
Prevention of Recurrent Benign Paroxysmal Positional Vertigo: The Role of Combined Supplementation with Vitamin D and Antioxidants

 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
- Posterior Semicircular Canal (PSC) BPPV: Geotropic and Apogeotropic variant
- Horizontal Semicircular Canal (HSC) BPPV: Geotropic and Apogeotropic variant
- Anterior Semicircular Canal (ASC) BPPV
- Multicanal BPPV
2. Materials and Methods
2.1. Study Design
- Arm 1: Including patients with “insufficient” (between 20 and 30 ng/mL) or “deficient” (less than 20 ng/mL) serum concentration of 25-hydroxyvitamin D or 25 (OH) D who were given food supplementation with LICA®, vitamin D3, and vitamins of group B composed as follows: LICA® (ALA 600 mg, L-carnosine 165 mg, zinc 7.5 mg), vitamin B2 0.8 mg, vitamin B6 1 mg, vitamin D3 800 UI (Vertistop® D (Difass International, Coriano (RN), Italy), 1 tablet/day before meals).
- Arm 2: Including patients with “sufficient” serum concentration of 25 (OH) D (between 31 and 100 ng/mL) and no treated
- Arm 3: Including patients with “sufficient” serum level of 25 (OH) D (between 31 and 100 ng/mL) who were given food supplementation with LICA® and Curcumin composed as follows: LICA® (ALA 600 mg, L-carnosine 165 mg, zinc 7.5 mg), Curcumin 100 mg, Piperine 1 mg (Vertistop® L, 2 tablets/day, b.i.d. before meals).
2.2. Diagnostic Protocol and Vestibular Symptoms Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhattacharyya, N.; Gubbels, S.P.; Schwartz, S.R.; Edlow, J.A.; El-Kashlan, H.; Fife, T.; Holmberg, J.M.; Mahoney, K.; Hollingsworth, D.B.; Roberts, R.; et al. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol.-Head Neck Surg. 2017, 156, S1–S47. [Google Scholar] [CrossRef] [PubMed]
- Imai, T.; Takeda, N.; Ikezono, T.; Shigeno, K.; Asai, M.; Watanabe, Y.; Suzuki, M. Classification, diagnostic criteria and management of benign paroxysmal positional vertigo. Auris Nasus Larynx 2017, 44, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Epley, J.M. Positional vertigo related to semicircular canalithiasis. Otolaryngol.-Head Neck Surg. 1995, 112, 154–161. [Google Scholar] [CrossRef]
- Epley, J.M. Human Experience with Canalith Repositioning Maneuvers. Ann. N. Y. Acad. Sci. 2001, 942, 179–191. [Google Scholar] [CrossRef]
