Prediction of the Number of and Care Costs for Disabled Elderly from 2020 to 2050: A Comparison between Urban and Rural Areas in China


Abstract
:1. Introduction
1.1. LTCI in China and Other Countries
1.2. Previous Research
2. Materials and Methods
2.1. Data Sources
2.1.1. Demographic Data
2.1.2. Disability Rate
2.1.3. Proportion of Different Types of Care
2.1.4. Costs of LTC for Disabled Elderly
2.2. Statistical Analysis
3. Results
3.1. Disability Rate and Its Distribution
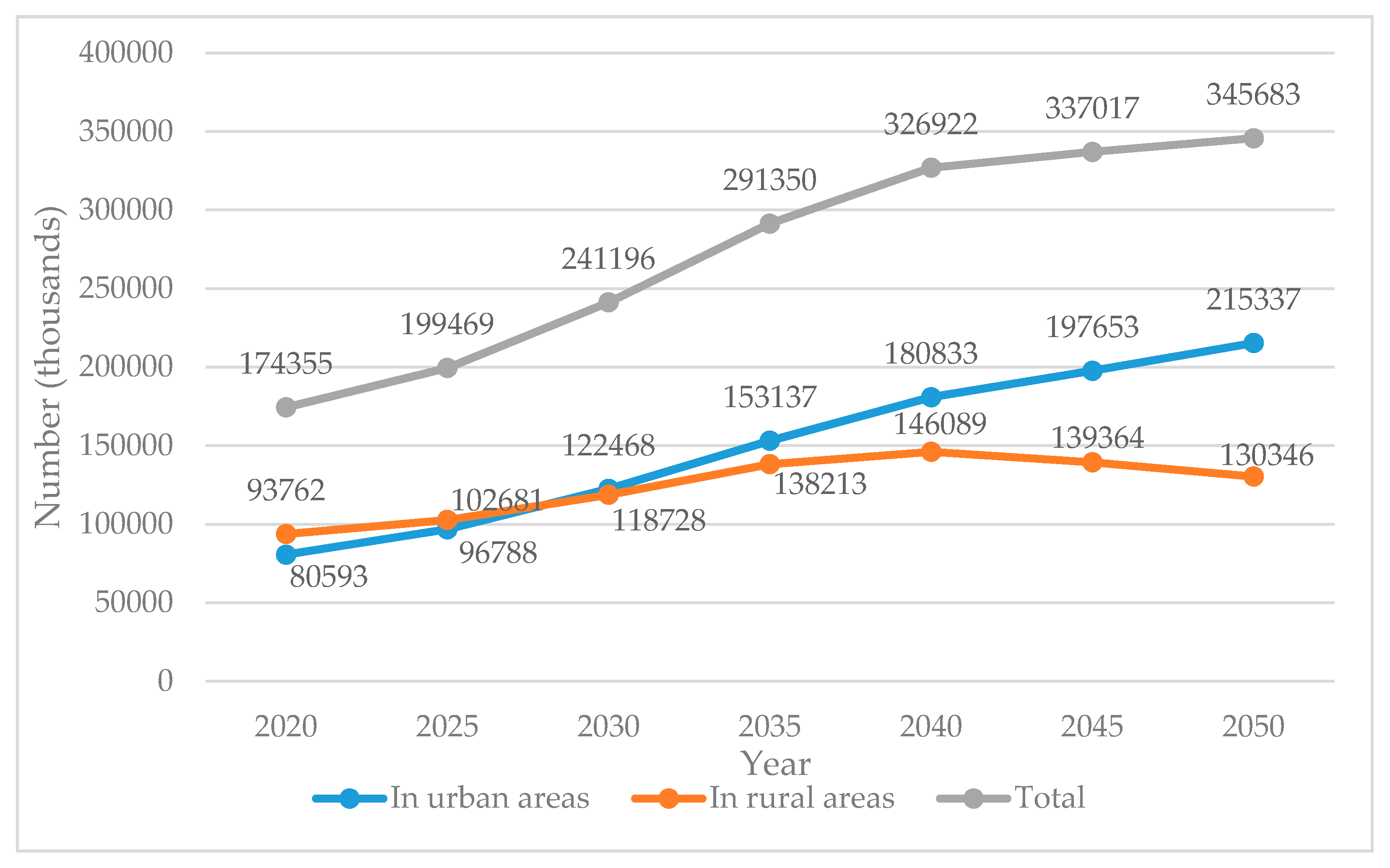
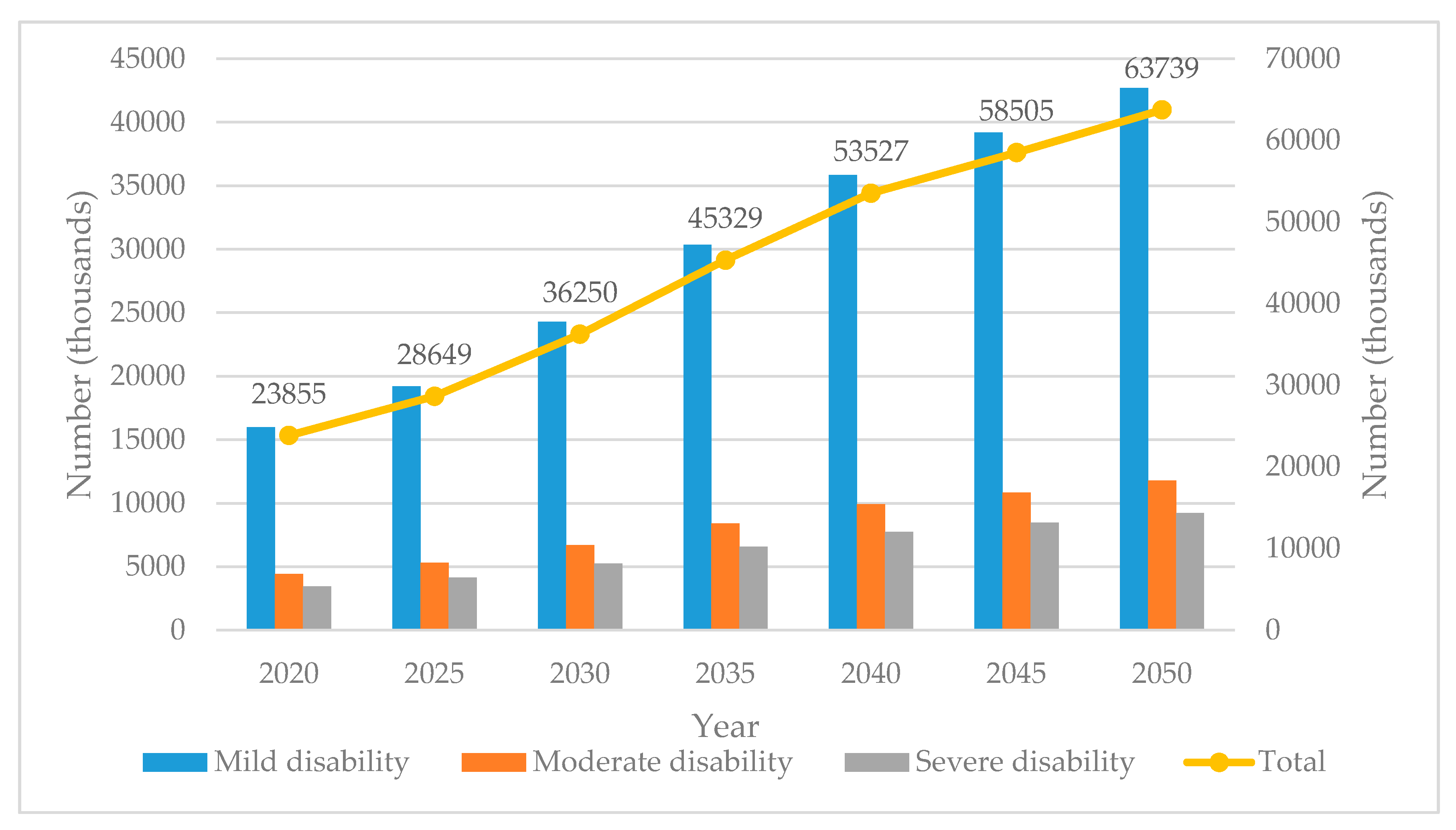
