
Why Do We Harm the Environment or Our Personal Health despite Better Knowledge? The Knowledge Action Gap in Healthy and Climate-Friendly Behavior

 , and
, and
Abstract
:
1. Introduction to the Knowledge-Action-Gap
2. Behavior Change Theories
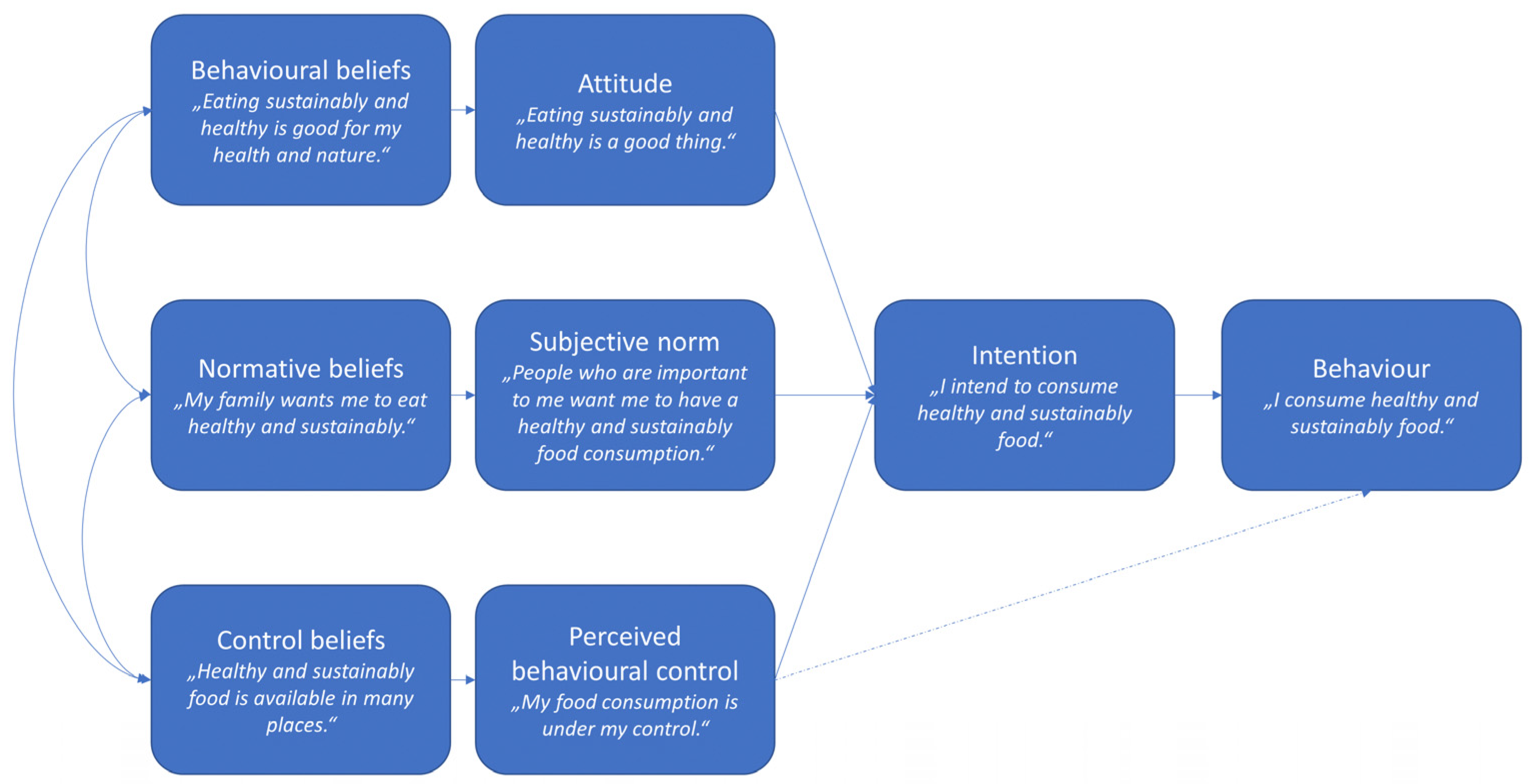
2.1. Theory of Planned Behavior
2.2. Stages of Change
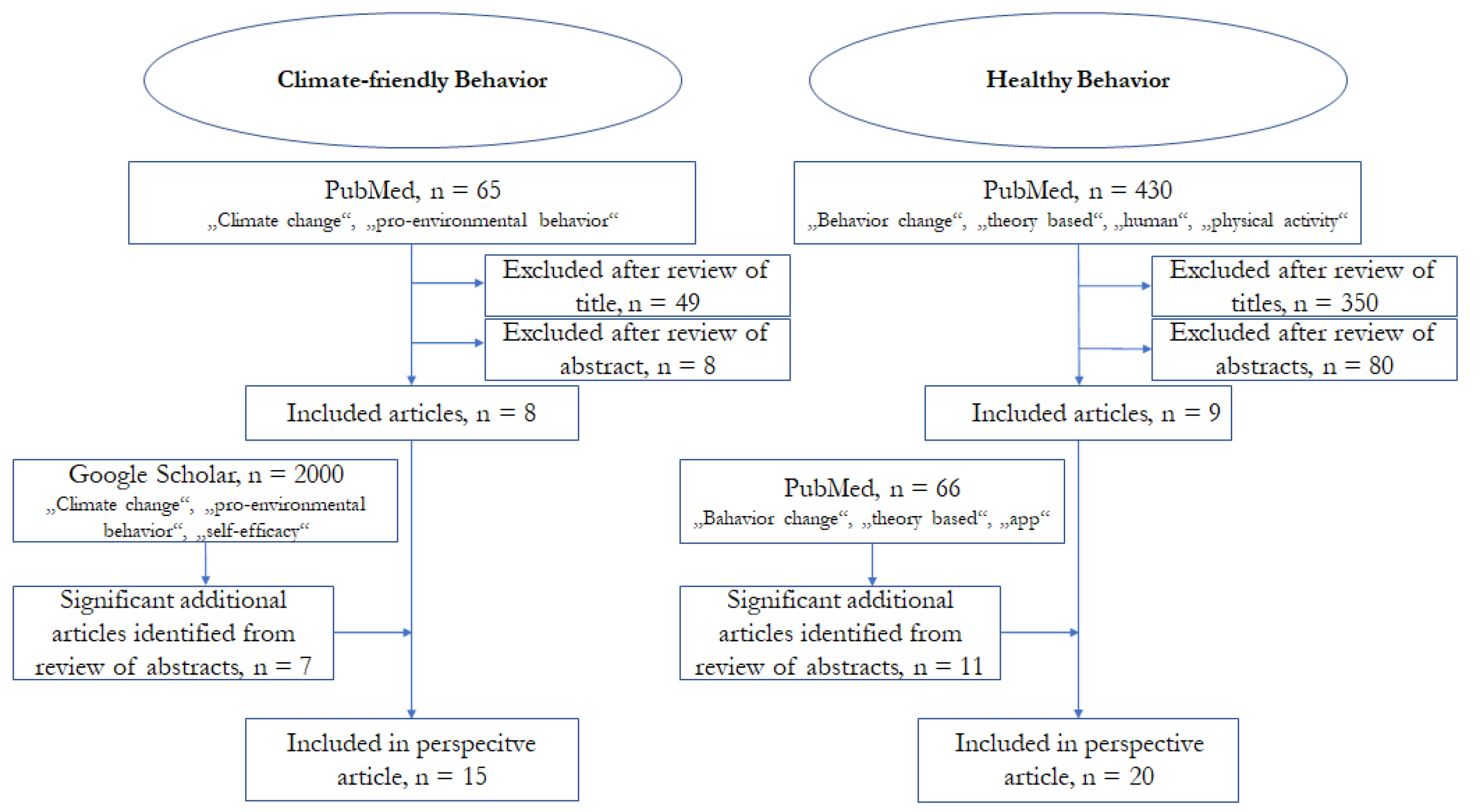
3. Methods
4. Healthy Behavior—Selected Examples from the Existing Literature
4.1. The Evaluation of Physical Activity Interventions
4.2. Targeted Interventions for Different Groups of People
4.3. App-Based Interventions
4.4. Long-Term Maintenance
4.5. Core Statement
5. Climate Friendly Behavior—Selected Examples from the Existing Literature
5.1. Current Research of Climate Friendly Behavior
5.2. Core Statement
6. Differences and Similarities in Pro-Environmental and Healthy Behavior
6.1. Differences
6.2. Similarities
7. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoegh-Guldberg, O.; Jacob, D.; Taylor, M. Impacts of 1.5 °C of Global Warming on Natural and Human Systems; Intergovernmental Panel on Climate Change: Geneva, Switzerland, 2018; pp. 175–181. ISBN 978-92-9169-151-7. [Google Scholar]
- The CAT Thermometer. 2021. Available online: https://climateactiontracker.org/global/cat-thermometer/x (accessed on 27 July 2021).
