

The Cardiovascular Event Risk Associated with Tyrosine Kinase Inhibitors and the Lipid Profile in Patients with Chronic Myeloid Leukemia
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
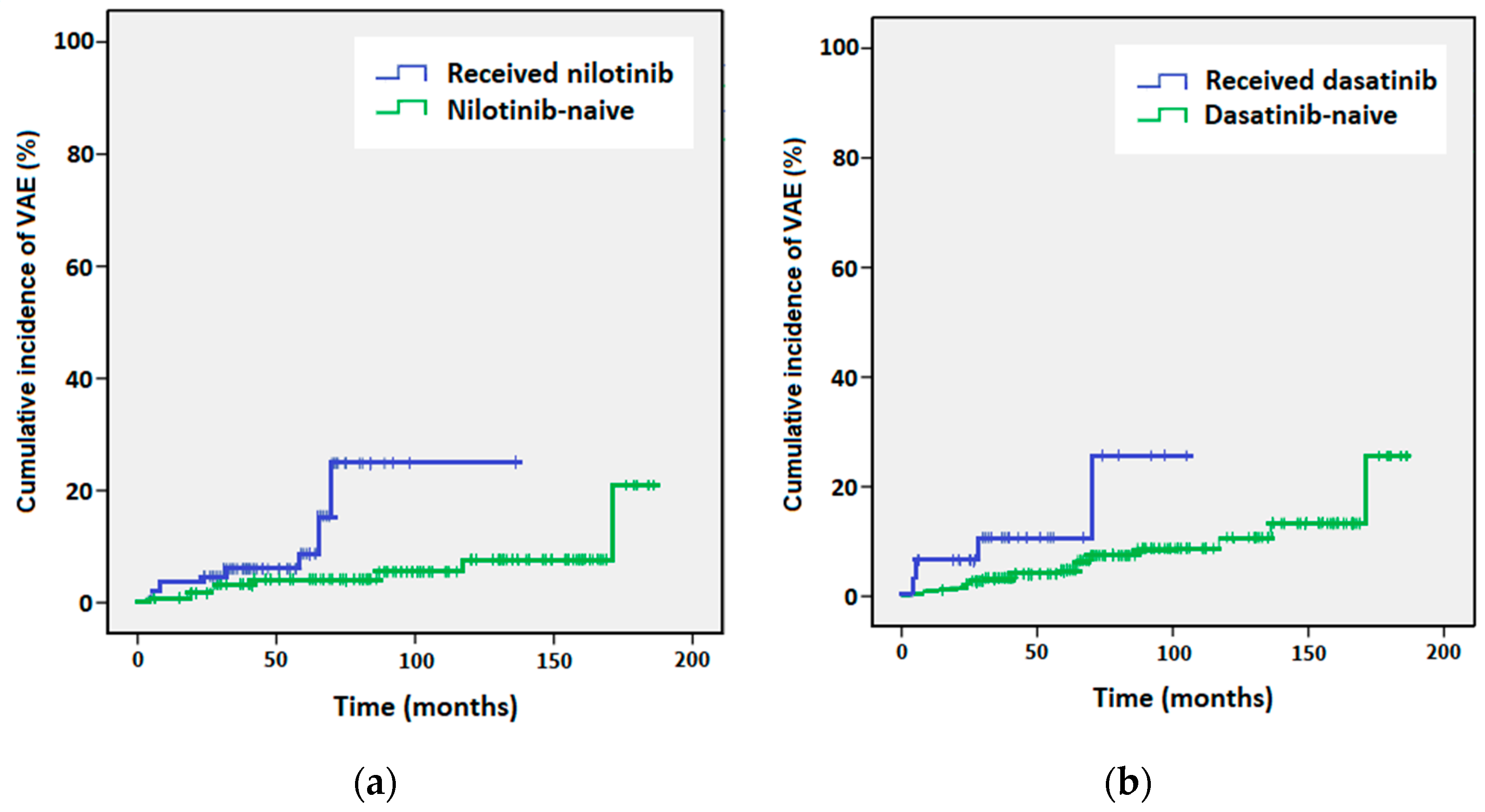
3.2. Incidence Analysis
3.3. Multivariable Logistic Regression
3.4. Biochemical Lipid Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bartram, C.R.; de Klein, A.; Hagemeijer, A.; van Agthoven, T.; Geurts van Kessel, A.; Bootsma, D.; Grosveld, G.; Ferguson-Smith, M.A.; Davies, T.; Stone, M. Translocation of c-ab1 oncogene correlates with the presence of a Philadelphia chromosome in chronic myelocytic leukaemia. Nature 1983, 306, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef] [PubMed]
- Larson, R.A.; Hochhaus, A.; Hughes, T.P.; Clark, R.E.; Etienne, G.; Kim, D.W.; Flinn, I.W.; Kurokawa, M.; Moiraghi, B.; Yu, R.; et al. Nilotinib vs. imatinib in patients with newly diagnosed Philadelphia chromosome-positive chronic myeloid leukemia in chronic phase: ENESTnd 3-year follow-up. Leukemia 2012, 26, 2197–2203. [Google Scholar] [CrossRef] [PubMed]
- Saglio, G.; Kim, D.W.; Issaragrisil, S.; le Coutre, P.; Etienne, G.; Lobo, C.; Pasquini, R.; Clark, R.E.; Hochhaus, A.; Hughes, T.P.; et al. Nilotinib versus imatinib for newly diagnosed chronic myeloid leukemia. N. Engl. J. Med. 2010, 362, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Kantarjian, H.; Shah, N.P.; Hochhaus, A.; Cortes, J.; Shah, S.; Ayala, M.; Moiraghi, B.; Shen, Z.; Mayer, J.; Pasquini, R.; et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N. Engl. J. Med. 2010, 362, 2260–2270. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Saglio, G.; Kantarjian, H.M.; Baccarani, M.; Mayer, J.; Boqué, C.; Shah, N.P.; Chuah, C.; Casanova, L.; Bradley-Garelik, B.; et al. Final 5-Year Study Results of DASISION: The Dasatinib Versus Imatinib Study in Treatment-Naïve Chronic Myeloid Leukemia Patients Trial. J. Clin. Oncol. 2016, 34, 2333–2340. [Google Scholar] [CrossRef] [PubMed]
- Giles, F.J.; le Coutre, P.D.; Pinilla-Ibarz, J.; Larson, R.A.; Gattermann, N.; Ottmann, O.G.; Hochhaus, A.; Radich, J.P.; Saglio, G.; Hughes, T.P.; et al. Nilotinib in imatinib-resistant or imatinib-intolerant patients with chronic myeloid leukemia in chronic phase: 48-month follow-up results of a phase II study. Leukemia 2013, 27, 107–112. [Google Scholar] [CrossRef]
- Shah, N.P.; Guilhot, F.; Cortes, J.E.; Schiffer, C.A.; le Coutre, P.; Brümmendorf, T.H.; Kantarjian, H.M.; Hochhaus, A.; Rousselot, P.; Mohamed, H.; et al. Long-term outcome with dasatinib after imatinib failure in chronic-phase chronic myeloid leukemia: Follow-up of a phase 3 study. Blood 2014, 123, 2317–2324. [Google Scholar] [CrossRef]
