
Review of Bone Conduction Hearing Devices

Department of Otolaryngology—Head and Neck Surgery, University of Michigan, Ann Arbor, MI 48109, USA
*
Author to whom correspondence should be addressed.
Audiol. Res. 2021, 11(2), 207-219; https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020019
Submission received: 12 March 2021
/
Revised: 30 April 2021
/
Accepted: 6 May 2021
/
Published: 18 May 2021
(This article belongs to the Special Issue Bone and Cartilage Conduction)
Abstract
:Bone conduction is an efficient pathway of sound transmission which can be harnessed to provide hearing amplification. Bone conduction hearing devices may be indicated when ear canal pathology precludes the use of a conventional hearing aid, as well as in cases of single-sided deafness. Several different technologies exist which transmit sound via bone conduction. Here, we will review the physiology of bone conduction, the indications for bone conduction amplification, and the specifics of currently available devices.
1. Introduction
The concept of bone conduction hearing, the phenomenon through which a vibrating object can transmit sound, was first described in writing in the 1500s and credited to Girolamo Cardano [1]. Rudimentary devices such as a rod or spear were initially utilized as assistive devices for those with hearing loss by providing a route for vibrations to reach the listener. As technology advanced and the carbon microphone was developed in the early 1900s, bone conduction devices designed to convert sounds into mechanical signals that vibrate the mastoid bone were created. Early devices were held in place with a headband or eyeglasses and proved to be beneficial despite the cumbersome design and inefficient sound transmission. These early investigations paved the way for the development of modern bone-anchored hearing aids surgically implanted into the temporal bone. In 1977, Anders Tjellström and his colleagues in Sweden were the first to implant a percutaneous titanium device utilizing an osseointegrated screw [2]. The concept of osseointegration, direct contact between living osteocytes and the titanium implant, was developed by Brånemark and initially utilized for dental implants [3]. The first bone-anchored hearing device became widely commercially available in the 1980s, and since that time, patients with conductive hearing loss (CHL), mixed hearing loss (MHL), and unilateral hearing loss or single-sided deafness (SSD) have benefitted from these devices [4]. This review aims to provide an overview of bone conduction hearing physiology and the currently available bone conduction hearing devices including the indications, fitting range, benefits, and drawbacks of each.
2. Bone Conduction Physiology
Multiple physiologic mechanisms contribute to bone conduction hearing. Put simply, sound energy is transmitted from vibrations in the skull to the cochlea, which ultimately results in wave propagation along the basilar membrane and stimulation of the cochlear nerve—the same endpoint as air conduction hearing [5]. There is ongoing investigation to fully describe the mechanisms by which bone conduction hearing occurs and the relative contributions of each pathway. Five major pathways were well summarized by Stenfelt and Goode in 2005 [6]. In their review of previously published data and their own findings, they describe (1) sound radiation to the external ear canal, (2) middle ear ossicle inertia, (3) inertia of cochlear fluids, (4) compression of the cochlear walls (or inner ear compression), and (5) pressure transmission from cerebrospinal fluid (CSF) as the principal contributors to bone conduction. Inertia of cochlear fluids is felt to be the most important contributor [6].
Bone conduction hearing aids take advantage of the above mechanisms by converting sound energy into skull vibrations. Since the initial work by Tjellström [2] and his colleagues, there have been numerous commercial devices introduced, including surgically implanted and extrinsically applied devices. These devices are intended to assist with hearing rehabilitation for patients with conductive or mixed hearing loss who are unable to utilize conventional air conduction hearing aids or for patients with single-sided deafness. The ability to use conventional, transcanal devices may be limited by recurrent infections such as chronic otitis externa, prior surgical intervention and altered anatomy, microtia or anotia, canal atresia or stenosis, or other anatomic constraints. In the single-sided deafness population, bone conduction devices route signals transcranially to the contralateral, normal hearing cochlea.
When choosing a bone conduction device, many factors must be considered. Each patient has unique needs which are related to their degree and type of hearing impairment, anatomy, vocational or educational needs, and personal preferences. Finding this information in a consolidated location can be challenging for patients and providers. The goal of this review is to provide an overview of the current device landscape including the hearing losses best treated by each device, surgical and nonsurgical advantages and disadvantages for each class of devices, magnetic resonance imaging (MRI) compatibility, processor characteristics, wireless connectivity, and available accessories. The following description of devices includes products currently available and utilized in the United States. While meant to be inclusive of all manufacturers and products, devices in the ever-evolving landscape may have been inadvertently excluded or developed following the preparation of this review.
3. Currently Available Devices
3.1. Surgically Implanted Devices
Surgically implanted bone conduction devices convert acoustic sound waves into mechanical vibration, which is conducted to the inner ear via direct contact with the skull. These can be classified broadly into percutaneous and transcutaneous devices based on the presence or absence of a skin-penetrating abutment. The transcutaneous devices can be further classified into active and passive implants. Passive transcutaneous devices have an implanted portion of the device in direct connection with the skull and a separate, external portion held in place magnetically which drives vibration through the skin to the implanted device. In a passive system, vibration occurs at the level of the external processor, and vibrations are transmitted transcutaneously to the implanted device. Active transcutaneous devices contain an external microphone and processor which send electronic signals to an implanted, vibrating device in direct contact with the skull. With an active system, the external processor is static and transmits electronic signals. Vibration occurs at the level of the implanted device only. Currently available devices including indications for the selection of each, benefits, and drawbacks will be discussed.
3.1.1. Percutaneous Devices
Direct contact with the skull affords a meaningful advantage for percutaneous devices over passive transcutaneous devices. Passive transcutaneous devices rely on vibratory signal delivery through the skin and are subject to signal attenuation up to 20 dB, especially at high frequencies [7]. The direct connection of the percutaneous devices allows for efficient signal transmission at all frequencies without skin and soft tissue impedance. Surgical insertion of percutaneous devices is performed under local or general anesthesia through a variety of skin incisions [8]. Single-stage procedures are now standardly utilized except in situations with concern for poor wound healing or poor bone mineralization in which a two-stage operation may be considered. Traditionally, the sound processor is activated and loaded onto the abutment three months post-operatively, but the recent literature has examined the role for earlier activation at one to two weeks, or even one day post-operatively without sacrificing implant stability [9,10,11].
The most significant disadvantage of percutaneous implants is the potential for adverse skin reactions, device extrusion, and the need for revision surgery. The reported complication rate varies widely and appears to be influenced by the surgical technique, surgeon experience, patient age, and patient factors predisposing to infection or poor wound healing. Surgery for the placement of a percutaneous abutment was often performed with skin grafting in the past; however, skin grafting is no longer performed regularly which has resulted in overall improved cosmesis with fewer graft complications. Adverse skin reactions continue to be the most common complication of percutaneous devices, and can be categorized using the Holgers classification, a scale from zero to four described in Table 1 [12]. A 2016 systematic review published by Mohamad et al. included 30 published studies and cites a skin complication rate ranging from 9.4 to 84% [13]. A 2013 meta-analysis by Kiringoda and Lustig included 2310 implants and cited a rate of grade 2 or higher skin complications ranging from 2.4 to 38.1% [14]. The rate of revision surgery ranged from 1.7 to 34.5% in adult or mixed populations and 0 to 44.4% in pediatric populations [14].