- Mann, T.; De Ridder, D.; Fujita, K. Self-regulation of health behavior: Social psychological approaches to goal setting and goal striving. Health Psychol. 2013, 32, 487–498. [Google Scholar] [CrossRef] [Green Version]
- Kollmuss, A.; Agyeman, J. Mind the gap: Why do people act environmentally and what are the barriers to pro-environmental behavior? Environ. Educ. Res. 2002, 8, 239–260. [Google Scholar] [CrossRef] [Green Version]
- Keller, S. Motivation zur verhaltensänderung-aktuelle deutschsprachige forschung zum transtheoretischen modell. Z. Gesundh. 2004, 12, 35–38. [Google Scholar] [CrossRef]
- Arena, R.; Guazzi, M.; Lianov, L.; Whitsel, L.; Berra, K.; Lavie, C.J.; Kaminsky, L.; Williams, M.; Hivert, M.-F.; Franklin, N.C.; et al. Healthy Lifestyle Interventions to Combat Noncommunicable Disease—A Novel Nonhierarchical Connectivity Model for Key Stakeholders: A Policy Statement From the American Heart Association, European Society of Cardiology, European Association for Cardiovascular Prevention and Rehabilitation, and American College of Preventive Medicine. Mayo Clin. Proc. 2015, 90, 1082–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contento, I.R.; Basch, G.I.; Bronner, Y.L.; Lytle, L.A.; Maloney, S.K. The effectiveness of nutrition education and implications for nutrition education policy, programs, and research: A review of research. J. Nutr. Educ. 1995, 27, 277–423. [Google Scholar]
- Rimal, R.N. Closing the knowledge-behavior gap in health promotion: The mediating role of self-efficacy. Health Commun. 2009, 12, 219–237. [Google Scholar] [CrossRef] [PubMed]
- Moura, L.R.; Lamounier, J.R.; Guimarães, P.R.; Duarte, J.M.; Beling, M.T.C.; Pinto, J.A.; Goulart, E.M.d.A.; Grillo, C.d.F.C. The gap between knowledge on HIV/Aids and sexual behavior: A study of teenagers in vespasiano, minas gerais state, brazil. Cad. Saude Publica 2013, 29, 1008–1018. [Google Scholar] [CrossRef]
- Nagy-Pénzes, G.; Vincze, F.; Sándor, J.; Bíró, É. Does better health-related knowledge predict favorable health behavior in adolescents? Int. J. Environ. Res. Public Health 2020, 17, 1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Gennari, A. Editorial: Why are guidelines not followed in clinical practice? Breast 2017, 32, 245–246. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. (accessed on 23 June 2021).
- Vandenberghe, D.; Albrecht, J. The financial burden of non-communicable diseases in the European Union: A systematic review. Eur. J. Public Health 2020, 30, 833–839. [Google Scholar] [CrossRef]
- Lifestyle Medicine—Global Aliance. 2020. Available online: https://lifestylemedicineglobal.org/lifestyle-medicine/ (accessed on 30 July 2020).
