Changes in Cognitive Function and in the Levels of Glycosylated Haemoglobin (HbA1c) in Older Women with Type 2 Diabetes Mellitus Subjected to a Cardiorespiratory Exercise Programme

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
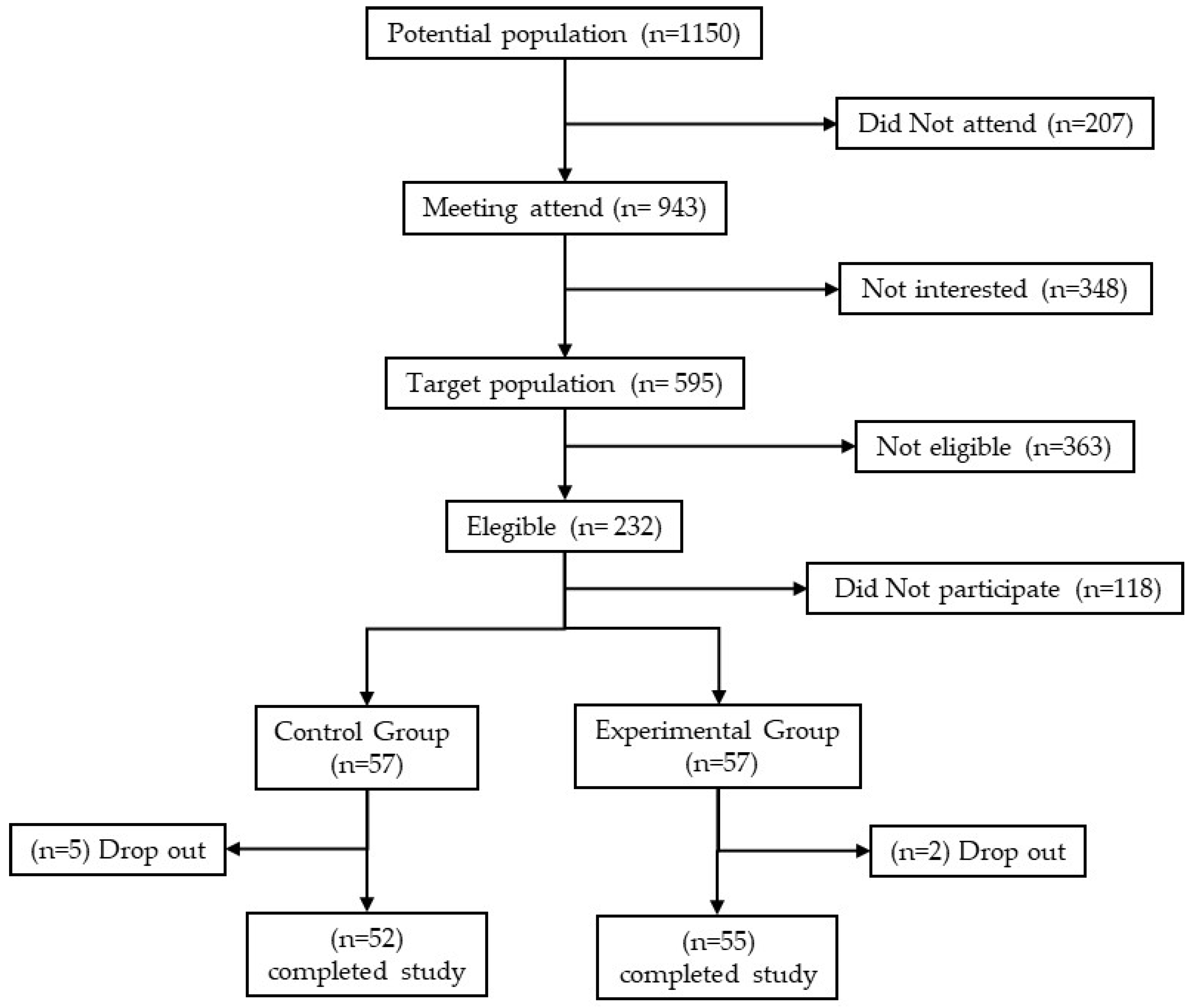
2.1. Participants
2.2. Procedure
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Cardiorespiratory Fitness
4.2. Body Mass Index
4.3. Glycosylated Haemoglobin
4.4. Cognitive State
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Naghavi, M.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Adetokunboh, O.; Afshin, A.; Agrawal, A.; et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.J.T.L. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Casals, C.; Casals Sanchez, J.L.; Suarez Cadenas, E.; Aguilar-Trujillo, M.P.; Estebanez Carvajal, F.M.; Vazquez-Sanchez, M.A. Frailty in older adults with type 2 diabetes mellitus and its relation with glucemic control, lipid profile, blood pressure, balance, disability grade and nutritional status. Nutr. Hosp. 2018, 35, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Salcedo Rocha, A.L.; Garcia de Alba, J.E.; de la Rosa Hernandez, S. Chronic pathology, frailty, and functionality in older adults from Guadalajara. Mexico. Aten. Primaria 2018, 50, 511–513. [Google Scholar] [CrossRef]
- Chao, C.-T.; Wang, J.; Chien, K.-L.; COGENT. Both pre-frailty and frailty increase healthcare utilization and adverse health outcomes in patients with type 2 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 130. [Google Scholar] [CrossRef]
- Strain, W.D.; Hope, S.V.; Green, A.; Kar, P.; Valabhji, J.; Sinclair, A.J. Type 2 diabetes mellitus in older people: A brief statement of key principles of modern day management including the assessment of frailty. A national collaborative stakeholder initiative. Diabet. Med. 2018, 35, 838–845. [Google Scholar] [CrossRef] [Green Version]
- Simpson, F.R.; Pajewski, N.M.; Nicklas, B.; Kritchevsky, S.; Bertoni, A.; Ingram, F.; Ojeranti, D.; Espeland, M.A. Impact of multidomain lifestyle intervention on frailty through the lens of deficit accumulation in adults with type 2 diabetes mellitus. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 130, 1–7. [Google Scholar] [CrossRef]
- Thein, F.S.; Li, Y.; Nyunt, M.S.Z.; Gao, Q.; Wee, S.L.; Ng, T.P. Physical frailty and cognitive impairment is associated with diabetes and adversely impact functional status and mortality. Postgrad. Med. 2018, 130, 561–567. [Google Scholar] [CrossRef]
- Meneilly, G.S.; Berard, L.D.; Cheng, A.Y.Y.; Lin, P.J.; MacCallum, L.; Tsuyuki, R.T.; Yale, J.-F.; Nasseri, N.; Richard, J.-F.; Goldin, L.; et al. Insights into the current management of older adults with type 2 diabetes in the ontario primary care setting. Can. J. Diabetes 2018, 42, 23–30. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Wang, X.; Li, F.; Xu, F.; Li, Q.; Zhang, F. Risk of depressive symptoms associated with impaired glucose metabolism, newly diagnosed diabetes, and previously diagnosed diabetes: A meta-analysis of prospective cohort studies. Acta Diabetol. 2016, 53, 589–598. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Münzenmayer, B.; Osorio, T.; Arancibia, M.; Madrid, E. Sintomatologia depresiva y control metabólico en pacientes ambulatorios portadores de diabetes mellitus tipo 2. Rev. Med. Chil. 2018, 146, 1415–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Degmecic, D.; Bacun, T.; Kovac, V.; Mioc, J.; Horvat, J.; Vcev, A. Depression, anxiety and cognitive dysfunction in patients with type 2 diabetes mellitus--a study of adult patients with type 2 diabetes mellitus in Osijek, Croatia. Coll. Antropol. 2014, 38, 711–716. [Google Scholar] [PubMed]
