Municipal Health Promotion as Part of Urban Health: A Policy Framework for Action

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Method
3. Results
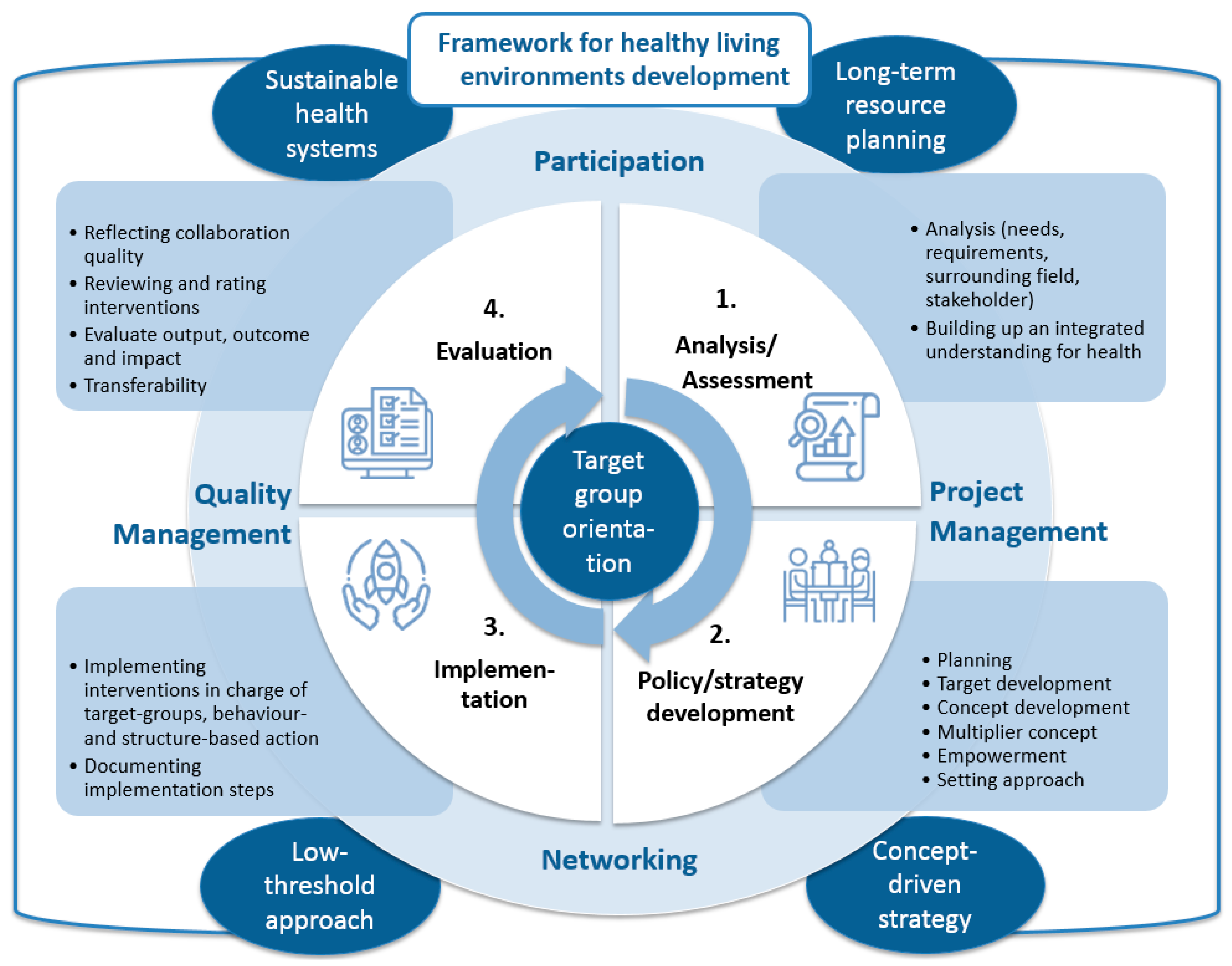
Creating Healthy Living Environments and Actual Evidence of Community Health Promotion and Prevention
- Targeted interventions
- Universal policies
- Redistributive policies
- Proportionate universalism (targeted and universal policies)
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Policy, S.F.E. Links between noise and air pollution and socioeconomic status. In In-Depth Report 13 Produced for the European Commission, DG Environment by the Science Communication Unit; UWE: Bristol, CT, USA, 2016; Available online: http://ec.europa.eu/science-environment-policy.pdf (accessed on 6 December 2018).
