
Effects of Two Online Mindfulness-Based Interventions for Early Adolescents for Attentional, Emotional, and Behavioral Self-Regulation

 , , , and
, , , and 
Abstract
:1. Introduction
2. Method
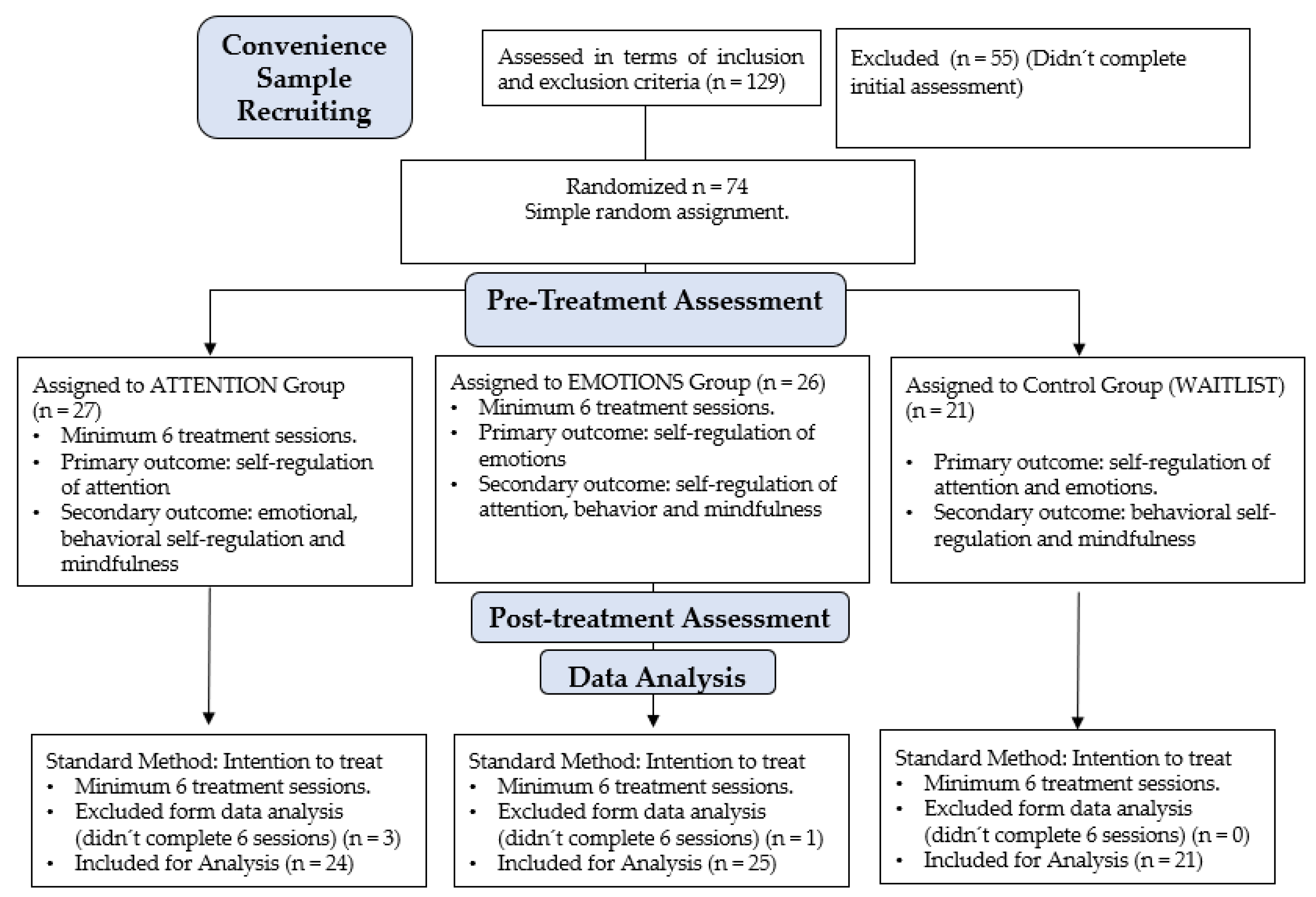
2.1. Participants
2.2. Measures
2.2.1. Child and Adolescent Mindfulness Measure, CAMM [35]
2.2.2. Difficulties in Emotion Regulation Scale, DERS [36]
2.2.3. Behavior Rating Inventory of Executive Function, BRIEF-2 Family Form [37,38]
2.2.4. Flanker Task [40,41]
2.3. Interventions
2.3.1. Intervention 1: Program Based on Mindfulness with a Focus on Attention
