
The Effect of Alpha-Lipoic Acid in the Treatment of Chronic Subjective Tinnitus through the Tinnitus Handicap Inventory Scores
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Casuistry
2.2. Medical Treatment
2.3. Audiological Evaluation and Questionnaire Survey
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus. Trends Neurosci. 2004, 27, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Polanski, J.F.; Soares, A.D.; Cruz, O.L.D.M. Antioxidant therapy in the elderly with tinnitus. Braz. J. Otorhinolaryngol. 2016, 82, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Biswas, R.; Lugo, A.; Akeroyd, M.; Schlee, W.; Gallus, S.; Hall, D. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg. Health Eur. 2021, 12, 100250. [Google Scholar] [CrossRef] [PubMed]
- Tziridis, K.; Friedrich, J.; Brüeggemann, P.; Mazurek, B.; Schulze, H. Estimation of Tinnitus-Related Socioeconomic Costs in Germany. Int. J. Environ. Res. Public Health 2022, 19, 10455. [Google Scholar] [CrossRef]
- Jarach, C.M.; Lugo, A.; Scala, M.; Brandt, P.A.V.D.; Cederroth, C.R.; Odone, A.; Garavello, W.; Schlee, W.; Langguth, B.; Gallus, S. Global Prevalence and Incidence of Tinnitus. JAMA Neurol. 2022, 79, 888. [Google Scholar] [CrossRef]
- Hall, D.A.; Láinez, M.J.; Newman, C.W.; Sanchez, T.G.; Egler, M.; Tennigkeit, F.; Koch, M.; Langguth, B. Treatment options for subjective tinnitus: Self reports from a sample of general practitioners and ENT physicians within Europe and the USA. BMC Health Serv. Res. 2011, 11, 302. [Google Scholar] [CrossRef] [Green Version]
- Koops, E.A.; Eggermont, J.J. The thalamus and tinnitus: Bridging the gap between animal data and findings in humans. Hear. Res. 2021, 407, 108280. [Google Scholar] [CrossRef]
- Tziridis, K.; Forster, J.; Buchheidt-Dörfler, I.; Krauss, P.; Schilling, A.; Wendler, O.; Sterna, E.; Schulze, H. Tinnitus development is associated with synaptopathy of inner hair cells in Mongolian gerbils. Eur. J. Neurosci. 2021, 54, 4768–4780. [Google Scholar] [CrossRef]
- Kanzaki, J.; Satoh, A.; Kunihiro, T. Does Hearing Preservation Surgery for Acoustic Neuromas Affect Tinnitus? Skull Base Surg. 1999, 9, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, C.J.; Gilden, D.H. Ramsay Hunt syndrome. J. Neurol. Neurosurg. Psychiatry 2001, 71, 149–154. [Google Scholar] [CrossRef]