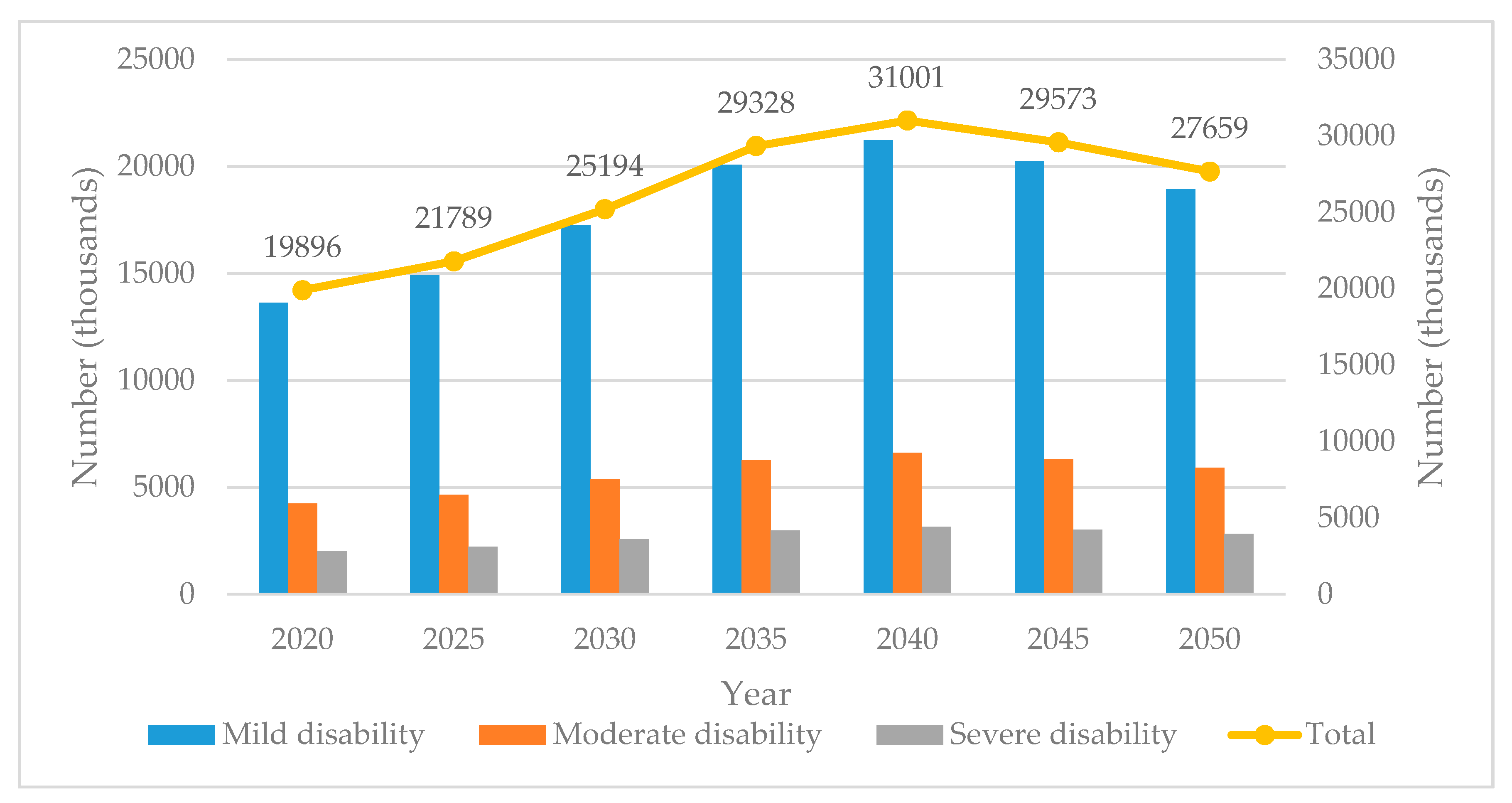
3.2. Prediction of Disabled Population
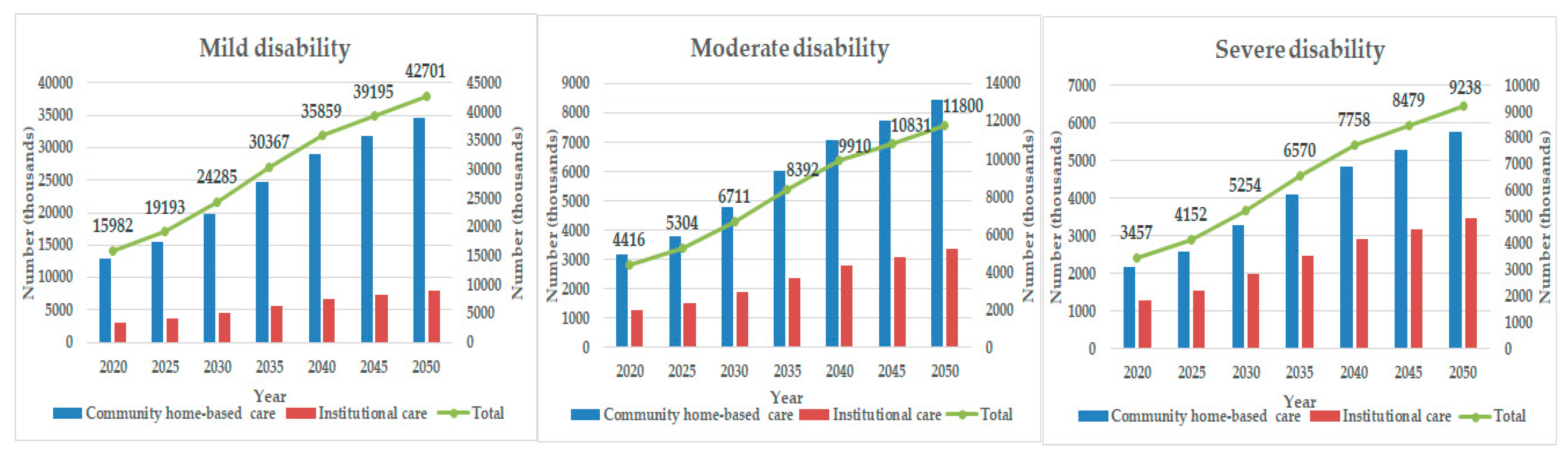
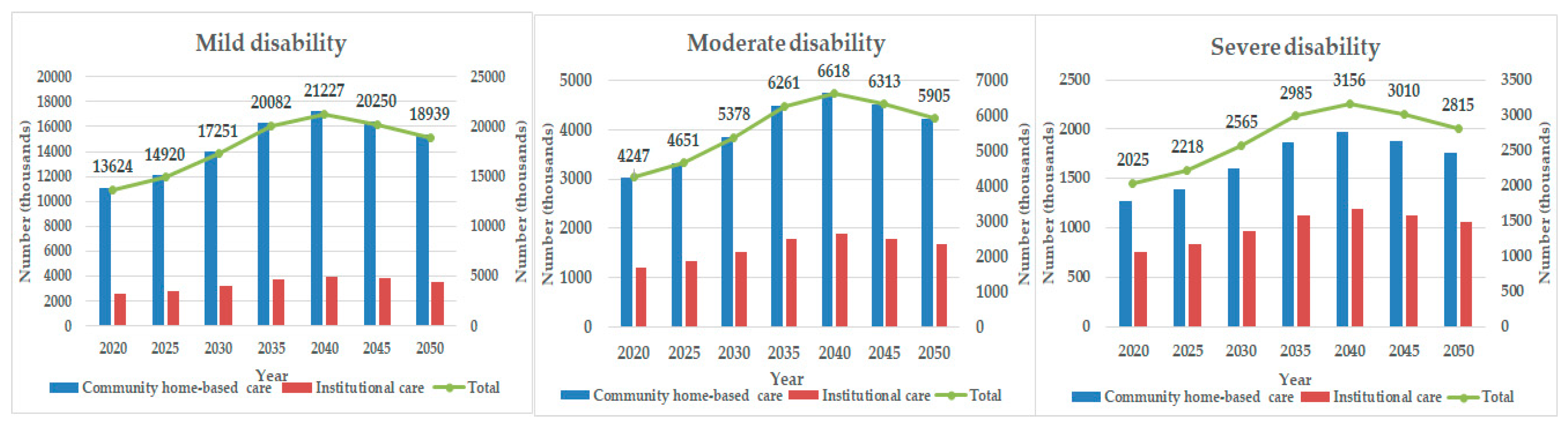
3.3. Demand for Different Care Types in Urban and Rural Areas
3.4. Projection of LTC Costs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. China Country Assessment Report on Ageing and Health; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- National Bureau of Statistics of China. 2019. Available online: http://www.stats.gov.cn/tjsj/zxfb/201902/t20190228_1651265.html (accessed on 1 December 2019).