2.3.2. Intervention 2: Mindfulness-Based Program with a Focus on Emotions
2.4. Procedure
Data Analysis
3. Results
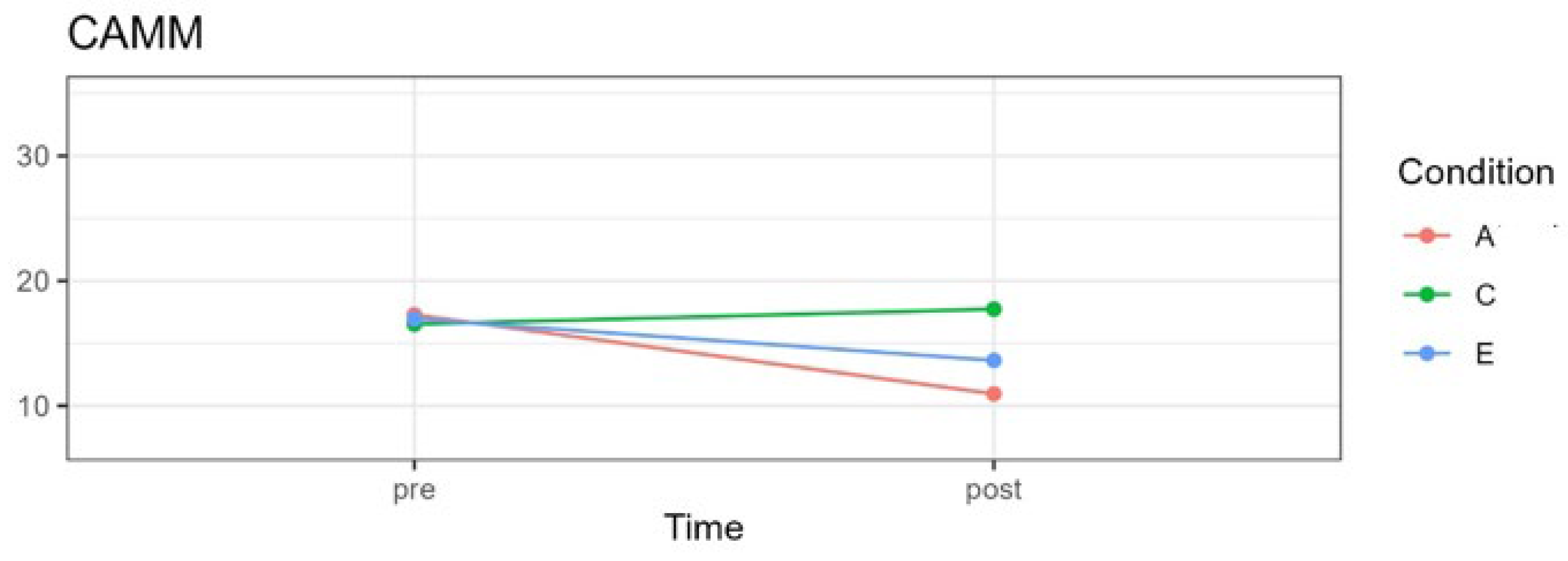
3.1. Mindfulness
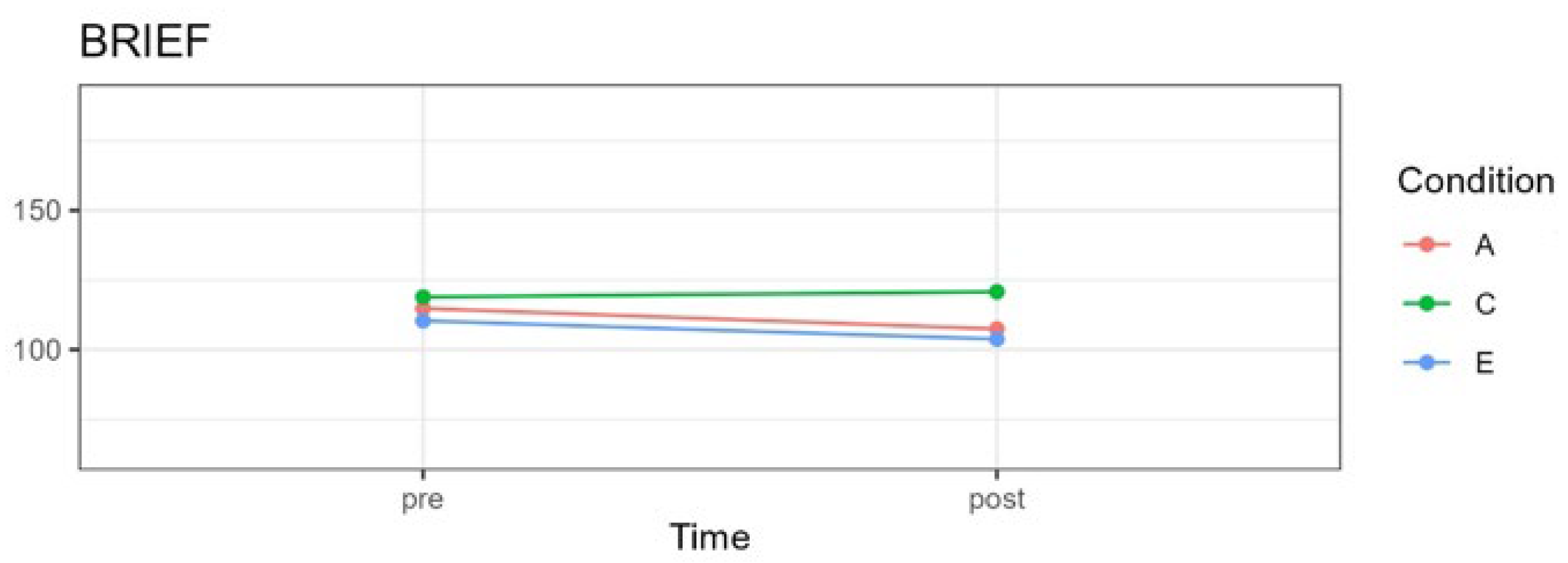
3.2. Behavioral Self-Regulation
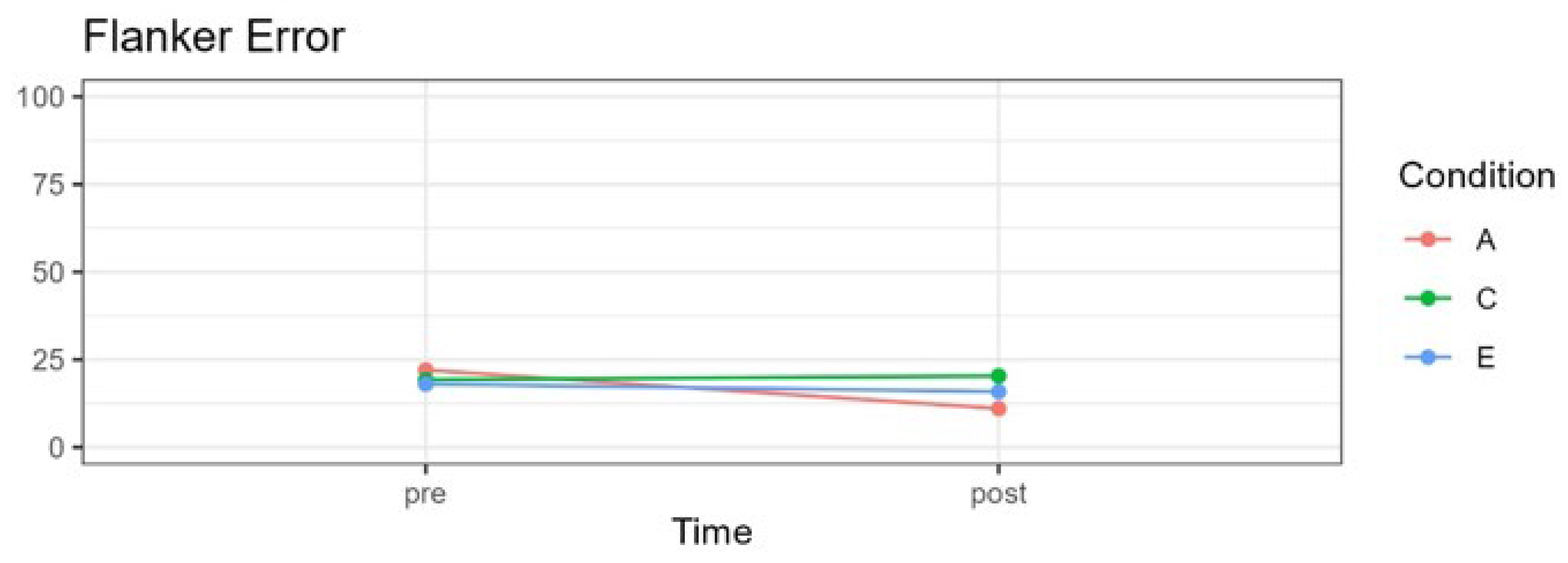
3.3. Attention Self-Regulation
3.4. Emotional Self-Regulation
4. Discussion
4.1. Mindfulness
4.2. Behavioral Self-Regulation
4.3. Attentional Self-Regulation
4.4. Emotional Self-Regulation
4.5. Limitations
4.6. Future Research
5. Conclusions
- (1)
- Results show that both interventions resulted in improvements in trait or dispositional mindfulness.
- (2)
- Both the program with a focus on attention and the program with a focus on emotions resulted in significant changes in the regulation of emotions and behavior.
- (3)
- Only children who participated in the program with a focus on attention showed a significant change in the precision of their responses, decreasing the percentage of errors for incompatible stimuli. The program with a focus on emotion did not affect attentional self-regulation.
