
Incorporating Fuzzy Cognitive Inference for Vaccine Hesitancy Measuring
by
 ,
,
Kun Sun
1 ,
,
Tian-Fang Zhao
1,*, 
Xiao-Kun Wu
2,
Kai-Sheng Lai
1,
Wei-Neng Chen
2 and
Jin-Sheng Zhang
1,* 1
School of Journalism & Communication, Jinan University, Guangzhou 510630, China
2
School of Computer Science and Engineering, South China University of Technology, Guangzhou 510006, China
*
Authors to whom correspondence should be addressed.
Sustainability 2022, 14(14), 8434; https://0-doi-org.brum.beds.ac.uk/10.3390/su14148434
Submission received: 3 May 2022
/
Revised: 3 July 2022
/
Accepted: 4 July 2022
/
Published: 10 July 2022
(This article belongs to the Topic Applied System on Biomedical Engineering, Healthcare and Sustainability)
Abstract
:Vaccine hesitancy plays a key role in vaccine delay and refusal, but its measurement is still a challenge due to multiple intricacies and uncertainties in factors. This paper attempts to tackle this problem through fuzzy cognitive inference techniques. Firstly, we formulate a vaccine hesitancy determinants matrix containing multi-level factors. Relations between factors are formulated through group decision-making of domain experts, which results in a fuzzy cognitive map. The subjective uncertainty of linguistic variables is expressed by fuzzy numbers. A double-weighted method is designed to integrate the distinguished decisions, in which the subjective hesitancy is considered for each decision. Next, three typical scenarios are constructed to identify key and sensitive factors under different experimental conditions. The experimental results are further discussed, which enrich the approaches of vaccine hesitancy estimation for the post-pandemic global recovery.
1. Introduction
The global pandemic of COVID-19 (SARS-CoV-2) has been one of the most hazardous public health emergencies over the past few years. A report from WHO shows that there have been 544,324,069 confirmed cases as of 30 June 2022, including 6,332,963 deaths [1]. Though many resources have been devoted to epidemic prevention, such as respirator masks, social distancing, physical quarantine, etc., the fast-evolving COVID-19 variants are still a threat to the human race. Vaccination is considered one of the most essential ways to prevent the pandemic [2]. Many vaccines have been tested, granted, and eventually produced and delivered [3], such as the Moderna mRNA-1273 [4,5], Pfizer/BioNTech BNT162b2 [6], and Janssen Ad26.COV2-S [7]. However, the newly emerged Omicron variants show the sharpest growth rate over other variants of concern (VOA). For examples, the original virus of COVID-19 is said to have an R0 of 2.5, and the R0 of the delta variant (B.1.617.2) is up to 7, while the R0 of omicron variants can be up to 10 as estimated by the researchers in London School of Hygiene & Tropical Medicine [8]. Currently, omicron has developed at least three sublineages (BA.1, BA.2, and BA.3) [9], which means that the vaccine campaigns against COVID-19 cannot terminate soon [10,11]. A global vaccination dataset published in Natural Human Behavior in June 2022 shows that the global vaccination coverage with a complete initial protocol has reached 60.62%. The vaccination rate is highly related to the level of regional economy, with 77.96% in middle- and high-income countries, 54.27% in middle- and low-income countries, and 14.43% in low-income countries [12]. Vaccine hesitancy plays a significant role in both the high-income and low-income countries [12]. To improve the vaccination rate, it is necessary to figure out key factors leading to vaccine hesitancy.
Existing studies of vaccine hesitancy can be divided into two categories. The first category focuses on some macroscopic factors leading to vaccine hesitancy, such as the factors of socioeconomics [13], political policies [14], scientific cognitive attitudes [15], and media environment [16]. These studies are usually based on some qualitative discussion and empirical analysis [17]. These studies give insights into realistic problems and provide instructive comments to some extent. Since these factors are not constructed mathematically, their measurement is still a challenge. The second category focuses on the quantitative analysis of factors influencing vaccine hesitancy. Questionnaires are the mostly commonly seen method of investigation [18,19]. These studies provide experimental evidence of the vaccine hesitancy happening in specific populations or regions [19], such as children and adolescents [20,21,22]. However, a holistic view of the key factors of vaccine hesitancy and the measurement of the factors’ relationships needs to be further studied. Luckily, the organization “WHO EURO Vaccine Communications Working Group” has noticed this problem, and therefore defined the vaccine hesitancy determinants matrix in 2015, which illustrates the major 24 factors influencing vaccine hesitancy. However, the complex and nonlinear relations among the 24 factors are hard to be defined by simple multi-variable linear equations, as the boundaries among the values of factors are blurred. For example, “media environment” can be assigned values within the range of {“low”, “middle”, “high”}, where the numerical range of “low” and “middle” is partly overlapped.
This study attempts to measure the nonlinear and uncertain relationships among factors of vaccine hesitancy by incorporating fuzzy cognitive inference techniques. The major contributions are as follows:
- (1)
- Designing a double-weighted group decision-making strategy to measure nonlinear correlations among factors of vaccine hesitancy determinants. Eight experts from three professions (hospital, government, and academia) are invited to finish the determinants matrix composed of the edges between a pair of factors. Features of edges include information of sign, weight, and certainty of their decision. Two weights are considered in integrating the decisions. The first level of weight concerns the relationship strength decided by each expert, and the second level of weight concerns the certainty degree of each decision. This strategy ensures an independent and efficient group decision-making process.
- (2)
- Inferring the state transition and interactive processes of factors through the fuzzy cognitive map. In the process, the fuzzy number is used to describe the fuzzy language of experts, with the trapezoidal fuzzy number of edge weights and the triangular fuzzy number of the certainties. Finally, a decision matrix with 24 × 24 dimensions is built to serve as the adjacent matrix of the fuzzy cognitive map.
- (3)
- Three scenarios are designed to simulate government, propaganda, and medical scenarios. Simulation results help identify the sensitive factors under different scenarios that need extra attention. An application case is conducted to demonstrate how the system can work in reality.
2. Related Work
2.1. Vaccine Hesitancy
Vaccine hesitancy describes the delay of people in receiving or refusing vaccine injections, even though the vaccination service is available [18]. Early in 2011, the World Health Organization (WHO) proposed the 3Cs model of vaccine hesitancy, which contains three kinds of factors (referring to confidence, complacency, and convenience) [23]. Later in 2015, WHO SAGE Group concluded the determinants of vaccine hesitancy and condensed the “Vaccine hesitancy Determinants Matrix” based on the 3Cs model from three impact scenarios: contextual, personal, and individual [18]. In 2019, the WHO ranked vaccine hesitancy as one of the top 10 global health threats [24].
From a macroscopic perspective, vaccine hesitancy—which involves complicated factors in religious, cultural, political, economic, medical, and geographical areas—is a complex social issue. First, as a political and economic issue, vaccine hesitancy is considered a kind of disempowerment of the public sphere. Though modest economic incentives can increase the vaccination rate [14], “vaccine nationalism” [25] still hinders a higher vaccination rate due to realistic reasons (e.g., huge economic costs, unreasonable vaccination policies, or unfair vaccine distribution) [16]. Second, improving public scientific knowledge is vital in eliminating vaccine hesitancy. Existing studies have illustrated that people in countries with good scientific trust hold better vaccine confidence [26]. Therefore, the promotion of scientific awareness of the public contributes to the reduction of vaccine hesitancy. Third, as a social identity issue, individuals with vaccine hesitancy have formed a close circle with cultural identity in the cyber society [27], which may the biggest problem in eliminating vaccine hesitancy.