Currently available percutaneous bone conduction devices include the Oticon Ponto System (Oticon Medical AB, Askim, Sweden) [15] and the CochlearTM Baha® Connect System (Cochlear Bone-Anchored Solutions AB, Mölnlycke, Sweden) [16,17]. In general, these devices consist of an osseointegrated implant (screw), skin penetrating abutment, and an external sound processor. The implant and abutment may be coupled and implanted together. The devices are recommended for patients with MHL, CHL, or SSD. The degree of accepted sensorineural hearing loss varies depending on the power of the processor. In patients with a purely conductive hearing loss, those with an air–bone gap of at least 30 dB are more likely to benefit from a bone-anchored device compared to a traditional air conduction aid [18]. Patients with SSD should have a pure tone average (PTA) of better than or equal to 20 dB hearing level (HL) in the contralateral, normal hearing ear.
The Oticon Ponto became commercially available in 2009. The currently utilized implant is a 4.5-mm-wide, 6 mm long, titanium screw with an abutment [19]. Currently available processors include the Ponto 3 and Ponto 4 series devices. The Ponto 3 has three versions: Ponto 3, Ponto 3 Power, and Ponto 3 SuperPower. These processors are intended for patients with bone conduction hearing thresholds up to 45 dB HL, 55 dB HL, and 65 dB HL, respectively (Table 2; Figure 1). The Ponto 4 is a smaller device and suitable for bone conduction hearing thresholds up to 45 dB HL (Table 2; Figure 1) [15].
The CochlearTM Baha® Connect System utilizes the BI300, a titanium osseointegrated implant which is available in 3- or 4-mm lengths. The percutaneous abutment, the BA400, is hydroxyapatite-coated and is available in 6-, 8-, 10-, 12-, and 14-mm lengths to accommodate a range of soft tissue thickness [32]. The currently available series includes the Baha® 5, Baha® 5 Power, and the Baha® 5 SuperPower sound processors. These devices are intended for patients with bone conduction hearing thresholds up to 45 dB HL, 55 dB HL, and 65 dB HL, respectively (Table 2; Figure 1) [17]. To achieve a higher output, the Baha®5 SuperPower has a behind-the-ear component to allow for the physical separation of the actuator from the microphone [17]. The Baha® 6 Max was recently FDA-approved and suitable for bone conduction hearing thresholds up to 55dB HL and is anticipated to be commercially available soon (Table 2; Figure 1) [16].
The SuperPower processors for the Ponto and Baha® systems each provide powerful processors intended for patients with bone conduction hearing thresholds up to 65 dB HL. The systems have some differences that impact the fitting and use of the processors. The Ponto 3 SuperPower is one piece and less bulky than the Baha® SuperPower processor [15,17]. Feedback may be harder to control due to the inability to separate the actuator from the microphone. In contrast, the Baha® 5 SuperPower system allows for the separation of the actuator from the microphone and can be worn in several configurations for even greater separation if feedback or physical placement becomes an issue [15]. This system is larger, with two pieces, and bulkier than the Ponto 3 SuperPower device. Placement of the larger device may be challenging in patients who were initially implanted in anticipation of a standard processor but have converted to a SuperPower processor to address the worsening of sensorineural hearing. The implant placement in these patients may not be ideal to accommodate the bulkier SuperPower processor. The Baha® 5 SuperPower processor uses rechargeable batteries similar to a cochlear implant (Table 3) [17]. Available accessories and streaming capabilities are listed in Table 4.
3.1.2. Passive Transcutaneous Devices
Transcutaneous systems were designed to avoid the cosmetic concerns and skin complications associated with percutaneous devices while still delivering adequate sound transmission. In the transcutaneous systems, a titanium implant is placed directly in the skull in the same manner as the percutaneous devices. A magnet is attached to this implant, and the skin is closed over the top of the implant, avoiding a percutaneous component. Once the incision has healed and osseointegration has occurred, the external device is then activated. The external device is retained via attraction to the internal magnet and vibrates in response to sound inputs. The vibratory force then passes through the intervening skin and soft tissue to reach the internal magnet and implant which allow the transmission of the vibration to the skull.
While skin complications are less common than those seen with percutaneous devices, the magnetic force required to hold the external device in place and effectively transmit sound in transcutaneous systems can lead to pain and irritation of the intervening skin and soft tissue. When this occurs, the magnet strength can be reduced to decrease the amount of pressure applied to the skin, and users may be instructed to reduce daily wearing time or avoid using their device altogether until symptoms improve. If the amount of pressure applied is greater than the patient’s capillary pressure, the skin may have inadequate blood supply and necrosis can occur [33]. A systematic review by Cooper et al. reported a 13.1% rate of minor soft tissue complications which resolved spontaneously or with use of a weaker magnet [34]. A grading system comparable to the Holgers scale for percutaneous implants has not been established; thus, reporting and comparing skin complications is challenging [12]. The rate of major complications, defined as complications requiring active management, such as post-operative seroma, hematoma, wound infections, skin ulcerations, and dehiscence, was 5.2% in the same systematic review [34].
The Baha® Attract System (Cochlear Bone-Anchored Solutions AB, Mölnlycke, Sweden) [35] and Alpha 2 MPO (formerly SOPHONOTM) system (Medtronic, Dublin, Ireland) [23] are the available passive transcutaneous devices. Both devices are intended for the treatment of CHL, MHL, or SSD with normal contralateral hearing. While auditory outcomes have shown significant improvement compared to unaided conditions, signal attenuation occurs due to signal loss during transmission through the skin and soft tissues [36]. This attenuation is most apparent at high frequencies and may be as high as 25 dB at 6000 to 8000 Hz higher frequencies when compared to percutaneous devices [37,38].
The Baha® Attract uses the same BI300 implant as the percutaneous Baha® Connect. During insertion of the device, bone polishing is performed if needed to accommodate the attachment of the BIM400 implant magnet to the BI300 without the magnet making direct contact to the bone [35]. The thickness of the skin flap over the magnet must be 6mm or less, which at times may require soft tissue reduction [35]. The Baha® Attract utilizes the same external processors as the Baha® Connect intended for use with the same bone conduction hearing thresholds previously listed (Table 2; Figure 1) [16,17]. The external processors are attached to a magnet rather than directly articulating to the percutaneous post. Once adequate healing and osseointegration have taken place, the external sound processor and magnet are applied and activated. Users are instructed to begin by wearing the device a few hours a day and slowly increase usage over time to avoid skin irritation and limit discomfort. The application of a SoftWearTM pad as a barrier between the skin and device is recommended by the manufacturer [39]. Six magnets of increasing strength are available to accommodate for variable soft tissue thickness, overlying hair, and patient comfort [39]. Since the Baha® Attract and Connect devices use the universal BI300 implant, it is possible to convert from a Baha® Connect to a Baha® Attract device, though the skin at the previous abutment site must be healed and healthy prior to conversion [40,41]. The Baha® Attract is MRI compatible at 1.5 Tesla with the internal magnet in place. A sizeable area of artifact will be present on the MRI, which is significantly larger than the degree of artifact with percutaneous devices. The magnet may be surgically removed if a higher strength MRI is required or if the resultant artifact obscures critical image sequences (Table 3) [24]. Available accessories and streaming capabilities are listed in Table 4.