- Nuti, D.; Zee, D.S.; Mandalà, M. Benign Paroxysmal Positional Vertigo: What We Do and Do Not Know. Semin. Neurol. 2020, 40, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Von Brevern, M.; Radtke, A.; Lezius, F.; Feldmann, M.; Ziese, T.; Lempert, T.; Neuhauser, H. Epidemiology of benign paroxysmal positional vertigo: A population based study. J. Neurol. Neurosurg. Psychiatry 2007, 78, 710–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Brevern, M.; Bertholon, P.; Brandt, T.; Fife, T.; Imai, T.; Nuti, D.; Newman-Toker, D. Benign paroxysmal positional vertigo: Diagnostic criteria. J. Vestib. Res. 2015, 25, 105–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libonati, G.A.; Martellucci, S.; Castellucci, A.; Malara, P. Minimum Stimulus Strategy: A step-by-step diagnostic approach to BPPV. J. Neurol. Sci. 2022, 434, 120158. [Google Scholar] [CrossRef]
- Eggers, S.D.; Bisdorff, A.; von Brevern, M.; Zee, D.S.; Kim, J.-S.; Perez-Fernandez, N.; Welgampola, M.S.; Della Santina, C.C.; Newman-Toker, D.E. Classification of vestibular signs and examination techniques: Nystagmus and nystagmus-like movements. J. Vestib. Res. 2019, 29, 57–87. [Google Scholar] [CrossRef] [Green Version]
- D’Elia, A.; Quaranta, N.; Libonati, G.A.; Ralli, G.; Morelli, A.; Inchingolo, F.; Cialdella, F.; Martellucci, S.; Barbara, F. The cochleo-vestibular secretory senescence. J. Gerontol. Geriatr. 2020, 68, 85–90. [Google Scholar] [CrossRef]
- Zucca, G.; Valli, S.; Valli, P.; Perin, P.; Mira, E. Why do benign paroxysmal positional vertigo episodes recover spontaneously? J. Vestib. Res. 1998, 8, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Büki, B.; Ecker, M.; Jünger, H.; Lundberg, Y.W. Vitamin D deficiency and benign paroxysmal positioning vertigo. Med. Hypotheses 2013, 80, 201–204. [Google Scholar] [CrossRef] [Green Version]
- Sheikhzadeh, M.; Lotfi, Y.; Mousavi, A.; Heidari, B.; Bakhshi, E. The effect of serum vitamin D normalization in preventing recurrences of benign paroxysmal positional vertigo: A case-control study. Casp. J. Intern. Med. 2016, 7, 173–177. [Google Scholar]
- Taneja, M.K.; Taneja, V. Vitamin D Deficiency in E.N.T. Patients. Indian J. Otolaryngol. Head Neck Surg. 2013, 65, 57–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhim, G.I. Serum vitamin D and recurrent benign paroxysmal positional vertigo. Laryngoscope Investig. Otolaryngol. 2016, 1, 150–153. [Google Scholar] [CrossRef]
- Talaat, H.S.; Abuhadied, G.; Talaat, A.S.; Abdelaal, M.S.S. Low bone mineral density and vitamin D deficiency in patients with benign positional paroxysmal vertigo. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 2249–2253. [Google Scholar] [CrossRef]
- Elmoursy, M.M.; Abbas, A.S. The role of low levels of vitamin D as a co-factor in the relapse of benign paroxysmal positional vertigo (BPPV). Am. J. Otolaryngol. 2021, 42, 103134. [Google Scholar] [CrossRef]
