
Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea


1
College of Hospitality and Tourism Management, Kyung Hee University, Seoul 02453, Korea
2
Public Healthcare Center & Department of Psychiatry, Seoul National University Hospital, Seoul 03080, Korea
*
Author to whom correspondence should be addressed.
Sustainability 2021, 13(14), 8106; https://0-doi-org.brum.beds.ac.uk/10.3390/su13148106
Submission received: 3 June 2021
/
Revised: 12 July 2021
/
Accepted: 15 July 2021
/
Published: 20 July 2021
(This article belongs to the Special Issue Business and Management Aspects of Sustainability on Media and Creative Industries)
Abstract
:Historically, the introduction of a new media in mass market caused a strong conflict starting from the nineteenth century popular literature, comics, rock music and film. Interestingly, these conflicts have shown similar and repeated patterns, which is now called media panic and moral regulation, and games are following this pattern. In 2019, Gaming disorder (GD) was decided to be included in the International Classification of Diseases (ICD-11), and similar conflicts on games arenow expected. However, the social cost and damage have not been fully addressed until now. Thus, this study focuses on the estimation of the social cost induced by GD for policy design and decisions in the public healthcare of South Korea. Using the contingent valuation method, a popular valuation method in econometrics for non-market goods, this study has tried to estimate the social cost induced by the introduction of GD into the public healthcare practice. Focusing on a false positive problem in the diagnosis, this study estimates that the willingness to pay for GD diagnosis for children is about KRW 152 K (USD 135). Considering the difference between the prevalence of GD (1.9%) and GD suspicion rate of children in the respondents (12.54%), the excessive medical diagnosis cost due to the false positive problem is estimated to KRW 101 billion (USD 89.6 M), which is about four times more than the annual medical cost for Attention Deficit Hyperactivity Disorder (ADHD) treatment in South Korea. Thus, strong scientific proof and a cautious policy approach on GD are needed before the inclusion of GD in the public health practice.
1. Introduction
The introduction of new media has brought a new value in the society, but it also has caused conflict and resistance from society [1]. The lively delivery power of film has brought about serious concerns that children and adolescents could be exposed to the violence or sexual stimuli of the film, which can cause a destruction of ethics in society [2]. The unlimited imagination in comics has been regarded as a serious risk factor for children who cannot tell the difference between reality and fantasy [3,4,5]. Interestingly, there is consistency in the reaction to these new media, and the result of the reaction is similar. The history repeatedly shows that the concern about new media has created regulations without enough scientific evidence and have caused a conflict between new media and society [1,3].
Further scientific studies on these regulations have found that most of the concerns about new media were actually non-existent or minimal and, in most cases, these negative effects were offset by the positive effects [6]. However, fears about the new media have been repeatedly shown, and this phenomenon, media panic or moral regulation, has been putting a heavy burden on creative industries and society. It has threatened the sustainability of the creative industry and innovation [7].
One of the representative cases of media panic is gaming disorder (GD). As the gaming industry has grown rapidly, concerns about the negative effects on games to children have emerged [8]. Based on the theoretical model of traditional media and aggression, scholars tried to prove the relationship between gameplay and the aggression of adolescents [9]. Fears that games can cause a serious problem in children’s health, relationships with families, and achievements in school have been also widespread in recent years [10,11]. However, the scientific evidence of these concerns is not quite clear. There are more than several hundred of studies on the negative effects of games, but in most cases, there are some faults on the sampling in the experiment or the scientific soundness of the analytical process to expand their experimental findings as a proof of the negative effect of games on humanbeing [12,13]. Recent longitudinal studies also proved that the exposure to violent games can change the psychological status of subjects in the short-term or experimental settings, but there is no negative effect of violent games in the long-term [14,15].
However, growing concerns about games is now pushing society to recognize the excessive game usage as a new kind of psychiatric disease. In 2019, gaming disorder (GD), a pattern of persistent and recurrent gaming behavior, was formalized as a disease in a new category for psychiatry in the 11th revision of the International Classification of Diseases (ICD-11). Based on this inclusion, the Korean government officials declared that GD will be included in the Korean Standard Classification of Disease in 2025, when it is revised. Due to the fierce opposition both from the gaming industry and from scientists from various fields, the announcement was officially retracted, but the discussion is still progressing [16].
There are still numerous debates on whether it is appropriate to recognize GD as a psychiatric disease [17,18,19,20]. Even scholars who strongly support the inclusion of GD in ICD-11 agree that there could be a serious false positive problem in the diagnosis of GD, which can cause overmedication [21]. Although there is a consensus on the false positive problem in GD, the estimation of its social cost is not yet fully investigated. To make proper policy decisions on this public issue, the estimation of the social cost due to the policy is essential, but it is often neglected in the public healthcare issue due to the difficulty of the estimation. Considering the conflict of the inclusion of GD and the relative importance of GD as an issue in the public healthcare of South Korea, this study focuses on the estimation of the social cost induced by GD in the future for the basis of the policy design.
Using the contingent valuation method (CVM) from environmental economics, this study has tried to measure the willingness to pay (WTP) for GD diagnosis tests under the hypothetical scenario, and estimated the social cost induced by the false positive problem in GD as a form of excessive medical cost. Based on the survey of 1012 respondents in South Korea, we have found that about 12.5% of respondents suspect that one of their family members has GD, and this is far more than the prevalence of GD from the previous studies (1.94%) [22]. Through the hypothetical scenario analysis, we have estimated that the average WTP for GD diagnosis test is approximately KRW 152 K (USD 135), and the excessive medical cost due to GD diagnosis for children and adolescent is KRW 101 billion (USD 89.6 million), which is four times more than the annual direct medical cost of ADHD in South Korea. The next section briefly reviews the background and relevant literature on this issue. The subsequent sections describe CVM, estimation method and data. Estimation of WTP and social cost is discussed in the result section. Implications and limitation of the study are suggested in the discussion section.
2. Background and Literature Review
2.1. Concerns on Games and Media Panic
Following the fast growth of the game industry through new technologies, concerns about games have also increased, especially among children and adolescents, and concerns about gaming are now creating some level of conflict in society and academia [6,7]. One of the prominent cases in this conflict is the study on the relationship between games and aggression. Based on the general aggression model (GAM), lots of studies were conducted to prove the relationship between games and violence [13]. Originally, GAM was developed to analyze the relationship between aggressive attitude and video media such as TV and film [23]. The theory assumes that external stimuli such as violent video content can change the psychological state of a person, and this change can be expressed as a behavior [9]. This theory explains that the exposure to violent games can cause aggressive behavior in society [24,25]. Using this theoretical background, more than hundreds of experimental studies in psychology and psychiatry have reported the positive relationship between violent games and aggressive behavior [26]. Based on these findings, several countries are putting regulations on games to minimize the risk for children and adolescents [11].