- Douglas Smith, B.; Brummendorf, T.H.; Roboz, G.J.; Gambacorti-Passerini, C.; Charbonnier, A.; Viquiera, A.; Leip, A.; Giles, F.; Ernst, T.; Hochhaus, A.; et al. Efficacy of bosutinib in imatinib-resistant vs. dasatinib/nilotinib-resistant chronic phase chronic myeloid leukemia: Results from the Phase 4 BYOND Study. Blood 2019, 134, 1650. [Google Scholar] [CrossRef]
- Grupo Español de Leucemia Mieloide Crónica (GELMC). Manual Para el Control y el Tratamiento de los Pacientes con Leucemia Mieloide Crónica [Manual for the Control and Treatment of Patients with Chronic Myeloid Leukemia] (Spanish); Edición 2020; MFAR, Ed.; GELMC: Barcelona, Brazil, 2020. [Google Scholar]
- Hantschel, O.; Rix, U.; Superti-Furga, G. Target spectrum of the BCR-ABL inhibitors imatinib, nilotinib and dasatinib. Leuk. Lymphoma 2008, 49, 615–619. [Google Scholar] [CrossRef]
- Steegmann, J.L.; Baccarani, M.; Breccia, M.; Casado, L.F.; García-Gutiérrez, V.; Hochhaus, A.; Kim, D.W.; Kim, T.D.; Khoury, H.J.; Le Coutre, P.; et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia 2016, 30, 1648–1671. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.A.; Garcia Gonzalez, A.G.; Ault, P.; Mendoza, T.R.; Sailors, M.L.; Williams, J.L.; Huang, F.; Nazha, A.; Kantarjian, H.M.; Cleeland, C.S.; et al. Measuring the symptom burden associated with the treatment of chronic myeloid leukemia. Blood 2013, 122, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Valent, P.; Hadzijusufovic, E.; Schernthaner, G.H.; Wolf, D.; Rea, D.; le Coutre, P. Vascular safety issues in CML patients treated with BCR/ABL1 kinase inhibitors. Blood 2015, 125, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.D.; Rea, D.; Schwarz, M.; Grille, P.; Nicolini, F.E.; Rosti, G.; Levato, L.; Giles, F.J.; Dombret, H.; Mirault, T.; et al. Peripheral artery occlusive disease in chronic phase chronic myeloid leukemia patients treated with nilotinib or imatinib. Leukemia 2013, 27, 1316–1321. [Google Scholar] [CrossRef]
- Le Coutre, P.; Rea, D.; Abruzzese, E.; Dombret, H.; Trawinska, M.M.; Herndlhofer, S.; Dörken, B.; Valent, P. Severe peripheral arterial disease during nilotinib therapy. J. Natl. Cancer Inst. 2011, 103, 1347–1348. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Kim, D.W.; Pinilla-Ibarz, J.; le Coutre, P.; Paquette, R.; Chuah, C.; Nicolini, F.E.; Apperley, J.F.; Khoury, H.J.; Talpaz, M.; et al. A phase 2 trial of ponatinib in Philadelphia chromosome-positive leukemias. N. Engl. J. Med. 2013, 369, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Stuckey, R.; Segura-Díaz, A.; Sáez Perdomo, M.N.; Pérez Encinas, M.M.; González San Miguel, J.D.; Florido, Y.; Sánchez-Sosa, S.; López-Rodríguez, J.F.; Bilbao-Sieyro, C.; Gómez-Casares, M.T. Presence of Myeloid Mutations in Patients with Chronic Myeloid Leukemia Increases Risk of Cardiovascular Event on Tyrosine Kinase Inhibitor Treatment. Cancers 2023, 15, 3384. [Google Scholar] [CrossRef]
