
Virtual Reality and Metacognition Training Techniques for Learning Disabilities


1
Net Media Lab & Mind & Brain R&D, N.C.S.R. ‘Demokritos’, 153 41 Agia Paraskevi, Greece
2
Communication Systems Engineering Department, University of the Aegean, 811 00 Mitilini, Greece
*
Author to whom correspondence should be addressed.
Sustainability 2022, 14(16), 10170; https://0-doi-org.brum.beds.ac.uk/10.3390/su141610170
Submission received: 28 July 2022
/
Revised: 8 August 2022
/
Accepted: 13 August 2022
/
Published: 16 August 2022
(This article belongs to the Special Issue Digital Technologies for Sustainable Education)
Abstract
:The current research aims to investigate the effectiveness of brain-rewiring techniques applied in virtual reality environments as a pioneer intervention for people with learning disabilities and various disorders. In addition, we examine whether these VR-assisted techniques can improve metacognitive skills. Specifically, we emphasize the advantage of VR clinical hypnosis, VR neurolinguistic programming, VR subliminal training, VR fast learning, VR mindfulness, and VR breathing training. The results of this review study revealed that virtual reality provides a fertile ground for the practice of therapeutic metacognitive techniques. In addition, experimental research revealed beneficial effects on learning disabilities, cognitive impairments, autism, ADHD (attention deficit hyperactivity disorder), depression, generalized anxiety disorder, phobias, and behavioral and emotional disorders. It was revealed that VR brain-rewiring techniques constitute effective metacognitive strategies for people with various disorders. Therapists, educators, parents, and even patients could utilize VR brain-rewiring techniques at home, at school, or in the workplace to train the 21st-century meta-abilities. This study also highlights the need to create virtual metacognitive training environments to accelerate inclusion, equity, and peak performance.
1. Introduction
1.1. Learning Disabilities
Learning disabilities are defined as a set of neurodevelopmental disorders of biological basis that induce cognitive abnormalities as well as symptoms related to emotional and behavioral disorders. The biological etiology is indeed a combination of genetic, epigenetic, and environmental factors that alter the brain’s ability to recognize or process verbal or nonverbal information effectively and precisely [1].
1.2. Classification of Learning Disabilities
Mental health specialists, including learning impairment associations, consider the following conditions to contain serious learning difficulties. They distinguish autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD) as related but distinct neurodevelopmental disorders that impact learning [2,3]: (1) physical disabilities, (2) sensory impairments, (3) moderate/severe cognitive disabilities, (4) autism, (5) learning disabilities, (6) attention deficit, (7) behavioral disorders, (8) giftedness.
1.3. Metacognition (Definition)
Metacognition is defined by Drigas and Mitsea [15] as the “set of regulatory meta-abilities and meta-skills that are consciously applied aiming at the smooth operation of the cognitive & psychophysiological mechanism as a means of achieving functional capability, self-efficacy, independent living & life satisfaction. Metacognition involves consciousness-raising skills and strategies such as individuals’ ability to observe, regulate and adapt their internal cognitive processes, recognize the difference between functional and dysfunctional states of mind and consciously choose those states that awaken the full range of their abilities and identity” (Figure 1 and Figure 2).
1.4. The Eight Pillars of Metacognition
- Acquiring knowledge: Humans’ ability to construct knowledge, especially about their cognitive mechanisms, making meta-representations of the knowledge. It includes also grasping the concept of cognition, its functions, as well as its hierarchical relationships. It also requires comprehension about meta- abilities and meta-skills that allows people to “learn how to learn”. In other words, to be aware of the phenomenon of self-conscious learning itself.
- Applied knowledge: The human meta-ability to strategically use his/her mental tools evaluating the degrees of freedom defined by a specific situation, problem, or task. Applied knowledge requires experience and practical use of knowledge in the real world. It also implies self-awareness of personal strengths and weaknesses. Finally, it includes the ability to transfer previous knowledge to novel contexts.
- Self-observation: Real-time conscious monitoring of the external (exteroception) and internal processes (introspection). It is a kind of internal attention and control that lights up the patterns of thoughts and feelings, using the feedback received from the external environment such as our social environment. Therefore, self-observation is standing at the crossroad between intrapersonal and interpersonal routes. Although most typical individuals are aware of this capacity, it is a metacognitive, self-conscious meta-skill that develops gradually and after regular training.
- Self-regulation: The capability to restore any observed disturbance that disrupts the regular functioning of cognitive and psychophysiological operations (i.e., anxiety, impulses, over-reactivity).