From a microscopic perspective, studies related to vaccine hesitancy of COVID-19 can be summarized into two categories: empirical investigative studies and empirical exploratory studies. Most empirical studies use questionnaires to investigate the public attitude toward COVID-19 vaccines. Recently, a survey published in Nature [28] showed that, though doctors are usually considered as the authority in vaccination promotion, media reports give the false impression that there is widespread vaccine controversy in the doctor community. Enhancing consensus in this community can help improve the public trust level for vaccines. Furthermore, the vaccination rate among children also attracts much attention. Existing studies show that the parents’ attitudes about children’s vaccination are affected by complicated factors, including economic incentives, compensatory measures, punishment regulations, et al. [22].
Some mathematical analyses on vaccine hesitancy have also been conducted during the prevalence of COVID-19 [29], such as predicting epidemic spread effect through data mining [30], analyzing the networked risks through propagation models [31,32], generating non-pharmacological interventions through optimization methods [33], etc.
Overall, both qualitative and quantitative studies play an important role in studying vaccine hesitancy. The qualitative studies are usually based on the methods of field research, interviewing, discourse analysis, grounded theory, ethnography, etc., which inspire the latter quantitative studies [34] or provide an in-depth discussion of the latter’s analysis results. The quantitative studies are usually conducted based on questionnaire surveys, regression analysis, factorial analysis, etc., which provide some measurable, educible, and cumulative findings. In the context of global recovery, it is promising to combine the two kinds of studies, so that vaccine hesitancy can be fully understood, measured, and adjusted [35].
2.2. Fuzzy Cognitive Inference
Computing methods are critical tools in dealing with the complexity of infectious disease dynamics [36,37]. However, most data in the medical field have the problems of fuzziness and uncertainties [38], due to substantial individual differences (e.g., personal health status, medical history, medical diagnosis, demographic characteristics, and other standard medical information) [39] and measurement errors [38]. Likewise, vaccine hesitancy also involves huge uncertainties that are hard to be represented by quantitative values, such as the measurement of social and religious culture, political and media environment, historical and geographical information, etc. [40]. In many other research fields, the fuzziness of data information is inevitably “neglected” [41], for example, neglecting the interactions among multiple factors in the modeling process [42] and correcting the values from the ambiguous details [43]. However, in healthcare decision support systems, the ambiguous details cannot be simply ignored or corrected due to the precise requirements. Instead, it requires a fuzzy modeling approach [44] to extract causal relationships from fuzzy information.
Fuzzy cognitive map (FCM), as a classical and powerful mathematical method for fuzzy inference, can help extract the knowledge of experts from various fields. It has been extensively applied in many fields (e.g., sociology [45], Bioinformatics [46], pattern recognition [47], image processing, machine learning [48], medical diagnosis, and decision support systems [49]) over the past few years. It facilitates the intuitive description of the causal and interactive relationships among factors [50], and provides a measurement tool for observing complex systems [51]. A successful FCM depends on two aspects: how well the prior knowledge is collected and understood, and how well the fuzzy boundaries of linguistic values are handled [52].
Regarding the FCM studies during COVID-19, most focus on the clinical diagnosis of the epidemic or the supply chain of vaccines [43], for example, inferring whether a suspected case is infected with the COVID-19 virus based on Advanced Fuzzy Cognitive Map (AFCM) in state-space [53], simulating the propagation dynamics of the epidemic [38], or predicting the spread of the virus [40,54]. Furthermore, in the field of the vaccine supply chain, a modified fuzzy geometric mean (FGM) method was developed to determine the selection of suitable alternative suppliers [54]. The Analytic Hierarchy and Processes (AHP) technique with FCM was used to identify 13 factors that may affect the supply chain of COVID-19 vaccines [55].
Though FCM has shown its value and potential in helping to prevent the prevalence of COVID-19, there are still few studies investigating vaccine hesitancy, though it is a promising direction for determining the key factors in vaccine hesitancy [56].
3. Data and Method
3.1. Fuzzy Cognitive Map of Vaccine Hesitancy
Fuzzy Cognitive Map (FCM), a map-based knowledge representation method [57], was proposed by Kosko in 1986 [58]. It is a kind of soft computing method that is tolerant of uncertainty and approximation. Notably, FCM follows the principles of fuzzy logic, in which the values are ranged within a normalized scope, usually [0, 1] or [−1, +1] [59]. Compared to Boolean logic, fuzzy logic can express fuzzy concepts or relations in problems, which is closer to human observation, reasoning, and decision-making [60,61]. In this paper, FCM as one of the most typical fuzzy logic methods is adopted to bridge the gap between the fuzzy knowledge and the quantitative expression of vaccine hesitancy. It possesses advantages in three aspects: embodying the knowledge and experience of experts in resolving problems, quantifying the fuzzy descriptions of linguistic variables, and providing an explainable way for knowledge inference.
Figure 1 shows a typical case of FCM, where nodes represent concepts and edges represent relationships among nodes. The weights of edges are determined by prior knowledge, whose absolute values represent the strength of relationships, and plus-or-minus signs denote the positive-or-negative effect of relationships. In this paper, vaccine hesitancy is regarded as a complex dynamic system composed of multiple factors, in which the factors are defined as conceptual nodes in the FCM of vaccine hesitancy, and the causal effects among the factors are defined as edges. The FCM of vaccine hesitancy is defined as below. Let represent the ith factor influencing vaccine hesitancy, in which . The edges and weights of FCM are determined in a weighted matrix:
where > 0 means a positively correlated relationship between the conceptual nodes and . Namely, an increased value of will lead to the increased value of . < 0, means a negatively correlated relationship between the conceptual nodes and . = 0 means that there is no direct relationship between and .
At time t, for each node , its state can be changed by the following rule:
where is the node state whose value is within the range of [0, 1]. and are parameters used to respectively measure the proportion of influences of the previous states and all the connected nodes, whose values are set as 1 in this paper. is the threshold function that generates the next state of nodes, formulated by the sigmoid function:
where represents the steepness of the function, which is set to 0.5 in this paper. Some initial values are assigned to the nodes, representing the initial states of nodes.
In the FCM model of vaccine hesitancy, the inference process can be triggered as follows: (1) Generating the fuzzy cognitive map, whose weighted adjacent matrix is made by the group decision of experts; (2) initializing the states of nodes, whose values are within the range of [−1, 1] according to concrete scenarios; (3) inferencing the next state of nodes through the rules of (2); and (4) analyzing the results of state transition.
3.2. Model Building
There are two methods to build FCM: the manual building method and the learning-based building method. The former is to use expert knowledge and experience to build a FCM. The latter is to carry out training using sample data to construct a model [59]. Vaccine hesitancy, especially in the context of the COVID-19 pandemic, is a complex problem that involves many areas of knowledge, including medicine, sociology, communication, politics, and the management and distribution of vaccines during the vaccination process. It is more suitable to invite experts from various fields to build FCM based on their knowledge and experience. Accordingly, the FCM of vaccine hesitancy proposed in this paper is based on the first kind of method.