- Yu, L. How to solve the problem of insufficient supply of more than 4 million registered nurses in China? Available online: http://www.cnr.cn/sxpd/ws/20190512/t20190512_524609391.shtml (accessed on 14 March 2019).
- Robine, J.-M.; Michel, J.-P. Looking forward to a general theory on population aging. J. Gerontol. A Biol. 2004, 59, M590–M597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, Z.; Channon, A.; Van Lerberghe, W. Will There be Enough People to Care? Notes on Workforce Implications of Demographic Change 2005–2050; WHO: Geneva, Switzerland.
- Karlsson, M.; Mayhew, L.; Plumb, R.; Rickayzen, B. Future costs for long-term care: Cost projections for long-term care for older people in the United Kingdom. Health Policy 2006, 75, 187–213. [Google Scholar] [CrossRef] [PubMed]
- Nadash, P.; Doty, P.; von Schwanenflügel, M. The German long-term care insurance program: Evolution and recent developments. Gerontology 2018, 58, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.C.; Ikegami, N.; Gibson, M.J. Lessons from public long-term care insurance in Germany and Japan. Health Aff. 2010, 29, 87–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, X.; Liu, H. Comparison of Long-term Care Insurance System in Japan and Germany and Implications for China. Jpn. Res. 2019, 33, 64–72. [Google Scholar]
- Shimizutani, S. The future of long-term care in Japan. Asia Pac. Rev. 2014, 21, 88–119. [Google Scholar] [CrossRef] [Green Version]
- Rhee, J.C.; Done, N.; Anderson, G.F. Considering long-term care insurance for middle-income countries: Comparing South Korea with Japan and Germany. Health Policy 2015, 119, 1319–1329. [Google Scholar] [CrossRef] [Green Version]
- Seok, J.E. Public long-term care insurance for the elderly in Korea: Design, characteristics, and tasks. Soc. Work. Public. Health 2010, 25, 185–209. [Google Scholar] [CrossRef]
- Kwon, S. Future of long-term care financing for the elderly in Korea. J. Aging Soc. Policy 2008, 20, 119–136. [Google Scholar] [CrossRef]
- Brown, J.R.; Finkelstein, A. The interaction of public and private insurance: Medicaid and the long-term care insurance market. Amer. Econ. Rev. 2008, 98, 1083–1102. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.; Jingwei He, A.; Fang, L.; Mossialos, E. Financing institutional long-term care for the elderly in China: A policy evaluation of new models. Health Policy Plan. 2016, 31, 1391–1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.; Yang, W.; Deguchi, H. Care providers, access to care, and the Long-term Care Nursing Insurance in China: An agent-based simulation. Soc. Sci. Med. 2020, 244, 112667. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.-H.; Wang, S.-S.; Du, S.-H. Regional comparison and implications of China’s long-term care insurance system. Chin. J. Health Policy. 2018, 11, 1–7. [Google Scholar]
- Wang, L. Study on the Current Situation of Pilot Long-Term Care Insurance in Shanghai. Master’s Thesis, Shanghai Normal University, Shanghai, China, March 2019. [Google Scholar]
- Lei, X.; Feng, Y. Financing Channel of Social Long-term Care Insurance: Experience, Difficulties and Future choices. J. Northwest. Univ. 2016, 46, 108–115. [Google Scholar]
- Lu, Y.; Yang, C. A Review of the Construction of Long-term Care Insurance System in China. Soc. Secur. Stud. 2016, 98–105. [Google Scholar]