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.G.; Basu, N.; Balde, A.B.; Bertollini, R.; Boseoreilly, S.; Boufford, J.I.M.; et al. The Lancet Commission on pollution and health. Lancet 2018, 391, 462–512. [Google Scholar] [CrossRef] [Green Version]
- Diderichsen, F.; Andersen, I.; Manuel, C.; Andersen, A.N.; Bach, E.; Baadsgaard, M.; Bronnumhansen, H.; Hansen, F.K.; Jeune, B.; Jorgensen, T.; et al. Health Inequality-determinants and policies. Scand. J. Public Health 2012, 40, 12–105. [Google Scholar] [CrossRef] [Green Version]
- Boyce, T.; Brown, C.; World Health Organization (WHO). Engagement and Participation for Health Equity. In A Core Principle of Health 2020 is Reducing Health Inequities across the Population, Along with the Importance of Participation and Responsiveness, with the Full Engagement of People; 2017; Available online: https://tinyurl.com/y74rvwk8 (accessed on 25 March 2020).
- Cushing, L.; Morellofrosch, R.; Wander, M.; Pastor, M. The haves, the have-nots, and the health of everyone: The relationship between social inequality and environmental quality. Annu. Rev. Public Health 2015, 36, 193–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Children’s Bureau. Environmental Inequalities and Their Impact on the Health Outcomes of Children and Young People. In Policy and Evidence Briefing; 2012; Available online: https://tinyurl.com/y92sxwce (accessed on 25 March 2020).
- Marmot, M.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I. The Marmot review: Fair Society, Healthy Lives. Strategic Review of Health Inequalities in England Post-2010; The Marmot Review; University College London: London, UK, 2010. [Google Scholar]
- Morellofrosch, R.; Zuk, M.; Jerrett, M.; Shamasunder, B.; Kyle, A.D. Understanding the cumulative impacts of inequalities in environmental health: Implications for policy. Health Aff. 2011, 30, 879–887. [Google Scholar] [CrossRef] [PubMed]
- European Union. EU Gesundheitsprogramm. Available online: https://ec.europa.eu/health/funding/programme_de (accessed on 9 July 2020).
- Tountas, Y.; Dimitrakaki, C.; Bollars, C.; van den Broucke, S.; Kok, H.; Molleman, G. Evaluating quality in health promotion: The EQUIHP. Arch. Hell. Med. 2007, 24, 75. [Google Scholar]
- Gesundheitliche-Chancengleichheit. Good Practice-Kriterien. Available online: https://www.gesundheitliche-chancengleichheit.de/good-practice-kriterien/ (accessed on 12 July 2020).
- JANPA. Janpa Toolbox. Available online: https://janpa-toolbox.eu/ (accessed on 12 July 2020).
- Chrodis. CHRODIS. Available online: http://chrodis.eu/ (accessed on 11 July 2020).
- Inherit. Inherit Model. Available online: https://www.inherit.eu/project/inherit-model/ (accessed on 10 July 2020).