- Giles, F.J.; Rea, D.; Rosti, G.; Cross, N.C.P.; Steegmann, J.L.; Griskevicius, L.; le Coutre, P.; Coriu, D.; Petrov, L.; Ossenkoppele, G.J.; et al. Impact of age on efficacy and toxicity of nilotinib in patients with chronic myeloid leukemia in chronic phase: ENEST1st subanalysis. J. Cancer Res. Clin. Oncol. 2017, 143, 1585–1596. [Google Scholar] [CrossRef]
- Hochhaus, A.; Saglio, G.; Hughes, T.P.; Larson, R.A.; Kim, D.W.; Issaragrisil, S.; le Coutre, P.D.; Etienne, G.; Dorlhiac-Llacer, P.E.; Clark, R.E.; et al. Long-term benefits and risks of frontline nilotinib vs. imatinib for chronic myeloid leukemia in chronic phase: 5-year update of the randomized ENESTnd trial. Leukemia 2016, 30, 1044–1054. [Google Scholar] [CrossRef]
- Cortes, J.E.; Kim, D.W.; Kantarjian, H.M.; Brümmendorf, T.H.; Dyagil, I.; Griskevicius, L.; Malhotra, H.; Powell, C.; Gogat, K.; Countouriotis, A.M.; et al. Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: Results from the BELA trial. J. Clin. Oncol. 2012, 30, 3486–3492. [Google Scholar] [CrossRef]
- World Health Organization. WHO Consultation on Obesity; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Selvin, E.; Erlinger, T.P. Prevalence of and risk factors for peripheral arterial disease in the United States: Results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation 2004, 110, 738–743. [Google Scholar] [CrossRef]
- Aichberger, K.J.; Herndlhofer, S.; Schernthaner, G.H.; Schillinger, M.; Mitterbauer-Hohendanner, G.; Sillaber, C.; Valent, P. Progressive peripheral arterial occlusive disease and other vascular events during nilotinib therapy in CML. Am. J. Hematol. 2011, 86, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Caocci, G.; Mulas, O.; Abruzzese, E.; Luciano, L.; Iurlo, A.; Attolico, I.; Castagnetti, F.; Galimberti, S.; Sgherza, N.; Bonifacio, M.; et al. Arterial occlusive events in chronic myeloid leukemia patients treated with ponatinib in the real-life practice are predicted by the Systematic Coronary Risk Evaluation (SCORE) chart. Hematol. Oncol. 2019, 37, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Di Lisi, D.; Madaudo, C.; Alagna, G.; Santoro, M.; Rossetto, L.; Siragusa, S.; Novo, G. The new HFA/ICOS risk assessment tool to identify patients with chronic myeloid leukaemia at high risk of cardiotoxicity. ESC Heart Fail. 2022, 9, 1914–1919. [Google Scholar] [CrossRef]
- Fujioka, I.; Takaku, T.; Iriyama, N.; Tokuhira, M.; Kimura, Y.; Sato, E.; Ishikawa, M.; Nakazato, T.; Sugimoto, K.J.; Fujita, H.; et al. Features of vascular adverse events in Japanese patients with chronic myeloid leukemia treated with tyrosine kinase inhibitors: A retrospective study of the CML Cooperative Study Group database. Ann. Hematol. 2018, 97, 2081–2088. [Google Scholar] [CrossRef]