- Rabia, M.; Knäuper, B.; Miquelon, P. The eternal quest for optimal balance between maximizing pleasure and minimizing harm: The compensatory health beliefs model. Br. J. Health 2006, 11 Pt 1, 139–153. [Google Scholar] [CrossRef] [PubMed]
- Amrein, M.A.; Scholz, U.; Inauen, J. Compensatory health beliefs and unhealthy snack consumption in daily life. Appetite 2021, 157, 104996. [Google Scholar] [CrossRef]
- Mitchell, D.; Heaviside, C.; Vardoulakis, S.; Huntingford, C.; Masato, G.; Guillod, B.P.; Frumhoff, P.; Bowery, A.; Wallom, D.; Allen, M. Attributing human mortality during extreme heat waves to anthropogenic climate change. Environ. Res. Lett. 2016, 11, 74006. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef] [PubMed]
- Abrahamse, W. Encouraging Pro-Environmental Behaviour. What Works, What Doesn’t, and Why; Academic Press: London, UK, 2019. [Google Scholar]
- Heller, L.J.; Skinner, C.S.; Tomiyama, A.J.; Epel, E.S.; Hall, P.A.; Allan, J.; LaCaille, L.; Randall, A.K.; Bodenmann, G.; Li-Tsang, C.W.P.; et al. Theories of Behavior Change. Encycl. Behav. Med. 2013, 1, 1963. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Hasler, G.; Klaghofer, R.; Buddeberg, C. Der Fragebogen zur Erfassung der Veränderungsbereitschaft (FEVER). Psychother. Psychosom. Med. Psychol. 2003, 53, 406–411. [Google Scholar] [CrossRef]
- Krebs, P.; Norcross, J.C.; Nicholson, J.M.; Prochaska, J.O. Stages of change and psychotherapy outcomes: A review and meta-analysis. J. Clin. Psychol. 2018, 74, 1964–1979. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.F. Self-efficacy or collective efficacy within the cognitive theory of stress model: Which more effectively explains people’s self-reported pro environmental behavior? J. Environ. Psychol. 2015, 42, 66–75. [Google Scholar] [CrossRef]
- Page, N.; Page, M. Climate change: Time to do something different. Front. Psychol. 2014, 5, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Knoll, N.; Rieckmann, N.; Schwarzer, R. Brief Cope. Eur. J. Personal. 2005, 19, 229–247. [Google Scholar] [CrossRef]
- Berry, J.M.; West, R.L.; Dennehey, D.M. Reliability and validity of the Memory Self-Efficacy Questionnaire. Dev. Psychol. 1989, 25, 701–713. [Google Scholar] [CrossRef]
- Norcross, J.C.; Krebs, P.M.; Prochaska, J.O. Stages of change. J. Clin. Psychol. 2011, 67, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Romain, A.J.; Bortolon, C.; Gourlan, M.; Carayol, M.; Decker, E.; Lareyre, O.; Ninot, G.; Boiché, J.; Bernard, P. Matched or nonmatched interventions based on the transtheoretical model to promote physical activity. A meta-analysis of randomized controlled trials. J. Sport Health Sci. 2018, 7, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haileamlak, A. Physical inactivity: The major risk factor for non-communicable diseases. Ethiop. J. Health Sci. 2019, 29, 810. [Google Scholar] [CrossRef]
- Howlett, N.; Trivedi, D.; Troop, N.A.; Chater, A.M. Are physical activity interventions for healthy inactive adults effective in promoting behavior change and maintenance, and which behavior change techniques are effective? A systematic review and meta-analysis. Transl. Behav. Med. 2019, 9, 147–157. [Google Scholar] [CrossRef]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kohl Iii, H.W.; Pettee Gabriel, K.K.; Han, H. Differential use of strategic constructs of the transtheoretical model across accelerometer-determined sedentary time. Am. J. Health Behav. 2020, 44, 18–25. [Google Scholar] [CrossRef]
- Romain, A.J.; Caudroit, J.; Hokayem, M.; Bernard, P. Is there something beyond stages of change in the transtheoretical model? The state of art for physical activity. Can. J. Behav. Sci. 2018, 50, 42–53. [Google Scholar] [CrossRef]
- Han, H.; Pettee Gabriel, K.; Kohl, H.W. Application of the transtheoretical model to sedentary behaviors and its association with physical activity status. PLoS ONE 2017, 12, e0176330. [Google Scholar] [CrossRef] [Green Version]