- (4)
- Both programs examined in this study contributed to strengthening self-regulation skills of emotions and behavior in boys and girls aged between 8 and 12 years old, with the program focusing on attention also being effective in terms of attentional self-regulation.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vicente, B.; Saldivia, S.; de la Barra, F.; Melipillán, R.; Valdivia, M.; Kohn, R. Salud mental infanto-juvenil en Chile y brechas de atención sanitarias. Rev. Méd. Chile 2012, 140, 447–457. [Google Scholar] [CrossRef] [PubMed]
- Vicente, B.; Saldivia, S.; Pihán, R. Prevalencias y brechas hoy: Salud mental mañana. Acta Bioethica 2016, 22, 51–61. [Google Scholar] [CrossRef]
- Anto, S.P.; Jayan, C. Self-esteem and emotion regulation as determinants of mental health of youth. SIS J. Proj. Psychol. Ment. Health 2016, 23, 34. [Google Scholar]
- Arango, C.; Díaz-Caneja, C.M.; McGorry, P.D.; Rapoport, J.; Sommer, I.E.; Vorstman, J.A.; McDaid, D.; Marín, O.; Serrano-Drozdowskyj, E.; Freedman, R. Preventive strategies for mental health. Lancet Psychiatry 2018, 5, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Boyce, W.T. The lifelong effects of early childhood adversity and toxic stress. Pediatr. Dent. 2014, 36, 102–108. [Google Scholar] [PubMed]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; De Graaf, R.O.N.; Demyttenaere, K.; Gasquet, I.; De Girolamo, G.; Gluzman, S.; Gureje, O.Y.E.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 6, 168–176. [Google Scholar] [PubMed]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Luby, J.L.; Barch, D.; Whalen, D.; Tillman, R.; Belden, A. Association between early life adversity and risk for poor emotional and physical health in adolescence: A putative mechanistic neurodevelopmental pathway. JAMA Pediatr. 2017, 171, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A. Future directions in childhood adversity and youth psychopathology. In Future Work in Clinical Child and Adolescent Psychology; Routledge: London, UK, 2018; pp. 345–366. [Google Scholar]
- Errázuriz, P.; Valdés, C.; Vöhringer, P.A.; Calvo, E. Financiamiento de la salud mental en Chile: Una deuda pendiente. Rev. Méd. Chile 2015, 143, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; Belfer, M.; Daniels, A.; Flisher, A.; Villé, L.; Lora, A.; Saxena, S. Treated prevalence of and mental health services received by children and adolescents in 42 low-and-middle-income countries. J. Child Psychol. Psychiatry 2011, 52, 1239–1246. [Google Scholar] [CrossRef]
- Zúñiga-Fajuri, A.; Zúñiga, M. Propuestas para ampliar la cobertura de salud mental infantil en Chile. Acta Bioethica 2020, 26, 73–80. [Google Scholar] [CrossRef]
- Fourneret, P.; des Portes, V. Developmental approach of executive functions: From infancy to adolescence. Arch. Pediatr. Organe Off. Soc. Fr. Pediatr. 2017, 24, 66–72. [Google Scholar]
- McClelland, M.M.; John Geldhof, G.; Cameron, C.E.; Wanless, S.B. Development and self-regulation. In Handbook of Child Psychology and Developmental Science; Wiley: Hoboken, NJ, USA, 2015; pp. 1–43. [Google Scholar]
- McClelland, M.; Geldhof, J.; Morrison, F.; Gestsdóttir, S.; Cameron, C.; Bowers, E.; Duckworth, A.; Little, T.; Grammer, J. Self-regulation. In Handbook of Life Course Health Development; Springer: Berlin/Heidelberg, Germany, 2018; pp. 275–298. [Google Scholar]
- Palacios, X. Adolescencia:¿ una etapa problemática del desarrollo humano? Rev. Cienc. Salud 2019, 17, 5–8. [Google Scholar] [CrossRef]
- Kaunhoven, R.J.; Dorjee, D. How does mindfulness modulate self-regulation in pre-adolescent children? An integrative neurocognitive review. Neurosci. Biobehav. Rev. 2017, 74, 163–184. [Google Scholar] [CrossRef] [PubMed]
- Rueda, M.R.; Posner, M.I.; Rothbart, M.K. The development of executive attention: Contributions to the emergence of self-regulation. In Measurement of Executive Function in Early Childhood; Psychology Press: Hove, UK, 2016; pp. 573–594. [Google Scholar]
- Cavicchioli, M.; Ogliari, A.; Movalli, M.; Maffei, C. Persistent Deficits in Self-Regulation as a Mediator between Childhood Attention-Deficit/Hyperactivity Disorder Symptoms and Substance Use Disorders. Subst. Use Misuse 2022, 57, 1837–1853. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Some reflections on the origins of MBSR, skillful means, and the trouble with maps. In Mindfulness; Routledge: London, UK, 2013; pp. 281–306. [Google Scholar]