- Xu, X.; Chen, L. Projection of Long-Term Care Costs in China, 2020–2050: Based on the Bayesian Quantile Regression Method. Sustainability 2019, 11, 3530. [Google Scholar] [CrossRef] [Green Version]
- Moody, H.R. Environmentalism as an aging issue. Public Policy Aging Rep. 2008, 18, 1–7. [Google Scholar] [CrossRef]
- Wark, S. Ageing, end-of-life care, and the National Disability Insurance Scheme: What can we learn from overseas? J. Intellect. Dev. Dis. 2015, 40, 92–98. [Google Scholar] [CrossRef]
- Comas-Herrera, A.; Pickard, L.; Wittenberg, R.; Davies, B.P.; Darton, R. Future Demand for Long-Term Care, 2001 To 2031: Projections of Demand for Long-Term Care for Older People in England; University of Kent: Canterbury, UK, 2003. [Google Scholar]
- Garber, A.M.; MaCurdy, T.E. Predicting nursing home utilization among the high-risk elderly. In Issues in the Economics of Aging; University of Chicago Press: Chicago, IL, USA, 1990; pp. 173–204. [Google Scholar]
- Hare, W.; Alimadad, A.; Dodd, H.; Ferguson, R.; Rutherford, A. A deterministic model of home and community care client counts in British Columbia. Health Care Manage. Sci. 2009, 12, 80. [Google Scholar] [CrossRef]
- Fukawa, T. Household projection and its application to health/long-term care expenditures in Japan using INAHSIM-II. Soc. Sci. Comput. Rev. 2011, 29, 52–66. [Google Scholar] [CrossRef]
- Rong, P. Analysis of Senior Population Nursing Needs Based on Markov Model. Stat. Inf. Forum. 2009, 24, 77–80. [Google Scholar]
- Yu, W.; Liu, B. Elderly care system construction and demand forecast. J. Popul. 2012, 4, 3–13. [Google Scholar]
- Hu, H.; Li, Y.; Zhang, L. Estimation and Prediction of Demand of Chinese Elderly Long-term Care Service. Chin. Popul. Sci. 2015, 79, 89–127. [Google Scholar]
- Huang, F.; Wu, C. A Study of Long-Term-Care Demand of the Elderly in China: Based on Multistatus Transition Model. Econ. Res. J. 2012, 47, 119–130. [Google Scholar]
- Huang, K.; Lu, J. Study on Time Expectancy of Care for Daily Living of Chinese Elderly. Chin. J. Popul. Sci. 2014, 92, 101–128. [Google Scholar]
- Gu, D.-N.; Liu, Y.-Y. A review on latest studies on elderly care needs and costs. J. Northwest. Popul. 2008, 1, 1–6. [Google Scholar]
- Kang, Q.; Cao, X. A Review of Researches on Long-term Care Insurance Funding Theory. China Econ. 2019, 56, 57–61. [Google Scholar]
- Wen, T. A Literature Review on Financing for Long-term Care in China. J. Sichuan. Univ. Sci. 2018, 33, 18–32. [Google Scholar]
- Li, X. Financial Supply and Demand Balance Analysis of Long-Term Care Insurance in Jiangsu. Master’s Thesis, Nanjing University of Finance & Economics, Nanjing, China, November 2015. [Google Scholar]
- Zhang, L.; Zeng, Y.; Fang, Y. The effect of health status and living arrangements on long term care models among older Chinese: A cross-sectional study. PLoS ONE 2017, 12, e0182219. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Ministry of Health and Welfare. Available online: https://www.mohw.gov.tw/mp-1.html (accessed on 14 March 2019).
- Government, S.M. Notice of the Municipal Government on Printing and Distributing the "Measures for Piloting Long-term Care Insurance in Shanghai". Available online: http://www.shanghai.gov.cn/nw2/nw2314/nw2319/nw12344/u26aw54809.html (accessed on 14 March 2019).
- National Bureau of Statistics of China. 2014. Available online: http://www.stats.gov.cn/tjsj/ndsj/2015/indexch.htm (accessed on 14 March 2019).