- Keyworth, C.; Epton, T.; Goldthorpe, J.; Calam, R.; Armitage, C.J. Delivering opportunistic behavior change interventions: A systematic review of systematic reviews. Prev. Sci. Off. J. Soc. Prev. Res. 2020, 21, 319–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flannery, C.; McHugh, S.; Anaba, A.E.; Clifford, E.; O’Riordan, M.; Kenny, L.C.; McAuliffe, F.M.; Kearney, P.M.; Byrne, M. Enablers and barriers to physical activity in overweight and obese pregnant women: An analysis informed by the theoretical domains framework and com-b model. BMC Pregnancy Childbirth 2018, 18, 178. [Google Scholar] [CrossRef]
- Sharma, M.; Nahar, V.K. Promoting physical activity in upper elementary children using multi-theory model (mtm) of health behavior change. J. Prev. Med. Hyg. 2018, 59, 267–276. [Google Scholar] [CrossRef]
- Milne-Ives, M.; Lam, C.; Cock, C.; Van Velthoven, M.H.; Meinert, E. Mobile apps for health behavior change in physical activity, diet, drug and alcohol use, and mental health: Systematic review. JMIR MHealth UHealth 2020, 8, e17046. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.S.H.; Rouf, A.; Allman-Farinelli, M. Effectiveness and behavioral mechanisms of social media interventions for positive nutrition behaviors in adolescents: A systematic review. J. Adolesc. Health Off. 2018, 63, 531–545. [Google Scholar] [CrossRef]
- Schoeppe, S.; Alley, S.; Rebar, A.L.; Hayman, M.; Bray, N.A.; van Lippevelde, W.; Gnam, J.-P.; Bachert, P.; Direito, A.; Vandelanotte, C. Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: A review of quality, features and behaviour change techniques. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 83. [Google Scholar] [CrossRef]
- West, J.H.; Belvedere, L.M.; Andreasen, R.; Frandsen, C.; Hall, P.C.; Crookston, B.T. Controlling your appetite: How diet and nutrition-related mobile apps lead to behavior change. JMIR MHealth UHealth 2017, 5, e95. [Google Scholar] [CrossRef]
- Ferrara, G.; Kim, J.; Lin, S.; Hua, J.; Seto, E. A focused review of smartphone diet-tracking apps: Usability, functionality, coherence with behavior change theory, and comparative validity of nutrient intake and energy estimates. JMIR MHealth UHealth 2019, 7, e9232. [Google Scholar] [CrossRef]
- McKay, F.H.; Slykerman, S.; Dunn, M. The app behavior change scale: Creation of a scale to assess the potential of apps to promote behavior change. JMIR MHealth UHealth 2019, 7, e11130. [Google Scholar] [CrossRef] [PubMed]
- Middelweerd, A.; Te Velde, S.J.; Mollee, J.S.; Klein, M.C.; Brug, J. App-based intervention combining evidence-based behavior change techniques with a model-based reasoning system to promote physical activity among young adults (active2gether): Descriptive study of the development and content. JMIR Res. Protoc. 2018, 7, e185. [Google Scholar] [CrossRef] [Green Version]
- Brickwood, K.-J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-based wearable activity trackers increase physical activity participation: Systematic review and meta-analysis. JMIR MHealth UHealth 2019, 7, e11819. [Google Scholar] [CrossRef]
- Ringeval, M.; Wagner, G.; Denford, J.; Paré, G.; Kitsiou, S. Fitbit-based interventions for healthy lifestyle outcomes: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e23954. [Google Scholar] [CrossRef] [PubMed]
- McKay, F.H.; Wright, A.; Shill, J.; Stephens, H.; Uccellini, M. Using health and well-being apps for behavior change: A systematic search and rating of apps. JMIR MHealth UHealth 2019, 7, e11926. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.P.; Daniel, C.L.; Thind, H.; Benitez, T.J.; Pekmezi, D. Applying psychological theories to promote long-term maintenance of health behaviors. Am. J. Lifestyle Med. 2016, 10, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Kwasnicka, D.; Dombrowski, S.U.; White, M.; Sniehotta, F. Theoretical explanations for maintenance of behaviour change: A systematic review of behaviour theories. Health Psychol. Rev. 2016, 10, 277–296. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Spring, B.; Nigg, C.R. Multiple health behavior change research: An introduction and overview. Prev. Med. 2008, 46, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Kravitz, R.L.; Reisman, A. Getting from intention to action. J. Gen. Intern. Med. 2016, 31, 703–704. [Google Scholar] [CrossRef] [Green Version]