- Pecci, R.; Mandalà, M.; Marcari, A.; Bertolai, R.; Vannucchi, P.; Santimone, R.; Bentivegna, L.; Di Giustino, F.; Mengucci, A.; Vanni, S.; et al. Vitamin D Insufficiency/Deficiency in Patients with Recurrent Benign Paroxysmal Positional Vertigo. J. Int. Adv. Otol. 2022, 18, 158–166. [Google Scholar] [CrossRef]
- Sheikhzadeh, M.; Lotfi, Y.; Mousavi, A.; Heidari, B.; Monadi, M.; Bakhshi, E. Influence of supplemental vitamin D on intensity of benign paroxysmal positional vertigo: A longitudinal clinical study. Casp. J. Intern. Med. 2016, 7, 93–98. [Google Scholar]
- Jeong, S.-H.; Kim, J.-S.; Kim, H.-J.; Choi, J.-Y.; Koo, J.-W.; Choi, K.-D.; Park, J.-Y.; Lee, S.-H.; Choi, S.-Y.; Oh, S.-Y.; et al. Prevention of benign paroxysmal positional vertigo with vitamin D supplementation: A randomized trial. Neurology 2020, 95, e1117–e1125. [Google Scholar] [CrossRef]
- Jeong, S.-H.; Lee, S.-U.; Kim, J.-S. Prevention of recurrent benign paroxysmal positional vertigo with vitamin D supplementation: A meta-analysis. J. Neurol. 2022, 269, 619–626. [Google Scholar] [CrossRef]
- Gucluturk, M.T.; Unal, Z.N.; Ismi, O.; Cimen, M.B.Y.; Unal, M. The Role of Oxidative Stress and Inflammatory Mediators in Benign Paroxysmal Positional Vertigo. J. Int. Adv. Otol. 2016, 12, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Goto, F.; Hayashi, K.; Kunihiro, T.; Ogawa, K. The possible contribution of angiitis to the onset of benign paroxysmal positional vertigo (BPPV). Int. Tinnitus J. 2010, 16, 25–28. [Google Scholar] [PubMed]
- Malara, P.; Castellucci, A.; Martellucci, S. Upright head roll test: A new contribution for the diagnosis of lateral semicircular canal benign paroxysmal positional vertigo. Audiol. Res. 2020, 10, 236. [Google Scholar] [CrossRef]
- Martellucci, S.; Castellucci, A.; Malara, P.; Ralli, G.; Pagliuca, G.; Botti, C.; Gallo, A.; Ghidini, A.; Libonati, G.A. Is it possible to diagnose Posterior Semicircular Canal BPPV from the sitting position? The role of the Head Pitch Test and the upright tests along the RALP and LARP planes. Am. J. Otolaryngol. 2022, 43, 103474. [Google Scholar] [CrossRef]
- Martellucci, S.; Malara, P.; Castellucci, A.; Pecci, R.; Giannoni, B.; Marcelli, V.; Scarpa, A.; Cassandro, E.; Quaglieri, S.; Manfrin, M.L.; et al. Upright BPPV Protocol: Feasibility of a New Diagnostic Paradigm for Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo Compared to Standard Diagnostic Maneuvers. Front. Neurol. 2020, 11, 578305. [Google Scholar] [CrossRef]
- Nola, G.; Mostardini, C.; Salvi, C.; Ercolani, A.; Ralli, G. Validity of Italian adaptation of the Dizziness Handicap Inventory (DHI) and evaluation of the quality of life in patients with acute dizziness. Acta Otorhinolaryngol. Ital. 2010, 30, 190. [Google Scholar]
