
Fish Roe-Induced Anaphylaxis in Italy: A Pediatric Case Report

 ,
,
Abstract
:1. Introduction
2. Case Presentation
2.1. Medical History
2.2. Clinical Presentation
2.3. Clinical Course
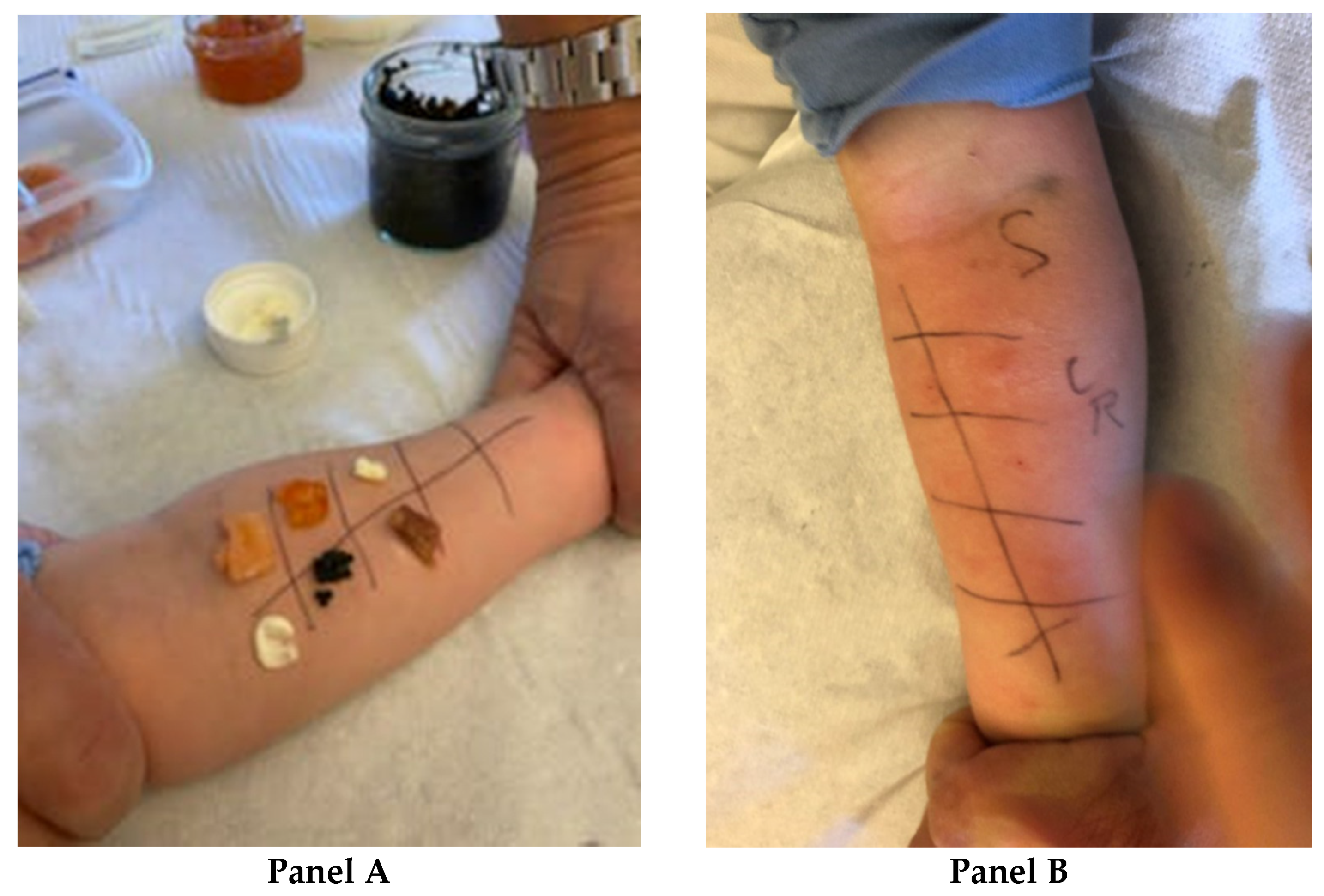
2.4. Follow Up and Specific Allergy Tests
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ebisawa, M.; Ito, K.; Fujisawa, T. Committee for Japanese Pediatric Guideline for Food Allergy, The Japanese Society of Pediatric Allergy and Clinical Immunology, The Japanese Society of Allergology. Japanese Guidelines for Food Allergy 2017. Allergol. Int. 2017, 66, 248–264. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Nakamura, A.; Kishimura, H.; Hara, A.; Watanabe, K.; Saeki, H. Major allergen and its IgE cross-reactivity among salmonid fish roe allergy. J. Agric. Food Chem. 2009, 57, 2314–2319. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Oda, Y.; Suzuki, I. Intussusception secondary to anaphylactic reaction to salmon roe (ikura). Pediatr. Int. 2013, 55, 649–651. [Google Scholar] [CrossRef] [PubMed]
- Pages, A.; Leduc, V.; De Lacoste de Laval, A.; Nelson, J.R.; Pere, B. Allergy to salmon eggs without concomitant fish allergies, three pediatric cases. Rev. French Allergol. 2015, 44, 301–304. [Google Scholar]
- Minhas, J.; Saryan, J.A.; Balekian, D.S. Salmon roe (ikura) induced anaphylaxis in a child. Ann. Allergy Asthma Immunol. 2017, 118, 365–383. [Google Scholar] [CrossRef] [PubMed]
- Flais, M.J.; Kim, S.S.; Harris, K.E.; Greenberger, P.A. Salmon caviar-induced anaphylactic shock. Allergy Asthma Proc. 2004, 24, 233–236. [Google Scholar]
- Cosme, J.; Spínola-Santos, A.; Bartolomé, B.; Pastor-Vargas, C.; Branco-Ferreira, M.; Pereira-Santos, M.C.; Pereira-Barbosa, M. Salmon Roe as an Emerging Allergen in Western Countries. J. Investig. Allergol. Clin. Immunol. 2019, 29, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Muraro, A.; Roberts, G.; Worm, M.; Bilò, M.B.; Brockow, K.; Fernández Rivas, M.; Santos, A.F.; Zolkipli, Z.Q.; Bellou, A.; Beyer, K.; et al. EAACI Food Allergy and Anaphylaxis Guidelines Group. Anaphylaxis: Guidelines from the European Academy of Allergy and Clinical Immunology. Allergy 2014, 69, 1026–1045. [Google Scholar] [CrossRef] [PubMed]
- Grabenhenrich, L.B.; Dölle, S.; Moneret-Vautrin, A.; Köhli, A.; Lange, L.; Spindler, T.; Ruëff, F.; Nemat, K.; Maris, I.; Roumpedaki, E.; et al. Anaphylaxis in children and adolescents: The European Anaphylaxis Registry. J. Allergy Clin. Immunol. 2016, 137, 1128–1137.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, H.P.; Bansil, S.; Uygungil, B. Signs and Symptoms of Food Allergy and Food-Induced Anaphylaxis. Pediatr Clin. N. Am. 2015, 62, 1377–1392. [Google Scholar] [CrossRef] [PubMed]