- Germer, C. What is mindfulness. Insight J. 2004, 22, 24–29. [Google Scholar]
- Burke, C.A. Mindfulness-based approaches with children and adolescents: A preliminary review of current research in an emergent field. J. Child Fam. Stud. 2010, 19, 133–144. [Google Scholar] [CrossRef]
- Klingbeil, D.A.; Renshaw, T.L.; Willenbrink, J.B.; Copek, R.A.; Chan, K.T.; Haddock, A.; Yassine, J.; Clifton, J. Mindfulness-based interventions with youth: A comprehensive meta-analysis of group-design studies. J. Sch. Psychol. 2017, 63, 77–103. [Google Scholar] [CrossRef] [PubMed]
- Klingbeil, D.A.; Fischer, A.J.; Renshaw, T.L.; Bloomfield, B.S.; Polakoff, B.; Willenbrink, J.B.; Copek, R.A.; Chan, K.T. Effects of Mindfulness-Based Interventions on Disruptive Behavior: A Meta-Analysis of Single-Case Research. Psychol. Sch. 2017, 54, 70–87. [Google Scholar] [CrossRef]
- Zoogman, S.; Goldberg, S.B.; Hoyt, W.T.; Miller, L. Mindfulness interventions with youth: A meta-analysis. Mindfulness 2015, 6, 290–302. [Google Scholar] [CrossRef]
- Felver, J.C.; Tipsord, J.M.; Morris, M.J.; Racer, K.H.; Dishion, T.J. The Effects of Mindfulness-Based Intervention on Children’s Attention Regulation. J. Atten. Disord. 2014, 21, 872–881. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, A.; Vine, V.; Curtiss, J.; Klemanski, D.H. Observing nonreactively: A conditional process model linking mindfulness facets, cognitive emotion regulation strategies, and depression and anxiety symptoms. J. Affect. Disord. 2014, 165, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.; Herwig, U.; Opialla, S.; Hittmeyer, A.; Jäncke, L.; Rufer, M.; Grosse Holtforth, M.; Brühl, A.B. Mindfulness and emotion regulation—An fMRI study. Soc. Cogn. Affect. Neurosci. 2013, 9, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Schonert-Reichl, K.A.; Smith, V.; Zaidman-Zait, A.; Hertzman, C. Promoting children’s prosocial behaviors in school: Impact of the “Roots of Empathy” program on the social and emotional competence of school-aged children. Sch. Ment. Health 2012, 4, 1–21. [Google Scholar] [CrossRef]
- Schonert-Reichl, K.A.; Oberle, E.; Lawlor, M.S.; Abbott, D.; Thomson, K.; Oberlander, T.F.; Diamond, A. Enhancing cognitive and social–emotional development through a simple-to-administer mindfulness-based school program for elementary school children: A randomized controlled trial. Dev. Psychol. 2015, 51, 52. [Google Scholar] [CrossRef] [PubMed]
- Felver; Hoyos, C.-D.; Tezanos, K.; Singh, N.N. A systematic review of mindfulness-based interventions for youth in school settings. Mindfulness 2016, 7, 34–45. [Google Scholar] [CrossRef]
- Porter, B.; Oyanadel, C.; Sáez-Delgado, F.; Andaur, A.; Peñate, W. Systematic review of mindfulness-based interventions in child-adolescent population: A developmental perspective. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1220–1243. [Google Scholar] [CrossRef] [PubMed]
- Ato, M.; López, J.J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. An. Psicol. 2013, 29, 1038–1059. [Google Scholar] [CrossRef]
- García-Rubio, C.; Rodríguez-Carvajal, R.; Langer, A.I.; Paniagua, D.; Steinebach, P.; Andreu, C.I.; Vara, M.D.; Cebolla, A. Validation of the Spanish Version of the Child and Adolescent Mindfulness Measure (CAMM) with Samples of Spanish and Chilean Children and Adolescents. Mindfulness 2019, 10, 1502–1517. [Google Scholar] [CrossRef]
- Guzmán-González, M.; Trabucco, C.; Urzúa, M.A.; Garrido, L.; Leiva, J. Validez y Confiabilidad de la Versión Adaptada al Español de la Escala de Dificultades de Regulación Emocional (DERS-E) en Población Chilena. Ter. Psicológica 2014, 32, 19–29. [Google Scholar] [CrossRef]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. Test Review Behavior Rating Inventory of Executive Function. Child Neuropsychol. 2000, 6, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.A.; Isquith, P.K.; Retzlaff, P.D.; Espy, K.A. Confirmatory Factor Analysis of the Behavior Rating Inventory of Executive Function (BRIEF) in a Clinical Sample. Child Neuropsychol. 2002, 8, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Salas, C.; Ramos-Galarza, C.; Oliva, K.; Ortega, G.A. Bifactor Modeling of the Behavior Rating Inventory of Executive Function (BRIEF) in a Chilean Sample. Percept. Mot. Ski. 2016, 122, 757–776. [Google Scholar] [CrossRef] [PubMed]