The Alpha 2 MPO implant system consists of two internal magnets hermitically sealed in a titanium case. This device is designed to sit within shallow bone beds which are drilled based on manufacturer recommendations. The Alpha 2 MPO device is then attached to the skull with five screws [34,37]. The Alpha 2 MPO ePlusTM sound processor is then applied and drives vibrations through the skin and soft tissue using transcutaneous energy transfer or TETTM. The device is approved for patients with up to a 45 dB hearing loss with ideal candidacy up to 35 dB HL (Table 2; Figure 1) [42]. The Alpha 2 MPO system is MRI compatible up to 3 Tesla (Table 3) [28]. Available accessories and streaming capabilities are listed in Table 4.
3.1.3. Active Transcutaneous Devices
Active transcutaneous bone conduction devices were designed to maximize the benefits of percutaneous and passive transcutaneous devices while avoiding skin complications and soft tissue signal attenuation. Active devices have an external processor and implanted transducer which are connected by magnetic coils. Signals are transmitted electrically from the external to internal device using technology akin to that of cochlear implants. As the internal device is responsible for generating mechanical forces against the skull, skin attenuation does not occur, and magnet strength can be significantly reduced.
Available devices include the BonebridgeTM (MED-EL, Innsbruck, Austria) [29], and the recently introduced Osia® 2 System (Cochlear Bone-Anchored Solutions AB, Mölnlycke, Sweden) [25]. The BonebridgeTM was first introduced in 2012 with the second version, the BCI602, released in 2019. The device is indicated for patients with CHL, MHL with BC PTA thresholds better than or equal to 45 dB HL, or SSD (Table 2; Figure 1). The implanted device consists of a magnet, receiving coil, demodulator which processes sounds, and an electromagnetic floating mass transducer (FMT) which generates mechanical vibrations [29]. The FMT is attached to the skull via cortical fixation screws that do not require osseointegration [43]. The BCI602 requires a bony recess drilled into the skull, though the BCI602 is smaller in size than the original implant making placement more straightforward. Optimal placement is in the pre-sigmoid mastoid bone. In patients that have had a prior mastoidectomy, alternative placement in a retrosigmoid position or above the temporal line may be required. The device has a flexible bridge between the receiver coil and the FMT to allow for greater flexibility in placement when needed. Lifts are available to limit the amount of required bone excavation and separate the device from underlying dura or sinuses [44,45]. Preoperative CT imaging is recommended [45]. The external processor is the SAMBA 2 processor which is held in place magnetically with six magnet strengths available [30]. With the external processor removed, this device is MRI compatible up to 1.5 Tesla (Table 3) [29].
The Osia® System was introduced in the United States in 2019 and indicated for patients with CHL, MHL with BC PTA thresholds of 55 dB HL or better, and SSD (Table 2; Figure 1) [25]. The system uses the same BI300 osseointegrated implant as other CochlearTM devices with the OSI200 implant fixated to the osseointegrated BI300 screw [26]. Bone polishing may be required to ensure the transducer is in contact with the implant only and not surrounding bone, but drilling a bony well is not required [46]. This device uses a piezoelectric transducer which undergoes mechanical deformation when an electric voltage is applied [47]. This motion drives vibration through the BI300 implant to the skull, allowing for bone conduction hearing. The current device is not MRI compatible; the implanted magnet must be surgically removed before an MRI can be safely performed (Table 3) [27]. Available accessories and streaming capabilities are listed in Table 4.
3.2. Extrinsic Devices
Non-surgical bone conduction hearing devices are also available. These are attached to the patient via a headband, softband, adhesive, eyeglasses, or another mechanism. The external device is in contact with the skin, vibrates in response to sound, and transmits vibratory signals through the intact skin and soft tissue to the skull, leading to bone conduction hearing. These devices are subject to signal attenuation, especially at high frequencies, as the signal travels through soft tissue [7]. Depending on the attachment mechanism, the force required to hold the device in place and effectively transmit sound may limit wear time [48]. The same bone-anchored hearing processors used in the transcutaneous passive devices can be attached to a test band. Pre-implantation testing is recommended for patients considering bone-anchored hearing aid placement to help patients understand the benefits of such devices, sound quality, and the utility of choosing a bone conduction device.
Similar to passive transcutaneous devices, signal attenuation, especially at high frequencies, is expected [7]. Percutaneous or active transcutaneous devices would be expected to perform better, but the trial period allows patients to make a more informed decision about proceeding with surgery and the hearing quality they can anticipate post-operatively. Bone-anchored hearing aid placement is currently FDA-approved for children five years of age or older [49]. Children too young for implantation or adult patients for whom surgery is contraindicated may use a headband device as for amplification beyond the trial environment.
Previously introduced processors including CochlearTM Baha® 5 series, Ponto 3 and 4 series, and Alpha MPO ePlusTM devices can all be worn externally on a soft band, headband, or other attachment mechanism. Two devices may be worn when bilateral amplification is indicated.
In addition to these devices, an adhesive option, the ADHEAR (MED-EL, Innsbruck, Austria) is also available [31]. This device is anchored with an adhesive applied to the skin over the mastoid bone which is designed to be worn for three to seven days. The audio processor connects to the adhesive and vibrates in response to sound, driving vibratory signal transmission through the skin and soft tissue to the underlying bone [31]. Since it is attached by an adhesive, pressure-induced discomfort is not a limitation to wear [48]. The ADHEAR is indicated for patients with unilateral or bilateral conductive hearing loss with a bone conduction HL better than or equal to 25 dB and for patients with single-sided deafness (Table 2; Figure 1) [31]. Available accessories and streaming capabilities are listed in Table 4.
The SoundBite (Sonitus Technologies, San Mateo, CA, USA) is a dental appliance designed to transmit vibratory signals to the skull via the teeth [50,51]. The device is not currently available, but a brief discussion is included here for reference. The device was designed for patients with single-sided deafness or conductive hearing loss with a bone conduction PTA better than or equal to 25 dB HL [20]. The SoundBiteTM consists of an in-the-mouth (ITM) piezoelectric transducer placed on the buccal surface of the maxillary molars and a device worn on the poorer hearing ear which consists of a behind-the-ear (BTE) transducer and a microphone in the ear canal [51]. This has been found to be safe and uses forces far below those typically felt by the teeth during normal functions [50]. Production of the device stopped in 2015, but Sonitus Technologies was recently awarded a contract with the United States Department of Defense with the plan to rebrand the device as the Molar MicTM for military personnel [52].
Figure 1.
