
Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo: Zuma e Maia Maneuver versus Appiani Variant of Gufoni

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
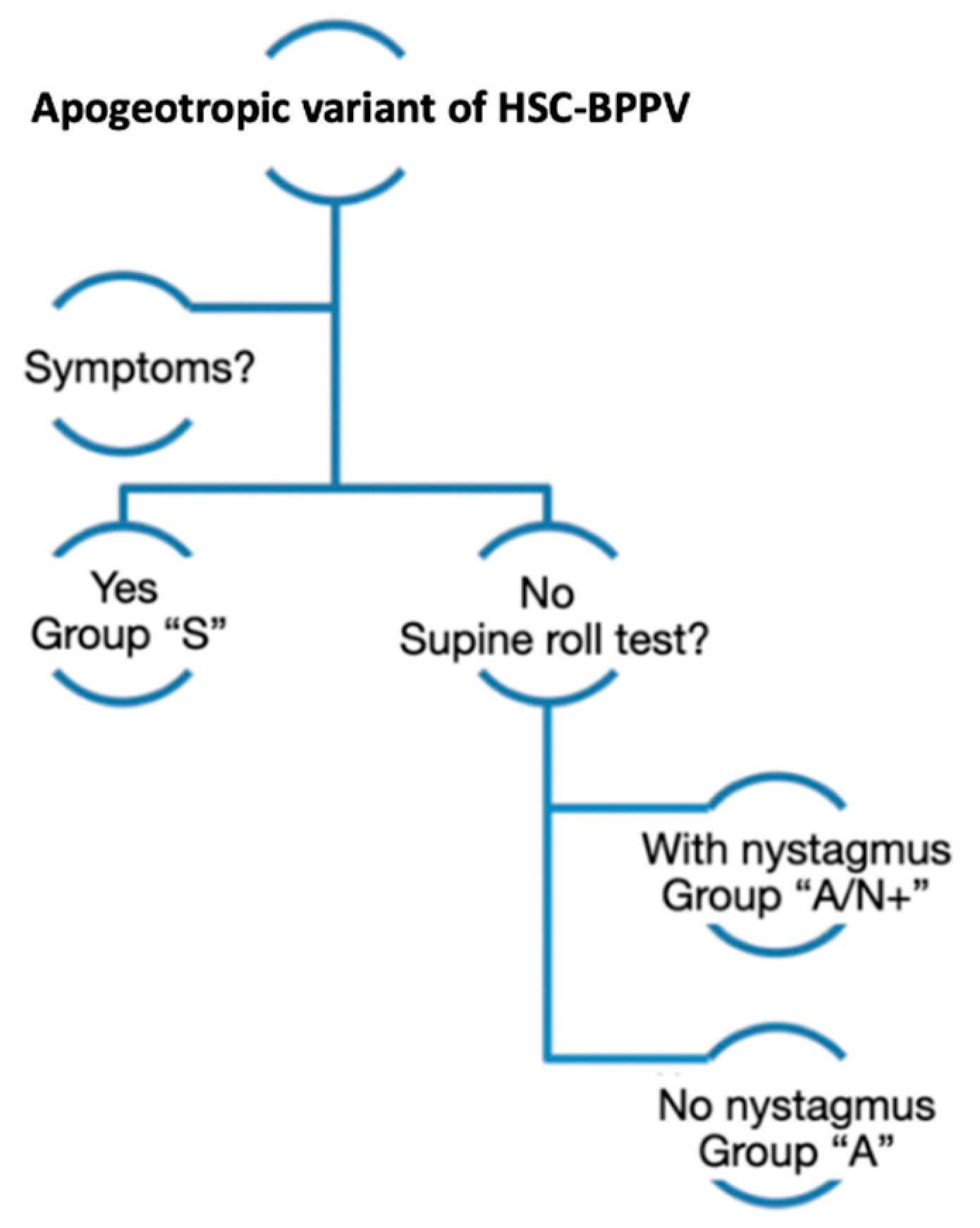
2.1. Inclusion Criteria
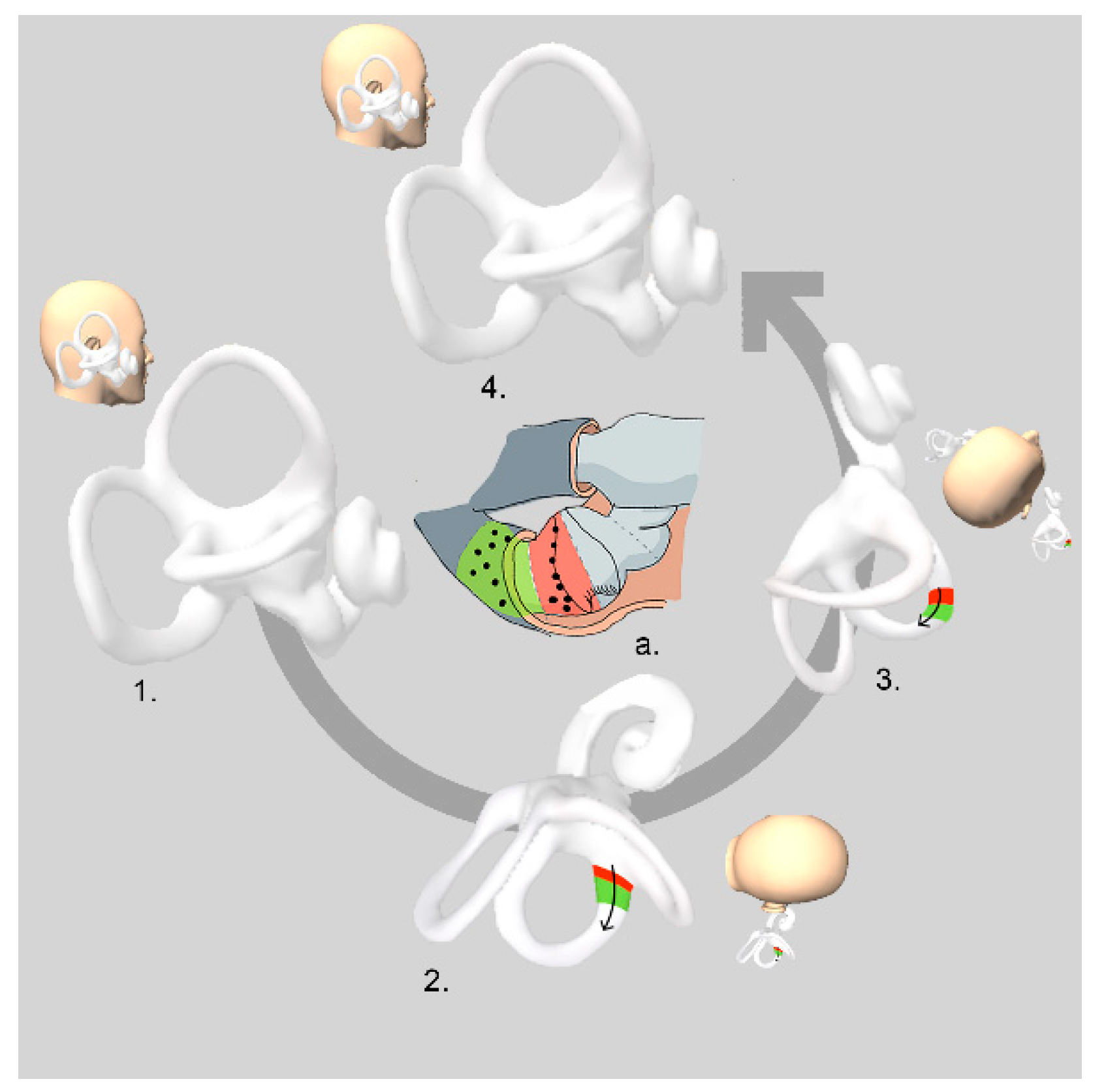
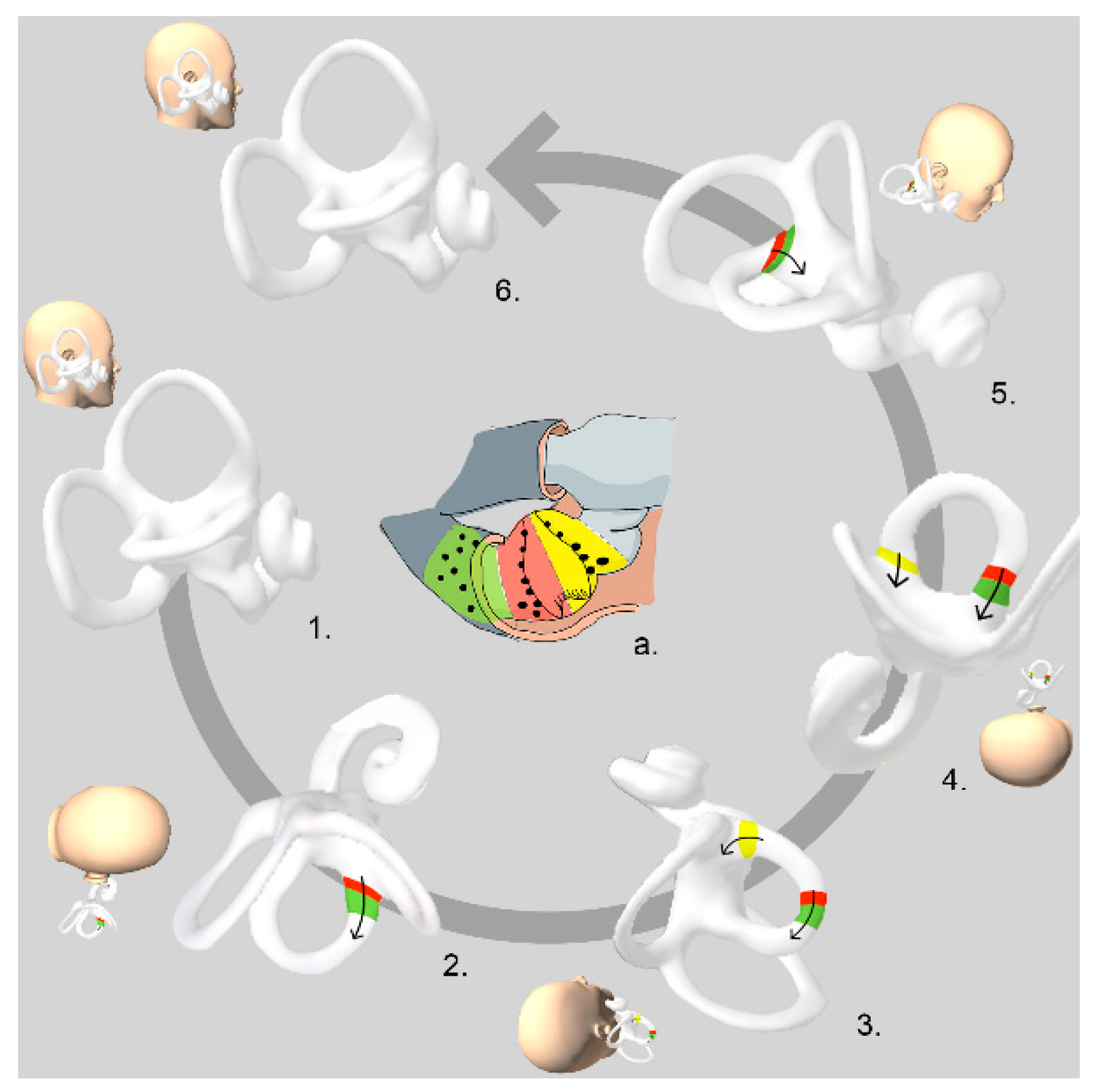
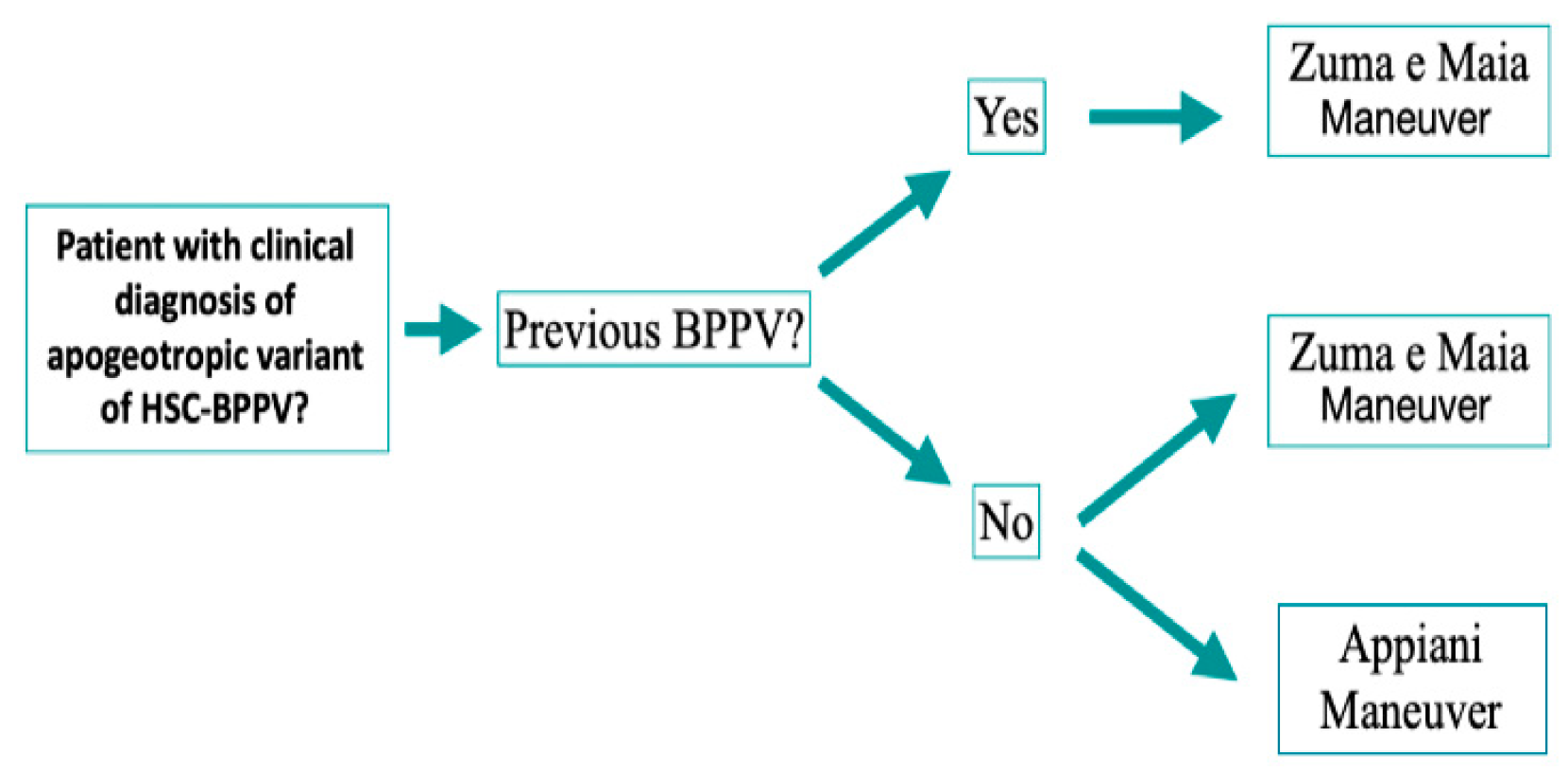
2.2. Treatment: Maneuvers
2.3. Follow-Up
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Argaet, E.; Bradshaw, A.; Welgampola, M. Benign positional vertigo, its diagnosis, treatment and mimics. Clin. Neurophysiol. Pract. 