However, further studies and meta-analyses on this issue have found contradictory results, and they have also expressed a serious concern about the validity of the previous studies [13]. Serious faults in the sampling, experiment design, or analytical process in the previous studies have been reported through meta-analyses [12,13]. Although some studies have shown the meaningful positive relationship between games and aggression in the short-term experiments [26], recent longitudinal studies under the acute scientific process have found that there is no long-term relationship between games and aggression [14,15]. In addition, there was no scientific proof that the experimental finding of the relationship between the games and aggressive behavior can cause an actual crime or violence in society. Rather, the opposite result has been reported through empirical studies [27,28,29,30]. Thus, there is still a controversy about the relationship between games and aggression.
Experimental studies also insisted that games have negative effects on the health, quality of life, anxiety disorders, and depression for children and adolescents [8,10], and based on these findings, several countries, mainly Asian countries, have introduced the restrictions on game usage for children and adolescents [11]. The policy evaluation result of the game usage restriction in South Korea shows that the restrictions have decreased the game usage of problematic gamers and have increased the sleeping time for children [31]. However, the average increase of sleeping time was 1.5 minutes per day, and this difference has faded four years after the introduction of the restriction [32]. Thus, the relationship between games and sleep disorders or general health cannot be concluded in the scientific perspective.
Scholars in sociology have pointed out that the dispute on games has similar patterns to previous disputes on other new media in history. Starting from popular literature in the nineteenth century, rock music, comics, TV, and film have experienced similar disputes about the negative effects of new media on children [2,4,5,6,7,33,34], and these disputes have surprisingly similar patterns [1,3]: (1) new media emerges based on a new technology or new application and becomes popular; (2) content, which describes criminal, violent, or sexual activities, is found in the new media; (3) the new media is identified as a danger to children who cannot tell the difference between reality and fantasy, and scholars support this identification based on scientific tools; (4) government regulation or legal restriction is placed on the media.
This pattern is known as media panic or moral regulation by sociologists [3], and it can be defined as a practice for some social agents to problematize the conduct, value, and culture of others based on morals and to seek the imposing regulation on them [35,36]. In this perspective, sociologists in new media have been criticizing the dispute on the negative effect of games [3,6], and they have been insisting that both the positive effect and negative effect of new media should be considered as a whole [7].
2.2. Gaming Disorder
Despite the controversy on the dispute of games, scholars in psychiatry have developed the idea of GD. In 2013, American Psychiatric Association added the internet gaming disorder (IGD) as a disease in the Diagnostic and Statistical Manual 5 (DSM-5) under the conditions for further study [37,38]. World Health Organization (WHO) also started the discussion on GD starting from 2014 and decided to register the GD as a disease in the International Classification of Disease 11 (ICD-11) in 2019 [39]. Following the decision of WHO, the listing of GD as a formal disease in South Korea is expected in 2025 when the regular revision of the Korean Classification of Disease (KCD) occurs, but the government has announced that the decision is not fully made due to the fierce opposition both from the industry and scientists [16].
Scholars who are supporting GD insist that the formalizing of GD as a disease will help the development, accessibility, and reimbursement of the treatment for it despite that the candidate of GD is limited to few people [18,19,20,40]. On the contrary, scholars who are opposing it argue that it is too early for the listing GD as a formal disease when there is no acceptable diagnostic standard for it. Although there are some diagnostic standards, most of them are based on gambling or substance abuse, and these diagnostic results are infamous for their inaccuracy [17,41,42,43].
However, both the supporters and objectors have agreed that there is a high probability of a false positive problem in the diagnostics of GD, and they are expressing concern about it [17,21,44,45]. Considering the increased accessibility and popularity of child and adolescent mental health services in Korea, the concern on the false positive problem should be measured precisely. Thus, a high level of social cost due to the false positive problem is expected when GD is introduced in the practice without enough consideration [21], but there is no study on the measurement of social cost due to GD until now.
2.3. Contingent Valuation Model
The contingent valuation method (CVM) is a valuation method for non-market goods using a stated preference choice. It was first suggested by Ciriacy-Wantrup based on the idea that the value of non-market goods can be inferred through a direct investigation of the WTP of individual economic entities [46]. CVM establishes a hypothetical scenario in which an individual should decide on a phenomenon that has not yet occurred, and this can allow CVM to directly estimate the quantitative value or cost by conducting a questionnaire on the degree of WTP for these changes. In addition, CVM has a powerful advantage in that it can derive non-use value through the survey and hypothetical scenario. [47,48].
The validity of CVM became a critical issue when it was used to estimate the non-use value from the pollution of the 1989 Exxon Valdez oil spill in Alaska. The government and academia have organized US National Oceanographic and Atmospheric Administration (NOAA) panel with Nobel-prize-winning experts to carefully examine CVM. After the verification and modification by NOAA, CVM has been established as a strong and valid economic evaluation methodology [48,49]. CVM has been primarily used in the environment area, but in recent years, it has been used in various fields such as energy [50,51,52], tourism ([53,54,55], and cultural industries [56,57].
CVM was also applied in the medical and healthcare fields to estimate WTP for medical service in the areas of medical technology [58], health policy [59,60], public health service [61,62], cancer prevention [63], insurance [64], and vaccines [65]. However, CVM has not yet been applied for cost estimation related to false positive problems. Even in psychiatry, where the seriousness of the false positive problem and its damage has been widely recognized [44,45], the social cost induced by the false positive problem has not been analyzed in quantitative manner except for some anecdotal analysis [44,45]. Thus, this study focuses on the estimation of social cost due to the inclusion of GD in the public healthcare system through the quantitative perspective and suggests CVM as one of the measurement methods for the social cost in the public healthcare policy.