- Adaptation: Individuals’ flexibility to adjust their mental functions and behavior in response to the demands of specific environments and personal goals.
- Recognition: The faculty of perception is what allows one to identify and be aware of sensations, objects, thoughts, and emotions. Furthermore, it entails individuals’ meta-ability to attribute mental and emotional states to themselves as well as others, to be empathetic, to perceive and predict intentions, and to comprehend the underlying motives.
- Discrimination: The ability to filter, assess, and strategically select what is vital or unnecessary in a given situation, in terms of information, knowledge, motivations, desires, attitudes, strategies, and behaviors. At a more abstract level, discrimination helps people to have prudence and make wise judgments and decisions.
- Mnemosyne: The state of awakening. The ability to voluntarily maintain a state of relaxed awareness while being awake, aiming to achieve peak performance. It also symbolizes the internalized wisdom that awakens and propels humans toward independence and self-fulfillment.
1.5. Virtual Reality
VR is commonly regarded as a technology that induces virtual immersion in a digital world via the use of a computerized graphic simulation that allows users to immerse themselves in an interactive three-dimensional world brimming with various sensory and emotional experiences [17].
To assist learners’ interaction with the VR environments, special interfaces are necessary, designed to input learners’ commands into the computer and provide feedback to the learner. Input/output devices such as user monitoring devices (i.e., body tracking), VR navigation devices (i.e., tracker-based navigation/manipulation, trackballs), visual displays (i.e., projection VR, head-based displays), auditory displays, and haptic displays are some examples of commonly used VR interfaces [18].
1.6. VR in Special Education
Virtual reality (VR) is increasingly being used in formal education as a tool for cognitive training and inquiry-based learning [19,20,21,22], while serving as an intervention tool for psychiatric disorders such as depression, anxiety, phobias, and anxiety [22]. The increasing number of research publications regarding the role of virtual reality (VR) technologies in the field of special education indicates that VR applications are gaining attention as promising intervention tools for students with neurodevelopmental disorders, physical disabilities, and learning difficulties [13,23,24,25,26,27,28]. The axes of VR implementation in special education are at least the following three (Figure 3):
VR in Assessment and Diagnosis: Assessment demands expert observations in neutral settings, which imposes limitations and biases because of a lack of objectivity. In addition, conventional assessments often do not capture performance in real-world settings [29]. Studies have already shown the potential advantages of using virtual reality in assessment, as it facilitates the diagnosis of various neurodevelopmental disorders. Virtual reality and sensors (such as eye-tracking tools) have been utilized to track eye movements and identify various cognitive and behavioral abnormalities, enriching assessments with more objective data than standard methods. In some cases, virtual reality tests show better sensitivity and specificity than typical tests in identifying disorder-related symptoms [29,30].
VR in Intervention and Rehabilitation: VR systems have become a cutting-edge clinical tool for patients with specific psychiatric symptoms. The use of virtual reality has already expanded to the field of intervention and rehabilitation of neurodevelopmental disorders, and physical and learning disabilities such as autism, ADHD, posttraumatic stress disorder, depression, schizophrenia, and psychosis [22,31].
VR in Skills Training: The use of VR facilitates skills training. Research has already shown virtual reality training skills environments help people with and without disabilities to develop skills such as social and emotional skills [27,32], metacognitive skills [13,24,26], vocational skills [33], 21st-century skills including problem solving, collaboration, communication skills, critical thinking skills [19], digital skills [34], as well as soft skills [35].
In more recent studies, researchers consider alternative intervention strategies, new methods, and techniques as a priority for dealing with learning disabilities and related disorders [36,37]. When used separately, both technologies and therapeutic techniques have already shown positive results for individuals with disabilities [22,27,28,31,32,33]. However, researchers propose a hybrid approach, such as implementing psychotherapeutic principles used in learning disability therapy in virtual worlds [38]. For instance, some researchers have developed interventions that combine cognitive behavioral therapy techniques with immersive virtual reality exposure [39]. Although such types of interventions have provided beneficial outcomes, they have not been sufficiently examined [38,39]. In addition, less emphasis has been given to approaches such as clinical hypnosis and neuro-linguistic programming, which are already utilized in clinical interventions with beneficial effects [23,24,25,26]. As a result, the motivation of this study is to present a review that brings together representative findings from previous experimental research and evaluate both whether VR can provide suitable conditions for the application of training techniques and whether the blending of VR with such techniques can improve the metacognitive abilities needed for the inclusion of people with disabilities. In the same context, we will examine the benefits that virtual reality provides as well as the features that may facilitate the implementation of brain-rewiring techniques, especially in cases of people with disabilities. This is the first study, according to our knowledge, that reviews the implementation of VR brain-rewiring techniques for people with learning disabilities.