- Kotsani, M.; Chatziadamidou, T.; Economides, D.; Benetos, A. Higher prevalence and earlier appearance of geriatric phenotypes in old adults with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2018, 135, 206–217. [Google Scholar] [CrossRef] [PubMed]
- Nogueira Costa, L.D.L.; Medeiros Verzaro, P.; Lopes Ericeira, V.V.; de Lima Sardinha, A.H. Cognitive deficit in older women with Type 2 Diabetes Mellitus. J. Nurs. UFPE 2016, 10, 2818–2824. [Google Scholar] [CrossRef]
- Bangen, K.J.; Werhane, M.L.; Weigand, A.J.; Edmonds, E.C.; Delano-Wood, L.; Thomas, K.R.; Nation, D.A.; Evangelista, N.D.; Clark, A.L.; Liu, T.T.; et al. Reduced regional cerebral blood flow relates to poorer cognition in older adults with type 2 diabetes. Front. Aging Neurosci. 2018, 10, 270. [Google Scholar] [CrossRef] [Green Version]
- Buss, S.S.; Padmanabhan, J.; Saxena, S.; Pascual-Leone, A.; Fried, P.J. Atrophy in distributed networks predicts cognition in alzheimer’s disease and type 2 diabetes. J. Alzheimers Dis. 2018, 65, 1301–1312. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Wang, C.; Tian, S.; Huang, R.; Guo, D.; Zhang, H.; Shi, J.; Wang, S. Higher plasma level of nampt presaging memory dysfunction in chinese type 2 diabetes patients with mild cognitive impairment. J. Alzheimers Dis. 2019, 70, 303–314. [Google Scholar] [CrossRef]
- Zheng, F.; Yan, L.; Yang, Z.; Zhong, B.; Xie, W. HbA1c, diabetes and cognitive decline: The English Longitudinal Study of Ageing. Diabetologia 2018, 61, 839–848. [Google Scholar] [CrossRef] [Green Version]
- West, R.K.; Ravona-Springer, R.; Schmeidler, J.; Leroith, D.; Koifman, K.; Guerrero-Berroa, E.; Preiss, R.; Hoffman, H.; Silverman, J.M.; Heymann, A.; et al. The association of duration of type 2 diabetes with cognitive performance is modulated by long-term glycemic control. Am. J. Geriatr. Psychiatry 2014, 22, 1055–1059. [Google Scholar] [CrossRef] [Green Version]
- Wium-Andersen, I.K.; Rungby, J.; Jørgensen, M.B.; Sandbæk, A.; Osler, M.; Wium-Andersen, M.K. Risk of dementia and cognitive dysfunction in individuals with diabetes or elevated blood glucose. Epidemiol. Psychiatr. Sci. 2020, 29, e43. [Google Scholar] [CrossRef] [Green Version]
- Pappas, C.; Small, B.J.; Andel, R.; Laczo, J.; Parizkova, M.; Ondrej, L.; Hort, J. Blood glucose levels may exacerbate executive function deficits in older adults with cognitive impairment. J. Alzheimers Dis. 2019, 67, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Duarte, S.; Hoang, T.; Ewing, S.K.; Cawthon, P.M.; Cummings, S.; Stone, K.L.; Cauley, J.A.; Bauer, D.C.; Hillier, T.A.; Yaffe, K. Glycated peptide levels are associated with cognitive decline among nondiabetic older women. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 74, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Mehta, B.K.; Singh, K.K.; Banerjee, S. Effect of exercise on type 2 diabetes-associated cognitive impairment in rats. Int. J. Neurosci. 2019, 129, 252–263. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, H.; Teo, W.-P.; Schneider, L.A.; Smith, A.E. A life-long approach to physical activity for brain health. Front. Aging Neurosci. 2017, 9, 147. [Google Scholar] [CrossRef] [PubMed]