- Quilling, E.; Kruse, S. Evidenzlage Kommunaler Strategien der Prävention und Gesundheitsförderung: Eine Literatur- und Datenbankrecherche (Rapid Review); On Behalf of GKV-Spitzenverband: Berlin, Germany, 2018. [Google Scholar]
- Rosenbrock, R. Public health as a social innovation. Gesundheitswesen 1995, 57, 140. [Google Scholar]
- Rosenbrock, R.; Gerlinger, T. Gesundheitspolitik: Eine Systematische Einführung; Verlag Hans Huber: Bern, Switzerland, 2014. [Google Scholar]
- Dahlgren, G.; Whitehead, M. Policies and Strategies to Promote Social Equity in Health; Institut for Future Studies: Stockhom, Sweden, 1991. [Google Scholar]
- Benach, J.; Malmusi, D.; Yasui, Y.; Martínez, J.M. A new typology of policies to tackle health inequalities and scenarios of impact based on Rose’s population approach. J. Epidemiol. Community Health 2013, 67, 286–291. [Google Scholar] [CrossRef]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. Levelling up (part 2): A Discussion Paper on European Strategies for Tackling Social Inequities in Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- World Health Organization (WHO). Ottawa Charter for Health Promotion; Copenhagen, Denmark, 1986. Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/129532/Ottawa_Charter.pdf (accessed on 25 March 2020).
- Barton, H.; Grant, M. Urban planning for healthy cities. J. Urban Health 2013, 90, 129–141. [Google Scholar] [CrossRef] [Green Version]
- Baumgart, S.; Köckler, H.; Ritzinger, A.; Rüdiger, A. Lanung für Gesundheitsfördernde Städte; Akademie für Raumentwicklung in der Leibniz-Gemeinschaft: Hannover, Germany, 2018. [Google Scholar]
- World Health Organization. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Köckler, H. Umweltbezogene Gerechtigkeit: Anforderungen an Eine Zukunftsweisende Stadtplanung; Peter Lang GmbH, Internationaler Verlag der Wissenschaften: Bern, Switzerland, 2017. [Google Scholar]
- Nutbeam, D. Evaluating health promotion—Progress, problems and solutions. Health Promot. Int. 1998, 13, 27–44. [Google Scholar] [CrossRef]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood environments and socioeconomic inequalities in mental well-being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef]
- Bucksch, J.; Schneider, S. Walkability: Das Handbuch zur Bewegungsförderung in der Kommune; Verlag Hans Huber: Bern, Switzerland, 2014. [Google Scholar]
- Galvez, M.P.; Pearl, M.; Yen, I.H. Childhood obesity and the built environment: A review of the literature from 2008–2009. Curr. Opin. Pediatrics 2010, 22, 202. [Google Scholar] [CrossRef] [Green Version]
- Poland, B.; Dooris, M. A green and healthy future: The settings approach to building health, equity and sustainability. Crit. Public Health 2010, 20, 281–298. [Google Scholar] [CrossRef]
- Goldfeld, S.; Oconnor, E.; Oconnor, M.; Sayers, M.; Moore, T.; Kvalsvig, A.; Brinkman, S. The role of preschool in promoting children’s healthy development: Evidence from an Australian population cohort. Early Child. Res. Q. 2016, 35, 40–48. [Google Scholar] [CrossRef]
- Foran, C. How to design a city for women. Citylab. Available online: https://www.citylab.com/transportation/2013/09/how-design-city-women/6739/ (accessed on 28 December 2018).