2. Materials and Methods
The purpose of the current study is to investigate the efficacy of brain-rewiring techniques within virtual reality environments in the treatment of various learning and mental disorders. Specifically, we investigate whether virtual reality brain-rewiring techniques can improve the metacognitive abilities and skills needed to be more inclusive in 21st-century society. To that end, we present a brief, representative, and non-exhaustive literature review of research studies that investigate the effectiveness of brain-rewiring techniques within virtual environments. Intending to examine the subject as comprehensively as possible, we include two sections concerning the benefits and features of virtual reality that may facilitate the application and effectiveness of such techniques, while we provide a brief overview of the techniques that may have the potential to work in conjunction with virtual reality.
The central research question of our review study is whether interventions that implement brain-rewiring techniques within virtual environments have beneficial effects on metacognitive abilities that people with learning and other related disorders struggle with.
For this review study, an electronic search was conducted using the following databases and search engines: Google Scholar, Mendeley, PubMed, Science Direct. The key terms we used were VR speed learning, VR hypnosis, VR mindfulness, VR neurolinguistic programming, VR breathing training, and VR subliminal techniques, autism, ADHD, specific learning disabilities, depression, anxiety, and phobias.
Studies were included if they used virtual reality as a primary component. In addition, we selected studies that applied the techniques that we have decided to examine in the current study. We mainly focused on experimental research and randomized clinical trials. In addition, case studies were incorporated. Concerning participants, initially, we gave priority to studies that recruited individuals with learning difficulties and related disorders, including behavioral and emotional disorders. Given the lack of studies that fulfill all criteria, we opted to include several studies with healthy subjects, provided that they give evidence about the effectiveness of VR techniques on variables related to metacognition such as cognitive and emotional regulation, self-control, and self-awareness. Participants were children and adults irrespective of gender.
Those studies which focused on conventional virtual reality intervention in learning and other disabilities were excluded. Non-English publications were also excluded. Furthermore, research studies before 2000 were not included in this review.
Following the identification of publications that met the search criteria, abstracts were evaluated to see if they met the inclusion criteria. When it was unclear from the abstract whether an article met the inclusion and exclusion criteria, the entire text was examined. All the indicated articles’ full texts were obtained. The reference lists of these papers were also examined to detect any publications that may have been missed during database searching. Finally, we concluded with a list of 25 selected articles with a total of 1073 participants.
3. Results
3.1. Virtual Reality and Metacognitive Skills in Special Education
Research has already revealed that virtual reality can contribute to metacognitive skills training [13,27,32]. Virtual reality can help people with severe neurodevelopmental disorders such as autism to develop adaptive skills in cognitive and socio-emotional tasks [40,41]. Other studies have revealed improvements in self-regulation skills such as self-observation, attentional flexibility, inhibition control, and other executive functions [42,43]. Several studies highlight the role of VR in emotional regulation in various mental and behavioral disorders such as heavy anxiety, phobias, and depression [44].
3.2. Benefits of VR Environments in Special Education
Safe, Structured and Controlled Environments: Virtual environments provide well-controlled sensory stimuli according to the needs of users, because people with learning disabilities face serious sensory processing difficulties. For instance, therapists can provide either more stimulation to motivate subjects or less sensory stimulation to relax them. In addition, we avoid the risks and dangers associated with exposing patients to real-life situations [31].
Interactive and Multisensory: VR makes it possible to create highly interactive 3D environments involving multi-sensory channels (vision, audition, haptics), enabling the brain to behave as it would in a real-life situation. These features maximize learning outcomes, but also play a crucial role for people with sensory disabilities [19].
Attention Manipulation: VR utilizes attention as a tool for rehabilitation. The ability to direct attention is a key feature of virtual reality that distinguishes it from various technologies and gives VR an advantage in intervention. Attention has a regulatory role and thus plays a crucial role in behavior modification. VR can either distract users’ attention from stressful stimuli or direct attention in the appropriate direction (i.e., a goal, a piece of important information). VR familiarizes subjects with the functions of attention. Most importantly, it helps users to develop attentional awareness, that is, the realization that they possess and can utilize in various ways a powerful mental tool responsible for self-regulation [15,16,23,24,25,26].