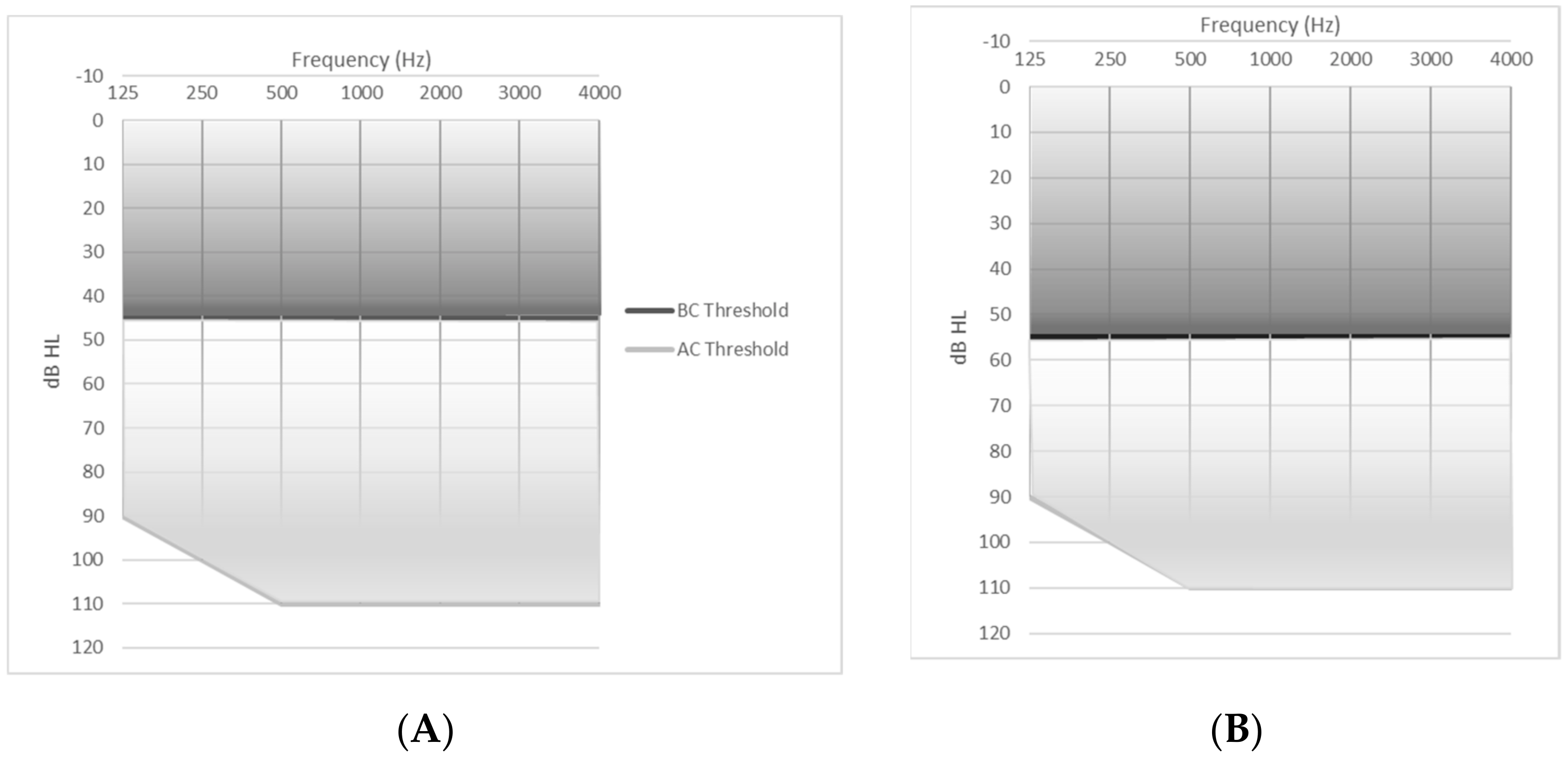
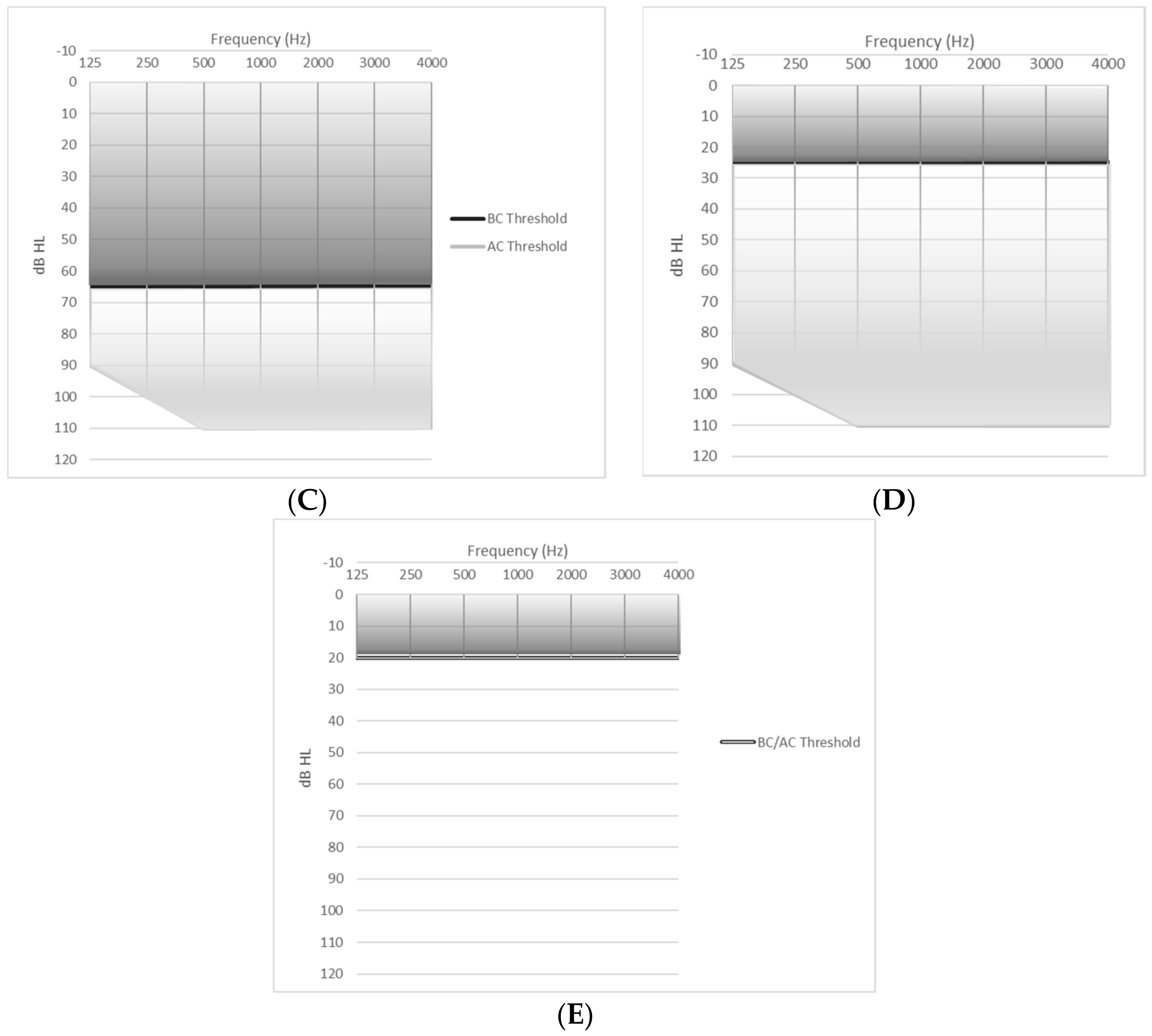
This figure depicts the fitting ranges for the described devices. The dark grey shaded area represents the range of recommended bone conduction thresholds in patients being considered for bone conduction hearing devices. The light grey shaded area demonstrates possible air conduction thresholds. (A) represents a 45 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 [15], Ponto 4 [15], Baha® 5 [17], Alpha 2 MPO ePlusTM [42], and SAMBA 2 [30] processors. (B) represents a 55 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 Power [15], Baha® 5 Power [17], Baha® 6 Max [16], and Osia® 2 [25] processors. (C) represents a 65 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 SueprPower [15] and the Baha® 5 SuperPower [17]. (D) represents a 25 dB BC PTA, the recommended bone conduction hearing threshold for the ADHEAR processor [31]. (E) represents a 20 dB BC PTA. For patients with SSD, the contralateral ear should have normal hearing—a BC and AC PTA of 20 dB or better. These figures were created from publicly available device information and reproduced with permission from CochlearTM, MED-EL, Medtronic, and Oticon representatives.