- Podolski, N.; Brixius, K.; Predel, H.G.; Brinkmann, C. Effects of regular physical activity on the cognitive performance of type 2 diabetic patients: A systematic review. Metab. Syndr. Relat. Disord. 2017, 15, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Espeland, M.A.; Lipska, K.; Miller, M.E.; Rushing, J.; Cohen, R.A.; Verghese, J.; McDermott, M.M.; King, A.C.; Strotmeyer, E.S.; Blair, S.N.; et al. Effects of physical activity intervention on physical and cognitive function in sedentary adults with and without diabetes. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 861–866. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Uricoechea, H.; Casas-Figueroa, L.Á. Epidemiología de la diabetes mellitus en Sudamérica: La experiencia de Colombia. Clínica Investig. Arterioscler. 2016, 28, 245–256. [Google Scholar] [CrossRef]
- Zhao, R.R.; O’Sullivan, A.J.; Fiatarone Singh, M.A. Exercise or physical activity and cognitive function in adults with type 2 diabetes, insulin resistance or impaired glucose tolerance: A systematic review. Eur. Rev. Aging Phys. Act. 2018, 15, 1. [Google Scholar] [CrossRef] [Green Version]
- Dyer, A.H.; Briggs, R.; Mockler, D.; Gibney, J.; Kennelly, S.P. Non-pharmacological interventions for cognition in patients with Type 2 diabetes mellitus: A systematic review. QJM 2020, 113, 155–161. [Google Scholar] [CrossRef]
- WMA. World Medical Association declaration of helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Quiroga, L.P.; Albala, B.C.; Klaasen, P.G. Validación de un test de tamizaje para el diagnóstico de demencia asociada a edad, en Chile. Rev. Med. Chil. 2004, 132, 467–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llamas-Velasco, S.; Llorente-Ayuso, L.; Contador, I.; Bermejo-Pareja, F. Spanish versions of the Minimental State Examination (MMSE). Questions for their use in clinical practice. Rev. Neurol. 2015, 61, 363–371. [Google Scholar] [PubMed]
- Muñoz Silva, C.A.; Rojas Orellana, P.A.; Marzuca-Nassr, G.N. Criterios de valoración geriátrica integral en adultos mayores con dependencia moderada y severa en Centros de Atención Primaria en Chile. Rev. Med. Chil. 2015, 143, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Laskin, J.J.; Bundy, S.; Marron, H.; Moore, H.; Swanson, M.; Blair, M.; Humphrey, R. Using a treadmill for the 6-minute walk test—Reliability and validity. J. Cardiopulm. Rehabil. Prev. 2007, 27, 407–410. [Google Scholar] [CrossRef]
- Salci, Y.; Karanfil, E.; Balkan, A.F.; Kutukcu, E.C.; Ceren, A.N.; Ayvat, F.; Bekircan-Kurt, C.E.; Armutlu, K. Functional exercise capacity evaluated by timed walk tests in myasthenia gravis. Muscle Nerve 2019, 59, 208–212. [Google Scholar] [CrossRef] [Green Version]
- Sperandio, E.F.; Arantes, R.L.; Matheus, A.C.; Silva, R.P.; Lauria, V.T.; Romiti, M.; Gagliardi, A.R.T.; Dourado, V.Z. Intensity and physiological responses to the 6-minute walk test in middle-aged and older adults: A comparison with cardiopulmonary exercise testing. Braz. J. Med. Biol. Res. 2015, 48, 349–353. [Google Scholar] [CrossRef] [Green Version]