In this section, a double-weighted group decision-making strategy is designed to generate the weights of the fuzzy cognitive map of vaccine hesitancy. Eight experts were invited to take part in the program. Two experts are governmental personnel of the Chinese Center of Disease Control and Prevention, considering their experience in vaccine distribution management; four experts are medical personnel of a public hospital with a 3A-grade certification, owing to their actual vaccination management; two experts are professors who are employed at two well-known public universities specializing in the subject of sociology and communication. The building process comprises four stages as follows:
Step 1. Determine the nodes in the FCM. According to the above matrix of vaccine hesitancy determinants, 24 determinants of vaccine hesitancy serve as all nodes of this vaccine hesitancy FCM, as shown in Table 1. However, most of them are expressed in conceptual explanation. Therefore, the quantitative expression of each factor is defined in this paper, and the questionnaire design is conducted according to the matrix of vaccine hesitancy determinants with concrete descriptions, as provided in the Supplementary Materials section.
Step 2. Determine whether there is a causal relationship between nodes. As the nodes in the FCM of vaccine hesitancy are determined, the next step is to examine whether there is a causal relationship between the nodes. If there is a causal relationship, it is necessary to examine whether the causal relationship is positive or negative. Subsequently, the influence of the causal relationship between nodes should be considered, that is, strong influence, medium influence, or weak influence. Lastly, this paper also considers the degree of certainty of experts in the judgment process, i.e., whether the judgment result given in the questionnaire is certain, generally certain, or not very certain. After the concepts in the matrix of vaccine hesitancy determinants are fully explained to the experts, each of them is required to fulfill a matrix-like form with blanks (the questionnaire we designed). Such a form is named “vaccine hesitancy determinants matrix”, where row indexes denote source nodes and column indexes denote target nodes. Each blank should be filled with three attribute values (corresponding to in (6)), respectively representing the sign of the edge, the weight of the edge, and the certainty to the weight.
Step 3. Evaluate the influence of the causal relationship between nodes. For convenience and efficiency, original decisions of experts are made in natural language. When integrating the decisions, these natural languages are transformed into fuzzy numbers to facilitate computing. The signs of edges should be discussed by the experts again to form a consensus. For each element in the form, all the weight values and certainty degrees filled by experts are considered the weight of the edges, which is calculated using a double weighting strategy. The normalized weight can be calculated using Equation (8).
Definition 1.
Let (D, C, A) represent an information system for multi-attribute group decision making. D is the set of decision makers, where each element is an independent expert denoted as follows:
C is the set of concepts, where each concept in it represents a factor influencing vaccine hesitancy, as expressed by
A is the set of decision matrixes. The decision matrix of the kth expert is formulated by
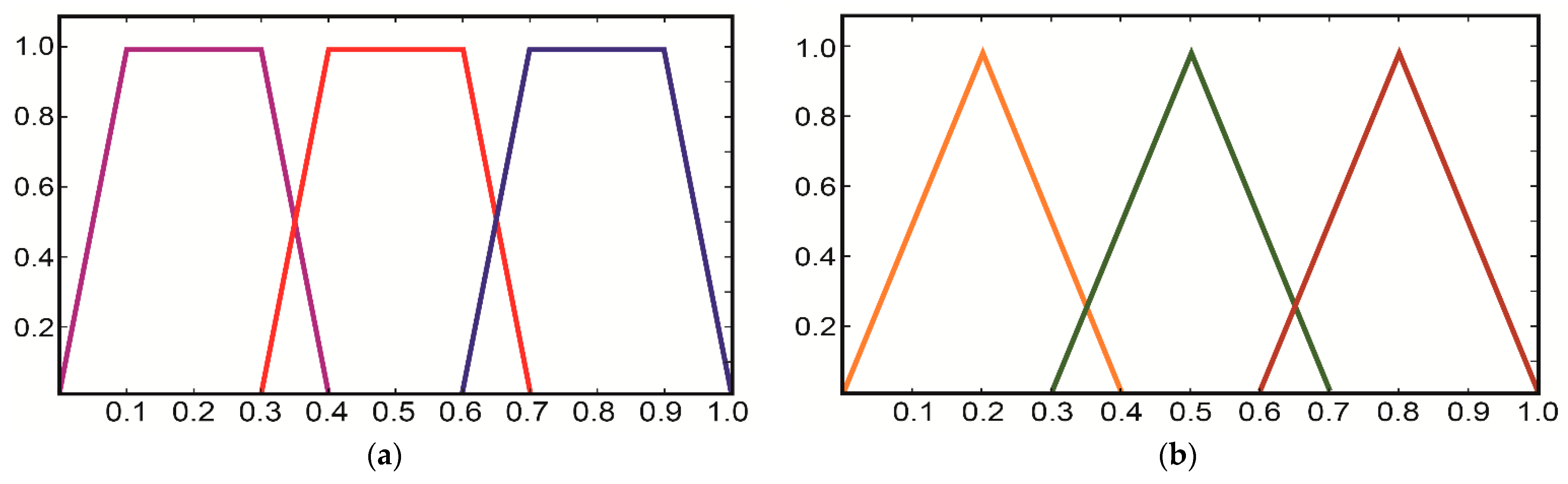
whererepresents the correlation relationship between the two conceptsand,denotes the direction of the correlation betweenand. The sign +1 indicates a positive correlation, and −1 indicates a negative correlation.denotes a trapezoidal fuzzy number, which describes the weight of the relationship.is a triangular fuzzy number describing the degree of certainty of the experts in the decision-making process. The membership functions of the fuzzy numbers are shown inFigure 2.
Definition 2.
Let denote the weight of certainty degree of the kth expert, which is calculated by
Then, the normalized certainty weight for the expert is calculated by
Definition 3.
The weight of edges provided by experts is represented by the trapezoidal fuzzy number , which is the first-level weight. The second-level weightdescribes the certainty degree of the kth expert. The final weight of edges in the FCM is formulated by
where, anddenotes the symbolic function. The defuzzification of fuzzy numbers is implemented by the arithmetic mean.is a threshold function, which assigns 0 to the values less than 0.2.
Step 4. Generating the fuzzy cognitive map. After defuzzification and normalization, the decisions in experts are integrated into a matrix. This matrix is the adjacent matrix of the FCM network.
4. Result
4.1. Network Analysis
The topology characteristics of FCM are shown in Table 2. The network, with 24 nodes and 292 edges, contains a relatively high average clustering coefficient and a short average path length, which conforms to the characteristics of the small-world network. Figure 3 shows the community structure of the network, where blue nodes denote contextual factors, green nodes represent individual and group factors, and orange nodes represent the vaccine as well as vaccination factors. The larger the node size, the higher the degree. From a systemic perspective, there are dense edges among the three groups of factors. As factors in different groups interact and communicate with each other frequently, the states of nodes will quickly change over time.
Degree refers to the number of edges of one node in the network. A higher degree value of a node indicates that it is closer to the center of the network and has a wider range of influence. In a directed network, the degree equals the sum of the in-degree and out-degree, the relationship between which in the FCM network is shown in Figure 4. Some observations are as follows:
- (1)
- Degree analysis. C19 (mode of administration) and C8 (politics/policies) are the top two nodes with the highest degree value, both of which are macro-factors with obvious social and political attributes. In contrast, nodes with smaller degree values have obvious personal and environmental attributes, including C6 (gender structure), C5 (age structure), and C9 (geographic barriers), indicating that these factors are not easily influenced by the nodes in the network.