2019, 4, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Choung, Y.H.; Shin, Y.R.; Kahng, H.; Park, K.; Choi, S.J. ‘Bow and lean test’ to determine the affected ear of horizontal canal benign paroxysmal positional vertigo. Laryngoscope 2006, 116, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Bin Lee, J.; Han, D.H.; Choi, S.J.; Park, K.; Park, H.Y.; Sohn, I.K.; Choung, Y.-H. Efficacy of the “bow and lean test” for the management of horizontal canal benign paroxysmal positional vertigo. Laryngoscope 2010, 120, 2339–2346. [Google Scholar]
- Zuma e Maia, F. New Treatment Strategy for Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo. Audiol. Res. 2016, 6, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rabbitt, R.D. Semicircular canal biomechanics in health and disease. J. Neurophysiol. 2019, 121, 732–755. [Google Scholar] [CrossRef] [Green Version]
- Baloh, R.W.; Yue, Q.; Jacobson, K.M.; Honrubia, V. Persistent direction-changing positional nystagmus: Another variant of benign positional nystagmus? Neurology 1995, 45, 1297–1301. [Google Scholar] [CrossRef]
- Ramos, B.F.; Cal, R.; Brock, C.M.; Albernaz, P.L.M.; Maia, F.Z.E. Apogeotropic variant of horizontal semicircular canal benign paroxysmal positional vertigo: Where are the particles? Audiol. Res. 2019, 9, 228. [Google Scholar] [CrossRef] [Green Version]
- Eggers, S.D.; Bisdorff, A.; von Brevern, M.; Zee, D.S.; Kim, J.-S.; Perez-Fernandez, N.; Welgampola, M.S.; Della Santina, C.C.; Newman-Toker, D.E. Classification of Vestibular Signs and Examination Techniques: Nystagmus and Nystagmus-like Movements. J. Vestib. Res. 2019, 29, 57–87. [Google Scholar] [CrossRef] [Green Version]
- Boleas-Aguirre, M.S.; Pérez, N.; Batuecas-Caletrío, A. Bedside therapeutic experiences with horizontal canal benign paroxysmal positional vertigo (cupulolithiasis). Acta Otolaryngol. 2009, 129, 1217–1221. [Google Scholar] [CrossRef]
- Schubert, M.C. Stop the World–I Want to Get off. Vestibular SIG Newsletter. Available online: https://webcache.googleusercontent.com/search?q=cache:paFXf8Ykv_QJ:https://www.neuropt.org/docs/vsig-newsletters/bppv-special-edition-nov-2012.pdf%3Fsfvrsn%3D502ee99b_2+&cd=1&hl=zh-CN&ct=clnk (accessed on 13 May 2022).