Visualization: VR primarily employs visual interaction pathways minimizing cognitive load and processing energy. According to a recent study, 90 percent of the total information transmitted and processed to the brain is visual, and the time it takes for the visual system to detect and process an image is 60,000 times faster than text [45]. VR replaces many stimuli that patients struggle to visualize via verbal cueing, and thus, it can be useful for those with attention deficits and mental imagery disorders [23,24,25,26]. Imaginative play can also help people with learning disabilities to use both divergent and convergent reasoning to build new knowledge [18]. The use of visual paths can boost creative imagination and complex problem-solving skills required for open-ended problems [18,19].
Personalized Environments for Intervention/Virtual Personalized Scenarios: VR provides personalized environments targeted to people who require training for some physical or cognitive pathology. In addition, trainers can develop virtual scenarios considering the skills to be taught by the subjects according to their abilities and needs. For instance, they can present social scenarios for developing daily living skills for people with autism [46].
Distance Learning: Cloud computing and the widespread adoption of 5G technology have allowed distance education to become meaningful, and with the incorporation of VR technology, realistic distance learning has become a reality for people with learning disabilities [47].
Cooperative/collaborative learning: VR technologies that facilitate immersive learning are considered as having great potential for social scaffolding in cooperative/collaborative settings. For instance, numerous users can interact inside the same virtual area or simulation. Participants can be aware of one another and share a common learning environment by using virtual shared spaces, avatars, and chat rooms. Learners are thus encouraged to collaborate, exchange ideas, and share experiences to gain new knowledge during the learning process [18]. In addition, a VR collaborative environment promotes the flexibility and sociability of younger learners with or without disabilities [48].
Problem-based learning: VR learning environments present real problems, individualize the level of challenge with regular feedback, provide a rich, focused, reflexive, and collaborative learning environment, motivate learners to develop independent thinking ability, and allow learners to observe the simulated situation and identify various aspects of a problem, even a personal problem [18].
Game-based Learning: VR environments have already incorporated serious games (for non-entertainment purposes) showing major learning outcomes when compared to conventional learning scenarios. These playful virtual environments enhance intrinsic motivation and motivate skills learning without external pressure [49].
Immersion and Presence: VR allows the subjects to immerse themselves in a virtual environment, experience the virtual environment as a real and new reality, and, thus, change perspective more easily. Immersive environments intensify the sense of presence, which in turn facilitates deeper levels of information processing [18]. In addition, immersion works as the “greatest empathy generator” since it allows subjects to experience any situation as real, and to adopt different points of view [50], accelerating behavior modification. Last but not least, immersion and presence provide the best possible combination for conscious attention, which constitutes a key feature in cognitive and behavioral regulation [23,24,25,26].
Avatars, Embodied Avatars, and Role-Playing: Virtual avatars are graphical illustrations either of the users or other characters within the virtual space. These virtual agents have a fundamental pedagogical as well as therapeutic role. They can play various roles such as the role of teacher, mentor, advisor, friend, co-worker, or a positive role model (i.e., a successful person) [51]. Avatars also interact with users, helping them to develop new skills and express socially appropriate behaviors in scenarios where virtual job interviews and virtual social meetings can take place [31]. Most importantly, users can interact with an illustrated avatar of themselves, a process that enhances self-observation skills. In addition, embodied avatars can accelerate behavioral modification [23,24,25,26,51]. Avatar embodiment motivates action, enables people to experience different identities, and imbues people with agency. For instance, subjects can imitate superhero or super-villain behaviors. By acting in these virtual roles, individuals may develop self-regulated behaviors, and demonstrate their own, real-life behaviors after them [52,53]. Role-playing using avatars can reverse a potential pattern of behavior, facilitating behavior change [52].
3.3. Brain-Rewiring Techniques in Special Education
Medical Hypnosis Techniques: Hypnosis techniques induce a state of consciousness that occurs when the subject has both focused attention and reduced peripheral awareness. In this state of reduced awareness, subjects are more likely to be open to suggestions (i.e., positive affirmations), which in turn can accelerate behavioral change [54]. Hypnosis targets dysfunctional or overlearned schemas, distorted beliefs, defense mechanisms, undesired automatisms, and conflicting thoughts that decelerate metacognitive capacity and create those conditions that trigger various disorders [23,24]. VR hypnosis delivers hypnotic induction via a customized virtual reality hardware/software setup [23,24,54].
Neurolinguistic Programming Techniques: Neuro-linguistic programming (NLP) is a psychological strategy that applies effective techniques to assist individuals to amplify behavior (Figure 4). NLP is in line with positive psychology and fundamental learning theories such as social learning theory developed by Bandura, which supports the premise that we acquire knowledge in our social interactions through observation and imitation. NLP techniques include Role-Playing, Reframing, Modelling, Positive Affirmations, and Positive Visualizations [25,26,53].