Figure 1.
This figure depicts the fitting ranges for the described devices. The dark grey shaded area represents the range of recommended bone conduction thresholds in patients being considered for bone conduction hearing devices. The light grey shaded area demonstrates possible air conduction thresholds. (A) represents a 45 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 [15], Ponto 4 [15], Baha® 5 [17], Alpha 2 MPO ePlusTM [42], and SAMBA 2 [30] processors. (B) represents a 55 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 Power [15], Baha® 5 Power [17], Baha® 6 Max [16], and Osia® 2 [25] processors. (C) represents a 65 dB BC PTA, the recommended bone conduction hearing threshold for the Ponto 3 SueprPower [15] and the Baha® 5 SuperPower [17]. (D) represents a 25 dB BC PTA, the recommended bone conduction hearing threshold for the ADHEAR processor [31]. (E) represents a 20 dB BC PTA. For patients with SSD, the contralateral ear should have normal hearing—a BC and AC PTA of 20 dB or better. These figures were created from publicly available device information and reproduced with permission from CochlearTM, MED-EL, Medtronic, and Oticon representatives.



{kind=link}
{kind=link}
Table 3.
Sound Processor Characteristics.
| Device | Processor | Size | Weight | Battery Type | Average Battery Life | IP Rating [53] | |
|---|---|---|---|---|---|---|---|
| Percutaneous | Ponto [15,21] | Ponto 3 | 3.4 × 2.1 × 1.4 cm | 14 g (without battery) | 13 | 70–130 h | IP 57 |
| Ponto 3 Power | 17 g (without battery) | 675 | 70–150 h | IP 57 | |||
| Ponto 3 Superpower | 17 g (without battery) | 675 HP | 35–80 h | IP 57 | |||
| Ponto 4 | 2.6 × 1.9 × 1.1 cm | 13.2 g (without battery) | 312 | 48–70 h | IP 57 | ||
| Baha® Connect [16,17,54,55] | Baha® 5 | 2.6 × 1.9 × 1.2 cm | 9.8 g (without battery) | 312 | 36–100 h | IP 63 | |
| Baha® 5 Power | 3.6 × 2.2 × 1.3 cm | 17 g (without battery) | 675 | 80–220 h | IP 63 | ||
| Baha® 5 SuperPower | 3.9 × 4.8 × 0.9 cm | 14.4 g (actuator); 9.8 −12.7 g (processing unit + battery) | Rechargeable lithium | ≤16 h (mini) ≤32 h (standard) | IP 63 | ||
| Baha® 6 Max | 2.6 × 1.9 × 1.2 cm | 11.5 g (without battery) | 312 | 44–132 h | IP 68 | ||
| Transcutaneous Passive | Alpha 2 MPO [23] | Alpha 2 MPO ePlusTM | 4.1 cm × 1.63 cm | 13 or rechargeable | 320 h or 32 h (rechargeable) | IP 22 | |
| Baha® Attract [16,17,24] | Same as Baha® Connect | Same as above | |||||
| Transcutaneous Active | Osia® [22,25,26,27] | Osia® 2 | 3.6 × 3.2 x 1.04 | 7.8 g (with magnet; without battery) | 675 HP | IP 52; IP 68 (with cover) | |
| BonebridgeTM [28,29,30] | SAMBA 2 | 3.0 × 3.5 × 1.0 cm | 7.5 g (with magnet; without battery) * | 675 | 133–210 h | IP 54; IP 68 (with cover) | |
| Adhesive | ADHEAR [31] | ADHEAR | 0.6 × 3.0 cm (adhesive) 1.5 × 3.5 cm (processor) | 13.5 g (without battery) | 13 | Up to 300 h | |
Device characteristics and compatibility for each processor are listed including external processor size, weight, battery type, battery life, and IP (ingress protection) rating. IP Rating = “ingress protection” rating, indicates the amount of resistance to solids and liquids. The first number indicates the amount of resistance to solids (with 0 being not protected, and 6 being dust-tight), and the second digit indicates the amount of resistance to liquids (with 0 being not protected, and 8 being protected from liquids up to 1m of submersion) [55]. Device information is included with permission from CochlearTM, MED-EL, Medtronic, and Oticon representatives. Note that battery life is variable depending on the programs and features utilized and streaming time. (HP = high power battery type). * D. Franz, email communication, April 2021.
Table 4.
Sound Processor Connectivity and Accessories.
| Device | Processor | Wireless Accessories | Streaming Method | Direct iPhone Streaming | Direct Android Streaming | |
|---|---|---|---|---|---|---|
| Percutaneous | Ponto [15,53,56] | Ponto 3 | Ponto 3
| NFMI on neck loop; 2.4 GHz to devices | ||
| Ponto 3 Power | ||||||
| Ponto 3 Superpower | ||||||
| Ponto 4 | 2.4 GHz | X | ||||
| Baha® Connect [16,17,21,54,55,57] | Baha® 5, Baha® 5 Power, and Baha® 5 SuperPower | Baha 5 and 6
| 2.4 GHz | X | ||
| Baha® 6 Max | 2.4 GHz; Bluetooth LE | X | X | |||
| Transcutaneous Passive | Alpha 2 MPO [23] | Alpha 2 MPO ePlusTM | None Note that DAI can be used for wired streaming and FM systems | DAI | ||
| Baha® Attract [7,16,17,24] | Baha® 5, Baha® 5 Power, and Baha® 5 SuperPower; Baha® 6 Max | Same as above | ||||
| Transcutaneous Active | Osia® [25,26,27,58] | Osia® 2 | Osia® Smart App TrueWirelessTM Phone Clip Mini mic 2 Remote control 2 TV streamer | 2.4 GHz | X | |
| BONEBRIDGETM [9,28,29,30,59] | SAMBA 2 | SAMBA2GO SAMBA 2 Remote App Note that DAI can be used for wired streaming and FM systems | NFMI on neck loop; Bluetooth or DAI to devices | |||
| Adhesive | ADHEAR [31,60] | ADHEAR | None Note that DAI can be used for wired streaming and FM systems | DAI | ||
2.4 GHz = The 2.4 GHz Industrial Scientific Medical (ISM) band is similar to Bluetooth streaming and allows wireless signal to propagate through the air to connect/stream with the hearing processor. NFMI = near field magnetic induction; BT LE = Bluetooth low energy; Bluetooth technology that utilizes the traditional “frequency-hopping” 2.4 GHz band technology, but requires less energy consumption. Best for devices in short range of each other [61]. Device information is included with permission from CochlearTM, MED-EL, Medtronic, and Oticon representatives.
4. Conclusions
Since the introduction of bone conduction hearing technology, numerous devices have been developed to optimize signal transmission, limit skin and wound complications, and rehabilitate hearing for patients with conductive and mixed hearing loss and single-sided deafness. The recently introduced active transcutaneous devices, the Osia® and BonebridgeTM, take advantage of new electronic signal transmission, optimize bone conduction efficiency, and reduce the incidence of skin complications. The current landscape of devices is described here and includes fitting criteria, patient selection, and benefits and drawbacks of each device. This condensed information is intended to be a resource for patients and providers alike to assist with proper device selection for each situation.