- Lee, S.H.; Kim, J.S. Benign paroxysmal positional vertigo. J. Clin. Neurol. 2010, 6, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Asprella-Libonati, G. Pseudo-Spontaneous Nystagmus: A new sign to diagnose the affected side in Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo. Acta Otorhinolaryngol. Ital. 2008, 28, 73–78. [Google Scholar] [PubMed]
- Yamanaka, T.; Sawai, Y.; Murai, T.; Okamoto, H.; Fujita, N.; Hosoi, H. New treatment strategy for cupulolithiasis associated with benign paroxysmal positional vertigo of the lateral canal: The head-tilt hopping exercise. Eur. Arch. Otorhinolaryngol. 2014, 271, 3155–3160. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Lee, J.; Shin, J.E.; Kim, C.H. Treatment Efficacy of Forced Prolonged Position After Cupulolith Repositioning Maneuver in Apogeotropic HSCC BPPV. Ear Nose Throat J. 2021. ahead of print. [Google Scholar] [CrossRef]
- Gufoni, M.; Mastrosimone, L.; di Nasso, F. Repositioning maneuver in benign paroxysmal positional vertigo of the horizontal semi-circular canal. Acta Otorhinolaryngol. Ital. 1998, 18, 363–367. [Google Scholar] [PubMed]
- Appiani, G.C.; Catania, G.; Gagliardi, M.; Cuiuli, G. Repositioning Maneuver for the Treatment of the Apogeotropic Variant of Horizontal Canal Benign Paroxysmal Positional Vertigo. Otol. Neurotol. 2005, 26, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Von Brevern, M.; Bertholon, P.; Brandt, T.; Fife, T.; Imai, T.; Nuti, D.; Newman-Toker, D. Benign paroxysmal positional vertigo: Diagnostic criteria. J. Vestib. Res. 2015, 25, 105–117. [Google Scholar] [CrossRef] [Green Version]
- Shi, T.; Yu, L.; Yang, Y.; Wang, Y.; Shao, Y.; Wang, M.; Geng, Y.; Shi, Z.; Yin, X. The effective clinical outcomes of the Gufoni maneuver used to treat 91 vertigo patients with apogeotropic direction-changing positional nystagmus (apo-DCPN). Medicine 2018, 97, e12363. [Google Scholar] [CrossRef]
- Bhattacharyya, N.; Gubbels, S.P.; Schwartz, S.R.; Edlow, J.A.; El-Kashlan, H.; Fife, T.; Holmberg, J.M.; Mahoney, K.; Hollingsworth, D.B.; Roberts, R.; et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol. Head Neck Surg. 2017, 156 (Suppl. 3), S1–S47. [Google Scholar] [CrossRef]
- Riga, M.; Korres, S.; Korres, G.; Danielides, V. Apogeotropic variant of lateral semicircular canal benign paroxysmal positional vértigo: Is there a correlation between clinical findings, underlying pathophysiologic mechanisms and the effectiveness of repositioning maneuvers? Otol. Neurotol. 2013, 34, 1155–1164. [Google Scholar] [CrossRef]