- Qi, M. Labor Supply and Labor Demand Forecasting in China, 2010-2050. Popul. Res. 2010, 34, 76–87. [Google Scholar]
- Zhu, L. The Monte Carlo Method and Application. Master’s Thesis, Central China Normal University, Wuhan, China, December 2014. [Google Scholar]
- Duan, N.; Xue, H.; Pan, Y. The selection of simulation times when calculating reliability with Monte Carlo method. Coal Mine Mach. 2002, 13–14. [Google Scholar]
- Zhou, F.; Zhang, J. A Summary of Research on Social Insurance and Commercial Insurance Cooperation in Long-term Care Insurance. Soc. Welfare. 2018, 18, 24–31. [Google Scholar]
- Tian, S.; Wang, D.; Song, F.; Li, Y. Governance strategies for the development of rural left-behind elderly human resources in the process of urbanization. Chin. J. Gerontol. 2017, 37, 2848–2850. [Google Scholar]
- Zhang, Y.; Yu, X. Evaluation of Long-Term Care Insurance Policy in Chinese Pilot Cities. Int. J. Environ. Res. Public Health 2019, 16, 3826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zeng, Y.; Fang, Y.; Wen, C. Study on Pension Methods and its Influential Factors among the Elderly by Using Andersen Behavior Model. Chin. J. Health. Stats. 2017, 34, 721–725. [Google Scholar]
- Guo, L. Research on the Development Status and Planning Design of Home-based Elderly Community in China. J. Anhui Agr. Sci. 2015, 43, 327–329. [Google Scholar]
- Li, Y. Calculation and Analysis of the Scale of Long-term Care Funds for Disability Elderly in China. J. Popul. 2018, 40, 78–85. [Google Scholar]
- Zhang, Y. Research on the long term care for disabled elderly in rural areas in the perspective of social support theory. Master’s Thesis, Nanchang University, Nanchang, China, May 2017. [Google Scholar]
- Wang, Q.; Zhou, Y.; Ding, X.; Ying, X. Demand for long-term care insurance in China. Int. J. Environ. Res. Public Health 2018, 15, 6. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Urban (Age Groups) | Rural (Age Groups) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 65–69 | 70–74 | 75–79 | 80–84 | 85+ | 65–69 | 70–74 | 75–79 | 80–84 | 85+ | |
| 2020 | 33,622 | 21,424 | 12,623 | 7975 | 4949 | 37,565 | 25,533 | 15,506 | 9313 | 5845 |
| 2025 | 34,943 | 29,788 | 17,372 | 8777 | 5908 | 32,425 | 32,757 | 20,330 | 10,531 | 6638 |
| 2030 | 47,765 | 31,173 | 24,369 | 12,300 | 6861 | 41,897 | 28,472 | 26,430 | 14,143 | 7786 |
| 2035 | 57,475 | 42,879 | 25,804 | 17,541 | 9438 | 48,407 | 37,222 | 23,265 | 18,775 | 10,544 |
| 2040 | 60,338 | 51,907 | 35,885 | 18,915 | 13,788 | 40,266 | 43,360 | 30,933 | 16,868 | 14,662 |
| 2045 | 55,435 | 54,833 | 43,876 | 26,778 | 16,731 | 28,043 | 36,293 | 36,446 | 22,975 | 15,607 |
| 2050 | 61,266 | 50,756 | 46,842 | 33,297 | 23,176 | 26,434 | 25,443 | 30,807 | 27,533 | 20,129 |
| Age Groups | Mild (%) | Moderate (%) | Severe (%) | Total (%) |
|---|---|---|---|---|
| 65–69 | 2.00 | 0.74 | 0.32 | 3.06 |
| 70–74 | 3.54 | 0.88 | 0.44 | 4.86 |
| 75–79 | 5.28 | 0.67 | 0.92 | 6.87 |
| 80–84 | 6.88 | 2.04 | 1.02 | 9.94 |
| 85+ | 19.33 | 5.60 | 3.50 | 28.43 |