- Racodon, M.; Porrovecchio, A.; Pezé, T. Use of the 6-minute walk test to assess the pursuit of physical activity after cardiac rehabilitation. Rech. Soins Infirm. 2019, 137, 18–25. [Google Scholar] [CrossRef]
- Giannitsi, S.; Bougiakli, M.; Bechlioulis, A.; Kotsia, A.; Michalis, L.K.; Naka, K.K. 6-minute walking test: A useful tool in the management of heart failure patients. Ther. Adv. Cardiovasc. Dis. 2019, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sakai, Y.; Yamamoto, S.; Hoshina, M.; Kawachi, S.; Ichiyama, T.; Hanaoka, M. Using SpO2 recovery index after a 6-minute walk test to predict respiratory-related events in hospitalized patients with interstitial pneumonia. Sci. Rep. 2019, 9, 15226. [Google Scholar] [CrossRef]
- Lee, M.C. Validity of the 6-minute walk test and step test for evaluation of cardio respiratory fitness in patients with type 2 diabetes mellitus. J. Exerc. Nutr. Biochem. 2018, 22, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Meléndez, A.; Arias Vázquez, P.I.; Lucatero Lecona, I.; Luna Garza, R. Correlation between the six-minute walk test and maximal exercise test in patients with type ii diabetes mellitus. Rehabilitacion 2019, 53, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.L.S.; Pin, T.W. Reliability, validity and minimal detectable change of 2-minute walk test, 6-minute walk test and 10-meter walk test in frail older adults with dementia. Exp. Gerontol. 2019, 115, 9–18. [Google Scholar] [CrossRef]
- Peralta-Brenes, M.; Briceno-Torres, J.M.; Chacon-Araya, Y.; Moncada-Jimenez, J.; Salazar-Villanea, M.; Johnson, D.K.; Campos-Salazar, C. Prediction o peak aerobic power among costa rican older adults. J. Clin. Diagn. Res. 2018, 12, CC1–CC4. [Google Scholar] [CrossRef]
- Langhammer, B.; Bergland, A.; Rydwik, E. The importance of physical activity exercise among older people. BioMed Res. Int. 2018, 2018, 7856823. [Google Scholar] [CrossRef] [PubMed]
- Outayanik, B.; Carvalho, J.; Seabra, A.; Rosenberg, E.; Krabuanrat, C.; Chalermputipong, S.; Suwankan, S.; Sirisopon, N.; Rachrujithong, P.; Thanak, W.; et al. Effects of a physical activity intervention program on nutritional status and health-related physical fitness in thai older adults: Pilot study. Asian J. Sports Med. 2017, 8, e37508. [Google Scholar] [CrossRef] [Green Version]
- Viken, H.; Aspvik, N.P.; Ingebrigtsen, J.E.; Zisko, N.; Wisløff, U.; Stensvold, D. Correlates of objectively measured physical activity among norwegian older adults: The generation 100 study. J. Aging Phys. Act. 2016, 24, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Pollock, R.D.; Duggal, N.A.; Lazarus, N.R.; Lord, J.M.; Harridge, S.D.R. Cardiorespiratory fitness not sedentary time or physical activity is associated with cardiometabolic risk in active older adults. Scand. J. Med. Sci. Sports 2018, 28, 1653–1660. [Google Scholar] [CrossRef] [Green Version]
- LaRoche, D.P.; Melanson, E.L.; Baumgartner, M.P.; Bozzuto, B.M.; Libby, V.M.; Marshall, B.N. Physiological determinants of walking effort in older adults: Should they be targets for physical activity intervention? Geroscience 2018, 40, 305–315. [Google Scholar] [CrossRef]