Subliminal Techniques: Subliminal techniques expose humans to visual or/and auditory stimuli under the threshold of conscious perception. Subliminal cues can implicitly direct subjects’ attention to important information or a new positive goal, to distract them from negative information and habits to exposure to stressful stimuli to desensitize them from a phobia. ICTs and especially virtual reality seem to provide an ideal environment to support these techniques [55].
Fast Learning Techniques: An umbrella term that includes all those techniques that make learning fast and easy such as speed reading, speed listening, metamemory techniques, fast calculation, and eye training strategies. Speed learning techniques are considered all those techniques that either facilitate the factors that accelerate learning (i.e., visual acuity, perception, spatial attention, short-term memory, processing speed) or slow down the inhibitors of fast learning (i.e., cognitive load, anxiety, negative emotions, implicit bias) [56].
Breathing Training Techniques: Breathing, though nonconscious and often overlooked, is a central aspect of our whole being and one of our most vital functions. Systematic instruction in respiratory control exercises offers lasting physiological and neuropsychological benefits, reducing the signs of chronic illnesses as well as the subsequent abnormalities [57]. Recent research recognizes the feasibility of breathing training intervention in virtual environments as a means of physiological and neuropsychological regulation (Figure 5) [57,58,59].
Mindfulness Techniques: Mindfulness training refers to the practice of orienting one’s attention to the present moment, monitoring any thoughts, sensations, and emotions that arise in real-time experience [60]. Mindfulness techniques train subjects to develop sensory and attentional awareness, which are fundamental metacognitive abilities. Systematic training aims to help subjects to utilize attention as a tool for self- and emotional regulation [61]. Mindfulness-based interventions have already been applied to people with special needs [62].
3.4. VR-Assisted Techniques for Metacognitive Skills Training in Special Education
3.4.1. VR Hypnosis Techniques (VRH)
Clinical hypnosis provides a series of hypnotherapeutic techniques that have positive effects on learning disabilities [63]. According to Drigas and Mitsea [24], clinical hypnosis techniques constitute a powerful intervention for a wide range of mental or emotional problems that people with learning difficulties usually face (Table 1).
Virtual reality hypnosis is considered an innovative and effective intervention that deploys the opportunities offered by the virtual environment adjusted to various hypnotherapeutic techniques [64,65]. Virtual reality hypnosis concentrates attention on the present moment and removes disruptive stimuli, making it advantageous for individuals with attention deficits. VRH can be also beneficial for people with mental imagery difficulties (i.e., dyslexia, dyscalculia, depression) switching verbal stimuli that the patients struggle to visualize with visual cues. Moreover, it shows significant potential for hearing impairments [65].
Clinical hypnosis has been shown to help people with autism spectrum disorder deal with restrictive repetitive behaviors as well as emotional problems. Studies have already shown that hypnotherapeutic techniques can help patients to develop self-regulation abilities and more flexible behaviors [66]. However, in the case of autism, there is one more difficulty: individuals can not easily be hypnotized due to attention deficits and difficulties to receive verbal cues. Virtual environments are well-structured, safe, and offer sensory stimulation in a regulated manner.
Austin et al. [64] carried out a preliminary study to assess virtual reality hypnosis as an adjunctive treatment in a sample of two 14- and 15-year-old boys with severe autism. The findings revealed that, while this treatment relaxed and focused patients’ attention, it had little effect on autistic symptoms. However, more research is needed to discover the variables that may promote VRH effectiveness in autism.
Thomson et al. [67] carried out a randomized controlled trial to determine the efficacy of virtual reality hypnosis on mood, fatigue, and cortisol levels. Thirty-five participants were randomly assigned to one of the following three conditions: VR hypnosis, conventional hypnosis, and relaxation practices. The results revealed that participants in hypnosis interventions showed lower fatigue ratings than the control group. VR hypnosis had the most beneficial effects since it allowed subjects with limited absorption to attain higher engagement, which in turn meant reduced distraction and improved concentration.
Hirsch et al. [68] examined the case of a phobic patient with avoidance behavior using virtual reality exposure therapy in conjunction with hypnosis. Following the intervention, the participant was confident and capable of dealing with his phobias. VR hypnosis combined with exposure therapy assisted him to reframe, and to look at actual situations as being simulations. Similarly, Kraft et al. [69] in their case study achieved complete recovery for a patient with a phobia through systematic desensitization with virtual reality hypnosis.