Author Contributions
Conceptualization, S.E.E., E.M.N., and E.Z.S.; methodology, S.E.E., E.M.N., and E.Z.S.; investigation, S.E.E., E.M.N., and E.Z.S.; resources, S.E.E. and E.M.N.; data curation, S.E.E., E.M.N., and E.Z.S.; writing—original draft preparation, S.E.E., E.M.N., and E.Z.S.; writing—review and editing, S.E.E., E.M.N., and E.Z.S.; visualization, S.E.E. and E.M.N.; supervision, E.Z.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We would like to thank representatives from CochlearTM, MED-EL, Medtronic, and Oticon for providing device specifications and permission to reproduce this information in our review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mudry, A.; Tjellström, A. Historical background of bone conduction hearing devices and bone conduction hearing aids. Adv. Otorhinolaryngol. 2011, 71, 1–9. [Google Scholar]
- Tjellström, A.; Lindström, J.; Hallén, O.; Albrektsson, T.; Brånemark, P.I. Osseointegrated titanium implants in the temporal bone. A clinical study on bone-anchored hearing aids. Am. J. Otol. 1981, 2, 304–310. [Google Scholar] [PubMed]
- Brånemark, P.I.; Hansson, B.O.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar] [PubMed]
- Dun, C.A.J.; Faber, H.T.; de Wolf, M.J.F.; Cremers, C.W.R.J.; Hol, M.K.S. An overview of different systems: The bone-anchored hearing aid. Adv. Otorhinolaryngol. 2011, 71, 22–31. [Google Scholar] [PubMed]
- Stenfelt, S. Acoustic and physiologic aspects of bone conduction hearing. Adv. Otorhinolaryngol. 2011, 71, 10–21. [Google Scholar] [PubMed] [Green Version]
- Stenfelt, S.; Goode, R.L. Bone-conducted sound: Physiological and clinical aspects. Otol. Neurotol. 2005, 26, 1245–1261. [Google Scholar] [CrossRef] [PubMed]
- Verstraeten, N.; Zarowski, A.J.; Somers, T.; Riff, D.; Offeciers, E.F. Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the testband, and to the “snap” abutment. Otol. Neurotol. 2009, 30, 70–75. [Google Scholar] [CrossRef]
- Calon, T.G.A.; Johansson, M.L.; de Brujin, A.J.; Berge, H.V.D.; Wagenaar, M.; Eichhorn, E.; Janssen, M.M.; Hof, J.R.; Brunings, J.-W.; Joore, M.A.; et al. Minimally invasive ponto surgery versus the linear incision technique with soft tissue preservation for bone conduction hearing implants: A multicenter randomized controlled trial. Otol. Neurotol. 2018, 39, 882–893. [Google Scholar] [CrossRef]
- Høgsbro, M.; Agger, A.; Johansen, L.V. Successful loading of a bone-anchored hearing implant at two weeks after surgery: Randomized trial of two surgical methods and detailed stability measurements. Otol. Neurotol. 2015, 36, e51–e57. [Google Scholar] [CrossRef]
- Høgsbro, M.; Agger, A.; Johansen, L.V. Successful Loading of a Bone-Anchored Hearing Implant at 1 Week After Surgery. Otol. Neurotol. 2017, 38, 207–211. [Google Scholar] [CrossRef]
- McElveen, J.T., Jr.; Green, J.D., Jr.; Arriaga, M.A.; Slattery, W.H., 3rd. Next-Day Loading of a Bone-Anchored Hearing System: Preliminary Results. Otolaryngol. Head Neck Surg. 2020, 163, 582–587. [Google Scholar] [CrossRef] [PubMed]
- Holgers, K.M.; Tjellstro¨m, A.; Bjursten, L.M.; Erlandsson, B.E. Soft tissue reactions around percutaneous implants: A clinical study of soft tissue conditions around skin-penetrating titanium implants for bone-anchored hearing aids. Am. J. Otol. 1998, 9, 56–59. [Google Scholar]
- Mohamad, S.; Khan, I.; Hey, S.Y.; Hussain, S.S. A systematic review on skin complications of bone-anchored hearing aids in relation to surgical techniques. Eur. Arch. Otorhinolaryngol. 2016, 273, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Kiringoda, R.; Lustig, L.R. A meta-analysis of the complications associated with osseointegrated hearing aids. Otol. Neurotol. 2013, 34, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Candidacy Guide. Oticonmedical.com. 2017. Available online: https://www.oticonmedical.com/-/media/medical/main/files/for-professionals/bahs/audiological-materials/guide/eng/candidacy-guide---english---m52735.pdf?la=en-gb (accessed on 20 January 2021).
- Cochlear. Baha 6 Max Connect. Datasheet; Cochlear Bone Anchored Solutions AB: Mölnlycke, Sweden, 2020. [Google Scholar]
- Compare Baha® Sound Processors|Cochlear. Cochlear. 2018. Available online: https://www.cochlear.com/us/en/home/products-and-accessories/baha-system/baha-sound-processors/compare-baha-sound-processors (accessed on 22 January 2021).
- Mylanus, E.A.; van der Pouw, K.C.; Snik, A.F.; Cremers, C.W. Intraindividual comparison of the bone-anchored hearing aid and air-conduction hearing aids. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 271–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruyt, I.J.; Nelissen, R.C.; Mylanus, E.A.M.; Hol, M.K.S. Three-year Outcomes of a Randomized Controlled Trial Comparing a 4.5-mm-Wide to a 3.75-mm-Wide Titanium Implant for Bone Conduction Hearing. Otol. Neurotol. 2018, 39, 609–615. [Google Scholar] [CrossRef]
- Accessdata.fda.gov. 2011. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf11/K110831.pdf (accessed on 22 February 2021).
- Oticon Ponto MRI Safety/Security Control Information. Oticonmedical.com. 2016. Available online: https://www.oticonmedical.com/-/media/medical/main/files/bahs/users-and-candidates/mri-security-card/eng/mri-security-card---english---m52283.pdf (accessed on 22 January 2021).
- CochlearTM Osia ® 2 Sound Processor User Manual. Cochlear.com. Available online: https://www.cochlear.com/e33e12e0-896e-4bac-baa3-f35683a95336/P1600518_D1600539-V2_Osia_2_SP_UM_EN_US.pdf?MOD=AJPERES (accessed on 10 March 2021).
- Product Specification: Medtronic Alpha 2 MPO ePlusTM. Asiapac.medtronic.com. 2017. Available online: https://asiapac.medtronic.com/content/dam/medtronic-com/us-en/patients/treatments-therapies/bone-conduction/documents/alpha-2-mpo-eplus-spec-sheet.pdf (accessed on 21 January 2021).
- CochlearTM Baha® Attract System: Radiographers Instructions for MRI. Cochlear.com. Published 2015. 2015. Available online: https://www.cochlear.com/f5917ef2-bb35-4307-b330-8c15ffdd993c/BUN264+ISS2+APR15+Baha+Attract+Radiographers+Instructions+for+MRI.pdf (accessed on 8 March 2021).
- CochlearTM Osia® System-Candidate Selection Guide. Cochlear.com. 2019. Available online: https://www.cochlear.com/2bae95f1-5a89-405c-8733-25d28b1e3c4e/OSI007-ISS1-DEC19-Osia-Candidate-Selection-Guide.pdf (accessed on 21 January 2021).
- Technical Specifications: CochlearTM Osia® 2 System. Cochlear.com. 2019. Available online: https://www.cochlear.com/b2f659ec-ca9a-4fad-b7a6-b929e6eaa078/OSI001-ISS1-NOV19-Osia-System-Tech-Spec.pdf (accessed on 8 March 2021).