- Viprey, M.; Merle, B.; Riche, B.; Freyssenge, J.; Rippert, P.; Chakir, M.-A.; Thomas, T.; Malochet-Guinamand, S.; Cortet, B.; Breuil, V.; et al. Development and Validation of a Predictive Model of Hypovitaminosis D in General Adult Population: SCOPYD Study. Nutrients 2021, 13, 2526. [Google Scholar] [CrossRef]
- Giustina, A.; Bouillon, R.; Binkley, N.; Sempos, C.; Adler, R.A.; Bollerslev, J.; Dawson-Hughes, B.; Ebeling, P.R.; Feldman, D.; Heijboer, A.; et al. Controversies in Vitamin D: A Statement From the Third International Conference. JBMR Plus 2020, 4, e10417. [Google Scholar] [CrossRef]
- Lips, P. Worldwide status of vitamin D nutrition. J. Steroid Biochem. Mol. Biol. 2010, 121, 297–300. [Google Scholar] [CrossRef]
- Prentice, A.; Goldberg, G.R.; Schoenmakers, I. Vitamin D across the lifecycle: Physiology and biomarkers. Am. J. Clin. Nutr. 2008, 88, 500S–506S. [Google Scholar] [CrossRef]
- Isaia, G.; Giorgino, R.; Rini, G.B.; Bevilacqua, M.; Maugeri, D.; Adami, S. Prevalence of hypovitaminosis D in elderly women in Italy: Clinical consequences and risk factors. Osteoporos. Int. 2003, 14, 577–582. [Google Scholar] [CrossRef]
- Goldschagg, N.; Teupser, D.; Feil, K.; Strupp, M. No evidence for a specific vitamin D deficit in benign paroxysmal positional vertigo. Eur. J. Neurol. 2021, 28, 3182–3186. [Google Scholar] [CrossRef]
- Melis, A.; Rizzo, D.; Gallus, R.; Leo, M.E.; Turra, N.; Masnaghetti, D.; De Luca, L.M.; Piras, A.; Bussu, F. Relationship between calcium metabolism and benign paroxysmal positional vertigo in north Sardinia population. J. Vestib. Res. 2020, 30, 375–382. [Google Scholar] [CrossRef]
- Ross, M.D. Calcium Ion Uptake and Exchange in Otoconia. Adv. Otorhinolaryngol. 1979, 25, 26–33. [Google Scholar] [CrossRef]
- Thalmann, R.; Ignatova, E.; Kachar, B.; Ornitz, D.M.; Thalmann, I. Development and Maintenance of Otoconia: Biochemical considerations. Ann. N. Y. Acad. Sci. 2001, 942, 162–178. [Google Scholar] [CrossRef]
- Yamauchi, D.; Nakaya, K.; Raveendran, N.N.; Harbidge, D.G.; Singh, R.; Wangemann, P.; Marcus, D.C. Expression of epithelial calcium transport system in rat cochlea and vestibular labyrinth. BMC Physiol. 2010, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Yamauchi, D.; Raveendran, N.N.; Pondugula, S.R.; Kampalli, S.B.; Sanneman, J.D.; Harbidge, D.G.; Marcus, D.C. Vitamin D upregulates expression of ECaC1 mRNA in semicircular canal. Biochem. Biophys. Res. Commun. 2005, 331, 1353–1357. [Google Scholar] [CrossRef]