3. Materials and Method
3.1. Analysis Method: DBDC Model
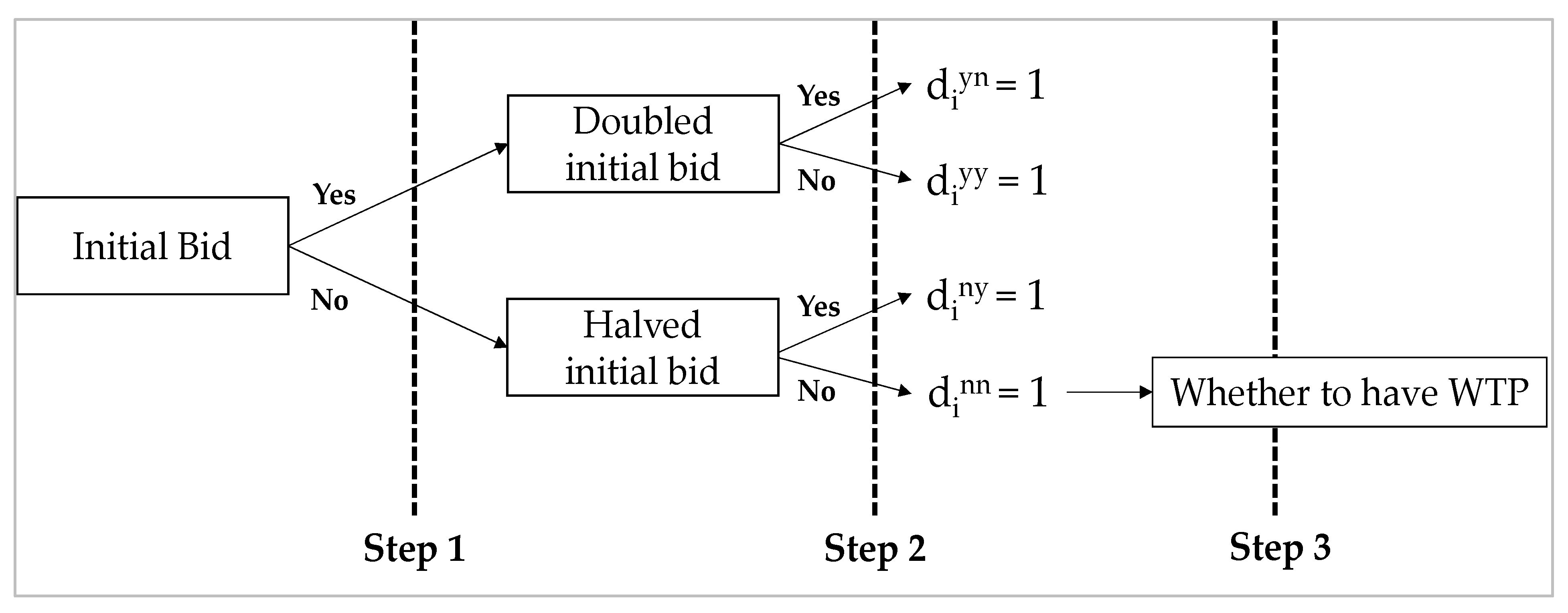
To estimate the WTP for the targeted non-market goods, CVM usually uses closed-ended questionnaires which ask respondents a dichotomous choice (DC) for the given mount or bid [49]. The DC format is highly recommended by NOAA for its convenience, low starting point bias, and reliability compared to open-ended questionnaires [66]. In this study, we use a double-bounded dichotomous choice (DBDC) method in the questionnaire. As shown in Figure 1, DBDC is usually structured in three steps. At the first step, DBDC asks the respondents WTP for the initial bid. If the respondent answers “Yes”, DBDC doubles the initial bid, and asks WTP for the higher bid. If the respondent answers “No”, DBDC halves the initial bid and asks WTP for the lower bid. If the respondent answers “No” to the lower bid, we ask whether the respondent has the intention to pay more than zero. If the respondent has no intention to pay, we treat the WTP of the respondent as a zero. Because DBDC uses multiple questions for WTP, it can derive more information from the respondents, and it is known to be more efficient than the single-bounded dichotomous choice model [67,68,69].
In the DBDC form, WTP can be described as a linear function, as shown in Equation (1):
In the Equation (1), zi is a vector of explanatory variables, is a vector of parameters, and ui is an error term which follows . For , the respondent answers “yes” for the first bid and answers “no” for the second bid , the probability of the case can be described such as in (2) where WTP follows the linear form (1), and is the standard cumulative normal:
Based on the probability for each case, we can construct a likelihood function (3), and we can obtain and for WTP through the maximum likelihood estimation:
In Equation (3), , , , and are indicator variables which have a value of 1 for (yes, no), (yes, yes), (no, yes), and (no, no) respectively, and a value of 0 for other cases.
3.2. Questionnaire Design and Procedure
The questionnaire for the study consisted of three sections. The first section provided the basic information of GD and asked the perception on GD and games in general. The second section was designed to ask the WTP for GD diagnosis test based on the hypothetical scenario. The final section asked for the demographic information of respondents such as gender, age, income, and education level.
For the survey, we developed the following hypothetical scenario. In the scenario, we provided the target of GD as one of the family members, not the respondent oneself to minimize the bias because there is a tendency to reserve or avoid the treatment for psychiatric diseases in South Korea.
This is a hypothetical scenario. Currently, one of your family members, your spouse or children, is strongly suspected as gaming disorder due to the excessive game usage, and you are highly concerned about his or her physical and mental health because of it. To solve the issue, a doctor suggests the treatment for gaming disorder. However, before the treatment, diagnosis tests should be performed to check the necessity for the treatment. After the diagnosis, your family member can get the treatment and public insurance can be applied to the cost of the treatment.
After the explanation of the scenario, the survey suggested the diagnosis test price, and asked whether the respondent can accept the price. The diagnosis price in the questionnaires was developed based on ADHD, which has a similar diagnosis procedure in the clinic practice. At first, we collected the actual ADHD and GD diagnosis price in the major psychiatric hospitals in South Korea. Experts in psychiatry have reviewed the validity of the diagnosis prices that we collected. Finally, we decided on six types of price suggestions, which is in the range of 10%~90% from the price assessment. This suggested price is listed in Table 1. The six types of initial bid were randomly distributed to the respondents.
To investigate factors affecting WTP, the questionnaire included several questions related to GD and games in general. For GD issues, we asked the respondents about their attitude and prior knowledge about GD. For games in general, we asked the respondents their interest using enjoyment and flow construct. Seven items for the interest on games were obtained from Teng [70,71]. Although we tried to use the different constructs of enjoyment and flow, the factor analysis showed that respondents did not separate the two concepts. Thus, we used all the seven items as the respondent’s interest for games. The average game playtime per day was also asked and used in the analysis.