- Halloway, S.; Wilbur, J.; Schoeny, M.E.; Semanik, P.A.; Marquez, D.X. Combined effects of sedentary behavior and moderate-to-vigorous physical activity on cardiovascular health in older, community-dwelling Latinos. J. Aging Phys. Act. 2016, 24, 296–304. [Google Scholar] [CrossRef]
- Bowden Davies, K.A.; Pickles, S.; Sprung, V.S.; Kemp, G.J.; Alam, U.; Moore, D.R.; Tahrani, A.A.; Cuthbertson, D.J. Reduced physical activity in young and older adults: Metabolic and musculoskeletal implications. Ther. Adv. Endocrinol. Metab. 2019, 10. [Google Scholar] [CrossRef]
- Elhakeem, A.; Hannam, K.; Deere, K.C.; Hartley, A.; Clark, E.M.; Moss, C.; Edwards, M.H.; Dennison, E.; Gaysin, T.; Kuh, D.; et al. Physical activity producing low, but not medium or higher, vertical impacts is inversely related to BMI in older adults: Findings from a multicohort study. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 643–651. [Google Scholar] [CrossRef] [Green Version]
- Stewart-Knox, B.; Duffy, E.M.; Bunting, B.; Parr, H.; Vas De Almeida, M.D.; Gibney, M. Associations between obesity (BMI and waist circumference) and socio-demographic factors, physical activity, dietary habits, life events, resilience, mood, perceived stress and hopelessness in healthy older Europeans. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [Green Version]
- Melo, K.C.B.; Araújo, F.S.; Cordeiro Júnior, C.C.M.; de Andrade, K.T.P.; Moreira, S.R. Pilates method training: Functional and blood glucose responses of older women with type 2 diabetes. J. Strength Cond. Res. 2020, 34, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Tan, S.; Wang, Z.; Guo, Z.; Li, Q.; Wang, J. Aerobic exercise training at maximal fat oxidation intensity improves body composition, glycemic control, and physical capacity in older people with type 2 diabetes. J. Exerc. Sci. Fit. 2020, 18, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; White, K.; O’Shields, K.R.; McLain, A.C.; Merchant, A.T. Light-intensity physical activity and cardiometabolic risk among older adults with multiple chronic conditions. Am. J. Health Promot. 2019, 33, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Li, G.; Jiang, S.; Yin, H.; Liu, P.; Chen, L. Effect of low-intensity, Kinect™-based Kaimai-style Qigong exercise in older adults with type 2 diabetes. J. Gerontol. Nurs. 2019, 45, 42–52. [Google Scholar] [CrossRef]
- Mendoza-Núñez, V.M.; Arista-Ugalde, T.L.; Rosado-Pérez, J.; Ruiz-Ramos, M.; Santiago-Osorio, E. Hypoglycemic and antioxidant effect of Tai Chi exercise training in older adults with metabolic syndrome. Clin. Interv. Aging 2018, 13, 523–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, R.; Sousa, N.; Reis, V.M.; Themudo-Barata, J.L. Implementing low-cost, community-based exercise programs for middle-aged and older patients with type 2 diabetes: What are the benefits for glycemic control and cardiovascular risk? Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef] [Green Version]