- Ridderinkhof, K.R.; Wylie, S.A.; van den Wildenberg, W.P.; Bashore, T.R.; van der Molen, M.W. The arrow of time: Advancing insights into action control from the arrow version of the Eriksen flanker task. Atten. Percept. Psychophys. 2021, 83, 700–721. [Google Scholar] [CrossRef]
- Kopp, B.; Rist, F.; Mattler, U. N200 in the flanker task as a neurobehavioral tool for investigating executive control. Psychophysiology 1996, 33, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Greco, L.A.; Baer, R.A.; Smith, G.T. Assessing mindfulness in children and adolescents: Development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol. Assess. 2011, 23, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Gustin García, M.G. Aplicación del Child and Adolescent Mindfulness Measure (CAMM) a Niños y Adolescentes Limeños: Adaptación y Evaluación del Instrumento; Universidad Antonio Ruiz de Montoya: Pueblo Libre, Peru, 2019. [Google Scholar]
- Gustin-García, M.G.; Alegre-Bravo, A.A. Validación de Child and Adolescent Mindfulness Measure en escolares de Lima, Perú. Rev. Eval. 2021, 21, 63–79. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Oyanadel, C.; Núñez, Y.; González-Loyola, M.; Jofré, I.; Peñate, W. Association of Emotion Regulation and Dispositional Mindfulness in an Adolescent Sample: The Mediational Role of Time Perspective. Children 2023, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Petersen, S.E.; Posner, M.I. The attention system of the human brain: 20 years after. Annu. Rev. Neurosci. 2012, 35, 73–89. [Google Scholar] [CrossRef] [PubMed]
- Posner, M.I.; Rothbart, M.K.; Sheese, B.E.; Voelker, V.P. Developing attention: Behavioral and brain mechanisms. Adv. Neurosci. 2014, 2014, 405094. [Google Scholar] [CrossRef] [PubMed]
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods; Sage: Newcastle-upon-Tyne, UK, 2002; Volume 1. [Google Scholar]
- Galecki, A.; Burzykowski, T. Linear Mixed-Effects Model; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Emerson, L.-M.; De Diaz, N.N.; Sherwood, A.; Waters, A.; Farrell, L. Mindfulness interventions in schools: Integrity and feasibility of implementation. Int. J. Behav. Dev. 2020, 44, 62–75. [Google Scholar] [CrossRef]
- Flook, L.; Goldberg, S.B.; Pinger, L.; Davidson, R.J. Promoting prosocial behavior and self-regulatory skills in preschool children through a mindfulness-based kindness curriculum. Dev. Psychol. 2015, 51, 44. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, A. A Still Quiet Place: A Mindfulness Program for Teaching Children and Adolescents to Ease Stress and Difficult Emotions; New Harbinger Publications: Oakland, CA, USA, 2014. [Google Scholar]
- Saltzman, A. A Still Quiet Place for Teens: A Mindfulness Workbook to Ease Stress and Difficult Emotions; New Harbinger Publications: Oakland, CA, USA, 2016. [Google Scholar]
- Saltzman, A. Still Quiet Place: Sharing mindfulness with children and adolescents. In Handbook of Mindfulness-Based Programmes; Routledge: London, UK, 2019; pp. 267–281. [Google Scholar]
- Snel, E. Tranquilos y Atentos Como una Rana: La Meditación para Niños... con Sus Padres; Editorial Kairós: Barcelona, Spain, 2013. [Google Scholar]
- Uşakli, H. Selected, adopted and implemented social-emotional learning program: The Kindness Curriculum for kids. Educ. Chall. 2021, 26, 6–14. [Google Scholar] [CrossRef]
- Fernández, T.G.; González-Pienda, J.A.; Pérez, C.R.; García, D.Á.; Pérez, L.Á. Psychometric characteristics of the BRIEF scale for the assessment of executive functions in Spanish clinical population. Psicothema 2014, 26, 47–54. [Google Scholar] [CrossRef]
- Guy, S.C.; Gioia, G.A.; Isquith, P.K. BRIEF-SR: Behavior Rating Inventory of Executive Function–Self-Report Version: Professional Manual; Psychological Assessment Resources: Lutz, FL, USA, 2004. [Google Scholar]