3.3. Participants
The social cost, which can be created by the false positive problem from the inclusion of GD in the national disease categories, is not bounded in specific areas. In addition, the decision to pay for the diagnosis is limited to adults. Thus, we used stratified sampling to draw the social cost from the national perspective and targeted adults over 20. To reflect the national characteristics of the South Korean population, we used the stratified sampling process on the online panel of an online marketing research company in South Korea. Using the geographical information of age groups, gender, and occupation, we divided the online panel into several groups, and set the quota for each group to depict the national characteristics of South Korea. After that, we have randomly recruited the participants from each group for the analysis. The survey was conducted from December 1 2019 to December 20 2019. After excluding the incomplete answers, a total of 1021 questionnaires were collected from the participants.
4. Results
4.1. Demographic Profile of the Participants
Respondents’ demographic characteristics are summarized in Table 2. In total, 50.15% of the respondents are male, and 49.85% are female. Moreover, 64.05% of the respondents were married, and most respondents’ monthly income was in the range of KRW 3 million~4 million (about USD 2600 ~ USD 3500), followed by KRW 4 million ~ 5 million (about USD 3500 ~ USD 4400). Considering the mediam monthly income level of 2018 in South Korea was KRW 4.11 million, the income distribution of the sample showed that the sample reflects the national characteristics well, as planned. Most respondents had a university degree (495; 48.48%), followed by a high school diploma (216; 21.16%), and graduate school (168; 16.45%).
4.2. WTP Estimation Results
Table 3 describes the response distribution of the bid. At the lowest bid, KRW 100,000 (USD 44) for the diagnosis, 53.8% of respondents in the same bid answered “yes” in the first step. The acceptance ratio shows a decreasing pattern as the initial bid increases, as expected. At the highest bid, KRW 300,000 (USD 265), 27.64% of respondents answered “Yes” in the first step. Moreover, 442 respondents rejected both the initial bid and the second bid. Among them, 153 respondents said that they had no intention to pay for the diagnosis. Thus, we excluded these responses from the analysis and treated their WTP as 0.
We use two models to estimate WTP for GD diagnosis. The first model, model 1, only includes the basic bid information, and demographic and other explanatory variables are not included. Model 2 includes all the explanatory variables and induces the marginal effect on WTP through the analysis. The maximum likelihood estimation is calculated using STATA 15 and DOUBLELEB module by Lopez [72].
Model 1 result in Table 4 shows that the estimated WTP for GD diagnosis is about KRW 179 K (USD 159). This result is not considered the zero bid respondents. Using a conservative perspective, we treated all the respondents who refused to answer as zero bidders followed by Haab & McConnell [48]. Under a conservative approach on the zero bidders, the WTP for GD diagnosis is reduced to KRW 152 (USD 135).
Through model 2, we have investigated which factors affect WTP for GD diagnosis. Before the analysis, we checked the reliability and validity test for attitude and interest, the construct with multiple items. We asked four items for attitude and excluded one item due to the reliability. The Cronbach’s alpha for attitude based on three items is 0.6314, and this exceeds the reliability standard. The C.R. (0.7849 > 0.7) and AVE (0.5574 > 0.5) of attitude also exceeded the reliability and validity standard. Similar to attitude, the Cronbach’s alpha (0.9386), C.R. (0.9290), and AVE (0.6880) of interest also exceeded the reliability and validity standard.
The estimation result of Model 2 is shown in Table 4. For the demographic variables, age and income level are statistically significant, but gender, education level, and status of marriage are not significant at a 5% level. In addition, the attitude on GD, agreement level of GD introduction, and interest in games are not significant. A suspicion that the respondent’s child has GD is statistically significant, but the respondent with this suspicion tends to pay less. This result seems to be based on the strategic bias for respondents not to show their true WTP for their profit [48]. To sustain the conservative perspective on the evaluation, we did not correct this bias, but there is a possibility that the true WTP for GD diagnosis is greater than our estimation.
4.3. Evaluation of Social Cost
There can be various social costs induced by the formal inclusion of GD in the disease categories, but this study only focuses on the excessive medical cost due to GD diagnosis. To review the false positive problem, we first checked the difference between the estimated prevalence of GD and the GD suspicion rate of children by their parents. The prevalence of GD range from 0.7% to 15.9% based on the previous studies [73], and 1.96% is estimated as the global prevalence of GD through the meta-analysis in [22]. This is less than the prevalence of ADHD (5.9% ~ 8.5%) in South Korea [74,75]. From the survey, 17.9% of respondents answered that one of their family members is under suspicion of having GD, and 12.54% of respondents suspect that their children have GD. Thus, the difference between the GD suspicion rate of children (12.54%) and the prevalence of GD (1.96%) is the possible target for the excessive medical cost due to the false positive diagnosis.
Most concerns about GD have focused on children and adolescents in previous studies [11,19]. Thus, our study assumes that the false positive problem will mainly occur to parents with children from 5 to 19 years old. Due to the radical changes in the population of South Korea, we use the estimated population from 5 to 19 years old in 2025 when GD is planned to be introduced in South Korea. The estimation of the population from 5 to 19 years old is conducted by the South Korean government [76], and the estimated population of the target range in 2025 is about 6,274,864.
The excessive medical cost due to GD is estimated based on the logic below:
WTP (152,493 KRW/person) × population (6274 K) × false positive rate (10.54%).
The estimation of the excessive medical cost due to false positive diagnosis is about KRW 101 billion (USD 89.6 million). Considering that the annual direct medical costs due to ADHD is about USD 25.5 million in 2012 [77], this is a quite large number just for the false positive medical diagnosis.
5. Discussions and Conclusions
This study has tried to investigate the social effect of the media panic and moral regulation due to GD, which is controversial both in the media industry and in psychiatry. A CVM using a hypothetical scenario has estimated that the excessive medical cost due to the false positive problem in GD will cost more than KRW 101 billion (USD 89.6 million) just for the diagnosis, and this is four times more than the annual medical cost for ADHD treatment in South Korea.