- Rea, D.; Mirault, T.; Cluzeau, T.; Gautier, J.F.; Guilhot, F.; Dombret, H.; Messas, E. Early onset hypercholesterolemia induced by the 2nd-generation tyrosine kinase inhibitor nilotinib in patients with chronic phase-chronic myeloid leukemia. Haematologica 2014, 99, 1197–1203. [Google Scholar] [CrossRef]
- Gottardi, M.; Manzato, E.; Gherlinzoni, F. Imatinib and hyperlipidemia. N. Engl. J. Med. 2005, 353, 2722–2723. [Google Scholar] [CrossRef]
- Breccia, M.; Colafigli, G.; Molica, M.; Alimena, G. Cardiovascular risk assessments in chronic myeloid leukemia allow identification of patients at high risk of cardiovascular events during treatment with nilotinib. Am. J. Hematol. 2015, 90, E100–E101. [Google Scholar] [CrossRef]
- Rea, D.; Mirault, T.; Raffoux, E.; Boissel, N.; Andreoli, A.L.; Rousselot, P.; Dombret, H.; Messas, E. Usefulness of the 2012 European CVD risk assessment model to identify patients at high risk of cardiovascular events during nilotinib therapy in chronic myeloid leukemia. Leukemia 2015, 29, 1206–1209. [Google Scholar] [CrossRef]
- García-Gutiérrez, V.; Jiménez-Velasco, A.; Gómez-Casares, M.T.; Sánchez-Guijo, F.; López-Sendón, J.L.; Steegmann Olmedillas, J.L. Cardiovascular management of patients with chronic myeloid leukemia from a multidisciplinary per-spective, and proposing action protocol by consensus meeting. Med. Clin. 2016, 146, 561.e1–561.e8. [Google Scholar]
- Mauro, M.J. Lifelong TKI therapy: How to manage cardiovascular and other risks. Hematol. Am. Soc. Hematol. Educ. Program 2021, 2021, 113–121. [Google Scholar]
- Stuckey, R.; López-Rodríguez, J.F.; Sánchez-Sosa, S.; Segura-Díaz, A.; Sánchez-Farías, N.; Bilbao-Sieyro, C.; Gómez-Casares, M.T. Predictive indicators of successful tyrosine kinase inhibitor discontinuation in patients with chronic myeloid leukemia. World J. Clin. Oncol. 2020, 11, 996–1007. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Gender | Age (Years) | Adverse Event | Treatment Group | Months on TKI to Onset | Dose at Onset | Received NIL | CVRF at Baseline |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 61 | PAOD with ischemic ulceration | First-line IMA (I) | 26 | IMA at 400 mg/24 h | No | DM, AHT |
| 2 | M | 86 | Intestinal occlusion with ischemic origin | First-line IMA (I) | 18 | IMA at 200 mg/24 h | No | Smoker, AHT |
| 3 | F | 70 | CVA | First-line IMA (I) | 136 | IMA at 400 mg/24 h | No | DM, AHT, hyperlipidemia |
| 4 | M | 64 | Acute myocardial infarction | First-line IMA (I) | 42 | IMA at 400 mg/24 h | No | DM, hyperlipidemia, smoker, ischemic cardiomyopathy |
| 5 | F | 68 | CVA | First-line IMA (I) | 87 | IMA at 400 mg/24 h | No | Smoker, AHT, hyperlipidemia |
| 6 | M | 86 | Lower limb amputation | First-line IMA (I) | 117 | IMA at 400 mg/24 h | No | Smoker, hyperlipidemia, acute myocardial infarction |