- Vibert, D.; Sans, A.; Kompis, M.; Travo, C.; Mühlbauer, R.C.; Tschudi, I.; Boukhaddaoui, H.; Häusler, R. Ultrastructural Changes in Otoconia of Osteoporotic Rats. Audiol. Neurotol. 2008, 13, 293–301. [Google Scholar] [CrossRef]
- Zhang, S.; Xing, J.; Gong, Y.; Li, P.; Wang, B.; Xu, L. Downregulation of VDR in benign paroxysmal positional vertigo patients inhibits otolith-associated protein expression levels. Mol. Med. Rep. 2021, 24, 591. [Google Scholar] [CrossRef]
- Bigelow, R.T.; Carey, J.P. Randomized controlled trial in support of vitamin D and calcium supplementation for BPPV. Neurology 2020, 95, 371–372. [Google Scholar] [CrossRef]
- Yang, Z.; Li, J.; Zhu, Z.; He, J.; Wei, X.; Xie, M. Effect of vitamin D supplementation on benign paroxysmal positional vertigo recurrence: A meta-analysis. Sci. Prog. 2021, 104, 368504211024569. [Google Scholar] [CrossRef] [PubMed]
- Wee, C.L.; Mokhtar, S.S.; Singh, K.K.B.; Yahaya, S.; Leung, S.W.S.; Rasool, A.H.G. Calcitriol Supplementation Ameliorates Microvascular Endothelial Dysfunction in Vitamin D-Deficient Diabetic Rats by Upregulating the Vascular eNOS Protein Expression and Reducing Oxidative Stress. Oxidative Med. Cell. Longev. 2021, 2021, 3109294. [Google Scholar] [CrossRef] [PubMed]
- Sahin, E.; Deveci, I.; Dinc, M.E.; Ozker, B.Y.; Bicer, C.; Erel, O. Oxidative Status in Patients with Benign Paroxysmal Positional Vertigo. J. Int. Adv. Otol. 2018, 14, 299–303. [Google Scholar] [CrossRef]
- Li, J.; Wu, R.; Xia, B.; Wang, X.; Xue, M. Serum levels of superoxide dismutases in patients with benign paroxysmal positional vertigo. Biosci. Rep. 2020, 40, BSR20193917. [Google Scholar] [CrossRef]
- Xie, K.-H.; Liu, L.-L.; Su, C.-Y.; Huang, X.-F.; Wu, B.-X.; Liu, R.-N.; Li, H.; Chen, Q.-Q.; He, J.-S.; Ruan, Y.-K. Low Antioxidant Status of Serum Uric Acid, Bilirubin, Albumin, and Creatinine in Patients with Benign Paroxysmal Positional Vertigo. Front. Neurol. 2020, 11, 601695. [Google Scholar] [CrossRef]
- Ajith, T.A. Alpha-lipoic acid: A possible pharmacological agent for treating dry eye disease and retinopathy in diabetes. Clin. Exp. Pharmacol. Physiol. 2020, 47, 1883–1890. [Google Scholar] [CrossRef]
- DeRosa, G.; D’Angelo, A.; Romano, D.; Maffioli, P. A Clinical Trial about a Food Supplement Containing α-Lipoic Acid on Oxidative Stress Markers in Type 2 Diabetic Patients. Int. J. Mol. Sci. 2016, 17, 1802. [Google Scholar] [CrossRef] [Green Version]
- Molinari, C.; Morsanuto, V.; Ghirlanda, S.; Ruga, S.; Notte, F.; Gaetano, L.; Uberti, F. Role of Combined Lipoic Acid and Vitamin D3 on Astrocytes as a Way to Prevent Brain Ageing by Induced Oxidative Stress and Iron Accumulation. Oxidative Med. Cell. Longev. 2019, 2019, 2843121. [Google Scholar] [CrossRef] [Green Version]