Although the WHO decided to include GD in the ICD-11, there is still controversy on the diagnosis among psychiatrists. For example, the DSM-5 by the American Psychiatric Association categorized internet gaming disorder in a proposed category for further study, which means that the diagnostic standard is still under research and needs more empirical findings and studies for the diagnosis and treatment [21]. On the contrary, GD in the ICD-11 is more focused on “behavioral addiction” than “dependence”, and the WHO has tried to suggest a clear diagnostic standard and symptomology for GD. However, there is still an ongoing debate about the necessity of including GD in ICD, and a consensus of diagnostic criteria has not yet been reached. Our results show that the social cost of the false positive problem regarding GD can be larger than the actual cost when GD is introduced in the public health practice without solid scientific proof and consensus. Thus, policymakers should be cautious on the introduction of GD into clinical practice.
As mentioned already, the introduction of GD follows a typical media panic and moral regulation process. First, some scholars separate the negative effects from games and identify them as a serious risk for children using scientific methods and regulations that follow under the moral standards of specific opinion groups. Considering the controversy of GD in psychiatry and various academic fields, the formal introduction of GD in the public health service can be a serious risk in the sustainable growth of the creative industry. For more than 200 years, popular literatures, comics, music, films, and TV have suffered heavily from media panic and moral regulations. The victims of the media panic were not limited to the creative industries. Many communities outside the norm in that era also had suffered a lot along the process. However, these sufferings and damages were not quantitatively measured until now. Using the contingent valuation method, this study has partially measured the social cost induced by the media panic about games and found that the media panic creates a substantial but unnecessary cost on society. Not only from the public health perspective, but GD should be approached also from the media policy and public welfare perspective.
In the theoretical perspective of the public health policy, this study has tried to suggest a measurement method of social cost through CVM. Starting from the environment economics, CVM is now widely used in the policy-making process to measure the effectiveness of the policy and the possible negative or positive outcome of the policy options [47,48,58]. However, policy analysis in a quantitative manner is not frequently used in the public healthcare policies of psychiatry. Based on the previous studies on the measurement of social cost in psychiatry [74,77], this study has suggested the DBDC model of CVM as a measurement tool for social cost due to the policy changes based on the theories in economics.
6. Limitation of the Study
Although we tried to follow the basic principles of CVM suggested by Arrows et al. (1993) [49], there are still some limitations in this study. First, we tried to measure the social cost induced by GD, but we only have measured the excessive medical cost due to the false positive diagnosis. Indirect cost, social insurance cost, and medical cost due to the wrong diagnosis is not considered in this study. From the public policy perspective, all the social costs induced by the policy changes should be considered. Because the inclusion of GD in the public healthcare category is controversial, this study has taken a conservative perspective in the measurement design.
Secondly, this study did not fully adjust the bias in the estimation process. Due to the data acquisition process using surveys, the CVM is exposed to various biases by nature. In the estimation, we found a possible strategic bias, but we did not adjust it to sustain the conservative perspective. Future studies should be designed to control the strategic bias, which can be easily found in the measurement of the willingness to pay for the specific policy. Thirdly, this study assumed that medical cost follows the market price. However, the price for the treatment and diagnosis have not been decided by the market. It has been determined by the governmental regulation, although it is influenced by various stakeholders. Thus, the social cost in this study should be considered as an estimation, not a direct measurement. Lastly, this study was performed based on the medical environment of South Korea. Considering the unique characteristics of the South Korean medical system such as low personal expenses and public insurance, there are some limitations in the generalization of our findings.
Author Contributions
Methodology design, C.Y.; Data management and analysis, C.Y. and Y.K.; project administration, J.H.S.; validation, J.H.S.; writing—original draft, C.Y., Y.K., and J.H.S.; writing—review and editing, C.Y. and J.H.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Korea Creative Content Agency (KOCCA) funded by the Ministry of Culture, Sports and Tourism (KOCCA 19-15, A predictive investigation of the social effects of the inclusion of gaming disorder to ICD-11).
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to the insignificant risk of online survey and public purpose for the government.
Data Availability Statement
Raw data were generated at KOCCA. The data will be made available on request from KOCCA.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Drotner, K. Dangerous media? Panic discourses and dilemmas of modernity. Paedagog. Hist. 1999, 35, 593–619. [Google Scholar] [CrossRef]
- Critcher, C. Screen savers. Case histories of social reaction to mass media, children and violence. Rech. et Anthropol. 2012, 43, 59–78. [Google Scholar] [CrossRef]
- Critcher, C. Making waves: Historical aspects of public debates about children and mass media. In The International Handbook of Children, Media and Culture; Sage: London, UK, 2008; pp. 91–104. [Google Scholar]
- Barker, M. A Haunt of Fears: The Strange History of the British Horror Comics Campaign; University Press of Mississippi: Jackson, MS, USA, 1984. [Google Scholar]
- Jensen, H.S. Why Batman was bad: A Scandinavian Debate about Children’s Consumption of Comics and Literature in the 1950s. Barn 2010, 3, 47–70. [Google Scholar]
- Buckingham, D.; Whiteman, N.; Willett, R.; Burn, A.N. The Impact of the Media on Children and Young People with a Particular Focus on Computer Games and the Internet; Prepared for the Byron Review on Children and New Technology; Department for Children, Schools and Families: London, UK, 2007.