| Weighted mean | 16.74 | 4.94 | 3.05 | 17.87 |
| Age Groups | Urban | Rural | ||||
|---|---|---|---|---|---|---|
| Mild n (%) | Moderate n (%) | Severe n (%) | Mild n (%) | Moderate n (%) | Severe n (%) | |
| 65–69 | 7(12.96) | 1(1.85) | 1(1.85) | 1(0.58) | 1(0.58) | 0(0.00) |
| 70–74 | 9(1.94) | 3(0.65) | 2(0.43) | 10(2.05) | 4(0.82) | 1(0.21) |
| 75–79 | 43(7.21) | 4(0.67) | 9(1.51) | 20(3.35) | 4(0.67) | 2(0.34) |
| 80–84 | 42(8.38) | 11(2.20) | 9(1.80) | 32(5.57) | 11(1.91) | 2(0.35) |
| 85+ | 365(23.20) | 98(6.23) | 79(5.02) | 343(16.42) | 107(5.12) | 49(2.35) |
| Weighted mean | 19.83% | 5.48% | 4.29% | 14.53% | 4.53% | 2.16% |
| Year | Urban | Rural | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | Total | Mild | Moderate | Severe | Total | ||
| 2020 | 15,982 | 4416 | 3457 | 23,855 | 13,624 | 4247 | 2025 | 19,896 | 43,751 |
| 2025 | 19,193 | 5304 | 4152 | 28,649 | 14,920 | 4651 | 2218 | 21,789 | 50,438 |
| 2030 | 24,285 | 6711 | 5254 | 36,250 | 17,251 | 5378 | 2565 | 25,194 | 61,444 |
| 2035 | 30,367 | 8392 | 6570 | 45,329 | 20,082 | 6261 | 2985 | 29,328 | 74,657 |
| 2040 | 35,859 | 9910 | 7758 | 53,527 | 21,227 | 6618 | 3156 | 31,001 | 84,528 |
| 2045 | 39,195 | 10,831 | 8479 | 58,505 | 20,250 | 6313 | 3010 | 29,573 | 88,078 |
| 2050 | 42,701 | 11,800 | 9238 | 63,739 | 18,939 | 5905 | 2815 | 27,659 | 91,398 |
| Community Home-Based Care | Institutional Care | |||
|---|---|---|---|---|
| Urban | Rural | Urban | Rural | |
| Mild disability | 1010.16 | 324 | 919.02 | 294.77 |
| Moderate disability | 1515.24 | 486 | 3595.66 | 1153.28 |
| Severe disability | 2020.32 | 648 | 4515.64 | 1448.35 |
| Year | Care Costs (100 Million yuan) | Per Capita Costs (yuan) | ||||
|---|---|---|---|---|---|---|
| Urban | Rural | Total | Urban | Rural | Total | |
| 2020 | 4277 | 1103 | 5380 | 17,931 | 5545 | 11,738 |
| 2025 | 7706 | 1812 | 9518 | 26,896 | 8317 | 17,607 |
| 2030 | 12,987 | 3493 | 16,480 | 35,827 | 13,863 | 24,845 |
| 2035 | 24,335 | 6505 | 30,840 | 53,686 | 22,180 | 37,933 |
| 2040 | 38,315 | 10,314 | 48,629 | 71,581 | 33,270 | 52,426 |
| 2045 | 52,348 | 13,119 | 65,467 | 89,476 | 44,360 | 66,918 |
| 2050 | 68,437 | 16,871 | 85,308 | 107,371 | 60,996 | 84,184 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Fu, S.; Fang, Y. Prediction of the Number of and Care Costs for Disabled Elderly from 2020 to 2050: A Comparison between Urban and Rural Areas in China. Sustainability 2020, 12, 2598. https://0-doi-org.brum.beds.ac.uk/10.3390/su12072598
Zhang L, Fu S, Fang Y. Prediction of the Number of and Care Costs for Disabled Elderly from 2020 to 2050: A Comparison between Urban and Rural Areas in China. Sustainability. 2020; 12(7):2598. https://0-doi-org.brum.beds.ac.uk/10.3390/su12072598
Chicago/Turabian StyleZhang, Liangwen, Sijia Fu, and Ya Fang. 2020. "Prediction of the Number of and Care Costs for Disabled Elderly from 2020 to 2050: A Comparison between Urban and Rural Areas in China" Sustainability 12, no. 7: 2598. https://0-doi-org.brum.beds.ac.uk/10.3390/su12072598