- Farghali, M.; Ruga, S.; Morsanuto, V.; Uberti, F. Can Brain Health Be Supported by Vitamin D-Based Supplements? A Critical Review. Brain Sci. 2020, 10, 660. [Google Scholar] [CrossRef]
- Alamro, A.A.; Alsulami, E.A.; Almutlaq, M.; Alghamedi, A.; Alokail, M.; Haq, S.H. Therapeutic Potential of Vitamin D and Curcumin in an In Vitro Model of Alzheimer Disease. J. Cent. Nerv. Syst. Dis. 2020, 12, 1179573520924311. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Arm 1 (Vitamin D3 + LICA®) | Arm 2 (No Treatment) | Arm 3 (LICA®) | p-Value | ||
|---|---|---|---|---|---|
| N | 93 | 16 | 19 | ||
| Age | 59.7 ± 14.0 | 62.0 ± 9.4 | 62.7 ± 12.6 | 0.6517 | |
| Sex | M | 62 (66.7%) | 13 (81.3%) | 14 (73.7%) | 0.4602 |
| F | 31 (33.3%) | 3 (18.8%) | 5 (26.3%) | ||
| Serum 25 (OH) D (ng/mL) | 18.2 ± 6.6 | 36.9 ± 5.7 | <0.0001 | ||
| BPPV recurrences | 3.0 ± 4.6 | 2.5 ± 0.9 | 2.5 ± 0.9 | ||
| Osteoporosis | No | 85 (91.4%) | 11 (68.8%) | 15 (83.3%) | 0.0288 |
| Yes | 8 (8.6%) | 5 (31.3%) | 3 (16.7%) | ||
| DHI | 23.5 ± 20.5 | 32.0 ± 21.3 | 28.4 ± 21.3 | 0.137 | |
| VAS dizziness | 3.6 ± 2.3 | 3.0 ± 1.9 | 2.5 ± 1.7 | 0.1427 | |
| VAS vertigo | 3.4 ± 2.8 | 2.9 ± 2.0 | 3.3 ± 3.0 | 0.9443 | |
| VNS dizziness | 3.8 ± 2.4 | 3.6 ± 2.1 | 3.2 ± 2.4 | 0.6383 | |
| VNS vertigo | 3.7 ± 3.1 | 2.9 ± 2.1 | 3.5 ± 3.1 | 0.8412 | |
| Timing | Arm Switch | Arm 1 (Vitamin D3 + LICA®) | Arm 2 (No Treatment) | Arm 3 (LICA®) | Dropouts | |
|---|---|---|---|---|---|---|
| T1 Randomization (n = 128) | 93 | 16 | 19 | |||
| T2 1° FU (n = 109) | 83 (76.1%) | 10 (9.2%) | 16 (14.7%) | 19 | ||
| Arm 1 | 74 (67.88%) | 70 (84.33%) | 0 | 4 (25%) | ||
| Arm 2 | 13 (11.92%) | 3 (3.61%) | 10 (100 %) | 0 | ||
| Arm 3 | 22 (20.18%) | 10 (12.04%) | 0 | 12 (75%) | ||
| T3 2° FU (n = 96) | 67 (69.79%) | 11 (11.45%) | 18 (18.75%) | 13 | ||
| Arm 1 | 64 (66.66%) | 58 (86.56%) | 3 (27.27%) | 3 (16.66%) | ||
| Arm 2 | 12 (12.5%) | 4 (5.97 %) | 8 (72.72%) | 0 | ||
| Arm 3 | 20 (20.83%) | 5 (7.46%) | 0 | 15 (83.33%) | ||
| T4 Final Visit (n = 89) | 60 (67.41%) | 12 (13.48%) | 17 (19.1%) | 7 |
| Arm1 | Arm2 | Arm 3 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T | Mean (95% CI) | Difference T0–T4 (95% CI) | Within- Group p-Value | Mean (95% CI) | Difference T0–T4 (95% CI) | Within- Group p-Value | Mean (95% CI) | Difference T0–T4 (95% CI) | Within- Group p-Value | Between- Group p-Value | |
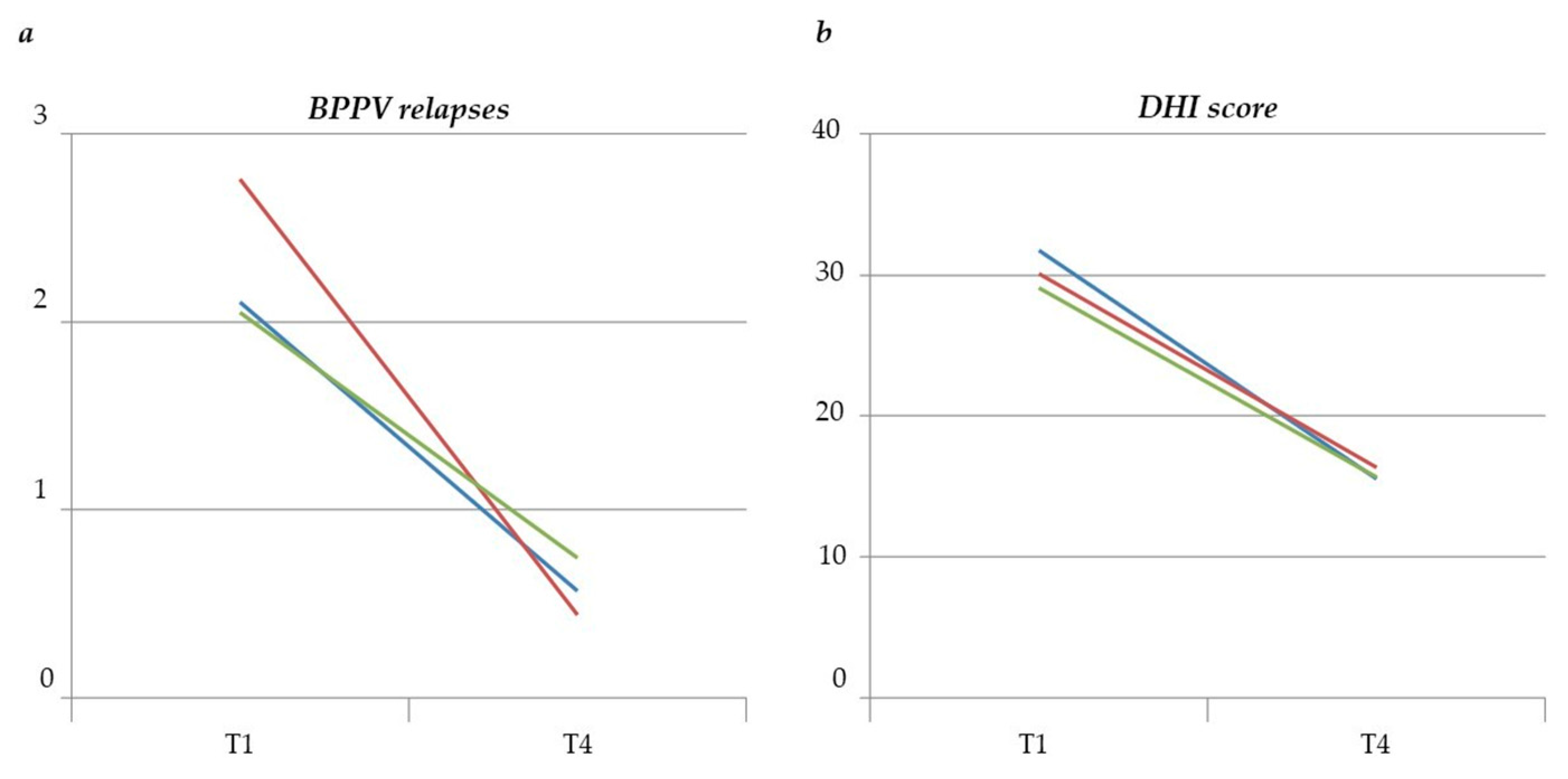
| BPPV relapses | T0 | 2.76 (1.85–4.12) | 2.11 (0.93–4.78) | 2.05 (0.9–4.65) | |||||||