- Buckingham, D.; Strandgaard Jensen, H. Beyond “media panics”: Reconceptualising public debates about children and media. J. Child. Media 2012, 6, 413–429. [Google Scholar] [CrossRef]
- Mentzoni, R.A.; Brunborg, G.S.; Molde, H.; Myrseth, H.; Skouverøe, K.J.M.; Hetland, J.; Pallesen, S. Problematic video game use: Estimated prevalence and associations with mental and physical health. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.A.; Shibuya, A.; Ihori, N.; Swing, E.L.; Bushman, B.J.; Sakamoto, A.; Rothstein, H.R.; Saleem, M. Violent video game effects on aggression, empathy, and prosocial behavior in eastern and western countries: A meta-analytic review. Psychol. Bull. 2010, 136, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.J.; Namkoong, K.; Ku, T.; Kim, S.J. The relationship between online game addiction and aggression, self-control and narcissistic personality traits. Eur. Psychiatry 2008, 23, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Király, O.; Griffiths, M.D.; King, D.L.; Lee, H.-K.; Lee, S.-Y.; Bányai, F.; Zsila, Á.; Takacs, Z.K.; Demetrovics, Z. Policy responses to problematic video game use: A systematic review of current measures and future possibilities. J. Behav. Addict. 2018, 7, 503–517. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, C.J. Evidence for publication bias in video game violence effects literature: A meta-analytic review. Aggress. Violent Behav. 2007, 12, 470–482. [Google Scholar] [CrossRef]
- Ferguson, C.J. Do angry birds make for angry children? A meta-analysis of video game influences on children’s and adolescents’ aggression, mental health, prosocial behavior, and academic performance. Perspect. Psychol. Sci. 2015, 10, 646–666. [Google Scholar] [CrossRef]
- Szycik, G.R.; Mohammadi, B.; Hake, M.; Kneer, J.; Samii, A.; Münte, T.F.; te Wildt, B.T. Excessive users of violent video games do not show emotional desensitization: An fMRI study. Brain Imaging Behav. 2017, 11, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Kühn, S.; Kugler, D.T.; Schmalen, K.; Weichenberger, M.; Witt, C.; Gallinat, J. Does playing violent video games cause aggression? A longitudinal intervention study. Mol. Psychiatry 2019, 24, 1220–1234. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.-h.S. Korea to classify gaming addiction as a disease. Business Korea, 27 May 2019. [Google Scholar]
- Aarseth, E.; Bean, A.M.; Boonen, H.; Colder Carras, M.; Coulson, M.; Das, D.; Deleuze, J.; Dunkels, E.; Edman, J.; Ferguson, C.J. Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. J. Behav. Addict. 2017, 6, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, S.; Nakayama, H.; Mihara, S.; Maezono, M.; Kitayuguchi, T.; Hashimoto, T. Inclusion of gaming disorder criteria in ICD-11: A clinical perspective in favor: Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (AARSETH ET AL.). J. Behav. Addict. 2017, 6, 293–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Király, O.; Demetrovics, Z. Inclusion of Gaming Disorder in ICD has more advantages than disadvantages: Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (Aarseth et al.). J. Behav. Addict. 2017, 6, 280–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Den Brink, W. ICD-11 Gaming Disorder: Needed and just in time or dangerous and much too early? Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (Aarseth et al.). J. Behav. Addict. 2017, 6, 290–292. [Google Scholar] [CrossRef] [Green Version]
- Van Rooij, A.J.; Ferguson, C.J.; Colder Carras, M.; Kardefelt-Winther, D.; Shi, J.; Aarseth, E.; Bean, A.M.; Bergmark, K.H.; Brus, A.; Coulson, M. A weak scientific basis for gaming disorder: Let us err on the side of caution. J. Behav. Addict. 2018, 7, 1–9. [Google Scholar] [CrossRef]
- Stevens, M.W.; Dorstyn, D.; Delfabbro, P.H.; King, D.L. Global prevalence of gaming disorder: A systematic review and meta-analysis. Aust. N. Z. J. Psychiatry 2020, 55, 553–568. [Google Scholar] [CrossRef]
- Anderson, C.A.; Gentile, D.A.; Buckley, K.E. Violent Video Game Effects on Children and Adolescents: Theory, Research, and Public Policy; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Allen, J.J.; Anderson, C.A. General aggression model. In The International Encyclopedia of Media Effects; John Wiley & Sons: Hoboken, NJ, USA, 2017; pp. 1–15. [Google Scholar]
- DeWall, C.N.; Anderson, C.A.; Bushman, B.J. The general aggression model: Theoretical extensions to violence. Psychol. Violence 2011, 1, 245–258. [Google Scholar] [CrossRef] [Green Version]
- Greitemeyer, T.; Mügge, D.O. Video games do affect social outcomes: A meta-analytic review of the effects of violent and prosocial video game play. Personal. Soc. Psychol. Bull. 2014, 40, 578–589. [Google Scholar] [CrossRef]
- Ward, M.R. Video games and crime. Contemp. Econ. Policy 2011, 29, 261–273. [Google Scholar] [CrossRef]
- Cunningham, S.; Engelstätter, B.; Ward, M.R. Understanding the effects of violent video games on violent crime. ZEW Cent. Eur. Econ. Res. Discuss. Pap. 2011. [Google Scholar] [CrossRef]
- Markey, P.M.; Markey, C.N.; French, J.E. Violent video games and real-world violence: Rhetoric versus data. Psychol. Pop. Media Cult. 2015, 4, 277–295. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, S.; Engelstätter, B.; Ward, M.R. Violent video games and violent crime. South. Econ. J. 2016, 82, 1247–1265. [Google Scholar] [CrossRef]
- Lee, C.; Kim, H.; Hong, A. Ex-post evaluation of illegalizing juvenile online game after midnight: A case of shutdown policy in South Korea. Telemat. Inform. 2017, 34, 1597–1606. [Google Scholar] [CrossRef]
- Choi, J.; Cho, H.; Lee, S.; Kim, J.; Park, E.-C. Effect of the online game shutdown policy on internet use, internet addiction, and sleeping hours in Korean adolescents. J. Adolesc. Health 2018, 62, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Hunt, A. The great masturbation panic and the discourses of moral regulation in nineteenth-and early twentieth-century Britain. J. Hist. Sex. 1998, 8, 575–615. [Google Scholar]