- CochlearTM Osia® Magnetic Resonance Imaging (MRI) Guidelines. Cochlear.com. 2019. Available online: https://www.cochlear.com/ce7aa1b1-2862-4bcf-a9aa-491707b3556a/P1638364_D1638388-V3_Osia_MRI_Guidelines_EN-US%5B1%5D.pdf (accessed on 22 January 2021).
- MRI Technologist’s Guide: Medtronic Magnetic Implant Precautions. Medtronic.com. 2017. Available online: https://www.medtronic.com/content/dam/medtronic-com/us-en/patients/treatments-therapies/bone-conduction/documents/alpha-2-mpo-eplus-mri-tech-guide.pdf (accessed on 20 January 2021).
- BCI 602: Active Bone Conduction Implant-BONEBRIDGE System. Sf.cdn.medel.com. 2019. Available online: https://sf.cdn.medel.com/docs/librariesprovider2/product/bci602/29214ce_r2_0-bci-602fs-web.pdf (accessed on 21 January 2021).
- MED-EL. BONEBRIDGE SAMBA 2 Audio Processor–Instructions for Use; MED-EL: Innsbruck, Austria, 2020. [Google Scholar]
- ADHEAR System-Including the ADHEAR Audio Processor and the ADHEAR Adhesive Adapter. S3.medel.com. Available online: https://s3.medel.com/pdf/28867_30_ADHEAR_Factsheet-EN.pdf (accessed on 23 January 2021).
- Surgery Guide: A Bone Conduction Hearing Solution-Cochlear™ Baha® DermaLock™ Surgical Procedure. Cochlear.com. 2015. Available online: https://www.cochlear.com/66b43e66-3e0b-453b-9751-bc904f3961fd/BUN128+ISS4+NOV30+-+Baha+Connect+Surgery+Guide+FINAL.pdf (accessed on 8 March 2021).
- Chen, S.; Mancuso, D.; Lalwani, A. Skin Necrosis After Implantation with the BAHA Attract: A Case Report and Review of the Literature. Otol Neurotol. 2017, 38, 364–367. [Google Scholar] [CrossRef]
- Cooper, T.; McDonald, B.; Ho, A. Passive Transcutaneous Bone Conduction Hearing Implants: A Systematic Review. Otol. Neurotol. 2017, 38, 1225–1232. [Google Scholar] [CrossRef]
- Surgery Guide: CochlearTM Baha® Attract System Surgical Procedure. Cochlear.com. 2017. Available online: https://www.cochlear.com/5e7d4527-a3c0-4b19-8814-e7494fdaba07/BUN226-ISS4-APR17-Baha-Attract-Surgery-Guide.pdf (accessed on 8 March 2021).
- den Betsen, C.A.; Monksfuekd, P.; Bosman, A.; Skarzynski, P.H.; Green, K.; Runge, C.; Wigren, S.; Blechert, J.I.; Flynn, M.C.; Mylanus, E.A.M.; et al. Audiological and clinical outcomes of a transcutaneous bone conduction hearing implant: Six-month results from a multicentre study. Clin. Otolaryngol. 2019, 44, 144–157. [Google Scholar]
- Hol, M.K.; Nelissen, R.C.; Agterberg, M.J.; Cremers, C.W.; Snik, A.F. Comparison between a new implantable transcutaneous bone conductor and percutaneous bone-conduction hearing implant. Otol. Neurotol. 2013, 34, 1071–1075. [Google Scholar] [CrossRef]
- Kurz, A.; Flynn, M.; Caversaccio, M.; Kompis, M. Speech understanding with a new implant technology: A comparative study with a new nonskin penetrating Baha system. Biomed. Res. Int. 2014, 2014, 416205. [Google Scholar] [CrossRef] [PubMed]
- CochlearTM Baha® Attract System: Sound Processor Magnet Selection Guide. Cochlear.com. 2016. Available online: https://www.cochlear.com/d41ece87-f6a5-44e3-8f94-53dd6a77edcd/BUN225-ISS3-SEP16-Baha-Attract-SP-Magnet-Selection-Guide.pdf (accessed on 22 January 2021).
- Cedars, E.; Chan, D.; Lao, A.; Hardies, L.; Meyer, A.; Rosbe, K. Conversion of traditional osseointegrated bone-anchored hearing aids to the Baha® attract in four pediatric patients. Int. J. Pediatr. Otorhinolaryngol. 2016, 91, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Bere, Z.; Vass, G.; Perenyi, A.; Tobias, Z.; Rovo, L. Surgical Solution for the Transformation of the Percutaneous Bone Anchored Hearing Aid to a Transcutaneous System in Complicated Cases. J. Int. Adv. Otol. 2020, 16, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Alpha 2 MPO ePLUSTM Candidacy Guide. Medtronic.com. 2017. Available online: https://www.medtronic.com/content/dam/medtronic-com/us-en/patients/treatments-therapies/bone-conduction/documents/alpha-2-mpo-eplus-candidacy-guide.pdf (accessed on 21 January 2021).
- Sprinzl, G.M.; Wolf-Magele, A. The Bonebridge bone conduction hearing implant: Indication criteria, surgery, and a systemic review of the literature. Clin. Otolaryngology. 2016, 42, 131–143. [Google Scholar] [CrossRef]
- Oh, S.J.; Goh, E.K.; Choi, S.W.; Lee, S.; Lee, H.-M.; Lee, I.-W.; Kong, S.-K. Audiologic, surgical and subjective outcomes of active transcutaneous bone conduction implant system (Bonebridge). Int. J. Audiol. 2019, 58, 956–963. [Google Scholar] [CrossRef]
- Carnevale, C.; Thomás-Barberán, M.; Til-Pérez, G.; Sarría-Echegaray, P. The Bonebridge active bone conduction system: A fast and safe technique for a middle fossa approach. J. Laryngol. Otol. 2019, 133, 344–347. [Google Scholar] [CrossRef]
- Mylanus, E.A.M.; Hua, H.; Wigren, S.; Arndt, S.; Skarzynski, P.H.; Telian, S.A.; Briggs, R.J.S. Multicenter Clinical Investigation of a New Active Osseointegrated Steady-State Implant System. Otol. Neurotol. 2020, 41, 1249–1257. [Google Scholar] [CrossRef]
- Calero, D.; Paul, S.; Gesing, A.; Alves, F.; Cordioli, J.A. A technical review and evaluation of implantable sensors for hearing devices. BioMed Eng. OnLine. 2018, 17, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Skarzynski, P.H.; Ratuszniak, A.; Osinska, K.; Koziel, M.; Krol, B.; Cywka, K.B.; Skarzynski, H. A Comparative Study of a Novel Adhesive Bone Conduction Device and Conventional Treatment Options for Conductive Hearing Loss. Otol. Neurotol. 2019, 40, 858–864. [Google Scholar] [CrossRef]
- Accessdata.fda.gov. 2016. Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/K161123.pdf (accessed on 24 January 2021).
- Popelka, G.R.; Derebery, J.; Blevins, N.H.; Murray, M.; Moore, B.C.; Sweetow, R.W.; Wu, B.; Katsis, M. Preliminary evaluation of a novel bone-conduction device for single-sided deafness. Otol. Neurotol. 2010, 31, 492–497. [Google Scholar] [CrossRef]
- Gurgel, R.K.; Shelton, C. The SoundBite hearing system: Patient-assessed safety and benefit study. Laryngoscope 2013, 123, 2807–2812. [Google Scholar] [CrossRef] [PubMed]
- Sonitus Technologies Wins Multi-Million Dollar DOD Award for ‘Molar Mic’. 11 September 2018. Available online: http://www.sonitustechnologies.com/sonitus-technologies-wins-multi-million-dollar-dod-award-for-molar-mic/ (accessed on 22 February 2021).