- Ng, C.L.; Goh, S.Y.; Malhotra, R.; Østbye, T.; Tai, E.S. Minimal difference between aerobic and progressive resistance exercise on metabolic profile and fitness in older adults with diabetes mellitus: A randomised trial. J. Physiother. 2010, 56, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Baptista, L.C.; MacHado-Rodrigues, A.M.; Martins, R.A. Back to basics with active lifestyles: Exercise is more effective than metformin to reduce cardiovascular risk in older adults with type 2 diabetes. Biol. Sport 2018, 35, 363–372. [Google Scholar] [CrossRef]
- Esain, I.; Rodriguez-Larrad, A.; Bidaurrazaga-Letona, I.; Gil, S.M. Exercise cessation in active older adults: Effects on inflammatory markers and adiponectin. Geriatr. Gerontol. Int. 2020, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Leite, N.J.C.; Mendes, R.D.C.; Raimundo, A.M.M.; Pinho, C.; Viana, J.L.; Marmeleira, J.F.F. Impact of a supervised multicomponent physical exercise program on cognitive functions in patients with type 2 diabetes. Geriatr. Nurs. 2020. [Google Scholar] [CrossRef]
- Molina-Sotomayor, E.; Orb, M.G.; de la Fuente, F.P.; Figueroa, G.C.; Sánchez-Oliver, A.J.; González-Jurado, J.A. Effects of cardiorespiratory exercise on cognition in older women exposed to air pollution. Int. J. Environ. Res. Public Health 2019, 16, 245. [Google Scholar] [CrossRef] [Green Version]
- Molina-Sotomayor, E.; Arreguín-Moreno, R.; Rodríguez-Rodríguez, F.; Pradas, F.; León, J.A.; González-Jurado, J.A. Effects of exercise on the cognition of older women treated with lovastatin. Biomedica 2018, 38, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, A.V.; Barbosa, A.R.; Meneghini, V. Active videogame-based physical activity vs. Aerobic exercise and cognitive performance in older adults: A randomized controlled trial. J. Phys. Educ. Sport. 2018, 18, 203–209. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Briken, S.; Gold, S.M.; Patra, S.; Vettorazzi, E.; Harbs, D.; Tallner, A.; Ketels, G.; Schulz, K.H.; Heesen, C. Effects of exercise on fitness and cognition in progressive MS: A randomized, controlled pilot trial. Mult. Scler. J. 2014, 20, 382–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haripriya, S.; Dhanesh Kumar, K.U.; Samuel, S.E.; Ajith, S. The effect of a multicomponent exercise program on cognitive function and functional ability in community dwelling older adults. Int. J. Res. Pharm. Sci. 2020, 11, 109–114. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Cadore, E.L.; Galbete, A.; Izquierdo, M. Assessing the impact of physical exercise on cognitive function in older medical patients during acute hospitalization: Secondary analysis of a randomized trial. PLoS Med. 2019, 16, e1002852. [Google Scholar] [CrossRef]
- Chang, M.; Ramel, A.; Jonsson, P.V.; Thorsdottir, I.; Geirsdottir, O.G. The effect of cognitive function on mobility improvement among community-living older adults: A 12-week resistance exercise intervention study. Aging Neuropsych. Cogn. 2019, 27, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, R.B.; Marins, J.C.B.; Amorim, P.R.S.; Teoldo, I.; Cupeiro, R.; Andrade, M.O.C.D.; Martins, Y.D.L.X.; Castilho, P.D.R.; Magalhães, D.D.; Palotás, A.; et al. Evaluating the effects of exercise on cognitive function in hypertensive and diabetic patients using the mental test and training system. World J. Biol. Psychiatry 2019, 20, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Callisaya, M.L.; Daly, R.M.; Sharman, J.E.; Bruce, D.; Davis, T.M.E.; Greenaway, T.; Nolan, M.; Beare, R.; Schultz, M.G.; Phan, T.; et al. Feasibility of a multi-modal exercise program on cognition in older adults with Type 2 diabetes—A pilot randomised controlled trial. BMC Geriatr. 2017, 17, 237. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Experimental Group (n = 55) | Control Group (n = 52) | |||