- Quach, D.; Jastrowski Mano, K.E.; Alexander, K. A Randomized Controlled Trial Examining the Effect of Mindfulness Meditation on Working Memory Capacity in Adolescents. J. Adolesc. Health 2016, 58, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.; Roach, A.T.; Kearney, M.A.; Zabek, F. Enhancing executive function skills in preschoolers through a mindfulness-based intervention: A randomized, controlled pilot study. Psychol. Sch. 2018, 55, 644–660. [Google Scholar] [CrossRef]
- Zelazo, P.D.; Forston, J.L.; Masten, A.S.; Carlson, S.M. Mindfulness Plus Reflection Training: Effects on Executive Function in Early Childhood. Front. Psychol. 2018, 9, 324033. [Google Scholar] [CrossRef] [PubMed]
- Lassander, M.; Hintsanen, M.; Suominen, S.; Mullola, S.; Fagerlund, Å.; Vahlberg, T.; Volanen, S.-M. The Effects of School-based Mindfulness Intervention on Executive Functioning in a Cluster Randomized Controlled Trial. Dev. Neuropsychol. 2020, 45, 469–484. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.; Seiden, D. Effects of a brief mindfulness curriculum on self-reported executive functioning and emotion regulation in Hong Kong adolescents. Mindfulness 2020, 11, 627–642. [Google Scholar] [CrossRef]
- Lemberger-Truelove, M.E.; Carbonneau, K.J.; Atencio, D.J.; Zieher, A.K.; Palacios, A.F. Self-regulatory growth effects for young children participating in a combined social and emotional learning and mindfulness-based intervention. J. Couns. Dev. 2018, 96, 289–302. [Google Scholar] [CrossRef]
- Alonso Maynar, M.; Germer, C.K. Autocompasión en Psicoterapia y el Programa Mindful Self Compassion: ¿Hacia las Terapias de Cuarta Generación? Rev. Psicoter. 2016, 27, 169–185. [Google Scholar] [CrossRef]
- Bluth, K.; Neff, K.D. New frontiers in understanding the benefits of self-compassion. Self Identity 2018, 17, 605–608. [Google Scholar] [CrossRef]
- Brito-Pons, G.; Campos, D.; Cebolla, A. Implicit or explicit compassion? Effects of compassion cultivation training and comparison with mindfulness-based stress reduction. Mindfulness 2018, 9, 1494–1508. [Google Scholar] [CrossRef]
- Germer, C.; Neff, K. Mindful Self-Compassion (MSC). In Handbook of Mindfulness-Based Programmes; Routledge: London, UK, 2019; pp. 357–367. [Google Scholar]
- Neff, K.; Knox, M.C. Self-compassion. Mindfulness Posit. Psychol. Sci. Medit. Wellbeing 2016, 37, 1–8. [Google Scholar]
- Fjell, A.M.; Walhovd, K.B.; Brown, T.T.; Kuperman, J.M.; Chung, Y.; Hagler, D.J.; Venkatraman, V.; Roddey, J.C.; Erhart, M.; McCabe, C. Multimodal imaging of the self-regulating developing brain. Proc. Natl. Acad. Sci. USA 2012, 109, 19620–19625. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Kofman, O.; Livneh, U.; Henik, A. Multidisciplinary perspectives on attention and the development of self-regulation. Prog. Neurobiol. 2007, 82, 256–286. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.-Y.; Tang, R.; Posner, M.I. Mindfulness meditation improves emotion regulation and reduces drug abuse. Drug Alcohol Depend. 2016, 163, S13–S18. [Google Scholar] [CrossRef] [PubMed]
- National Research Council; Institute of Medicine (US). Committee on the Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. In Preventing Mental, Emotional, and Behavioral Disorders among Young People: Progress and Possibilities; O’Connell, M.E., Boat, T., Warner, K.E., Eds.; National Academic Press: Washington, DC, USA, 2009. [Google Scholar]
- Dowdy, E.; Ritchey, K.; Kamphaus, R. School-based screening: A population-based approach to inform and monitor children’s mental health needs. Sch. Ment. Health 2010, 2, 166–176. [Google Scholar] [CrossRef]
- Gatica-Saavedra, M.; Vicente, B.; Rubí, P. Plan nacional de salud mental. Reflexiones en torno a la implementación del modelo de psiquiatría comunitaria en Chile. Rev. Méd. Chile 2020, 148, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Caponetto, I.; Earp, J.; Ott, M. Gamification and education: A literature review. In Proceedings of the European Conference on Games Based Learning, Berlin, Germany, 9–10 October 2014; Academic Conferences International Limited: Reading, UK, 2014; p. 50. [Google Scholar]
- Dicheva, D.; Dichev, C.; Agre, G.; Angelova, G. Gamification in education: A systematic mapping study. J. Educ. Technol. Soc. 2015, 18, 75–88. [Google Scholar]