- Lechner, C.; Taylor, R.L.; Todd, C.; MacDougall, H.; Yavor, R.; Halmagyi, G.M.; Welgampola, M.S. Causes and characteristics of horizontal positional nystagmus. J. Neurol. 2014, 261, 1009–1017. [Google Scholar] [CrossRef]
- Vibert, D.; Kompis, M.; Hausler, R. Benign paroxismal postional vértigo in older women may be related to osteoporosis and osteopenia. Ann. Otol. Rhinol. Laryngol. 2013, 112, 885–889. [Google Scholar] [CrossRef]
- Korres, S.; Balatsouras, D.G.; Kaberos, A.; Economou, C.; Kandiloros, D.; Ferekidis, E. Occurrence of semicircular canal involvement in benign paroxysmal positional vertigo. Otol. Neurotol. 2002, 23, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.J.; Lee, J.B.; Lim, H.J.; Park, H.Y.; Park, K.; In, S.M.; Oh, J.H.; Choung, Y.-H. Clinical Features of Recurrent or Persistent Benign Paroxysmal Positional Vertigo. Otolaryngol. Head Neck Surg. 2012, 147, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Shim, D.B.; Song, C.E.; Jung, E.J.; Ko, K.M.; Park, J.W.; Song, M.H. Benign paroxysmal positional vertigo with simultaneous involvement of multiple semicircular canals. Korean J. Audiol. 2014, 18, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, C.T.; Zhao, X.Q.; Ju, Y.; Wang, Y.; Chen, M.M.; Cui, Y. Clinical Characteristics and Risk Factors for the Recurrence of Benign Paroxysmal Positional Vertigo. Front. Neurol. 2019, 10, 1190. [Google Scholar] [CrossRef] [PubMed]
- Al Garni, M.A.; Mirza, A.A.; Althobaiti, A.A.; Al-Nemari, H.H.; Bakhsh, L.S. Association of benign paroxysmal positional vertigo with vitamin D deficiency: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2018, 275, 2705–2711. [Google Scholar] [CrossRef]
- Yoda, S.; Cureoglu, S.; Yildirim-Baylan, M.; Morita, N.; Fukushima, H.; Harada, T.; Paparella, M.M. Association between Type 1 Diabetes Mellitus and Deposits in the Semicircular Canals. Otolaryngol. Head Neck Surg. 2011, 145, 458–462. [Google Scholar] [CrossRef]
- Babac, S.; Djeric, D.; Petrovic-Lazic, M.; Arsovic, N.; Mikic, A. Why do treatment failure and recurrences of benign paroxysmal positional vertigo occur? Otol. Neurotol. 2014, 35, 1105–1110. [Google Scholar] [CrossRef]
- Webster, G.; Sens, P.M.; Salmito, M.C.; Cavalcante, J.D.R.; dos Santos, P.R.B.; da Silva, A.L.M.; de Souza, C.F. Hyperinsulinemia and hyperglycemia: Risk factors for recurrence of benign paroxysmal positional vertigo. Braz. J. Otorhinolaryngol. 2015, 81, 347–351. [Google Scholar] [CrossRef] [Green Version]