- De Ridder, D.; Heijneman, K.; Haarman, B.; van der Loo, E. Tinnitus in vascular conflict of the eighth cranial nerve: A surgical pathophysiological approach to ABR changes. Prog. Brain Res. 2007, 166, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Chandan, H.S.; Prabhu, P.; Deepthi, M. Prevalence and characteristics of tinnitus in individuals with auditory neuropathy spectrum disorder. Hear. Balance Commun. 2013, 11, 214–217. [Google Scholar] [CrossRef]
- Lockwood, A.H.; Salvi, R.J.; Coad, M.L. The functional neuroanatomy of tinnitus. Evidence for limbic system links and neural plasticity. Neurology 1998, 50, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Plewnia, C.; Reimold, M.; Najib, A.; Brehm, B.; Reischl, G.; Plontke, S.K.; Gerloff, C. Dose-dependent attenuation of auditory phantom perception (tinnitus) by PET-guided repetitive transcranial magnetic stimulation. Hum. Brain Mapp. 2006, 28, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, R.R.; Azevedo, A.A.; Penido, N.D.O. Positive Association between Tinnitus and Arterial Hypertension. Front. Neurol. 2016, 7, 171. [Google Scholar] [CrossRef] [Green Version]
- Pandey, D.; Pandit, A.; Pandey, A.K. Study of audio vestibular dysfunction in type 2 diabetes mellitus. Int. Arch. Integr. Med. 2016, 3, 23–26. [Google Scholar]
- Mousavi, S.H.G.; Sajadinejad, B.; Khorsandi, S.; Farhadi, A. Diabetes Mellitus and Tinnitus: An Epidemiology Study. Maedica 2021, 16, 580–584. [Google Scholar] [CrossRef]
- Musleh, A.; Alshehri, S.; Qobty, A. Hyperlipidemia and its relation with tinnitus: Cross-sectional approach. Niger. J. Clin. Pract. 2022, 25, 1046. [Google Scholar] [CrossRef]
- Edamatsu, M.; Kondo, Y.; Ando, M. Multiple expression of glucose transporters in the lateral wall of the cochlear duct studied by quantitative real-time PCR assay. Neurosci. Lett. 2011, 490, 72–77. [Google Scholar] [CrossRef]
- Ganança, M.M.; Caovilla, H.H.; Ganança, F.F.; Ganança, C.F.; Munhoz, M.S.; da Silva, M.L.; Serafini, F. Clonazepam in the pharmaco-logical treatment of vertigo and tinnitus. Int. Tinnitus J. 2002, 8, 50–53. [Google Scholar]