- Nah, F.F.-H.; Zeng, Q.; Telaprolu, V.R.; Ayyappa, A.P.; Eschenbrenner, B. Gamification of education: A review of literature. In Proceedings of the HCI in Business: First International Conference, HCIB 2014, Held as Part of HCI International 2014, Heraklion, Crete, Greece, 22–27 June 2014; Proceedings 1. Springer International Publishing: New York City, USA, 2014; pp. 401–409. [Google Scholar]
- Gromala, D.; Tong, X.; Choo, A.; Karamnejad, M.; Shaw, C.D. The virtual meditative walk: Virtual reality therapy for chronic pain management. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Republic of Korea, 18–23 April 2015; pp. 521–524. [Google Scholar]
- Achenbach, T.M. Achenbach System of Empirically Based Assessment (ASEBA): Development, Findings, Theory, and Applications; University of Vermont, Research Center of Children, Youth & Families: Burlington, VT, USA, 2009. [Google Scholar]
- Achenbach, T.M.; Ivanova, M.Y.; Rescorla, L.A.; Turner, L.V.; Althoff, R.R. Internalizing/externalizing problems: Review and recommendations for clinical and research applications. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Dehnabi, A.; Radsepehr, H.; Foushtanghi, K. The effect of mindfulness-based stress reduction on social anxiety of the deaf. Ann. Trop. Med. Public Health 2017, 10. [Google Scholar]
- Nejati, V.; Amini, R.; ZabihZadeh, A.; Masoumi, M.; Maleki, G.; Shoaie, F. Mindfulness as effective factor in quality of life of blind veterans. Iran. J. War Public Health 2011, 3, 1–7. [Google Scholar]
- Soleymani, M.; Jabari, G. Evaluation of mindfulness-based cognitive therapy on the quality of life and mental health of mothers of deaf children. J. Mod. Rehabil. 2017, 11, 13–22. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Girls | Boys | |||||
|---|---|---|---|---|---|---|
| Group | n | Age (SD) | n | Age (SD) | Total N | Average Age |
| Attention | 14 | 9.66 (1.33) | 10 | 9.90 (0.88) | 24 | 9.91 |
| Emotions | 13 | 10.00 (0.60) | 12 | 9.50 (0.80) | 25 | 9.75 |
| Control | 12 | 9.08 (1.04) | 9 | 9.11 (1.05) | 21 | 9.09 |
| Total | 39 | 9.66 (1.10) | 31 | 9.51 (0.92) | 70 | 9.60 |
| Session | Mindfulness Practices | Materials |
|---|---|---|
| 1 |
|
|
| 2 |
|
|
| 3 |
|
|
| 4 |
|
|
| 5 |
|
|
| 6 |
|
|
| 7 |
|
|
| 8 |
|
|
| Session | Mindfulness Practices | Materials |
|---|---|---|
| 1 |
|
|
| 2 |
|
|
| 3 |
|
|
| 4 |
|
|
| 5 |
|
|
| 6 |
|
|
| 7 |
|
|
| 8 |
|
|
| Pre-Treatment Time | Post-Treatment Time | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Tests | Attention | Emotion | Control | Attention | Emotion | Control |
| Mindfulness | CAMM * | 17.28 | 16.94 | 16.52 | 10.95 | 13.63 | 17.73 |
| (5.81) | (4.93) | (3.76) | (3.65) | (4.69) | (4.86) | ||
| Behavior self-regulation | BRIEF-2 | 114.81 | 110.36 | 118.89 | 107.42 | 103.78 | 120.78 |
| (22.91) | (18.32) | (21.02) | (19.68) | (15.66) | (17.88) | ||
| Attention self-regulation | Flanker test | 22.02 | 18.00 | 19.25 | 11.04 | 15.87 | 20.33 |
| (14.79) | (16.50) | (14.07) | (9.44) | (16.74) | (15.96) | ||
| Emotion self-regulation | DERS | 65.71 | 70.36 | 60.05 | 52.90 | 63.26 | 64.47 |
| (15.06) | (12.46) | (11.64) | (8.67) | (14.12) | (17.06) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porter, B.; Oyanadel, C.; Betancourt, I.; Worrell, F.C.; Peñate, W. Effects of Two Online Mindfulness-Based Interventions for Early Adolescents for Attentional, Emotional, and Behavioral Self-Regulation. Pediatr. Rep. 2024, 16, 254-270. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16020022
Porter B, Oyanadel C, Betancourt I, Worrell FC, Peñate W. Effects of Two Online Mindfulness-Based Interventions for Early Adolescents for Attentional, Emotional, and Behavioral Self-Regulation. Pediatric Reports. 2024; 16(2):254-270. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16020022
Chicago/Turabian StylePorter, Bárbara, Cristian Oyanadel, Ignacio Betancourt, Frank C. Worrell, and Wenceslao Peñate. 2024. "Effects of Two Online Mindfulness-Based Interventions for Early Adolescents for Attentional, Emotional, and Behavioral Self-Regulation" Pediatric Reports 16, no. 2: 254-270. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16020022