- Passia, E.; Jandus, P. Using Baseline and Peak serum tryptase levels to diagnose anaphylaxis: A Review. Clin. Rev. Allergy Immunol. 2020, 58, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Perez-Gordo, M.; Sanchez-Garcia, S.; Cases, B.; Pastor, C.; Vivanco, F.; Cuesta-Herranz, J. Identification of vitellogenin as an allergen in Beluga caviar allergy. Allergy 2008, 63, 479–480. [Google Scholar] [CrossRef] [PubMed]
- Kalic, T.; Radauer, C.; Lopata, A.L.; Breiteneder, H.; Hafner, C. Fish Allergy Around the World-Precise Diagnosis to Facilitate Patient Management. Front. Allergy 2021, 2, 732178. [Google Scholar]
- Kondo, Y.; Kakami, M.; Koyama, H.; Yasuda, T.; Nakajima, Y.; Kawamura, M.; Tokuda, R.; Tsuge, I.; Urisu, A. IgE Cross-reactivity between fish roe (salmon, herring and pollock) and chicken egg in patients anaphylactic to salmon roe. Allergol. Int. 2005, 54, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Saeki, H. Allergen in fish roe. Allergy Pract. 2008, 28, 625–630. [Google Scholar]
- Hanaoka, K.; Takahagi, S.; Ishii, K.; Nakano, M.; Chinuki, Y.; Tanaka, A.; Yanase, Y.; Hide, M. Type-I-hypersensitivity to 15 kDa, 28 kDa and 54 kDa proteins in vitellogenin specific to Gadus chalcogrammus roe. Allergol. Int. 2020, 69, 253–260. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Values | Normal Values | |
|---|---|---|
| White blood cells (×103/µL) | 9.50 | 6–17 |
| Red blood cells (×106/µL) | 5.34 | 4–5.1 |
| Platelets (×103/µL) | 459 | 150–450 |
| Hemoglobin (g/dL) | 14.9 | 10.3–14.3 |
| Hematocrit (%) | 42.5 | 31–43 |
| Neutrophils (%) | 31.3 | 33 |
| Lymphocytes (%) | 61.8 | 59 |
| Monocytes (%) | 4.5 | 5 |
| Eosinophils (%) | 2.1 | 3 |
| C-reactive protein (mg/dL) | 0.03 | 0–0.5 |
| Glycemia (mg/dL) | 112 | 74–100 |
| Urea (mg/dL) | 36 | 10–50 |
| Creatinine (mg/dL) | 0.31 | 0.6–1.2 |
| Sodium (mEq/L) | 141 | 135–146 |
| Potassium (mEq/L) | 4.3 | 3.6–5 |
| Chlorine (mEq/L) | 106 | 97–110 |
| Calcium (mg/dL) | 10.40 | 8.10–10.40 |
| Aspartate aminotransferase (U/L) | 41 | 10–50 |
| Alanine aminotransferase (U/L) | 34 | 15–40 |
| LDH (U/L) | 391 | 150–500 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Paulis, N.; Di Costanzo, M.; Capra, M.E.; Peveri, S.; Montagni, M.; Biasucci, G. Fish Roe-Induced Anaphylaxis in Italy: A Pediatric Case Report. Pediatr. Rep. 2022, 14, 170-174. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14020023
De Paulis N, Di Costanzo M, Capra ME, Peveri S, Montagni M, Biasucci G. Fish Roe-Induced Anaphylaxis in Italy: A Pediatric Case Report. Pediatric Reports. 2022; 14(2):170-174. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14020023
Chicago/Turabian StyleDe Paulis, Nicoletta, Margherita Di Costanzo, Maria Elena Capra, Silvia Peveri, Marcello Montagni, and Giacomo Biasucci. 2022. "Fish Roe-Induced Anaphylaxis in Italy: A Pediatric Case Report" Pediatric Reports 14, no. 2: 170-174. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric14020023