- (2)
- Out-degree analysis. Remarkably, that the outdegree of the nodes C2 (opinion leaders), C19 (mode of administration), C8 (politics/policies), C1 (communication and media environment), and C7 (socio-economic) occupies more than 50% of their degrees in total. These factors strongly correlate with other factors in the network and a stronger ability to influence others.
- (3)
- In-degree analysis. The node with the highest in-degree value is C17 (realistic level risk-return ratio), followed by C14 (trust in the healthcare system), C16 (social norm perception), C20 (level of mobilization for vaccination), and C24 (the strength of medical staff’s recommendation). The in-degree of these nodes exceeds 50% of the degree value, illustrating that the public perception of the risks of vaccination, social perception, and trust in the medical system will be influenced by multiple factors.
Betweenness centrality and closeness centrality are another two major metrics for measuring the influence of nodes. As is shown in Table 3, (1) the node with the highest value of intermediary centrality is C19 (mode of administration). Betweenness centrality measurement of centrality of one node is based on shortest paths, which illustrates that the administration mode has a strong ability to affect the social, economic, media, historical, religious, and medical factors; meanwhile, a well-established administrative system is an indispensable bridge for the effective implementation of the COVID-19 vaccination program. (2) C6 (gender structure) is the node with the smallest closeness centrality in the entire network. The closeness centrality is focused on the average distance between a node and all other nodes in the network. The smaller the closeness centrality, the more central the node location.
Studies have shown that during the vaccination process, women, middle-aged and young adults, and high-income people perceived a low risk of infection and showed higher hesitancy to take the COVID-19 vaccine [62]. This result reminds us that, when formulating policies to mitigate COVID-19 vaccine hesitancy, gender and target population are important reference factors. Except for the target population, hierarchical development by gender, age, and other demographic characteristics should be considered in the scientific study in relation to COVID-19 vaccines, so as to generate the best prevention and mitigation measures for vaccine hesitancy.
4.2. Simulations on Three Scenarios
The inference process of FCM can be considered as a process of answering some questions. In FCM, the initial state of the nodes is equivalent to posing the following question: if the event occurs, what will be the result? The output is the answer to the question. The experiments in this subsection aim to identify the key factors affecting vaccine hesitancy. Therefore, three experimental scenarios were set to explore the key or sensitive factors under different conditions, including the government scenario, the propaganda scenario, and the medical scenario. The three scenarios are introduced in the following.
Government scenario: simulating the relevant administrative agencies such as local governments and centers for disease control and prevention, etc. This scenario is focused on the relevant factors referring to vaccination and vaccination programs, involving the following factors: C8 (politics/policies), C19 (mode of administration), C20 (level of mobilization for vaccination), and C22 (vaccination planning).
Propaganda scenario: Simulating the propaganda organizations engaged in propaganda activities, such as state propaganda agencies, newspapers, radio and TV stations, social media, etc. This scenario is focused on the propaganda effect of the relevant information, involving the following factors: C1 (communication and media environment), C2 (opinion leaders), and C18 (popularity of vaccine science).
Medical scenario: Simulating the medical and health institutions or staff providing healthcare or medical service to the public, such as physicians, pharmacists, examiners, nurse practitioners, etc. These entities may affect the effectiveness of vaccination programs. The scenario factors involve C10 (perception of the pharmaceutical industry), C14 (trust in the healthcare system), C21 (reliability of vaccination), and C24 (the strength of the medical staff’s recommendation).
To fully observe the FCM inference results, we set three levels of parameters: low (0.2), medium (0.5), and high (0.8). Only the factor values under the corresponding scenarios are changed. For most factors, a higher state value means a lower vaccine hesitancy, except for C15 (risk–benefit ratio at cognitive level) and C17 (risk–benefit ratio at realistic level). Furthermore, to compare the steady state of the system under different scenarios, a baseline scenario was constructed by simply assigning all factors as 0.1. The simulation results of the baseline scenario show that after four iterations of FCM inference, the interactions among the factors reach a steady state.
4.3. Experiment Result Analysis
The experimental results in the three scenarios are shown in Figure 5. The x-axis represents the conceptual factors, excluding the factors belonging to the corresponding scenario. The y-axis records the changing rate of the steady-state values of factors under the corresponding scenario to the values under the baseline scenario.
- (1)
- Government scenario
Factors of the government scenario have a relatively weak effect on other factors. Compared to the baseline scenario, when the factors of the government scenario are assigned with high-level values (factor values = 0.8), the most significantly affected factors are C3 (historical influences), reaching a steady state increased by 0.83%, and C4 (religion/culture), increasing by 0.74%. When assigned with low-level values (factor values = 0.2), the steady-state value of C3 increases by 0.18%, and that of C4 increases by 0.16%. Comparing the two situations, C3 obtains an improvement of 0.65% in high-level settings than that in low-level settings. C15 (risk–reward ratio at the cognitive level) obtains a reduction of 0.20% in the high-level settings and a reduction of 0.05% in poor conditions compared to the baseline scenario. The value of C17 (realistic level risk–benefit ratio) obtains a reduction of 0.05% in the high-level setting compared to the baseline scenario, and a reduction of 0.01% in the low-level setting. This illustrates that as the factors of the government scenario are strengthened, public awareness of the risks of vaccination becomes clearer, and the risk–benefit ratio gradually decreases.
- (2)
- Propaganda scenario
The relevant factors in the propaganda scenario have a significant effect on public sentiment towards vaccination. When in the propaganda scenario with the high-level setting (factor values = 0.8), the steady-state value of C23 (vaccination costs) increases by 1.04% compared with that of the baseline scenario. The second is C3 (historical influences), with an increase of 1.26%. Under the low-level setting (factor values = 0.2), an increase of 0.22% is still obtained in the steady state of C23 (vaccination costs). Compared to the government scenario, the propaganda scenario has a greater impact on C15 (risk–benefit ratio at the cognitive level). Compared to the baseline condition, the steady state of C17 (risk–benefit ratio at the realistic level) decreases by 0.04% in the high-level setting and 0.01% in the low-level setting. These results suggest that disseminating information about vaccines can reduce public vaccine hesitancy to some extent.
- (3)
- Medical scenario
The relevant factors of the medical scenario show a wide influence on other factors. In the high-level setting (factor values = 0.8), the steady-state values of C3 (historical influences), C4 (religion/culture), C5 (age structure), C7 (socio-economic), C13 (education level), C9 (mode of administration), and C23 (vaccination costs) reach an increase of 0.57%, 0.45%, 0.23%, 0.18%, 0.18%, 0.19%, and 0.6%, respectively. In comparison, the steady-state value of C15 (risk–benefit ratio at the cognitive level) and C17 (risk–benefit ratio at the realistic level) decrease by 0.12% and 0.03%, respectively. In the low-level setting, the value of C3, C4, and C23 is increased by 0.11%, 0.09%, and 0.12% respectively; C5, C7, C9, and C13 show the same increase of 0.04%; the values of C15 and C17 decrease by 0.04% and 0.13%, respectively. These results show that, compared with government scenarios and propaganda scenarios, the relevant factors in medical scenarios have a wider scope of influence, which may influence not only some practical factors such as vaccination costs, but also some objective factors such as age, socioeconomic, geographic barriers, and education level.