- Hoekstra, C.E.; Rynja, S.P.; van Zanten, G.A.; Rovers, M.M. Anticonvulsants for tinnitus. Cochrane Database Syst. Rev. 2011, 7, CD007960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganança, M.M.; Caovilla, H.H.; Gazzola, J.M.; Ganança, C.F.; Ganança, F.F. Betahistine in the treatment of tinnitus in patients with vestibular disorders. Braz. J. Otorhinolaryngol. 2011, 77, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.; Knox, E.; Donaldson, I. The usefulness of nimodipine, an L-calcium channel antagonist, in the treatment of tinnitus. Br. J. Audiol. 1994, 28, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Monzani, D.; Barillari, M.R.; Alicandri Ciufelli, M.; Aggazzotti Cavazza, E.; Neri, V.; Presutti, L.; Genovese, E. Effect of a fixed combi-nation of nimodipine and betahistine versus betahistine as monotherapy in the long-term treatment of Ménière’s disease: A 10-year experience. Acta Otorhinolaryngol. Ital. 2012, 32, 393–403. [Google Scholar]
- Kim, J.-I.; Choi, J.-Y.; Lee, D.-H.; Choi, T.-Y.; Lee, M.S.; Ernst, E. Acupuncture for the treatment of tinnitus: A systematic review of randomized clinical trials. BMC Complement. Altern. Med. 2012, 12, 97. [Google Scholar] [CrossRef] [Green Version]
- Barth, S.W.; Lehner, M.D.; Dietz, G.P.H.; Schulze, H. Pharmacologic treatments in preclinical tinnitus models with special focus on Ginkgo biloba leaf extract EGb 761(R). Mol. Cell Neurosci. 2021, 116, 103669. [Google Scholar] [CrossRef]
- Meng, Z.; Liu, S.; Zheng, Y.; Phillips, J.S. Repetitive transcranial magnetic stimulation for tinnitus. Cochrane Database Syst. Rev. 2011, 10, CD007946. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.S.; McFerran, D. Tinnitus Retraining Therapy (TRT) for tinnitus. Cochrane Database Syst. Rev. 2010, 17, CD007330. [Google Scholar] [CrossRef] [PubMed]
- Zenner, H.-P.; Delb, W.; Kröner-Herwig, B.; Jäger, B.; Peroz, I.; Hesse, G.; Mazurek, B.; Goebel, G.; Gerloff, C.; Trollmann, R.; et al. A multidisciplinary systematic review of the treatment for chronic idiopathic tinnitus. Eur. Arch. Oto-Rhino-Laryngol. 2016, 274, 2079–2091. [Google Scholar] [CrossRef]
- Ziegler, D.; Jenner, P. Oxidative damage in neurodegenerative disease. Lancet 1996, 344, 796–798. [Google Scholar]
- Someya, S.; Prolla, T.A. Mitochondrial oxidative damage and apoptosis in age-related hearing loss. Mech. Ageing Dev. 2010, 131, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Lasisi, T.J.; Lasisi, A.O. Evaluation of serum antioxidants in age-related hearing loss. Aging Clin. Exp. Res. 2014, 27, 265–269. [Google Scholar] [CrossRef]