| 7 | M | 83 | PAOD | First-line IMA (I) | 171 | IMA at 100 mg/24 h | No | AHT |
| 8 | M | 77 | Coronary artery ischemic cardiomyopathy | First-line IMA (I) | 3 | IMA at 400 mg/24 h | No | DM, ex-smoker, AHT, hyperlipidemia |
| 9 | F | 74 | AION | First-line NIL (II) | 31 | NIL at 600 mg/24 h | Yes | DM, AHT |
| 10 | F | 67 | Unstable angina | First-line NIL (II) | 65 | NIL at 300 mg/24 h | Yes | DM, AHT |
| 11 | M | 65 | Intermittent claudication | First-line NIL (II) | 23 | NIL at 400 mg/24 h | Yes | Smoker, AHT, CVA |
| 12 | M | 72 | CVA | First-line DAS (III) | 28 | DAS at 100 mg/24 h | No | DM, ex-smoker, AHT |
| 13 | F | 80 | CVA | First-line IMA and second-line NIL (IV) | 65 | NIL at 600 mg/24 h | Yes | DM, ex-smoker, AHT, acute myocardial infarction |
| 14 | F | 86 | Toe amputation | First-line IMA and second-line NIL (IV) | 58 | NIL at 800 mg/24 h | Yes | DM, AHT |
| 15 | M | 59 | Acute myocardial infarction | First-line IMA and second-line NIL (IV) | 8 | NIL at 600 mg/24 h | Yes | DM, AHT, smoker, hyperlipidemia |
| 16 | F | 56 | Intermittent claudication | First-line IMA and second-line NIL (IV) | 70 | NIL at 600 mg/24 h | Yes | DM, AHT |
| 17 | F | 62 | CVA | Three treatment lines with first-line IMA (VIII) | 70 | DAS at 50 mg/24 h | Yes | DM, AHT |
| 18 | F | 73 | Lower limb amputation | Three treatment lines with first-line IMA (VIII) | 5 | NIL at 600 mg/24 h | Yes | DM, AHT |
| 19 | M | 50 | AION | Three treatment lines with first-line IMA (VIII) | 0.3 | IMA at 400 mg/24 h | Yes | Ex-smoker, AHT |
| Cohorts | Patients with VAE | Patients without VAE | Total | % |
|---|---|---|---|---|
| Nilotinib-naïve | 9 | 117 | 126 | 7.1 |
| Patients who received nilotinib | 10 | 74 | 84 | 11.9 |
| Total | 19 | 191 | 210 | |
| Dasatinib-naïve | 16 | 165 | 181 | 8.8 |
| Patients who received dasatinib | 3 | 26 | 29 | 10.3 |
| Total | 19 | 191 | 210 | |
| First-line imatinib (I) | 8 | 101 | 109 | 7.3 |
| First-line nilotinib (II) | 3 | 34 | 37 | 8.1 |
| First-line dasatinib (III) | 1 | 7 | 8 | 12.5 |
| First-line imatinib with second-line nilotinib (IV) | 4 | 28 | 32 | 12.5 |
| First-line imatinib with second-line dasatinib (V) | 0 | 8 | 8 | 0 |
| Two 2G-TKI lines (VI) | 0 | 3 | 3 | 0 |
| First-line 2G-TKI with second-line imatinib (VII) | 0 | 3 | 3 | 0 |
| Three lines of treatment with first-line imatinib (VIII) | 3 | 7 | 10 | 30.0 |
| Total | 19 | 191 | 210 |
| Treatment Group | Risk Factor | Effect | HR | 95% CI |
|---|---|---|---|---|
| Nilotinib-naïve | FRS | 10–20 vs. ≤10 | 7.75 | 2.20–26.37 |
| vs. nilotinib | FRS | ≥20 vs. ≤10 | 5.75 | 1.38–23.98 |
| Prior VAE | Yes vs. no | 2.71 | 0.77–9.48 | |
| Cohort | Nilotinib vs. nilotinib-naïve | 2.34 | 0.83–5.57 | |