- IEC 60529. Degrees of Protection Provided by Enclosures (IP Codes); International Electrotechnical Commision: Geneva, Switzerland, 2011. [Google Scholar]
- CochlearTM Baha® Connect System: Radiographers Instructions for MRI. Cochlear.com. 2015. Available online: https://www.cochlear.com/107fc39f-bf96-47b6-9527-7d603b654344/BUN380+ISS1+AUG15+Radiographers+Instructions.pdf (accessed on 8 March 2021).
- Datasheet: CochlearTM Baha® 6 Max Sound Processor. Cochlear.com. BUN871 ISS1 FEB21. Available online: https://www.cochlear.com/d6cd6d3d-8c98-4fae-b0aa-8a6bcaba405e/BUN871+Cochlear+Baha+6+Max+DataSheet+ISS1.pdf?MOD=AJPERES&CVID=nxbWkhz (accessed on 10 March 2021).
- Featured Accessories. Oticon Medical. 2021. Available online: https://www.oticonmedical.com/us/bone-conduction/solutions/accessories (accessed on 10 March 2021).
- Baha Accessories. Cochlear.com. 2020. Available online: https://store.mycochlear.com/store/index.php/aub2c/baha-implants.html (accessed on 10 March 2021).
- Osia® Smartphone Compatibility. Cochlear.Com. 2019. Available online: https://www.cochlear.com/us/en/home/products-and-accessories/cochlear-osia-system/osia-2/osia-smartphone-compatibility (accessed on 10 March 2021).
- MED-EL. SAMBA 2 GO–Instructions for Use; MED-EL: Innsbruck, Austria, 2020. [Google Scholar]
- MED-EL. ADHEAR: A Revolution in Bone Conduction Technology. Connectivity Information Provided by MED-EL; MED-EL: Innsbruck, Austria, 2020. [Google Scholar]
- Siekkinen, M.; Hiienkari, M.; Nurminen, J.K.; Nieminen, J. How low energy is bluetooth low energy? Comparative measurements with ZigBee/802.15.4. In Proceedings of the 2012 IEEE Wireless Communications and Networking Conference Workshops (WCNCW), Paris, France, 14 April 2012; pp. 232–237. [Google Scholar] [CrossRef]
Table 1.
Holgers classification of skin complications.
| Grade | Description | Management |
|---|---|---|
| 0 | No irritation | Remove epithelial debris if present |
| 1 | Slight redness | Local treatment |
| 2 | Red and slightly moist tissue (no granuloma) | Local treatment |
| 3 | Reddish and moist (may have granulation tissue) | Revision surgery indicated |
| 4 | Infection | Removal of skin penetrating implant necessary |
The Holgers classification is used to classify and describe skin complications following percutaneous device placement [12].
Table 2.
Sound processor specifications.
| Device | Processor | Fitting Range | Frequency Range (DIN45.605) | Peak OFL * at 90 dB SPL | Peak OFL * at 60 dB SPL | Processing Delay | MRI Compatibility | |
|---|---|---|---|---|---|---|---|---|
| Percutaneous | Ponto † [15,20] | Ponto 3 | BC PTA ≤ 45 dB | 200–9500 Hz | 124 dB | 107 dB | 6 ms | Compatible up to 3 Tesla |
| Ponto 3 Power | BC PTA ≤ 55 dB | 260–9600 Hz | 128 dB | 116 dB | 6 ms | |||
| Ponto 3 Superpower | BC PTA ≤ 65 dB | 260–9600 Hz | 135 dB | 125 dB | 6 ms | |||
| Ponto 4 | BC PTA ≤ 45 dB | 200–9500 Hz | 124 dB | 108 dB | 8 ms | |||
| Baha® Connect ‡ [16,17,21,22] | Baha® 5 | BC PTA ≤ 45 dB | 250–7000 Hz | 117 dB | 105 dB | 4.5 ms | Compatible up to 3 Tesla | |
| Baha® 5 Power | BC PTA ≤ 55 dB | 250–7000 Hz | 123 dB | 113 dB | 4.5 ms | |||
| Baha® 5 SuperPower | BC PTA ≤ 65 dB | 250–7000 Hz | 133 dB | 121 dB | 4.5 ms | |||
| Baha® 6 Max | BC PTA ≤ 55 dB | 200–9700 Hz | 121 dB | 108 dB | <6 ms | |||
| Transcutaneous Passive | Alpha 2 MPO ° [23] | Alpha 2 MPO ePlusTM | BC PTA ≤ 45 dB (ideal ≤ 35 dB) | 125–8000 Hz | 120 dB | 110 dB | Compatible up to 3 Tesla | |
| Baha® Attract ‡ [16,17,22,24] | Baha® 5 | BC PTA ≤ 45 dB | 250–6300 Hz | 114 dB | 104 dB | 4.5 ms | Compatible up to 1.5 Tesla | |
| Baha® 5 Power | BC PTA ≤ 55 dB | 250–7000 Hz | 125 dB | 115 dB | 4.5 ms | |||
| Baha® 5 SuperPower | BC PTA ≤ 65 dB | 250–7000 Hz | 134 dB | 123 dB | 4.5 ms | |||
| Baha® 6 Max | BC PTA ≤ 55 dB | 200–9250 Hz | 121 dB | 108 dB | <6 ms | |||
| Transcutaneous Active | Osia® ‡ [25,26,27] | Osia® 2 | BC PTA ≤ 55 dB | 400–7000 Hz | <6 ms | No–internal magnet must be removed | ||
| BONEBRIDGETM € [28,29,30] | SAMBA 2 | BC PTA ≤ 45 dB | 250–8000 Hz | 117 dB | 8 ms | Compatible up to 1.5 Tesla | ||
| Adhesive | ADHEAR € [31] | ADHEAR | BC PTA ≤ 25 dB | 250–8000 Hz | 124 dB | 10 ms | Yes–remove external device |
This table includes device specifics for each of the processors discussed and includes fitting ranges, frequency ranges, peak output, and MRI compatibility. (OFL = output force level relative to 1 µN on a skull simulator; * OFL may be measured at FOG (full on gain) or RTG (reference test gain), and therefore may not be directly comparable between devices). Device information is included with permission from CochlearTM, MED-EL, Medtronic, and Oticon representatives. † Oticon Medical AB, Askim, Sweden; ‡ Cochlear Bone-Anchored Solutions AB, Mölnlycke, Sweden; ° Medtronic, Dublin, Ireland; MED-EL, Innsbruck, Austria; € MED-EL, Innsbruck, Austria.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ellsperman, S.E.; Nairn, E.M.; Stucken, E.Z. Review of Bone Conduction Hearing Devices. Audiol. Res. 2021, 11, 207-219. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020019
AMA Style
Ellsperman SE, Nairn EM, Stucken EZ. Review of Bone Conduction Hearing Devices. Audiology Research. 2021; 11(2):207-219. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020019
Chicago/Turabian StyleEllsperman, Susan E., Emily M. Nairn, and Emily Z. Stucken. 2021. "Review of Bone Conduction Hearing Devices" Audiology Research 11, no. 2: 207-219. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres11020019