In conclusion, the common sensitive factors of the three experimental scenarios are C3 (historical influences), C4 (religion/culture), C23 (vaccination costs), C15 (risk–benefit ratio at the cognitive level), and C17 (risk–benefit ratio at the realistic level). That is, when the scenario factors change, these five factors show a larger range of fluctuations than the others. Specifically, C3 (historical influences), C4 (religion/culture), and C23 (vaccination costs) show positive responses, while C15 (risk–benefit ratio at the cognitive level) and C17 (risk–benefit ratio at the realistic level) show negative responses.
5. Application Case
An application case is demonstrated in this section to show how the FCM of vaccine hesitancy is used in realistic situations. The initial value of nodes has been assigned based on the survey results provided by Liu et al. [63], who conducted a cross-national survey to assess vaccine preferences and potential factors for vaccine acceptance in China and the United States. The reasons for choosing these results have two aspects: the conceptual factors for vaccine hesitancy in their survey are the same as those of FCM, and the Propensity Score Matching (PSM) fits well with the questions on group decision in this paper. Of note, the study of Liu et al. was based on partial population samples in the two countries; whether their study reflects the overall situations is not the subject of this paper. The purpose of this subsection is to provide a visible reference of how the FCM model of vaccine hesitancy is applied to realistic situations.
According to the investigation results, we set the initial state value of the 24 factors of FCM, whose results are shown in Table 4. With the inference of FCM, factors of both China and the United States reach a stable state after six iterations. Overall, the vaccine/vaccination factors and the individual/group factors are changed more significantly than the contextual factors. To observe the inference process more precisely, simulation experiments based on the government, propaganda, and medical scenarios were conducted, so as to help observe the key or sensitive factors.
In the simulation setting of China, the sensitive factors in the three scenarios are C15 (risk–benefit ratio at the cognitive level) and C17 (risk–benefit ratio at the realistic level), which have the largest fluctuation range. Figure 6a shows that the sensitive factors in the government scenario are C21 (reliability of vaccination), C22 (vaccination planning), and C23 (vaccination costs). The most sensitive factor in the propaganda scenario is C22 (vaccination planning). In medical scenarios, the sensitive factors are C11 (vaccine experience), C18 (popularity of vaccine science), and C23 (vaccination costs). To conclude, the public attitude to vaccination is closely related to political policies, media, and medical environment; science cognition is the key to the successful implementation of vaccination programs.
In the simulation setting of the US, C15 (risk–benefit ratio at the cognitive level) and C17 (risk–benefit ratio at the realistic level) are two common sensitive factors in all the three scenarios. Figure 6b shows that the sensitive factors in the government and propaganda scenarios are C18 (popularity of vaccine science) and C21 (reliability of vaccination), and those in the medical scenarios are C11 (vaccine experience) and C19 (administrative style). This illustrates that public trust in the government and medical systems is crucial in weakening vaccine hesitancy.
Furthermore, experimental results show that C15 (risk–benefit ratio at the cognitive level) and C17 (risk–benefit ratio at the realistic level) are common sensitive factors. In the simulation settings of China, the changes of C11 (vaccine experience) and C22 (vaccination planning) are significant. In the simulation settings of the United States, the change of C21 (reliability of vaccination) is significant. The differences may lie in cultural and political aspects. People in China may be more concerned about the convenience and experience of vaccine injection, while those in the US may focus more on vaccine industry chains and the safety of vaccine infection.
6. Discussion
Incorporating the FCM inference technique, a variety of experiments were conducted to test the common and sensitive factors for vaccine hesitancy in three different scenarios. Some findings deserve further discussion.
(1) Microscopic, embodied factors impact vaccine hesitancy more than macroscopic abstract factors. Specifically, compared to the macroscopic factors (C8, C19, and C20), the microscopic factors (C21, C23, and C24) affect public behavior and attitude more. A reasonable explanation concerning the macroscopic factors is that people can intuitively perceive the risks and benefits based on microscopic factors and make further judgements. The introspection of the massive propaganda about vaccine safety and efficacy is dominated by governmental agencies and is insufficient to eliminate vaccine hesitancy. It also reflects the gap between official perception and public perception. Therefore, it is imperative to take some other measures to decrease the temporal, spatial, social, and psychological distance between the information senders and the receivers.
(2) The factor “Mode of administration” is a core factor in vaccine hesitancy. The COVID-19 pandemic poses new challenges to the administration modes in global areas and countries, including how to establish an effective infectious disease prevention and control system on the premise of economic development, and how to upgrade the traditional vaccination system based on digital techniques. It has been found, quite interestingly, though the China and the United States have quite different mode of administration, there is still a consensus in both countries: protecting the rights and interests of minority groups, though China pays more attention to the digital dilemma brought by technological development, while in the United States, racial equality and religious faith have gained more attention.
(3) There are some common sensitive factors in vaccine hesitancy in the government, propaganda, and medical scenarios. Experimental results show that C3 (historical influence), C4 (religion/culture), C15 (risk–reward ratio at the cognitive level), and C17 (risk–reward ratio at the realistic level) are common sensitive factors in all the three scenarios. This illustrates that a comprehensive effort contributes to a high vaccination rate. Individually, it is imperative to understand that though some persons are reluctant, targeted material assistance or spiritual care can be effective. Massive, diversified propaganda strategies can help improve the crowd vaccination rate. In addition, a vaccine supply chain conducted on a digital system may increase the sense of security.
(4) Sensitive factors identified in different scenarios (government, propaganda, medicine) are different. Experiments show that most sensitive factors in government and propaganda scenarios belong to contextual and individual/group factors. Sensitive factors in medical scenarios are diversified. For example, C7 (socio-economic), C8 (political/policy), C9 (geographical barriers), and C23 (vaccination costs) are not easily affected by other factors. However, these factors are more easily changed in the medical scenarios. Therefore, the characteristics of specific scenarios should be considered in popularizing the vaccination program. When in developing regions, the direct and effective measures may be reducing the vaccination cost and increasing vaccine accessibility. In developed regions, it may be helpful to reduce the vaccine hesitancy caused by misinformation.
7. Conclusions
In this paper, the nonlinear correlations within factors of vaccine hesitancy have been quantified by incorporating fuzzy cognitive inference. A double-weighted group decision-making method was firstly designed to integrate the independence of experts’ decision-making and the opinions given by the expert group. Secondly, a FCM inference process was built to determine key factors in different scenarios, respectively the government, the propaganda, and the medical scenario. This paper enriches approaches of vaccine hesitancy estimation for the post-pandemic global recovery.
Table 5 lists the details about the concepts of this paper.
Supplementary Materials
The following supporting information can be downloaded at: https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/su14148434/s1, Table S1: Factors for vaccine hesitancy in the vaccine hesitancy determinants matrix.