- Lorenzoni, I.; Nicholson-Cole, S.; Whitmarsh, L. Barriers perceived to engaging with climate change among the UK public and their policy implications. Glob. Environ. Change 2007, 17, 445–459. [Google Scholar] [CrossRef]
- Busch, K.C.; Ardoin, N.; Gruehn, D.; Stevenson, K. Exploring a theoretical model of climate change action for youth. Int. J. Sci. Educ. 2019, 41, 2389–2409. [Google Scholar] [CrossRef]
- Stevenson, K.; Peterson, N. Motivating action through fostering climate change hope and concern and avoiding despair among adolescents. Sustainability 2016, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Yu, T. The Moderating Effects of Students’ Personality Traits on Pro-Environmental Behavioral Intentions in Response to Climate Change. Int. J. Environ. Res. Public Health 2017, 14, 1472. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Hurlstone, M.J.; Leviston, Z.; Walker, I.; Lawrence, C. Climate Change From a Distance: An Analysis of Construal Level and Psychological Distance From Climate Change. Front. Psychol. 2019, 10, 230. [Google Scholar] [CrossRef]
- Id, E.C.C.; Centeno, D.; Todd, A.M. The role of climate change education on individual lifetime carbon emissions. PLoS ONE 2020, 15, e0206266. [Google Scholar] [CrossRef] [Green Version]
- Muroi, S.K.; Bertone, E. From Thoughts to Actions: The Importance of Climate Change Education in Enhancing Students’ Self-Efficacy. Aust. J. Environ. Educ. 2019, 35, 123–144. [Google Scholar] [CrossRef]
- Lauren, N.; Fielding, K.S.; Smith, L.; Louis, W.R. You did, so you can and you will: Self-efficacy as a mediator of spillover from easy to more difficult pro-environmental behaviour. J. Environ. Psychol. 2016, 48, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Exercise of human agency through collective efficacy. Curr. Dir. Psychol. Sci. 2000, 9, 75–78. [Google Scholar] [CrossRef]
- Masud, M.M.; Al-Amin, A.Q.; Junsheng, H.; Ahmed, F.; Yahaya, S.R.; Akhtar, R.; Banna, H. Climate change issue and theory of planned behaviour: Relationship by empirical evidence. J. Clean. Prod. 2016, 113, 613–623. [Google Scholar] [CrossRef]
- Mackay, C.M.L.; Schmitt, M.T.; Lutz, A.E.; Mendel, J. ScienceDirect Recent developments in the social identity approach to the psychology of climate change. Curr. Opin. Psychol. 2021, 42, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Brosch, T. ScienceDirect Affect and emotions as drivers of climate change perception and action: A review. COBEHA 2021, 42, 15–21. [Google Scholar] [CrossRef]
- Sörqvist, P.; Marsh, J.E. The cognitive psychology of climate change. Front. Psychol. 2019. [Google Scholar] [CrossRef]
- Gardner, G.T.; Stern, P.C. The short list: The most effective actions U.S. Households can take to curb climate change. Environ. Sci. Policy Sustain. Dev. 2008, 50, 12–25. [Google Scholar] [CrossRef]
- Peters, E.; Shoots-Reinhard, B.; Evans, A.T.; Shoben, A.; Klein, E.; Tompkins, M.K.; Romer, D.; Tusler, M. Pictorial warning labels and memory for cigarette health-risk information over time. Annals of Behavioral Medicine. Publ. Soc. Behav. Med. 2019, 53, 358–371. [Google Scholar] [CrossRef] [PubMed]
- Amrein, M.A.; Lüscher, J.; Berli, C.; Radtke, T.; Scholz, U. Do daily compensatory health beliefs predict intention to quit and smoking behavior? A daily diary study during smoking cessation. Int. J. Environ. Res. Public Health 2020, 17, 6419. [Google Scholar] [CrossRef]
- Nigg, C.R.; Lee, H.; Hubbard, A.E.; Min-Sun, K. Gateway health behaviors in college students: Investigating transfer and compensation effects. J. Am. Coll. Health 2009, 58, 39–44. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Stage | Precontemplation | Contemplation | Preparation | Action | Maintenance |
|---|---|---|---|---|---|
 | |||||
| Definition | The person enters a situation but does not think that he/she has a problem. The problem is either not conscious, or it is ignored. | The person begins to realize that a problem exists. However, he/she is still struggling to understand the problem in terms of causation and possible solutions. | The person has tried at least once to change his/her problem behavior. Although this attempt was unsuccessful, he/she has learned from it. He/She plans to address his/her problem behavior again soon. | The person has started to change his/her behavior or environment actively. Difficulties become apparent in the process. However, he/she tries to overcome them and seeks the necessary support. | The person has succeeded in making significant changes and achieving essential treatment goals. However, he/she has difficulty maintaining the changes and fears so that relapse may occur. The treatment he/she is seeking is relapse prevention. |