People with disabilities frequently have a subjective sense of pain. Patterson et al. [70] explored the efficacy of immersive virtual reality hypnosis on pain and stress management. The post-hypnotic suggestions delivered in the virtual environment reduced pain and anxiety by approximately 40 percent.
Similarly, Teeley et al. [71] found a reduction in the sense of pain from 70% to 30% in a sample of three subjects using VRH. VRH caught subjects’ attention, facilitating their responsiveness to hypnosis. At the same time, VR distracted their attention from unpleasant sensations.
Patterson et al. [72], in a randomized control trial, found that virtual reality hypnosis had better results compared with virtual reality distraction methods. Virtual post-hypnotic suggestions (i.e., asking patients to forget suffering, recall positive memories, visualize a brighter future, to feel emotional peace) had a positive impact on self-regulation and pain management.
3.4.2. VR Neurolinguistic Programming Techniques
Banakou et al. [73] investigated whether embodiment in an avatar representing a positive model of a person with exceptional cognitive abilities would result in greater executive functions (i.e., intelligence, working memory) and improved cognitive performance. Fifteen participants were immersed in a virtual body of Einstein as well as the virtual body of someone their own age. It was revealed that the participants who played the role of Einstein performed better on a cognitive task than the usual body, with the effect being greater for those with poor self-esteem. Additionally, the embodiment had a positive effect on the reduction in implicit prejudice and stereotyping.
Osimo et al. [74] explored whether subjects’ embodiment in a virtual body of a famous counselor could regulate their mood and help them manage personal problems. Participants were immersed in digitalized duplicates of their bodies and expressed a personal problem to Sigmund Freud’s avatar. Afterward, they were immersed in Freud’s virtual body to see and hear their doppelganger describe the problem. Participants who were embodied in Freud’s body addressed their problems more successfully and elevated their mood. They could act as counselors, giving the best advice. They were then transferred back to their virtual bodies to receive Freud’s response. VR, immersion, and avatars trained participants in methods commonly used in NLP, such as reframing, perspective taking, and detachment. They were trained to shift their viewpoint away from habitual ways of thinking. In addition, it helped participants develop self-observation skills.
Rosenberg et al. [75] investigated whether the use of an avatar with superhero abilities in immersive virtual reality would increase prosocial behavior. A group of 60 people was randomly allocated to either receive the virtual superpower of flight (like Superman) or to fly as passengers in a helicopter. Afterward, participants were assigned either to a helping condition (to find a lost child in need) or to navigate a virtual city. The experimenter then solicited assistance from the volunteers. The individuals with the superhuman avatar were found to be quicker to assist. Therefore, the virtual interaction with a positive role model improved participants’ empathy and prosocial behavior.
Low mood and depression are characterized by unpleasant visualizations, pessimistic future projections, limited capacity to recall positive experiences, and verbal processing bias. Habak et al. [76] investigated the effects of VR positive visualizations on mood, well-being, and future planning. Seventy-nine subjects were immersed in spectacular virtual landscapes supported by other effects such as a pleasant wind, aiming to improve subjective perception. The virtual exploration aimed to elicit a sense of hopeful expectation, assisting users in realizing that openness and curiosity contribute to a positively rewarding experience. According to the findings, almost all participants felt less depressed. Negative emotion was better-controlled, whereas mindfulness, positive mood, and optimistic planning increased significantly.
Ganschow et al. [77] used virtual reality to conduct a perspective-taking exercise to improve future self-continuity. The exercise was based on the two-chair technique, which entails that the client sits across from an empty chair and visualizes the significant other. This technique was developed also to aid individuals in acting as their successful future selves. Participants responded to a list of questions and reflected on how they could become their positive future selves. The results demonstrated that the perspective-taking exercise in a virtual environment considerably improved participants’ ability to envisage themselves in the future and create future goals.
In another study, Gelder et al. [78] utilized an age-progressed avatar depicting participants’ future selves. During this virtual interaction, subjects reflected on their existing lifestyle, switching between the perspective of their present and future self. VR perspective changing technique helped participants to better self-regulate self-defeating behaviors such as self-criticism, risky behaviors, self-pity, and procrastination.
Empathy, or the ability to share and comprehend another person’s feelings, is a necessary element of interpersonal relationships [32]. However, people with autism or other disabilities face serious difficulties. Herrera et al. [50] carried out two experiments to evaluate the effects of VR perspective-taking practices as well as the role of immersion in various forms of perspective-taking activities. Results showed that VR perspective taking enhances empathy and connection with others. In particular, when subjects are immersed to play the role of someone in need, they adopt more positive attitudes and the outcomes are long-lasting.