|---|---|---|---|---|
| Mean ± SD | 95% (CI) | Mean ± SD | 95% (CI) | |
| Age (years) | 72.3 ± 3.7 | (71.3 to 73.3) | 71 ± 3.3 | (70.1 to 72) |
| Weight (kg) | 60.8 ± 3.7 | (59.7 to 61.8) | 60.1 ± 3.5 | (59.1 to 61.1) |
| Height (m) | 1.54 ± 0.05 | (1.52 to 1.55) | 1.53 ± 0.04 | (1.51 to 1.54) |
| Primary school completed | 100% | 100% | ||
| High school completed | 92% | 89% | ||
| Mesocycle 1 | Mesocycle 2 | Mesocycle 3 | Mesocycle 4 | Mesocycle 5 | Mesocycle 6 | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Week | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 |
| %VO2max | 40 | 45 | 40 | 45 | 50 | 45 | 50 | 45 | 50 | 55 | 50 | 55 | 50 | 55 | 55 | 60 | 50 | 60 | 55 | 60 | 65 | 55 | 60 | 65 |
| Speed (m/min) | 56.2 | 67.6 | 56.2 | 67.6 | 79.0 | 67.6 | 79.6 | 67.6 | 79.0 | 90.4 | 79.0 | 90.4 | 79.0 | 90.4 | 90.4 | 102 | 79.9 | 102 | 90.4 | 102 | 112 | 90.4 | 102 | 112 |
| Speed (km/h) | 3.3 | 4.0 | 3.3 | 4.0 | 4.7 | 4.0 | 3.3 | 4.0 | 4.7 | 5.4 | 4.7 | 5.4 | 4.7 | 5.4 | 5.4 | 6.1 | 4.7 | 6.1 | 5.4 | 6.1 | 6.3 | 5.4 | 6.1 | 6.3 |
| METs | 2.2 | 2.5 | 2.2 | 2.5 | 2.7 | 2.5 | 2.7 | 2.5 | 2.7 | 3.0 | 2.7 | 3.0 | 2.7 | 3.0 | 3.0 | 3.3 | 2.7 | 3.3 | 3.0 | 3.3 | 3.6 | 3.0 | 3.3 | 3.6 |
| Kcal/min | 2.8 | 3.2 | 2.8 | 3.2 | 3.6 | 3.2 | 3.6 | 3.2 | 3.6 | 3.9 | 3.6 | 3.9 | 3.6 | 3.9 | 3.9 | 4.3 | 3.6 | 4.3 | 3.9 | 4.3 | 4.6 | 3.9 | 4.3 | 4.6 |
| Experimental Group (n = 55) | |||||||
|---|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Effect Size | Magnitude | |||
| Mean ± SD | 95% (CI) | Mean ± SD | 95% (CI) | ||||
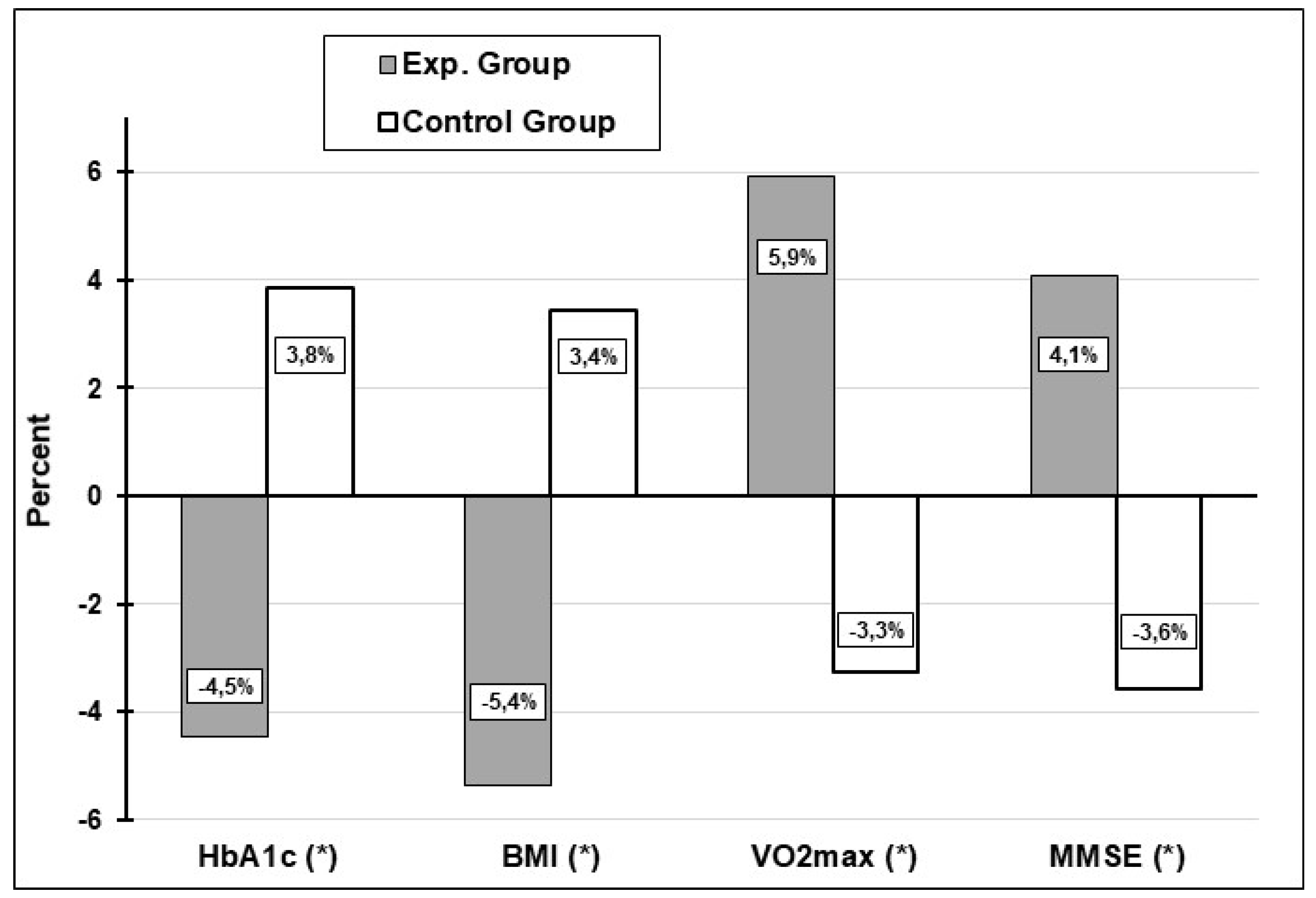
| HbA1c (a) | 8.10 ± 0.47 | (7.97 to 8.2) | 7.73 ± 0.55 | (7.6 to 7.9) | <0.001 | −0.66 | Medium |
| BMI (a) | 25.54 ± 2.17 | (24.9 to 26.1) | 24.13 ± 2.18 | (23.5 to 24.7) | <0.001 | −0.64 | Medium |
| VO2max (a) | 19.24 ± 1.64 | (18.8 to 19.7) | 20.35 ± 1.82 | (19.8 to 20.8) | <0.001 | 0.61 | Medium |
| MMSE (b) | 23.04 ± 0.69 | (22.8 to 23.2) | 23.96 ± 0.98 | (23.7 to 24.2) | <0.001 | 0.95 | Large |
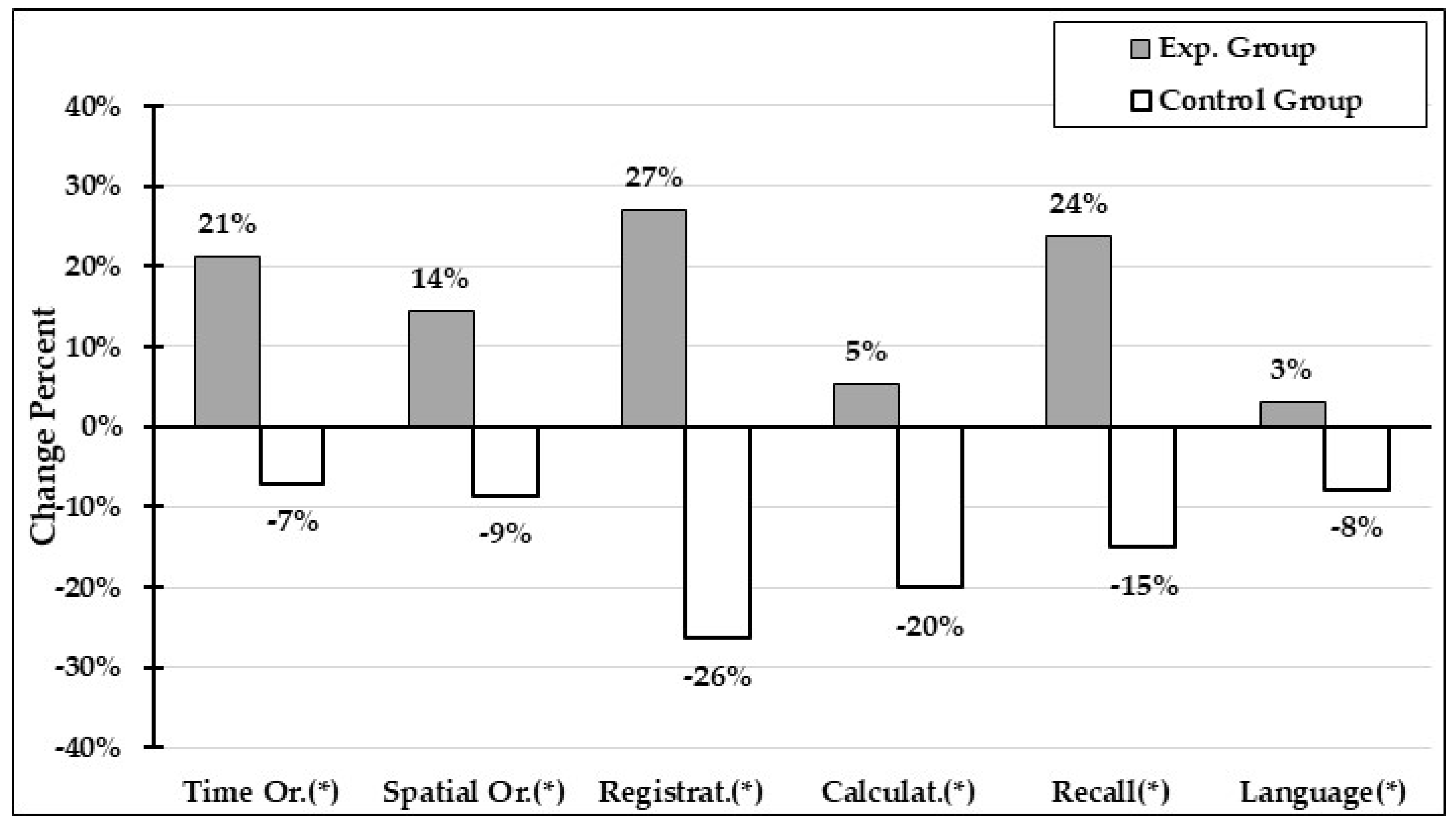
| Time Or. (b) | 3.71 ± 0.63 | (3.54 to 3.88) | 4.38 ± 0.59 | (4.22 to 4.54) | <0.001 | 1.10 | Large |
| Spatial Or. (b) | 3.76 ± 0.58 | (3.61 to 3.92) | 4.20 ± 0.59 | (4.04 to 4.36) | 0.001 | 0.75 | Medium |
| Registration (b) | 2.02 ± 0.62 | (1.85 to 2.19) | 2.36 ± 0.59 | (2.20 to 2.52) | 0.001 | 0.57 | Medium |
| Calculation (b) | 3.44 ± 0.66 | (3.26 to 3.61) | 3.53 ± 0.72 | (3.33 to 3.72) | 0.384 | 0.13 | Trivial |
| Recall (b) | 2.35 ± 0.67 | (2.16 to 2.53) | 2.62 ± 0.49 | (2.49 to 2.75) | 0.009 | 0.46 | Medium |
| Language (b) | 1.29 ± 0.17 | (1.24 to 1.34) | 1.32 ± 0.13 | (1.28 to 1.35) | 0.168 | 0.18 | Trivial |
| Control Group (n = 52) | |||||||
|---|---|---|---|---|---|---|---|
| Pre | Post | p-Value | Effect Size | Magnitude | |||
| Mean ± SD | 95% (CI) | Mean ± SD | 95% (CI) | ||||
| HbA1c (a) | 8.14 ± 0.51 | (8 to 8.3) | 8.45 ± 0.56 | (8.3 to 8.6) | <0.001 | 0.56 | Medium |
| BMI (a) | 25.71 ± 2.29 | (25.1 to 26.3) | 26.6 ± 2.44 | (25.9 to 27.3) | <0.001 | 0.36 | Small |