- Böhme, C.; Bunge, C.; Preuß, T. Umweltgerechtigkeit in der Stadt—Zur integrierten Betrachtung von Umwelt, Gesundheit, Sozialem und Stadtentwicklung in der kommunalen Praxis. Umweltpsychologie 2016, 20, 137–157. [Google Scholar]
- Große, J.; Menkouo, C.; Grande, G. Nachhaltige Strategien für die stadtteilbezogene Gesundheitsförderung. Gesundheitswesen 2015, 77, S116–S117. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, M.; Honeycutt, T.; Orfield, C.; Vine, M.; Cabili, C.; Morzuch, M.; Fisher, S.K.; Briefel, R. The Healthy Weight Collaborative: Using learning collaboratives to enhance community-based prevention initiatives addressing childhood obesity. J. Health Care Poor Underserved 2013, 24, 103–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, N.; Sandor, M. Defining sustainable practice in community-based health promotion: A Delphi study of practitioner perspectives. Health Promot. J. Aust. 2013, 24, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Reimann, B.; Böhme, C.; Bär, G. Mehr Gesundheit im Quartier. Prävention und Gesundheitsförderung in der Stadtteilentwicklung; Deutsches Institut für Urbanistik: Cologne, Germany, 2010. [Google Scholar]
- Rütten, A.; Wolff, A.; Streber, A. Interaktiver Wissenstransfer in der Gesundheitsförderung: Das GESTALT-Projekt. Erste Ergebnisse der Erprobung eines Ansatzes zur nachhaltigen Implementierung evidenzbasierter Bewegungsprogramme. Gesundheitswesen 2016, 78, 359–366. [Google Scholar]
- Steenbakkers, M.; Jansen, M.; Maarse, H.; De Vries, N.K. Challenging Health in All Policies, an action research study in Dutch municipalities. Health Policy 2012, 105, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, V.B.; Oesterle, S.; Hawkins, J.D. Relating coalition capacity to the adoption of science-based prevention in communities: Evidence from a randomized trial of Communities That Care. Am. J. Community Psychol. 2015, 55, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Does access to neighbourhood green space promote a healthy duration of sleep? Novel findings from a cross-sectional study of 259 319 Australians. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyment, J.E.; Bell, A.C.; Lucas, A.J. The relationship between school ground design and intensity of physical activity. Child. Geogr. 2009, 7, 261–276. [Google Scholar] [CrossRef]
- Larsen, M.; Pedersen, H.S.; Davies, J.; Gulis, G. Assessing public health intervention practices in a Danish municipality: Applying criteria based on the European Community Health Promotion Indicator Development (EUHPID) model. Scand. J. Public Health 2013, 41, 778–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Urban Green Space and Health: Intervention Impacts and Effectiveness Meeting Report. Bonn, Germany, 20–21 September 2016. Available online: https://tinyurl.com/y74rvwk8 (accessed on 25 March 2020).
- WHO. Age-Friendly World. City of Unley. 2020. Available online: https://extranet.who.int/agefriendlyworld/network/unley/ (accessed on 19 March 2020).
- Pope, J.; Galvin, L.; Anglicare, B.L. Making Bendigo a Child Friendly City: A Set of Indicators of Child and Young People’s Well-Being to Galvanise Action; Department of Planning and Community Development & Bendigo: Melbourne, Australia, 2013. [Google Scholar]
- Bloch, P.; Toft, U.; Reinbach, H.C.; Clausen, L.T.; Mikkelsen, B.E.; Poulsen, K.; Jensen, B.B. Revitalizing the setting approach–supersettings for sustainable impact in community health promotion. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constitution of the World Health Organization; WHO: Geneva, Switzerland, 1946.


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quilling, E.; Babitsch, B.; Dadaczynski, K.; Kruse, S.; Kuchler, M.; Köckler, H.; Leimann, J.; Walter, U.; Plantz, C. Municipal Health Promotion as Part of Urban Health: A Policy Framework for Action. Sustainability 2020, 12, 6685. https://0-doi-org.brum.beds.ac.uk/10.3390/su12166685
Quilling E, Babitsch B, Dadaczynski K, Kruse S, Kuchler M, Köckler H, Leimann J, Walter U, Plantz C. Municipal Health Promotion as Part of Urban Health: A Policy Framework for Action. Sustainability. 2020; 12(16):6685. https://0-doi-org.brum.beds.ac.uk/10.3390/su12166685
Chicago/Turabian StyleQuilling, Eike, Birgit Babitsch, Kevin Dadaczynski, Stefanie Kruse, Maja Kuchler, Heike Köckler, Janna Leimann, Ulla Walter, and Christina Plantz. 2020. "Municipal Health Promotion as Part of Urban Health: A Policy Framework for Action" Sustainability 12, no. 16: 6685. https://0-doi-org.brum.beds.ac.uk/10.3390/su12166685