- D’Silva, L.J.; Staecker, H.; Lin, J.; Sykes, K.J.; Phadnis, M.A.; McMahon, T.M.; Connolly, D.; Sabus, C.H.; Whitney, S.L.; Kluding, P.M. Retrospective data suggests that the higher prevalence of benign paroxysmal positional vertigo in Individuals with type 2 diabetes is mediated by hypertension. J. Vestib. Res. 2016, 25, 223–239. [Google Scholar] [CrossRef] [Green Version]
- Wada, M.; Takeshima, T.; Nakamura, Y.; Nagasaka, S.; Kamesaki, T.; Kajii, E. Carotid plaque is a new risk factor for peripheral vestibular disorder: A retrospective cohort study. Medicine 2016, 95, e4510. [Google Scholar] [CrossRef]
- De Stefano, A.; Dispenza, F.; Suarez, H.; Perez-Fernandez, N.; Manrique-Huarte, R.; Ban, J.H.; BeomKim, M.; Strupp, M.; Feil, K.; Oliveira, C.A.; et al. A multicenter observational study on the role of comorbidities in the recurrent episodes of benign paroxysmal positional vertigo. Auris Nasus Larynx 2014, 41, 31–36. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asymptomatic Rate | Appiani | Zuma e Maia |
|---|---|---|
| 1 maneuver | 57.1% | 76.9% |
| 2 maneuvers | 28.6% | 19.2% |
| 3 maneuvers | 9.5% | 3.8% |
| 4 maneuvers | 4.8% |
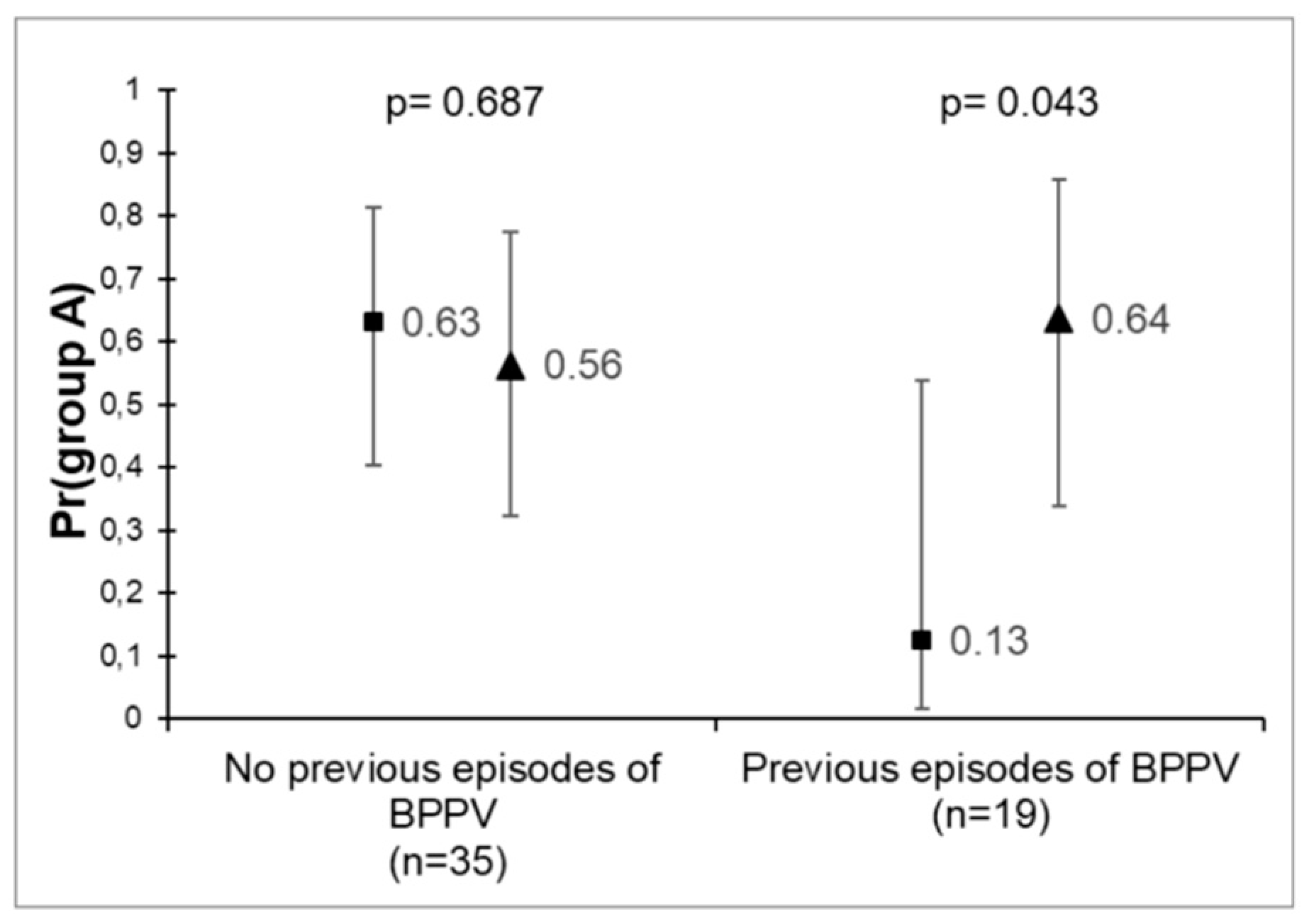
| No Pre-BPPV | Appiani | Zuma e Maia | p-Value | With Pre-BPPV | Appiani | Zuma e Maia | p-Value |
|---|---|---|---|---|---|---|---|
| A | 12 | 9 | 0.687 | A | 1 | 7 | 0.043 |
| A/N+ | 3 | 5 | 0.508 | A/N+ | 1 | 2 | 0.021 |
| S | 4 | 2 | S | 6 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez de Linera-Alperi, M.; Garaycochea, O.; Calavia, D.; Terrasa, D.; Pérez-Fernández, N.; Manrique-Huarte, R. Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo: Zuma e Maia Maneuver versus Appiani Variant of Gufoni. Audiol. Res. 2022, 12, 337-346. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12030035
Alvarez de Linera-Alperi M, Garaycochea O, Calavia D, Terrasa D, Pérez-Fernández N, Manrique-Huarte R. Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo: Zuma e Maia Maneuver versus Appiani Variant of Gufoni. Audiology Research. 2022; 12(3):337-346. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12030035
Chicago/Turabian StyleAlvarez de Linera-Alperi, Marta, Octavio Garaycochea, Diego Calavia, David Terrasa, Nicolas Pérez-Fernández, and Raquel Manrique-Huarte. 2022. "Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo: Zuma e Maia Maneuver versus Appiani Variant of Gufoni" Audiology Research 12, no. 3: 337-346. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12030035