Author Contributions
Data curation, X.-K.W. and K.-S.L.; Project administration, J.-S.Z.; Supervision, T.-F.Z.; Validation, W.-N.C.; Writing—original draft, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Self-Funded Project of the Academy of Chinese National Cohesion Research of Jinan University (No. JDGTT202209).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Institutional Review Board of Social Sciences and Humanities, Jinan University (protocol code IRB No. A2202001-022 and 2 February 2022 of approval) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to restrictions eg privacy or ethical. 1. The data presented in this study are available on request from the corresponding author [[email protected]]. The data are not publicly available due to [The data of the experimental cases in this paper involve the respondents’ questionnaires, according to the respondents’ expressed willingness to keep confidentiality]. 3rd Party Data: 2. Application Case Restrictions apply to the availability of these data in this study. Data was obtained from ref. [63] and are available [Email of the corresponding author published in this article: [email protected]] with the permission of [Wai-Kit Ming].
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2022. Available online: https://covid19.who.int/ (accessed on 1 May 2022).
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, D. Instructing durable humoral immunity for COVID-19 and other vaccinable diseases. Immunity 2022, 55, 945–964. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Mateus, J.; Coelho, C.H.; Dan, J.M.; Moderbacher, C.R.; Gálvez, R.I.; Cortes, F.H.; Grifoni, A.; Tarke, A.; Chang, J.; et al. Humoral and cellular immune memory to four COVID-19 vaccines. Cell, 2022, in press. [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA Vaccine against SARS-CoV-2—Preliminary Report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.B.; Kanevsky, I.; Che, Y.; Swanson, K.A.; Muik, A.; Vormehr, M.; Kranz, L.M.; Walzer, K.C.; Hein, S.; Güler, A.; et al. BNT162b vaccines protect rhesus macaques from SARS-CoV-2. Nature 2021, 592, 283–289. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Burki, T.K. Omicron variant and booster COVID-19 vaccines. Lancet Respir. Med. 2022, 10, e17. [Google Scholar] [CrossRef]
- Kurhade, C.; Zou, J.; Xia, H.; Cai, H.; Yang, Q.; Cutler, M.; Cooper, D.; Muik, A.; Jansen, K.U.; Xie, X.; et al. Neutralization of Omicron BA.1, BA.2, and BA.3 SARS-CoV-2 by 3 doses of BNT162b2 vaccine. Nat. Commun. 2022, 13, 3602. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484. [Google Scholar] [CrossRef]
- Kaku, C.I.; Bergeron, A.J.; Ahlm, C.; Normark, J.; Sakharkar, M.; Forsell, M.N.E.; Walker, L.M. Recall of pre-existing cross-reactive B cell memory following Omicron BA.1 breakthrough infection. Sci. Immunol. 2022. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Wong, E.L.Y.; Cheung, A.W.L.; Huang, J.; Lai, C.K.C.; Yeoh, E.K.; Chan, P.K.S. COVID-19 Vaccine Hesitancy in a City with Free Choice and Sufficient Doses. Vaccines 2021, 9, 1250. [Google Scholar] [CrossRef] [PubMed]
- Campos-Mercade, P.; Meier, A.N.; Schneider, F.H.; Meier, S.; Pope, D.; Wengström, E. Monetary incentives increase COVID-19 vaccinations. Science (1979) 2021, 374, 879–882. [Google Scholar] [CrossRef]
- Sturgis, P.; Brunton-Smith, I.; Jackson, J. Trust in science, social consensus and vaccine confidence. Nat. Hum. Behav. 2021, 5, 1528–1534. [Google Scholar] [CrossRef]
- Ergur, A. Social causes of vaccine rejection-vaccine indecision attitudes in the context of criticisms of modernity. Eurasian J. Med. 2020, 52, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.K.; Zhao, T.-F.; Chen, W.-N.; Zhang, J. Toward predicting active participants in tweet streams: A case study on two civil rights events. IEEE Trans. Knowl. Data Eng. 2020. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef]
- Buonsenso, D.; Valentini, P.; Macchi, M.; Folino, F.; Pensabene, C.; Patria, M.F.; Agostoni, C.; Castaldi, S.; Lecce, M.; Lorella, M.; et al. Caregivers’ Attitudes Toward COVID-19 Vaccination in Children and Adolescents with a History of SARS-CoV-2 Infection. Front. Pediatr. 2022, 7, 867968. [Google Scholar] [CrossRef]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 Vaccine Hesitancy among Parents of Children and Adolescents Living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef]
- Smith, L.E.; Carter, B. Parental preferences for a mandatory vaccination scheme in England: A discrete choice experiment. Lancet Reg. Health Eur. 2022, 16, 100359. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.; MacDonald, N.E.; Guirguis, S. Health communication and vaccine hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrich, M.J. WHO’s top health threats for 2019. JAMA 2019, 321, 1041. [Google Scholar] [CrossRef]
- Wagner, C.E.; Saad-Roy, C.M.; Morris, S.E.; Baker, R.E.; Mina, M.J.; Farrar, J.; Holmes, E.C.; Pybus, O.G.; Graham, A.L.; Emanuel, E.J.; et al. Vaccine nationalism and the dynamics and control of SARS-CoV-2. Medrxiv 2021, 373, 7364. [Google Scholar] [CrossRef] [PubMed]
- Brzezinski, A.; Kecht, V.; van Dijcke, D.; Wright, A.L. Science skepticism reduced compliance with COVID-19 shelter-in-place policies in the United States. Nat. Hum. Behav. 2021, 5, 1519–1527. [Google Scholar] [CrossRef] [PubMed]
- Attwell, K.; Smith, D.T. Parenting as politics: Social identity theory and vaccine hesitant communities. Int. J. Health Gov. 2017, 22, 183–198. [Google Scholar] [CrossRef]
- Bartoš, V.; Bauer, M.; Cahlíková, J.; Chytilová, J. Communicating doctors’ consensus persistently increases COVID-19 vaccinations. Nature 2022, 606, 542–549. [Google Scholar] [CrossRef]
- de Figueiredo, A.; Larson, H.J. Exploratory study of the global intent to accept COVID-19 vaccinations. Commun. Med. 2021, 1, 30. [Google Scholar] [CrossRef]
- Kogan, N.E.; Clemente, L.; Liautaud, P.; Kaashoek, J.; Link, N.B.; Nguyen, A.T.; Lu, F.S.; Huybers, P.; Resch, B.; Havas, C.; et al. An early warning approach to monitor COVID-19 activity with multiple digital traces in near real time. Sci. Adv. 2021, 7, eabd6989. [Google Scholar] [CrossRef]
- Zhang, J.; Litvinova, M.; Liang, Y.; Zheng, W.; Shi, H.; Vespignani, A.; Viboud, C.; Ajelli, M.; Yu, H. The impact of relaxing interventions on human contact patterns and SARS-CoV-2 transmission in China. Sci. Adv. 2021, 7, eabe2584. [Google Scholar] [CrossRef]