3.5. VR Subliminal Techniques Training
A threshold for conscious access exists in human perception. We consider this threshold as the “line” between conscious and subconscious perception [79].
Blanchfield et al. [80] explored the influence of subliminal priming on effort perception and endurance performance. According to the study, emotional and action-related visual cues had a significant impact on performance. The subject could voluntarily adapt to higher demands. They also proposed that non-conscious visual cues can be used as a performance-enhancing method during training by utilizing modern technologies such as virtual smart glasses.
Larsen [81] investigated whether subliminal primes can minimize cognitive processing loads, facilitating decision making and learning in 3D computer games. For that reason, a computer game design framework was applied, where subliminal signals within in-game tutorials aimed to improve the learning and play experience. An experiment with 40 participants was conducted. The experiment revealed that participants had a greater ability for rapid and flexible responses when solving a given task. They also had a better game experience.
Baumeister et al. [82] carried out two experiments to assess subliminal cueing techniques in spatial augmented reality (SAR). The researchers investigated whether supportive subliminal cues could result in faster reactions. The results demonstrated that using subliminal cueing improved reactions and procedural task performance in an SAR setting.
Chalfoun et al. [79,83,84,85] introduced a 3D virtual tutoring system that makes use of subliminal priming in a 3D gaming-like environment. The results of their studies showed that learners felt more motivated, retrieved previous knowledge faster, and could learn more easily. The two later studies conducted [84,85] presented participants with subliminal positive and negative cues. Positive subliminal cues improved reasoning and problem-solving skills by about 10%, according to the research.
3.5.1. VR Speed Learning Techniques
Method of loci refers to a meta-memory technique that has been utilized since classical times to aid individuals to speed up recall by utilizing spatial mappings and environmental attributes. The idea was to mentally map words or phrases onto a mental model of an environment (for instance an amphitheater) and then recall those words by mentally visualizing that place in the environment [86]. Krokos et al. [87] explored whether the implementation of the mnemonic exercise method of loci in a virtual environment would enhance 40 participants’ recollection of memories. When compared to the desktop condition, the virtual loci technique gave greater memory recall and spatial awareness. The authors recognized that mnemonic techniques such as the method of loci find a perfect breeding ground in virtual reality because VR enhances spatial awareness as well as the sense of presence, which plays a crucial role in memory processes.
3.5.2. VR Mindfulness Techniques
Serra-Pla et al. [88] developed and evaluated the first VR mindfulness treatment for people with ADHD. In a pilot study, 25 patients took part in four 30 min VR mindfulness sessions, whereas 25 participants were treated with psychostimulants. The findings indicated better self-management of depression and anxiety for the experimental group.
Modrego et al. [89] conducted a randomized controlled trial to evaluate the benefits of a virtual reality mindfulness program in stress management. A total of 280 university students were allocated randomly to one of the following three conditions: VR mindfulness, traditional mindfulness exercises, and relaxation therapy. Group sessions with 15 or 16 participants were held once a week for 6 weeks, with each session lasting 90 to 75 min. The VR sessions were applied on a personal level. The results revealed that VR mindfulness had a positive impact on stress regulation accompanied by higher retention rates and session attendance.
Asati et al. [90] assessed the benefits of a VR meditation on sustained attention. A calming virtual environment was built with pleasant scenery and relaxing sounds. The user could even feel the wind blowing. A non-action video game and Muse headband EEG signals were used to test the attention span of 12 participants before and after the VR session. Game scores improved following the 10 min virtual reality session. The data from the users’ brain waves suggested that they were more relaxed. Furthermore, the number of times they self-regulated by attempting to switch from arousal to a calming state increased.
Navarro-Haro et al. [91] conducted a pilot study to assess the efficacy of VR mindfulness on self-regulation under high stress. An additional goal was to evaluate the influence on depression, emotion control, mindfulness, and interoceptive awareness. Forty-two participants with generalized anxiety disorder were divided into either a mindfulness group or the mindfulness plus 10 min VR DBT® (Dialectical Behavior Therapy). VR mindfulness intervention had significantly better outcomes in terms of anxiety and depression symptom reduction, emotion regulation, mindfulness, and interoceptive awareness.