- Hier, S.P.; Lett, D.; Walby, K.; Smith, A. Beyond folk devil resistance: Linking moral panic and moral regulation. Criminol. Crim. Justice 2011, 11, 259–276. [Google Scholar] [CrossRef]
- Hunt, A. Moral regulation and making-up the new person: Putting Gramsci to work. Theor. Criminol. 1997, 1, 275–301. [Google Scholar] [CrossRef]
- Critcher, C. Widening the focus: Moral panics as moral regulation. Br. J. Criminol. 2009, 49, 17–34. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Petry, N.M.; Rehbein, F.; Ko, C.-H.; O’Brien, C.P. Internet gaming disorder in the DSM-5. Curr. Psychiatry Rep. 2015, 17, 72. [Google Scholar] [CrossRef]
- Stein, D.J.; Reed, G.M. ICD-11: The importance of a science of psychiatric nosology. Lancet Psychiatry 2019, 6, 6–7. [Google Scholar] [CrossRef]
- Shadloo, B.; Farnam, R.; Amin-Esmaeili, M.; Hamzehzadeh, M.; Rafiemanesh, H.; Jobehdar, M.M.; Ghani, K.; Charkhgard, N.; Rahimi-Movaghar, A. Inclusion of gaming disorder in the diagnostic classifications and promotion of public health response: Commentary to the “scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal”: A perspective from Iran. J. Behav. Addict. 2017, 6, 310–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zastrow, M. News Feature: Is video game addiction really an addiction? Proc. Natl. Acad. Sci. USA 2017, 114, 4268–4272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bean, A.M.; Nielsen, R.K.; Van Rooij, A.J.; Ferguson, C.J. Video game addiction: The push to pathologize video games. Prof. Psychol. Res. Pract. 2017, 48, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Dullur, P.; Starcevic, V. Internet gaming disorder does not qualify as a mental disorder. Aust. N. Z. J. Psychiatry 2018, 52, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Frances, A. The past, present and future of psychiatric diagnosis. World Psychiatry 2013, 12, 111–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakefield, J. DSM-5, psychiatric epidemiology and the false positives problem. Epidemiol. Psychiatr. Sci. 2015, 24, 188–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciriacy-Wantrup, S.V. Capital returns from soil-conservation practices. J. Farm Econ. 1947, 29, 1181–1196. [Google Scholar] [CrossRef]
- Carson, R.T. Contingent valuation: A user’s guide. Environ. Sci. Technol. 2000, 34, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Haab, T.C.; McConnell, K.E. Valuing Environmental and Natural Resources: The Econometrics of Non-Market Valuation; Edward Elgar Publishing: Cheltenham, UK, 2002. [Google Scholar]
- Arrow, K.; Solow, R.; Portney, P.R.; Leamer, E.E.; Radner, R.; Schuman, H. Report of the NOAA panel on contingent valuation. Fed. Regist. 1993, 58, 4601–4614. [Google Scholar]
- Jin, J.; Wan, X.; Lin, Y.; Kuang, F.; Ning, J. Public willingness to pay for the research and development of solar energy in Beijing, China. Energy Policy 2019, 134, 110962. [Google Scholar] [CrossRef]
- Zhu, L.; Song, Q.; Sheng, N.; Zhou, X. Exploring the determinants of consumer’s WTB and WTP for electric motorcycles using CVM method in Macau. Energy Policy 2019, 127, 64–72. [Google Scholar] [CrossRef]
- Woo, J.; Lim, S.; Lee, Y.-G.; Huh, S.-Y. Financial feasibility and social acceptance for reducing nuclear power plants: A contingent valuation study. Sustainability 2018, 10, 3833. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Chung, N.; Lee, W.S. Preserving the culture of Jeju Haenyeo (Women Divers) as a sustainable tourism resource. Sustainability 2020, 12, 564. [Google Scholar] [CrossRef]
- Zhao, F.; Huang, M. Exploring the Non-Use Value of Important Agricultural Heritage System: Case of Lingnan Litchi Cultivation System (Zengcheng) in Guangdong, China. Sustainability 2020, 12, 3638. [Google Scholar] [CrossRef]
- Jung, J.; Lee, W.S. Estimating the preservation value of the Confucianism symbol tree: Application of the contingent valuation method. Anatolia 2021, 1–13. [Google Scholar] [CrossRef]
- Humphreys, B.R.; Johnson, B.K.; Mason, D.S.; Whitehead, J.C. Estimating the value of medal success in the Olympic Games. J. Sports Econ. 2018, 19, 398–416. [Google Scholar] [CrossRef]
- Vinnicombe, T.; Sou, J.P.U. How can we correct for contingent valuation bias? A case study of the Macau Orchestra. Econ. Aff. 2019, 39, 346–362. [Google Scholar] [CrossRef]
- Shin, J.; Kim, Y.; Nam, H.; Cho, Y. Economic evaluation of healthcare technology improving the quality of social life: The case of assistive technology for the disabled and elderly. Appl. Econ. 2016, 48, 1361–1371. [Google Scholar] [CrossRef]
- Frew, E.; Wolstenholme, J.; Whynes, D. Willingness-to-pay for colorectal cancer screening. Eur. J. Cancer 2001, 37, 1746–1751. [Google Scholar] [CrossRef]
- Yasunaga, H.; Ide, H.; Imamura, T.; Ohe, K. Benefit evaluation of mass screening for prostate cancer: Willingness-to-pay measurement using contingent valuation. Urology 2006, 68, 1046–1050. [Google Scholar] [CrossRef]
- Shono, A.; Kondo, M.; Ohmae, H.; Okubo, I. Willingness to pay for public health services in rural Central Java, Indonesia: Methodological considerations when using the contingent valuation method. Soc. Sci. Med. 2014, 110, 31–40. [Google Scholar] [CrossRef]
- Tambor, M.; Pavlova, M.; Rechel, B.; Golinowska, S.; Sowada, C.; Groot, W. Willingness to pay for publicly financed health care services in Central and Eastern Europe: Evidence from six countries based on a contingent valuation method. Soc. Sci. Med. 2014, 116, 193–201. [Google Scholar] [CrossRef]
- Milligan, M.A.; Bohara, A.K.; Pagán, J.A. Assessing willingness to pay for cancer prevention. Int. J. Health Care Financ. Econ. 2010, 10, 301–314. [Google Scholar] [CrossRef]
- Asgary, A.; Willis, K.; Taghvaei, A.A.; Rafeian, M. Estimating rural households’ willingness to pay for health insurance. Eur. J. Health Econ. 2004, 5, 209–215. [Google Scholar] [CrossRef]