| T4 | 0.44 (0.21–0.92) | −2.32 (−3.4–−1.62) | <0.0001 | 0.57 (0.13–2.49) | −1.54 (−3.96–0.34) | 0.1113 | 0.74 (0.2–2.71) | −1.31 (−3.63–0.48) | 0.1549 | 0.9671 | |
| DHI score | T0 | 30.13 (25.06–35.2) | 31.79 (21.04–42.55) | 29.08 (18.35–39.81) | |||||||
| T4 | 16.37 (10.67–22.07) | −13.76 (−20.05–−7.47) | <0.0001 | 15.57 (4.41–26.72) | −16.22 (−30.63–−1.82) | 0.0278 | 15.64 (5.2–26.09) | −13.44 (−26.67–0.21) | 0.0466 | 0.9616 | |
| VAS dizziness | T0 | 3.95 (3.24–4.8) | 2.93 (1.89–4.52) | 2.47 (1.54–3.98) | |||||||
| T6 | 1.28 (0.89–1.84) | −2.67 (−3.19–−1.81) | <0.0001 | 1.42 (0.71–2.83) | −1.51 (−3–0.17) | 0.0719 | 2.18 (1.31–3.63) | −0.29 (−1.77–1.16) | 0.6871 | 0.8671 | |
| VAS positional vertigo | T0 | 3.63 (4.76–37.64) | 3.26 (5.72–26.04) | 3.95 (7.04–51.87) | |||||||
| T6 | 0.99 (1.54–2.7) | −2.64 (−3.31–−1.64) | <0.0001 | 1.05 | −2.21 (−3.77–−0.1) | 0.027 | 2.4 | −1.55 (−3.1–0.56) | 0.2049 | 0.614 | |
| VNS dizziness | T0 | 3.95 (3.25–4.8) | (2.48–2.86) | (4.51–11.07) | |||||||
| T6 | 1.18 (0.89–1.57) | −2.77 (−3.26–−2.04) | <0.0001 | 3.24 (2.16–4.85) | −1.44 (−2.88–0.03) | 0.0501 | 2.82 (1.84–4.31) | −1.14 (−2.6–0.17) | 0.0739 | 0.8231 | |
| VNS positional vertigo | T0 | 4.06 (3.13–5.28) | 1.8 (1.1–2.93) | 1.68 (1.04–2.71) | |||||||
| T6 | 0.8 (0.5–1.29) | −3.26 (−3.81–−2.2) | <0.0001 | 3.39 (1.94–5.95) | −2.06 | 0.05 | 4.45 (2.46–8.03) | −3.19 (−4.41–0.63) | 0.0099 | 0.6533 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Libonati, G.A.; Leone, A.; Martellucci, S.; Gallo, A.; Albera, R.; Lucisano, S.; Bavazzano, M.; Chiarella, G.; Viola, P.; Galletti, F.; et al. Prevention of Recurrent Benign Paroxysmal Positional Vertigo: The Role of Combined Supplementation with Vitamin D and Antioxidants. Audiol. Res. 2022, 12, 445-456. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12040045
Libonati GA, Leone A, Martellucci S, Gallo A, Albera R, Lucisano S, Bavazzano M, Chiarella G, Viola P, Galletti F, et al. Prevention of Recurrent Benign Paroxysmal Positional Vertigo: The Role of Combined Supplementation with Vitamin D and Antioxidants. Audiology Research. 2022; 12(4):445-456. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12040045
Chicago/Turabian StyleLibonati, Giacinto Asprella, Antonello Leone, Salvatore Martellucci, Andrea Gallo, Roberto Albera, Sergio Lucisano, Maurizio Bavazzano, Giuseppe Chiarella, Pasquale Viola, Francesco Galletti, and et al. 2022. "Prevention of Recurrent Benign Paroxysmal Positional Vertigo: The Role of Combined Supplementation with Vitamin D and Antioxidants" Audiology Research 12, no. 4: 445-456. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres12040045