- Haase, G.M.; Prasad, K.N.; Cole, W.C.; Baggett-Strehlau, J.M.; Wyatt, S.E. Antioxidant micronutrient impact on hearing disorders: Concept, rationale, and evidence. Am. J. Otolaryngol. 2011, 32, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Clerici, W.J.; Yung, L. Direct effects of intraperilynphatic reactive oxygen species generation in cochlear function. Hear. Res. 1996, 101, 14–22. [Google Scholar] [CrossRef]
- Ciorba, A.; Bianchini, C.; Pastore, A.; Mazzoli, M. Pathogenesis of Tinnitus: Any Role for Oxidative Stress? Int. Adv. Otol. 2013, 9, 249–254. [Google Scholar]
- Celik, M.; Koyuncu, I. A Comprehensive Study of Oxidative Stress in Tinnitus Patients. Indian. J. Otolaryngol. Head. Neck Surg. 2018, 70, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Gorąca, A.; Huk-Kolega, H.; Piechota, A.; Kleniewska, P.; Ciejka, E.; Skibska, B. Lipoic acid—Biological activity and therapeutic potential. Pharmacol. Rep. 2011, 63, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Cremer, D.; Rabeler, R.; Roberts, A.; Lynch, B. Safety evaluation of α-lipoic acid (ALA). Regul. Toxicol. Pharmacol. 2006, 46, 29–41. [Google Scholar] [CrossRef]
- Registro_Integratori_per Prodotto, Aggiornato al 1/03/2013. Available online: https://www.salute.gov.it (accessed on 22 March 2023).
- Salehi, B.; Berkay Yılmaz, Y.; Antika, G.; Boyunegmez Tumer, T.; Fawzi Mahomoodally, M.; Lobine, D.; Akram, M.; Riaz, M.; Capanoglu, E.; Sharopov, F.; et al. Insights on the Use of α-Lipoic Acid for Therapeutic Purpos-es. Biomolecules 2019, 9, 356. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, D.W.; Jones-King, K.L.; Whitworth, C.A.; Rybak, L.P. Potentiation of Ototoxicity by Glutathione Depletion. Ann. Otol. Rhinol. Laryngol. 1988, 97, 36–41. [Google Scholar] [CrossRef]
- Conlon, B.J.; Aran, J.M.; Erre, J.P.; Smith, D.W. Attenuation of amynoglicoside-induced coclea damage with the metabolic antioxidant al-pha-lipoic acid. Hear. Res. 1999, 128, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Diao, M.-F.; Liu, H.-Y.; Zhang, Y.-M.; Gao, W.-Y. Changes in antioxidant capacity of the guinea pig exposed to noise and the protective effect of alpha-lipoic acid against acoustic trauma. Sheng Li Xue Bao 2003, 55, 672–676. [Google Scholar] [PubMed]
- Quaranta, N.; Dicorato, A.; Matera, V.; D’Elia, A.; Quaranta, A. The effect of alpha-lipoic acid on temporary threshold shift in hu-mans: A preliminary study. Acta Otorhinolaryngol. Ital. 2012, 32, 380–385. [Google Scholar] [PubMed]