| Dasatinib-naïve | FRS | 10–20 vs. ≤10 | 6.87 | 1.99–23.61 |
| vs. dasatinib | FRS | ≥20 vs. ≤10 | 5.70 | 1.33–24.50 |
| Prior VAE | Yes vs. no | 3.04 | 0.86–10.70 | |
| Cohort | Dasatinib vs. dasatinib-naïve | 2.49 | 0.67–9.23 |
| Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|
| mg/dL | I | II | III | IV | V | VI | VII | VIII |
| TC Dx (range) | 175 (63–326) | 190 (99–265) | 151 * (85–243) | 168 ** (88–278) | 159 (132–207) | 141 (109–158) | 198 (142–274) | 156 * (92–227) |
| TC (range) | 167 (76–288) | 195 (126–286) | 162 * (118–203) | 188 ** (91–264) | 219 (182–248) | 172 (164–188) | 202 (131–285) | 193 * (164–254) |
| HDL Dx (range) | 40 * (21–75) | 42 ** (21–66) | - | 45 ** (17–102) | 44 (23–171) | - | 34 ** (31–37) | 38 (25–57) |
| HDL (range) | 45 * (18–83) | 54 ** (35–130) | - | 56 ** (34–93) | 52 (35–64) | - | 67 ** (41–78) | 52 (35–74) |
| TG Dx (range) | 179 ** (12–814) | 161 * (41–689) | 135 (97–218) | 160 (37–510) | 427 ** (83–1024) | 120 (75–124) | 142 (114–170) | 145 (90–268) |
| TG (range) | 132 ** (29–367) | 109 * (45–286) | 103 (68–254) | 126 (31–471) | 187 ** (89–338) | 124 (94–147) | 145 (65–225) | 121 (56–166) |
| LDL Dx ((range) | 101 (9–237) | 105 (43–165) | - | 102 (22–196) | 67 ** (46–114) | - | 96 (78–113) | 98 (49–136) |
| LDL (range) | 90 (20–227) | 116 (49–184) | - | 116 (22–181) | 134 ** (107–149) | - | 79 (161–199) | 117 (97–167) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saez Perdomo, M.N.; Stuckey, R.; González-Pérez, E.; Sánchez-Sosa, S.; Estupiñan-Cabrera, P.; Lakhwani Lakhwani, S.; González San Miguel, J.D.; Hernanz Soler, N.; Gordillo, M.; González Brito, G.; et al. The Cardiovascular Event Risk Associated with Tyrosine Kinase Inhibitors and the Lipid Profile in Patients with Chronic Myeloid Leukemia. Hematol. Rep. 2024, 16, 140-150. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep16010015
Saez Perdomo MN, Stuckey R, González-Pérez E, Sánchez-Sosa S, Estupiñan-Cabrera P, Lakhwani Lakhwani S, González San Miguel JD, Hernanz Soler N, Gordillo M, González Brito G, et al. The Cardiovascular Event Risk Associated with Tyrosine Kinase Inhibitors and the Lipid Profile in Patients with Chronic Myeloid Leukemia. Hematology Reports. 2024; 16(1):140-150. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep16010015
Chicago/Turabian StyleSaez Perdomo, María Nieves, Ruth Stuckey, Elena González-Pérez, Santiago Sánchez-Sosa, Paula Estupiñan-Cabrera, Sunil Lakhwani Lakhwani, José David González San Miguel, Nuria Hernanz Soler, Marina Gordillo, Gloria González Brito, and et al. 2024. "The Cardiovascular Event Risk Associated with Tyrosine Kinase Inhibitors and the Lipid Profile in Patients with Chronic Myeloid Leukemia" Hematology Reports 16, no. 1: 140-150. https://0-doi-org.brum.beds.ac.uk/10.3390/hematolrep16010015