- Catma, S.; Varol, S. Willingness to pay for a hypothetical COVID-19 vaccine in the United States: A contingent valuation approach. Vaccines 2021, 9, 318. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Juan, Y.; Choi, Y.; Lee, C.-K. Estimating the preservation value of world heritage site using contingent valuation method: The case of the Li River, China. Sustainability 2019, 11, 1100. [Google Scholar] [CrossRef] [Green Version]
- Hanemann, M.; Loomis, J.; Kanninen, B. Statistical efficiency of double-bounded dichotomous choice contingent valuation. Am. J. Agric. Econ. 1991, 73, 1255–1263. [Google Scholar] [CrossRef]
- Bateman, I.J.; Langford, I.H.; Jones, A.P.; Kerr, G.N. Bound and path effects in double and triple bounded dichotomous choice contingent valuation. Resour. Energy Econ. 2001, 23, 191–213. [Google Scholar] [CrossRef]
- Bateman, I.J.; Carson, R.T.; Day, B.; Hanemann, M.; Hanley, N.; Hett, T.; Jones-Lee, M.; Loomes, G.; Mourato, S.; Pearce, D.W. Economic Valuation with Stated Preference Techniques: A Manual; Edward Elgar: Cheltenham, UK, 2002. [Google Scholar]
- Teng, C.-I. How do challenges increase customer loyalty to online games? Cyberpsychol. Behav. Soc. Netw. 2013, 16, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.-I. Look to the future: Enhancing online gamer loyalty from the perspective of the theory of consumption values. Decis. Support Syst. 2018, 114, 49–60. [Google Scholar] [CrossRef]
- Lopez-Feldman, A. Introduction to Contingent Valuation Using Stata; MPRA Paper No. 41018; MPRA: Munich, Germany, 2012. [Google Scholar]
- Feng, W.; Ramo, D.; Chan, S.; Bourgeois, J. Internet gaming disorder: Trends in prevalence 1998–2016. Addict. Behav. 2017, 75, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kim, B.-N.; Cho, S.-C.; Kim, J.-W.; Shin, M.-S.; Yoo, H.-J. Prevalence, correlates, and comorbidities of DSM-IV psychiatric disorders in children in Seoul, Korea. Asia Pac. J. Public Health 2015, 27, NP1942–NP1951. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, I.; Lim, M.H.; Paik, K.C.; Cho, S.; Kwon, H.-J.; Lee, S.G.; Yoo, S.-J.; Ha, M. Prevalence of attention-deficit/hyperactivity disorder and its comorbidity among Korean children in a community population. J. Korean Med. Sci. 2017, 32, 401–406. [Google Scholar] [CrossRef]
- Korean Statistics. Estimation of the Population; Korean Statistics: Seoul, Korea, 2020. [Google Scholar]
- Hong, M.; Park, B.; Lee, S.M.; Bahn, G.H.; Kim, M.J.; Park, S.; Oh, I.-H.; Park, H. Economic burden and disability-adjusted life years (DALYs) of attention deficit/hyperactivity disorder. J. Atten. Disord. 2020, 24, 823–829. [Google Scholar] [CrossRef]
Figure 1.
Structure of questionnaire.


{kind=link}
Table 1.
Types of the initial bid in the questionnaire.
| Bid (GD Diagnosis Test Price: KRW) | Number of Surveys |
|---|---|
| 100,000 | 171 |
| 140,000 | 170 |
| 180,000 | 170 |
| 220,000 | 170 |
| 260,000 | 170 |
| 300,000 | 170 |
| Total | 1021 |
Table 2.
Demographic characteristics of respondents (n = 1021).
| Number of Respondent (%) | ||
|---|---|---|
| Gender | Male | 512 (50.15%) |
| Female | 509 (49.85%) | |
| Age | 20s | 200 (19.59%) |
| 30s | 207 (20.27%) | |
| 40s | 248 (24.29%) | |
| 50s | 258 (25.27%) | |
| Over 60 | 108 (10.58%) | |
| Marriage | Yes | 654 (64.05%) |
| No | 367 (35.95%) | |
| Education | Less than high school | 216 (21.16%) |
| Attending/Graduated College | 142 (13.91%) | |
| Attending/Graduated University | 495 (48.48%) | |
| Attending/Graduated Graduate school | 168 (16.45%) | |
| Monthly income | Less than 2 M (KRW) | 121 (11.85%) |
| 2 M ~less than 3 M (KRW) | 180 (17.63%) | |
| 3 M ~ less than 4 M (KRW) | 205 (20.08%) | |
| 4 M ~ less than 5 M (KRW) | 183 (17.92%) | |
| 5 M ~ less than 6 M (KRW) | 142 (13.91%) | |
| More than 6 M (KRW) | 190 (18.61%) |
Table 3.
Detailed WTP responses by bid amount.
| Bid Amount (KRW) | Number of Samples | Respond | |||||
|---|---|---|---|---|---|---|---|
| Initial | Higher | Lower | Yes-Yes | Yes-No | No-Yes | No-No | |
| 100,000 | 200,000 | 50,000 | 171 | 49 | 43 | 38 | 41 |
| 140,000 | 280,000 | 70,000 | 170 | 32 | 29 | 44 | 65 |
| 180,000 | 360,000 | 90,000 | 170 | 37 | 28 | 32 | 73 |
| 220,000 | 440,000 | 110,000 | 170 | 21 | 28 | 41 | 80 |
| 260,000 | 520,000 | 130,000 | 170 | 27 | 23 | 33 | 87 |
| 300,000 | 600,000 | 150,000 | 170 | 20 | 27 | 27 | 96 |
| Total | 1021 | 186 | 178 | 215 | 442 | ||
Table 4.
WTP estimation results.
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Coefficient | p-Value | Coefficient | p-Value | |||
| Constant | 179.40 | *** | 0.000 | −21.57 | 0.805 | |
| Age | - | 3.98 | *** | 0.000 | ||
| Gender (Male) | - | 1.11 | 0.952 | |||
| Education | - | 5.27 | 0.577 | |||
| Income | - | 17.90 | ** | 0.002 | ||
| Marriage | - | −0.01 | 1.000 | |||
| Prior knowledge | - | −21.04 | 0.162 | |||
| Attitude | - | −4.39 | 0.657 | |||
| Agree | - | 10.73 | 0.054 | |||
| Suspicion of GD | - | −71.42 | *** | 0.007 | ||
| Interest on game | - | −5.33 | 0.470 | |||
| Log likelihood | −1244.08 | −1212.59 | ||||
**: p < 0.01, *** p < 0.001.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yoo, C.; Kim, Y.; Sohn, J.H. Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea. Sustainability 2021, 13, 8106. https://0-doi-org.brum.beds.ac.uk/10.3390/su13148106
AMA Style
Yoo C, Kim Y, Sohn JH. Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea. Sustainability. 2021; 13(14):8106. https://0-doi-org.brum.beds.ac.uk/10.3390/su13148106
Chicago/Turabian StyleYoo, Changsok, Yelim Kim, and Jee Hoon Sohn. 2021. "Evaluating the Social Cost of Conflict between New Media and Society: The Case of Gaming Disorder in South Korea" Sustainability 13, no. 14: 8106. https://0-doi-org.brum.beds.ac.uk/10.3390/su13148106
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.