- Seidman, M.D.; Khan, M.J.; Bai, U.; Shirwany, N.; Quirk, W.S. Biologic activity of mitochondrial metabolites on aging and age-related hearing loss. Am. J. Otolaryngol. 2000, 21, 161–167. [Google Scholar] [CrossRef]
- Rybak, L.P.; Husain, K.; Whitworth, C.; Somani, S.M. Dose dependent protection by lipoic acid against cisplatin-induced ototoxicity in rats: Antioxidant defense system. Pharmacol. Toxicol. 2000, 86, 234–241. [Google Scholar] [CrossRef] [Green Version]
- Hounsom, L.; Horrobin, D.F.; Tritschler, H.; Corder, R.; Tomlinson, D.R. A lipoic acid-gamma linolenic acid conjugate is effective against multiple indices of experimental diabetic neuropathy. Diabetologia 1998, 41, 839–843. [Google Scholar] [CrossRef] [Green Version]
- Cameron, N.E.; Cotter, M.A. Effects of antioxidants on nerve and vascular dysfunction in experimental diabetes. Diabetes Res. Clin. Pract. 1999, 45, 137–146. [Google Scholar] [CrossRef]
- Agrawal, Y.; Platz, E.A.; Niparko, J.K. Prevalence of hearing loss and differences by demographic characteristics among US adults: Data from the National Health and Nutrition Examination Survey, 1999–2004. Arch. Intern. Med. 2008, 168, 1522–1530. [Google Scholar] [CrossRef] [Green Version]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Monzani, D.; Genovese, E.; Marrara, A.; Gherpelli, C.; Pingani, L.; Forghieri, M.; Rigatelli, M.; Guadagnin, T.; Arslan, E. Validity of the Italian adaptation of the Tinnitus Handicap Inventory; focus on quality of life and psychological distress in tinnitus-sufferers. Acta Otorhinolaryngol. Ital. 2008, 28, 126–134. [Google Scholar]
- Mavrogeni, P.; Maihoub, S.; Tamás, L.; Molnár, A. Tinnitus characteristics and associated variables on Tinnitus Handicap Inventory among a Hungarian population. J. Otol. 2022, 17, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Zeman, F.; Koller, M.; Figueiredo, R.; Aazevedo, A.; Rates, M.; Coelho, C.; Kleinjung, T.; de Ridder, D.; Langguth, B.; Landgrebe, M. Tinnitus Handicap Inventory for Evaluating Treatment Effects: Which changes are clinically relevant? Otolaryngol. Neck Surg. 2011, 145, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.-H.; Byun, S.W.; Park, Y.; Lee, H.Y. The Tinnitus Handicap Inventory is a better indicator of the overall status of patients with tinnitus than the Numerical Rating Scale. Am. J. Otolaryngol. 2022, 44, 103719. [Google Scholar] [CrossRef] [PubMed]