| VO2max (a) | 19.35 ± 1.53 | (18.9 to 19.8) | 18.6 ± 1.27 | (18.3 to 19) | <0.001 | −0.55 | Medium |
| MMSE (b) | 23.33 ± 0.65 | (23.1 to 23.5) | 22.5 ± 0.98 | (22.2 to 22.7) | <0.001 | −0.86 | Large |
| Time Or (b) | 3.65 ± 0.68 | (3.46 to 3.84) | 3.31 ± 0.64 | (3.13 to 3.49) | 0.002 | −0.52 | Medium |
| Spatial Or (b) | 3.81 ±0.56 | (3.65 to 3.96) | 3.44 ± 0.75 | (3.23 to 3.65) | 0.002 | −0.55 | Medium |
| Registrat. (b) | 1.96 ± 0.39 | (1.85 to 2.07) | 1.48 ± 0.73 | (1.28 to 1.68) | <0.001 | −0.82 | Large |
| Calculat. (b) | 3.35 ±0.76 | (3.13 to 3.56) | 2.67 ± 0.78 | (2.45 to 2.89) | <0.001 | −0.87 | Large |
| Recall (b) | 2.42 ± 0.67 | (2.24 to 2.61) | 2.04 ± 0.74 | (1.83 to 2.24) | <0.001 | −0.55 | Medium |
| Language (b) | 1.31 ±0.16 | (1.27 to 1.35) | 1.20 ± 0.18 | (1.15 to 1.25) | <0.001 | −0.67 | Medium |
| Change Exp. Group (n = 55) | Change Control Group (n = 52) | p-Value | Effect Size | Magnitude | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | 95% (CI) | Mean ± SD | 95% (CI) | ||||
| HbA1c (a) | −0.36 ± 0.31 | (−0.45 to 0.28) | 0.31 ± 0.30 | (0.23 to 0.39) | <0.001 | 2.20 | Large |
| BMI (a) | −1.41 ± 1.63 | (−1.85 to −0.96) | 0.88 ± 0.64 | (0.70 to 1.06) | <0.001 | 1.82 | Large |
| VO2max (a) | 1.11 ± 1.20 | (0.79 to 1.43) | −0.69 ± 1.31 | (−1.06 to −0.33) | <0.001 | −1.44 | Large |
| MMSE (b) | 0.93 ± 1.1 | (0.63 to 1.23) | −0.85 ± 1.04 | (−1.13 to −0.56) | <0.001 | −1.66 | Large |
| Time Or (b) | 0.67 ± 0.79 | (0.46 to 0.89) | −0.35 ± 0.74 | (−0.55 to −0.14) | <0.001 | −1.33 | Large |
| Spatial Or (b) | 0.44 ± 0.83 | (0.21 to 0.66) | −0.37 ± 0.77 | (−0.58 to −0.15) | <0.001 | −1.00 | Large |
| Registrat. (b) | 0.35 ± 0.70 | (0.16 to 0.53) | −0.48 ± 0.61 | (−0.65 to −0.31) | <0.001 | −1.26 | Large |
| Calculat. (b) | 0.09 ± 0.78 | (−0.12 to 0.30) | −0.67 ± 0.55 | (−0.83 to −0.52) | <0.001 | −1.13 | Large |
| Recall (b) | 0.27 ± 0.73 | (0.07 to 0.47) | −0.38 ± 0.66 | (−0.57 to −0.20) | <0.001 | −0.94 | Large |
| Language (b) | 0.03 ± 0.15 | (−0.01 to 0.07) | −0.11 ± 0.16 | (−0.15 to −0.06) | <0.001 | −0.88 | Large |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Sotomayor, E.; Onetti-Onetti, W.; Castillo-Rodríguez, A.; González-Jurado, J.A. Changes in Cognitive Function and in the Levels of Glycosylated Haemoglobin (HbA1c) in Older Women with Type 2 Diabetes Mellitus Subjected to a Cardiorespiratory Exercise Programme. Sustainability 2020, 12, 5038. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125038
Molina-Sotomayor E, Onetti-Onetti W, Castillo-Rodríguez A, González-Jurado JA. Changes in Cognitive Function and in the Levels of Glycosylated Haemoglobin (HbA1c) in Older Women with Type 2 Diabetes Mellitus Subjected to a Cardiorespiratory Exercise Programme. Sustainability. 2020; 12(12):5038. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125038
Chicago/Turabian StyleMolina-Sotomayor, Edgardo, Wanesa Onetti-Onetti, Alfonso Castillo-Rodríguez, and Jose Antonio González-Jurado. 2020. "Changes in Cognitive Function and in the Levels of Glycosylated Haemoglobin (HbA1c) in Older Women with Type 2 Diabetes Mellitus Subjected to a Cardiorespiratory Exercise Programme" Sustainability 12, no. 12: 5038. https://0-doi-org.brum.beds.ac.uk/10.3390/su12125038