| Climate friendly behavior | The person does not consider changing behavior for example to reduce car use. The reason could be that he/she is not fully aware of the environmental problems associated with his/her own behavior. | The person thought about changing behavior for example taking public transport instead of the car but had not started acting yet. | The person has set the intention to change behavior and may at this point have already tried to use the public transport on occasions | The person has changed his/her behavior and most of the time he/she use for example public transport. | The person has managed to make the desired behavior change such as using public transport over time. There is a chance of relapse when the person reverts to one of the earlier stages. |
| Healthy behavior | The person is mostly unaware of its problems, for example alcohol exposure. The motivation to change is in many cases conditioned by the external environment. | The person perceives that a problem exists. She or he is thinking about tackling the problem, but it is not clear how to overcome this challenge. For example, reducing alcohol consumption seems to cost too much effort and willpower. | The person has concrete plans to change the problematic behavior. She or he has already tried to reduce the amount of alcohol, but it was not effective yet. | The person has successfully changed the dysfunctional behavior. She or he is for example abstinent from alcohol abuse for a period from one day to six months. | In this stage the person prevents a relapse. In case of addiction, maintenance can last a lifetime. |
| Factor | Healthy Behavior | Climate Friendly Behavior |
|---|---|---|
| Concerns mainly the person her/himself. | Concerns mainly the planet, society, and future generations. |
| Effects are necessarily noticeable (not always directly but after a period). State health care system is burdened. | Effects are not necessarily noticeable (especially in European countries). Quality of life of future and current generations and state funds are burdened. |
| Healthy behavior is often clear. | Climate-friendly action and its concrete implementation into daily life is often unclear and difficult. |
| Factor | Healthy Behavior and Climate Friendly Behavior |
|---|---|
| Implementation of the respective behavior is often difficult. |
| Knowledge alone is not sufficient to achieve a change in behavior. |
| In the case of deterrent images and themes there is a habituation effect. |
| The biggest problem is people with no willingness to act. |
| A compensatory heuristic is often used to justify misconduct. |
| Self-efficacy is one of the most important determinants to change behavior. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frick, M.; Neu, L.; Liebhaber, N.; Sperner-Unterweger, B.; Stötter, J.; Keller, L.; Hüfner, K. Why Do We Harm the Environment or Our Personal Health despite Better Knowledge? The Knowledge Action Gap in Healthy and Climate-Friendly Behavior. Sustainability 2021, 13, 13361. https://0-doi-org.brum.beds.ac.uk/10.3390/su132313361
Frick M, Neu L, Liebhaber N, Sperner-Unterweger B, Stötter J, Keller L, Hüfner K. Why Do We Harm the Environment or Our Personal Health despite Better Knowledge? The Knowledge Action Gap in Healthy and Climate-Friendly Behavior. Sustainability. 2021; 13(23):13361. https://0-doi-org.brum.beds.ac.uk/10.3390/su132313361
Chicago/Turabian StyleFrick, Melanie, Leonie Neu, Nina Liebhaber, Barbara Sperner-Unterweger, Johann Stötter, Lars Keller, and Katharina Hüfner. 2021. "Why Do We Harm the Environment or Our Personal Health despite Better Knowledge? The Knowledge Action Gap in Healthy and Climate-Friendly Behavior" Sustainability 13, no. 23: 13361. https://0-doi-org.brum.beds.ac.uk/10.3390/su132313361