- Boecking, B.; Rausch, L.; Psatha, S.; Nyamaa, A.; Dettling-Papargyris, J.; Funk, C.; Mazurek, B. Hearing therapy improves tinnitus-related distress in mildly distressed patients with chronic tinnitus and mild-to-moderate hearing loss: A random-ized-controlled cross-over design. J. Clin. Med. 2022, 11, 1764. [Google Scholar] [CrossRef]
- Choi, Y.H. Antioxidant vitamins and magnesium and the risk of hearing loss in the US general population. Am. J. Clin. Nutr. 2014, 99, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moini, H.; Packer, L.; Saris, N.-E.L. Antioxidant and Prooxidant Activities of α-Lipoic Acid and Dihydrolipoic Acid. Toxicol. Appl. Pharmacol. 2002, 182, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Demircan, N.; Gürel, A.; Armuctu, F.; Ünalacak, M.; Aktunç, E.; Atmaca, H. The evaluation of serum cystatin C, malonildialdehyde and total antioxidant status in patients with metabolic syndrome. Med. Sci. Monit. 2008, 14, CR97–CR101. [Google Scholar]
- Brufani, M. Acido -lipoico farmaco o integratore. Una panoramica sulla farmacocinetica, le formulazioni disponibili e le evi-denze cliniche nelle complicanze del diabete. Prog. Nutr. 2014, 16, 62–74. [Google Scholar]
- Valdecantos, M.P.; Pérez-Matute, P.; González-Muniesa, P.; Prieto-Hontoria, P.L.; Moreno-Aliaga, M.J.; Martínez, J.A. Lipoic Acid Improves Mitochondrial Function in Nonalcoholic Steatosis Through the Stimulation of Sirtuin 1 and Sirtuin 3. Obesity 2012, 20, 1974–1983. [Google Scholar] [CrossRef]
- Markaryan, A.; Nelson, E.G.; Hinojosa, R. Quantification of the mitochondrial DNA common deletion in presbycusis. Laryngoscope 2009, 119, 1184–1189. [Google Scholar] [CrossRef]
- Markaryan, A.; Nelson, E.G.; Hinojosa, R. Major arc mitochondrial DNA deletions in cytochrome c oxidase-deficient human cochlear spiral ganglion cells. Acta Oto-Laryngol. 2010, 130, 780–787. [Google Scholar] [CrossRef] [PubMed]
- Tamilselvan, J.; Sivarajan, K.; Anusuyadevi, M.; Panneerselvam, C. Cytochrome c oxidase rather than cytochrome c is a major determinant of mitochondrial respiratory capacity in skeletal muscle of aged rats: Role of carnitine and lipoic acid. Rejuvenation Res. 2007, 10, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Tromba, L.; Perla, F.M.; Carbotta, G.; Chiesa, C.; Pacifico, L. Effect