- Monod, M.; Blenkinsop, A.; Xi, X.; Hebert, D.; Bershan, S.; Tietze, S.; Baguelin, M.; Bradley, V.C.; Chen, Y.; Coupland, H.; et al. Age groups that sustain resurging COVID-19 epidemics in the United States. Science (1979) 2021, 371, eabe8372. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Marcus, J.L.; Buckee, C.; Smith, T.C. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission dynamics should inform policy. Clin. Infect. Dis. 2021, 73, S170–S176. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Gagnon, D.; MacDonald, N.; Bocquier, A.; Peretti-Watel, P.; Verger, P. Underlying factors impacting vaccine hesitancy in high income countries: A review of qualitative studies. Expert Rev. Vaccines 2018, 17, 989–1004. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.-K.; Zhao, T.-F.; Lu, L.; Chen, W.-N. Predicting the Hate: A GSTM Model based on COVID-19 Hate Speech Datasets. Inf. Processing Manag. 2022, 59, 102998. [Google Scholar] [CrossRef]
- Zhao, T.-F.; Chen, W.-N.; Kwong, S.; Gu, T.-L.; Yuan, H.-Q.; Zhang, J.; Zhang, J. Evolutionary divide-and-conquer algorithm for virus spreading control over networks. IEEE Trans. Cybern. 2020, 51, 3752–3766. [Google Scholar] [CrossRef]
- Zhao, T.-F.; Chen, W.-N.; Liew, A.W.-C.; Gu, T.; Wu, X.-K.; Zhang, J. A binary particle swarm optimizer with priority planning and hierarchical learning for networked epidemic control. IEEE Trans. Syst. Man Cybern. Syst. 2019, 51, 5090–5104. [Google Scholar] [CrossRef] [Green Version]
- Onari, M.A.; Yousefi, S.; Rabieepour, M.; Alizadeh, A.; Rezaee, M.J. A medical decision support system for predicting the severity level of COVID-19. Complex Intell. Syst. 2021, 7, 2037–72051. [Google Scholar] [CrossRef]
- Jørgensen, F.J.; Bor, A.; Petersen, M.B. Compliance without fear: Individual-level protective behaviour during the first wave of the COVID-19 pandemic. Br. J. Health Psychol. 2021, 26, 679–696. [Google Scholar] [CrossRef]
- Ramalingam, S.; Govindan, K.; Broumi, S. Analysis of Covid-19 via Fuzzy Cognitive Maps and Neutrosophic Cognitive Maps. Neutrosophic Sets Syst. 2021, 42, 102–116. [Google Scholar]
- Bloom, D.E.; Canning, D.; Sevilla, J. The effect of health on economic growth: A production function approach. World Dev. 2004, 32, 1–13. [Google Scholar] [CrossRef]
- Sobkow, A.; Zaleskiewicz, T.; Petrova, D.; Garcia-Retamero, R.; Traczyk, J. Worry, risk perception, and controllability predict intentions toward COVID-19 preventive behaviors. Front. Psychol. 2020, 11, 582720. [Google Scholar] [CrossRef] [PubMed]
- Groumpos, P.P. Why Modelling the COVID-19 pandemic using Fuzzy Cognitive Maps (FCM)? IFAC-PapersOnLine 2021, 54, 305–310. [Google Scholar] [CrossRef]
- Groumpos, P. Modelling COVID-19 using Fuzzy Cognitive Maps (FCM). EAI Endorsed Trans. Bioeng. Bioinform. 2021, 1, 168728. [Google Scholar] [CrossRef]
- Amirkhani, A.; Kolahdoozi, M.; Wang, C.; Kurgan, L.A. Prediction of DNA-binding residues in local segments of protein sequences with Fuzzy Cognitive Maps. IEEE/ACM Trans. Comput. Biol. Bioinform. 2018, 17, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Papakostas, G.A.; Boutalis, Y.S.; Koulouriotis, D.E.; Mertzios, B.G. Fuzzy cognitive maps for pattern recognition applications. Int. J. Pattern Recognit. Artif. Intell. 2008, 22, 1461–1486. [Google Scholar] [CrossRef]
- Subramanian, K.; Suresh, S.; Sundararajan, N. A metacognitive neuro-fuzzy inference system (McFIS) for sequential classification problems. IEEE Trans. Fuzzy Syst. 2013, 21, 1080–1095. [Google Scholar] [CrossRef]
- Amirkhani, A.; Papageorgiou, E.I.; Mohseni, A.; Mosavi, M.R. A review of fuzzy cognitive maps in medicine: Taxonomy, methods, and applications. Comput. Methods Programs Biomed. 2017, 142, 129–145. [Google Scholar] [CrossRef]
- Georgopoulos, V.C.; Malandraki, G.A.; Stylios, C.D. A fuzzy cognitive map approach to differential diagnosis of specific language impairment. Artif. Intell. Med. 2003, 29, 261–278. [Google Scholar] [CrossRef]
- Kosko, B. Fuzzy systems as universal approximators. IEEE Trans. Comput. 1994, 43, 1329–1333. [Google Scholar] [CrossRef]
- Miao, Y.; Liu, Z.-Q. On Causal Inference in Fuzzy Cognitive Maps. IEEE Trans. Fuzzy Syst. 2000, 8, 107–119. [Google Scholar] [CrossRef]
- Ruhe, G. Hybrid intelligence in software release planning. Int. J. Hybrid Intell. Syst. 2004, 1, 99–110. [Google Scholar] [CrossRef]
- Sallam, M. Covid-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Vena-Oya, J.; García-Castañeda, J.A.; Rodríguez-Molina, M.Á. Forecasting a post-COVID-19 economic crisis using fuzzy cognitive maps: A Spanish tourism-sector perspective. Curr. Issues Tour. 2021, 1–15. [Google Scholar] [CrossRef]
- Bamakan, S.M.H.; Malekinejad, P.; Ziaeian, M.; Motavali, A. Bullwhip effect reduction map for COVID-19 vaccine supply chain. Sustain. Oper. Comput. 2021, 2, 139–148. [Google Scholar] [CrossRef]
- Reyna, V.F.; Broniatowski, D.A.; Edelson, S.M. Viruses, Vaccines, and COVID-19: Explaining and Improving Risky Decision-making. J. Appl. Res. Mem. Cogn. 2021, 10, 491–509. [Google Scholar] [CrossRef]
- Felix, G.; Nápoles, G.; Falcon, R.; Froelich, W.; Vanhoof, K.; Bello, R. A review on methods and software for fuzzy cognitive maps. Artif. Intell. Rev. 2019, 52, 1707–1737. [Google Scholar] [CrossRef]
- Kosko, B. Fuzzy cognitive maps. Int. J. Man-Mach. Stud. 1986, 24, 64–75. [Google Scholar] [CrossRef]
- Papageorgiou, E.I.; Salmeron, J.L. A review of fuzzy cognitive maps research during the last decade. IEEE Trans. Fuzzy Syst. 2013, 21, 66–79. [Google Scholar] [CrossRef]
- Zadeh, L.A. Fuzzy Logic. Computer 1988, 21, 83–93. [Google Scholar] [CrossRef]
- Toan, T.D.; Wong, Y.D. Fuzzy logic-based methodology for quantification of traffic congestion. Phys. A Stat. Mech. Its Appl. 2021, 570, 125784. [Google Scholar] [CrossRef]
- Zhao, Y.-M.; Liu, L.; Sun, J.; Yan, W.; Yuan, K.; Zheng, Y.-B.; Lu, Z.-A.; Liu, L.; Ni, S.-Y.; Su, S.-Z.; et al. Public willingness and determinants of COVID-19 vaccination at the initial stage of mass vaccination in China. Vaccines 2021, 9, 1172. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; He, Z.; Huang, J.; Yan, N.; Chen, Q.; Huang, F.; Zhang, Y.; Akinwunmi, O.; Akinwunmi, B.; Zhang, C.; et al. A comparison of vaccine hesitancy of COVID-19 vaccination in China and the United States. Vaccines 2021, 9, 649. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, B.; Jha, R.M. Soft Computing Techniques. In Soft Computing in Electromagnetics; Cambridge University Press: Cambridge, UK, 2016; pp. 9–44. [Google Scholar] [CrossRef]
- Novák, V.; Perfilieva, I.; Močkoř, J. Mathematical Principles of Fuzzy Logic; Springer: New York, NY, USA, 1999. [Google Scholar] [CrossRef]
- Dijkman, J.G.; van Haeringen, H.; de Lange, S.J. Fuzzy Numbers. J. Math. Anal. Appl. 1983, 92, 301–341. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
A case of fuzzy cognitive map.

