; Couto, D.C.C.; Pinto, D.S.; de Melo, L.S.C.; Costa, D.C.d.S.; Farias, T.C.B.; Maroja, M.C.F.d.S.; de Barros, S.H.P. Perfil epidemiológico e distribuição espacial da leishmaniose visceral no estado do Pará. Rev. Eletrônica Acervo Saúde 2022, 15, e10242. [Google Scholar] [CrossRef]
- Abdela, S.G.; Van Griensven, J.; Seife, F.; Enbiale, W. Neglecting the effect of COVID-19 on neglected tropical diseases: The Ethiopian perspective. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 730–732. [Google Scholar] [CrossRef]
- Leishmanioses: Informe Epidemiológico das Américas. No 11 (Dezembro de 2022)—OPAS/OMS|Organização Pan-Americana da Saúde [Internet]. Available online: https://www.paho.org/pt/documentos/leishmanioses-informe-epidemiologico-das-americas-no-11-dezembro-2022 (accessed on 1 February 2024).
- Ministério da Saúde. Boletim Epidemiológico Especial—Doença Pelo Coronavírus COVID-19—2020. Brasília. 2020. Available online: https://www.gov.br/saude/pt-br/coronavirus/boletins-epidemiologicos/boletim-epidemiologico-covid-19-no-42.pdf (accessed on 1 February 2024).
- Andrade, M.C.; Bonan, P.R.F.; Hilan, E.; Marques, N.P.; Guimarães-Carvalho, S.F.; Martelli, H. COVID-19 Pandemic Causes Increased Clinic Visits with Diagnosis of Tegumentary Leishmaniasis in Brazil in 2020. Int. J. Infect. Dis. 2021, 113, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Lima, I.D.; Lima, A.L.M.; Mendes-Aguiar, C.d.O.; Coutinho, J.F.V.; Wilson, M.E.; Pearson, R.D.; Queiroz, J.W.; Jeronimo, S.M.B. Changing demographics of visceral leishmaniasis in northeast Brazil: Lessons for the future. PLoS Neglected Trop. Dis. 2018, 12, e0006164. [Google Scholar] [CrossRef] [PubMed]
- Rocha, C.A.d.O.; Santana, G.B.d.A.; Leal, T.C.; de Paiva, J.P.S.; da Silva, L.F.; Santos, L.G.; Nunes, B.E.B.R.; Carmo, R.F.D.; de Souza, C.D.F. Impact of the COVID-19 pandemic on compulsory notification of meningitis during the first wave of the pandemic in Brazil: An ecological study using P-score. Sao Paulo Med. J. 2022, 140, 305–309. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | Period | Number of Municipalities | Regions | New Cases | New Expected Cases | Monthly Incidence Rates a | RR | LLR |
|---|---|---|---|---|---|---|---|---|
| Low rates | ||||||||
| 1 | March–August | 2349 | Central-west, Southeast, and South | 58 | 471 | 0.10 | 0.10 | 345.4 |
| 2 | January–June | 259 | North and Central-west | 1 | 50 | 0.02 | 0.02 | 46.2 |
| 3 | January–November | 116 | Northeast | 1 | 27 | 0.03 | 0.04 | 23.3 |
| 4 | March–August | 203 | Northeast | 9 | 44 | 0.20 | 0.20 | 21.4 |
| High rates | ||||||||
| 1 | July–December | 1549 | Northeast, North, and Central-west | 673 | 185 | 3.30 | 5.06 | 457.4 |
| 2 | April–September | 50 | Central-west and Southeast | 48 | 8 | 5.40 | 6.05 | 45.9 |
| 3 | May–October | 170 | Southeast | 49 | 16 | 2.80 | 3.07 | 22.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, J.R.S.; Lima, S.V.M.A.; dos Santos, A.D.; Siqueira, L.S.; Santos, G.R.d.S.; Sousa, Á.F.L.d.; de Oliveira, L.B.; Mendes, I.A.C.; Ribeiro, C.J.N. Impact of the COVID-19 Pandemic Surveillance of Visceral Leishmaniasis in Brazil: An Ecological Study. Infect. Dis. Rep. 2024, 16, 116-127. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16010009
Silveira JRS, Lima SVMA, dos Santos AD, Siqueira LS, Santos GRdS, Sousa ÁFLd, de Oliveira LB, Mendes IAC, Ribeiro CJN. Impact of the COVID-19 Pandemic Surveillance of Visceral Leishmaniasis in Brazil: An Ecological Study. Infectious Disease Reports. 2024; 16(1):116-127. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16010009
Chicago/Turabian StyleSilveira, Josefa Rayane Santos, Shirley Verônica Melo Almeida Lima, Allan Dantas dos Santos, Luana Silva Siqueira, Guilherme Reis de Santana Santos, Álvaro Francisco Lopes de Sousa, Layze Braz de Oliveira, Isabel Amélia Costa Mendes, and Caíque Jordan Nunes Ribeiro. 2024. "Impact of the COVID-19 Pandemic Surveillance of Visceral Leishmaniasis in Brazil: An Ecological Study" Infectious Disease Reports 16, no. 1: 116-127. https://0-doi-org.brum.beds.ac.uk/10.3390/idr16010009