of Alpha-Lipoic Acid Supplementation on Endothelial Function and Cardiovascular Risk Factors in Overweight/Obese Youths: A Double-Blind, Placebo-Controlled Randomized Trial. Nutrients 2019, 11, 375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopinath, B.; Flood, V.M.; McMahon, C.M.; Burlutsky, G.; Spankovich, C.; Hood, L.J.; Mitchell, P. Dietary antioxidant intake is associated with the prevalence but not inci-dence of age-related hearing loss. J. Nutr. Health Aging 2011, 15, 896–900. [Google Scholar] [CrossRef]
- Tang, T.-H.; Hwang, J.-H.; Yang, T.-H.; Hsu, C.-J.; Wu, C.-C.; Liu, T.-C. Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment? Nutrients 2019, 11, 1668. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, J.P.; McKinley, B.; Eckel, R.H. The metabolic syndrome and inflammation. Metab. Syndr. Relat. Disord. 2004, 2, 82–104. [Google Scholar] [CrossRef]
- Petridou, A.I.; Zagora, E.T.; Petridis, P.; Korres, G.S.; Gazouli, M.; Xenelis, I.; Kyrodimos, E.; Kontothanasi, G.; Kaliora, A.C. The Effect of Antioxidant Supplementation in Patients with Tinnitus and Normal Hearing or Hearing Loss: A Randomized, Double-Blind, Placebo Controlled Trial. Nutrients 2019, 11, 3037. [Google Scholar] [CrossRef] [Green Version]
- Elangovan, S.; Spankovich, C. Diabetes and Auditory-Vestibular Pathology. Semin. Hear. 2019, 40, 292–299. [Google Scholar] [CrossRef]
- Wood, J.; Freemantle, N.; King, M.; Nazareth, I. Trap of trends to statistical significance: Likelihood of near significant P value be-coming more significant with extra data. BMJ 2014, 348, g2215. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Group A | Group B | Ind. T-Test | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | df | p | |
| 4FA | 31.4 | 9.4 | 40.6 | 9.2 | −3.80 | 48 | <0.0001 ** |
| PTAhf | 54.4 | 12.5 | 48.9 | 6.9 | 1.78 | 48 | 0.053 |
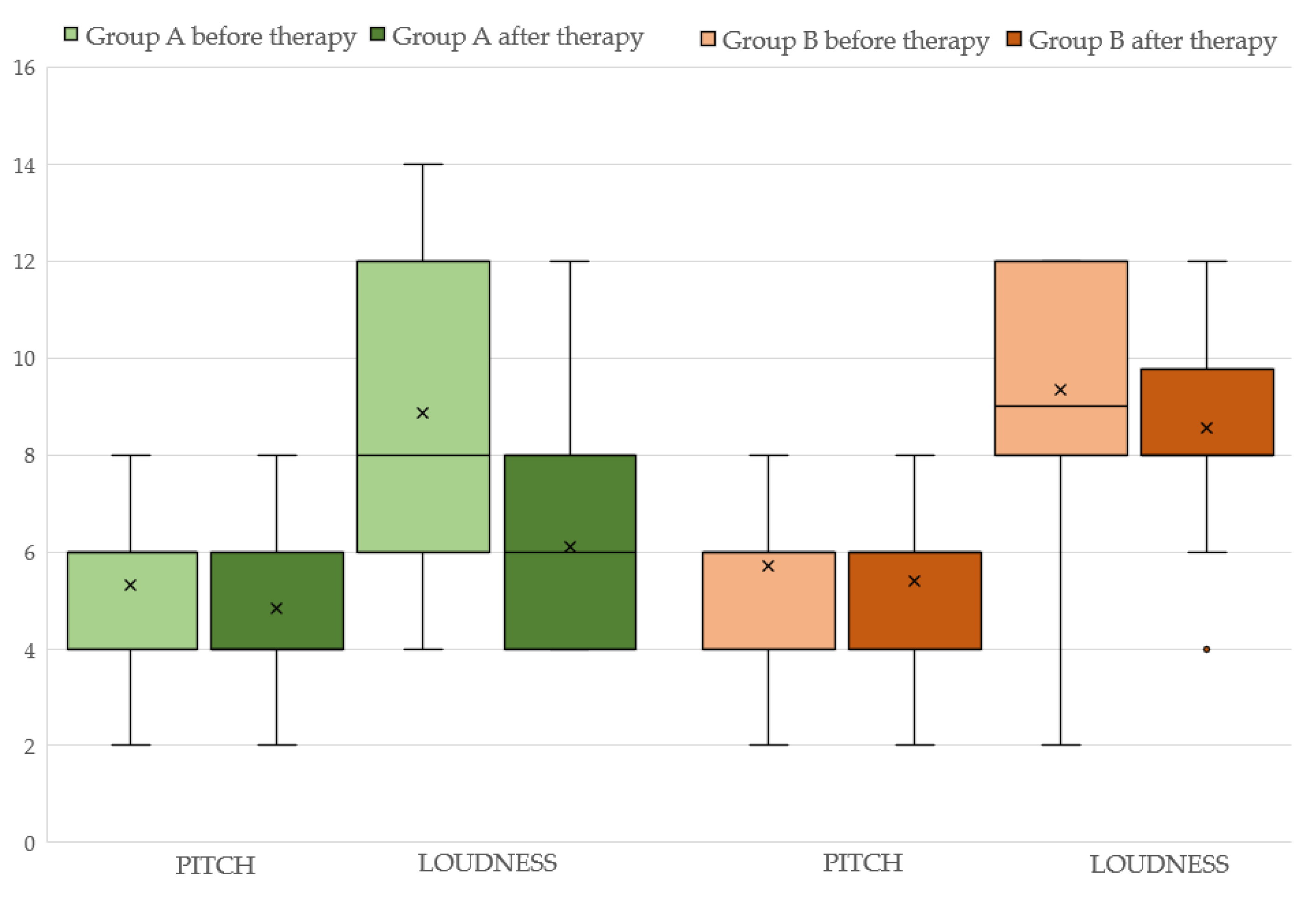
| Pitch | 5.3 | 1.9 | 5.7 | 1.6 | −0.75 | 48 | 0.455 |
| Loudness (SLL) | 8.9 | 2.9 | 9.3 | 2.7 | −0.59 | 48 | 0.556 |
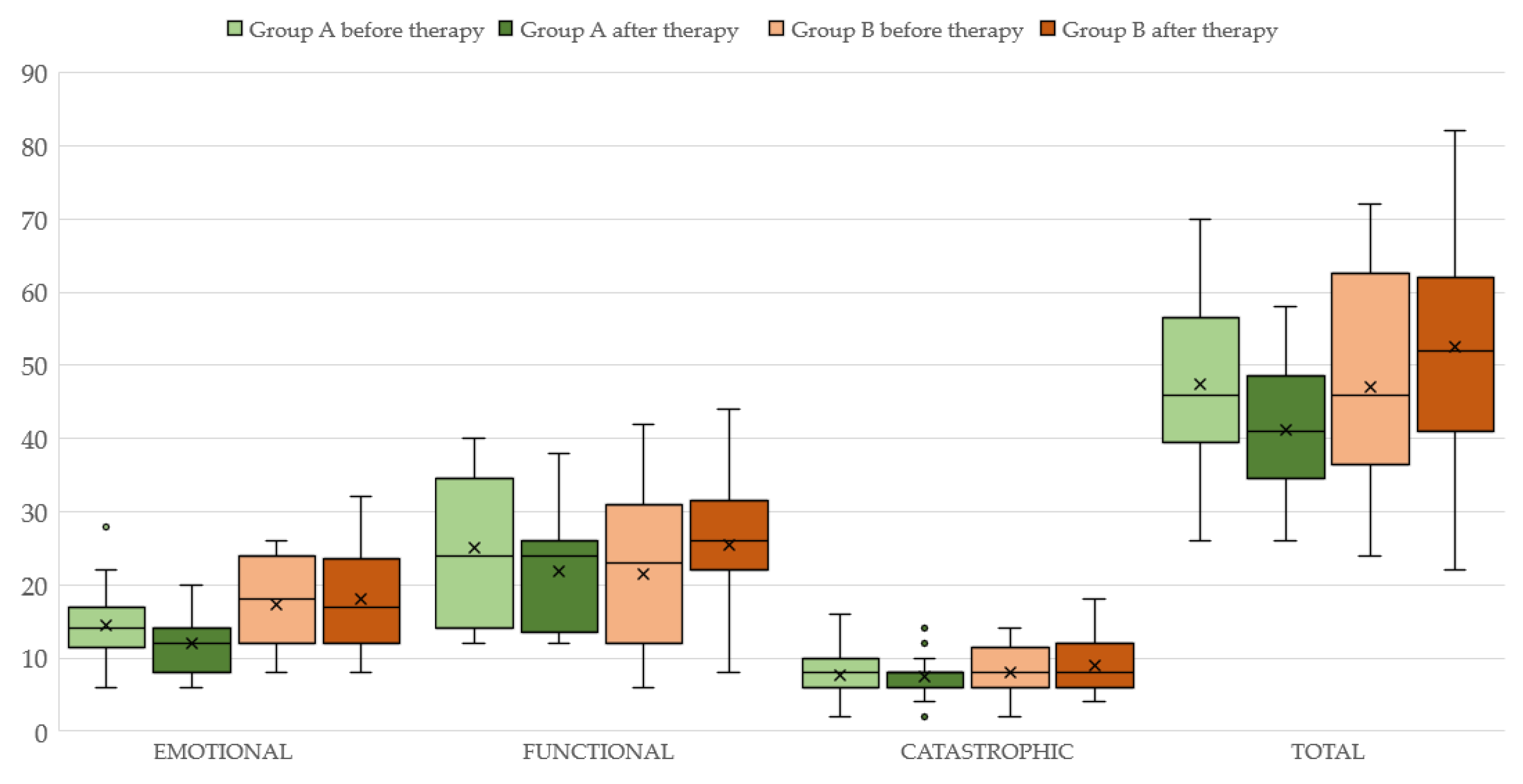
| THI total | 47.4 | 10.9 | 47.0 | 13.8 | 0.95 | 48 | 0.925 |
| THI (functional) | 25.1 | 9.7 | 21.5 | 10.6 | 1.24 | 48 | 0.220 |
| THI (emotional) | 14.5 | 4.9 | 17.4 | 6.8 | −1.76 | 48 | 0.085 |
| THI (catastrophic) | 7.7 | 3.5 | 8.1 | 3.6 | −0.36 | 48 | 0.723 |