Figure 2.
Membership function of linguistic variables. (a) For ; (b) For .

Figure 3.
The illustration of the FCM network.

Figure 4.
Chord chart of the FCM network.

Figure 5.
Experiment results. (a) Government scenario; (b) Propaganda scenario; (c) Medical scenario.
Figure 5.
Experiment results. (a) Government scenario; (b) Propaganda scenario; (c) Medical scenario.


Figure 6.
Analysis of sensitive Factors between China and the United States. (a) Sensitive factors in the China environment propaganda; (b) Sensitive factors in the US environment propaganda.
Figure 6.
Analysis of sensitive Factors between China and the United States. (a) Sensitive factors in the China environment propaganda; (b) Sensitive factors in the US environment propaganda.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Factors for vaccine hesitancy in the vaccine hesitancy determinants matrix.
| Factors |
|---|
| Contextual factors |
| C1 Communication and media environment |
| C2 Opinion leader |
| C3 Historical influences |
| C4 Religion/culture |
| C5 Age structure |
| C6 Gender structure |
| C7 Socio-economic |
| C8 Politics/policies |
| C9 Geographic barriers |
| C10 Perception of the pharmaceutical industry |
| Individual and group factors |
| C11 Vaccine experience |
| C12 Healthy attitude |
| C13 Education level |
| C14 Trust in the healthcare system |
| C15 Risk–benefit ratio at cognitive level |
| C16 Social norms perception |
| Vaccine and vaccination factors |
| C17 Risk–benefit ratio at realistic level |
| C18 Popularity of vaccine science |
| C19 Mode of administration |
| C20 Level of mobilization for vaccination |
| C21 Reliability of vaccination |
| C22 Vaccination planning |
| C23 Vaccination costs |
| C24 The strength of the medical staff’s recommendation |
Table 2.
Topology characteristics of the FCM.
| Name | Value |
|---|---|
| Node | 24 |
| Edge | 292 |
| Network diameter | 4 |
| Network density | 0.529 |
| Average clustering coefficient | 0.663 |
| Average path length | 1.514 |
Table 3.
Node centrality analysis of the FCM network.
| Node | Degree | Node | In-Degree | Node | Out-Degree | Node | Betweenness Centrality | Node | Closeness Centrality |
|---|---|---|---|---|---|---|---|---|---|
| C19 | 335 | C17 | 19 | C2 | 20 | C19 | 42.72 | C6 | 0.42 |
| C8 | 34 | C16 | 18 | C19 | 18 | C12 | 35.42 | C23 | 0.49 |
| C16 | 33 | C20 | 18 | C8 | 17 | C2 | 30.71 | C5 | 0.52 |
| C20 | 33 | C14 | 18 | C1 | 15 | C22 | 30.51 | C9 | 0.52 |
| C14 | 32 | C24 | 18 | C7 | 15 | C20 | 23.54 | C3 | 0.59 |
Table 4.
Case analysis model factor parameters.
| Factors | Parameters |
|---|---|
| C1 Communication and media environment | 0.575 |
| C2 Opinion leader | 0.65 |
| C3 Historical influences | 0.2 |
| C4 Religion/culture | 0.365 |
| C5 Age structure | 0.95 |
| C6 Gender structure | 0.45 |
| C7 Socio-economic | 0.605 |
| C8 Politics/policies | 0.75 |
| C9 Geographic barriers | 0.1 |
| C10 Perception of the pharmaceutical industry | 0.65 |
| C11 Vaccine experience | 0.8 |
| C12 Healthy attitude | 0.655 |
| C13 Education level | 0.5 |
| C14 Trust in the healthcare system | 0.44 |
| C15 Risk–reward ratio at the cognitive level | 0.645 |
| C16 Social norm perception | 0.225 |
| C17 Realistic level risk–return ratio | 0.155 |
| C18 Popularity of vaccine science | 0.25 |
| C19 Mode of administration | 0.8 |
| C20 Level of mobilization for vaccination | 0.605 |
| C21 Reliability of vaccination | 0.505 |
| C22 Vaccination planning | 0.7 |
| C23 Vaccination costs | 0.295 |
| C24 The strength of the medical staff’s recommendation | 0.4 |
Table 5.
List of Concepts.
| Soft computing | A set of computing techniques based on artificial intelligence (human-like decision making) and natural selection [64]. |
| Fuzzy logic | A form of many-valued logic in which the truth value of variables may be any real number between [0, 1] or [−1, +1] [65]. |
| Fuzzy numbers | A fuzzy number is a generalization of a regular, real number in the sense that it does not refer to one single value, but rather to a connected set of possible values, where each possible value has its own weight between 0 and 1 [66]. |
| Fuzzy cognitive mapping (FCM) | A map-based knowledge representation method, with nodes representing concepts, and edges representing causal relationships among concepts [58]. |
| Vaccine hesitancy | The delay in acceptance or refusal of vaccines despite availability of vaccine service [18]. |
| Group decision making | A method to achieve more effective and optimized solutions by integrating the opinions of committees, teams, small groups, partnerships, or other collaborative social processes. |
| Contextual factors | The factors influencing vaccine hesitancy [18]. |
| Individual and group factors | The influence of individual, group, social, peer environment, and other factors on vaccine hesitancy [18]. |
| Vaccine and vaccination Factors | Factors directly related to vaccines or directly related to vaccination [18]. |
| Vaccine hesitancy determinants matrix | A matrix describing the crucial factors in vaccine hesitancy conceptually, proposed by the WHO SAGE Working Group [18]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sun, K.; Zhao, T.-F.; Wu, X.-K.; Lai, K.-S.; Chen, W.-N.; Zhang, J.-S. Incorporating Fuzzy Cognitive Inference for Vaccine Hesitancy Measuring. Sustainability 2022, 14, 8434. https://0-doi-org.brum.beds.ac.uk/10.3390/su14148434
AMA Style
Sun K, Zhao T-F, Wu X-K, Lai K-S, Chen W-N, Zhang J-S. Incorporating Fuzzy Cognitive Inference for Vaccine Hesitancy Measuring. Sustainability. 2022; 14(14):8434. https://0-doi-org.brum.beds.ac.uk/10.3390/su14148434
Chicago/Turabian StyleSun, Kun, Tian-Fang Zhao, Xiao-Kun Wu, Kai-Sheng Lai, Wei-Neng Chen, and Jin-Sheng Zhang. 2022. "Incorporating Fuzzy Cognitive Inference for Vaccine Hesitancy Measuring" Sustainability 14, no. 14: 8434. https://0-doi-org.brum.beds.ac.uk/10.3390/su14148434
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.