| Before Therapy | After Therapy | Paired T-Test | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | df | p | |
| 4FA | 31.4 | 9.1 | 30.1 | 9.4 | −2.38 | 29 | 0.024 (*) |
| PTAhf | 54.4 | 12.5 | 48.6 | 10.4 | 8.2 | 29 | <0.0001 (**) |
| Pitch | 5.3 | 1.9 | 4.8 | 1.6 | 1.2 | 29 | 0.240 |
| Loudness (SLL) | 8.9 | 2.9 | 6.1 | 2.0 | 4.37 | 29 | <0.0001 (**) |
| THI total | 47.4 | 10.9 | 41.3 | 9.4 | 4.4 | 29 | <0.0001 (**) |
| THI (functional) | 25.1 | 9.7 | 21.9 | 8.2 | 2.57 | 29 | 0.015 (*) |
| THI (emotional) | 14.5 | 4.9 | 11.9 | 3.7 | 3.3 | 29 | 0.002 (**) |
| THI (catastrophic) | 7.7 | 3.5 | 7.4 | 2.9 | 0.68 | 29 | 0.502 |
| Before Therapy | After Therapy | Paired T-Test | |||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | t | df | p | |
| 4FA | 40.6 | 9.2 | 41.2 | 7.5 | −0.721 | 19 | 0.480 |
| PTA hf | 49.9 | 6.9 | 49.6 | 6.9 | −0.659 | 19 | 0.524 |
| Pitch | 5.7 | 1.6 | 5.4 | 1.6 | 1.37 | 19 | 0.186 |
| Loudness (SLL) | 9.3 | 2.7 | 8.5 | 2.0 | 1.22 | 19 | 0.237 |
| THI total | 47.0 | 13.8 | 52.5 | 14.5 | −1.88 | 19 | 0.075 |
| THI (functional) | 21.5 | 10.7 | 25.5 | 9.7 | −1.83 | 19 | 0.083 |
| THI (emotional) | 17.4 | 6.8 | 18.0 | 6.4 | −0.448 | 19 | 0.659 |
| THI (catastrophic) | 8.1 | 3.6 | 9.0 | 3.6 | −1.143 | 19 | 0.267 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sacchetto, L.; Monzani, D.; Apa, E.; Lovato, A.; Caragli, V.; Gherpelli, C.; Palma, S.; Genovese, E.; Nocini, R. The Effect of Alpha-Lipoic Acid in the Treatment of Chronic Subjective Tinnitus through the Tinnitus Handicap Inventory Scores. Audiol. Res. 2023, 13, 484-494. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres13040043
Sacchetto L, Monzani D, Apa E, Lovato A, Caragli V, Gherpelli C, Palma S, Genovese E, Nocini R. The Effect of Alpha-Lipoic Acid in the Treatment of Chronic Subjective Tinnitus through the Tinnitus Handicap Inventory Scores. Audiology Research. 2023; 13(4):484-494. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres13040043
Chicago/Turabian StyleSacchetto, Luca, Daniele Monzani, Enrico Apa, Andrea Lovato, Valeria Caragli, Chiara Gherpelli, Silvia Palma, Elisabetta Genovese, and Riccardo Nocini. 2023. "The Effect of Alpha-Lipoic Acid in the Treatment of Chronic Subjective Tinnitus through the Tinnitus Handicap Inventory Scores" Audiology Research 13, no. 4: 484-494. https://0-doi-org.brum.beds.ac.uk/10.3390/audiolres13040043