In a case study, Navarro-Haro et al. [92] investigated the effectiveness of VR mindfulness intervention in a 32-year-old female diagnosed with borderline personality disorder, a condition characterized by emotional instability, impulsivity, and dysfunctional interpersonal relationships. VR mindfulness intervention assisted patients in better regulating their urges to attempt suicide, self-harm, quit therapy, misuse substances, and experience negative emotions.
3.5.3. VR Breathing Techniques
Shiban et al. [93] studied the influence of diaphragmatic breathing on self-regulation during VR exposure therapy. Twenty-nine phobia patients were randomly allocated to VR exposure treatment with or without diaphragmatic breathing (six cycles per minute). The group that underwent VR exposure mixed with diaphragmatic breathing was more likely to successfully overcome their fear.
Yüksel et al. [94] evaluated the efficacy of VR breathing training in anxiety and sleep disorders in high-school adolescents. Twenty-nine teenagers with sleep problems engaged in slow diaphragmatic breathing while passively viewing a relaxation immersive VR environment designed to foster cognitive relaxation/distraction (20 min). The VR breathing intervention resulted in an immediate increase in relaxation as well as a significant reduction in worry. Heart rate dropped and sleep efficiency increased. The authors discussed the potential of combining cognitive relaxation and distraction strategies with immersive VR technology and physiological downregulation to induce relaxation and improve overall sleep quality in adolescents experiencing relevant issues.
4. Conclusions
The current study aimed to review the literature regarding virtual reality interventions that incorporate brain-rewiring techniques intending to improve metacognitive skills for people with learning disabilities. The results of this review study showed that virtual reality provides a fertile ground for practicing such techniques. The research revealed that interventions which combine virtual reality with therapeutic techniques are effective for training metacognitive skills in people with learning disabilities.
Virtual reality and clinical hypnosis had high potential for synergistic effects in self-regulation processes with attentional and visualization mechanisms as a shared denominator. VR hypnosis helped subjects to overcome various cognitive and behavioral difficulties by captivating and intensifying their attention, minimizing distraction, and boosting imagery, especially in the case of low-imagination individuals. This was established as a fruitful approach for learning impairments.
VR Neurolinguistic programming allowed individuals to detach and shift their perspective away from habitual modes of thought. VR embodiment enhanced subjects’ flexibility to change and adopt new ways of thinking and acting. VR NLP cultivated positive visualizations, positive expectations, hope, and optimism. The most significant asset of VR was the heightened sense of presence and image vividness, which minimized subjects’ distraction and released attentional resources. The use of avatars had a pivotal role in developing self-control skills.
NLP-based techniques were also thought to be effective in VR environments as they supported participants to: (a) modify and follow self-regulated behaviors both in virtual and real life, (b) think about and analyze their beliefs, (c) have faith in their self (d) acknowledge unrecognized abilities, (e) transcend self-imposed constraints and effectively find solutions to personal problems, (f) develop self-perception (g) make wise decisions, (h) improve intelligence (i) boost self-esteem, trust, and curiosity, (j) eliminate implicit bias and stereotyping, and (k) strengthen prosocial behaviors and emotional regulation.
VR provided fertile ground for the practice of subliminal training techniques, assuring high-quality experience and that stimuli are unnoticed. Results showed a positive impact on reaction time, improved mood, motivation, and goal setting, which are important variables in self-regulation.
VR has the potential to support training in fast learning techniques. VR can train the abilities needed for fast and conscious learning such as visual acuity, perceptual span, processing speed, and reaction time.
VR mindfulness training provided rich sensory stimulation and relaxing surroundings. Most importantly, VR mindfulness techniques assisted subjects in consciously using their attention as a tool for self-regulation. Subjects could better observe and be aware of surroundings, sensations, and sounds as if they were in a real-life setting. In addition, VR mindfulness improved various physiological and neuropsychological variables that interact with metacognitive abilities.
VR breathing techniques improved cardiac coherence, induced relaxation, and reduced distraction and mind wandering, helping participants to effortlessly focus attention. VR provided relaxing and engaging conditions. VR breathing trained subjects to be aware of and appropriately use the power of their breathing to interact with the VR space. It also improved internal control, self-monitoring skills, and intrinsic motivation. Participants acquired better awareness of their physiological and neuropsychological conditions. Finally, VR breathing facilitated the coordination between respiration and attention resulting in physiological regulations and metacognitive improvements [58,59].
Virtual reality provides a fertile ground for the practice of various techniques which are considered metacognitive because they train various meta-abilities and meta-skills such as self-observation, self-regulation, and adaptation. In addition, these techniques improve metacognition in two directions, engaging both the pathways of effortful and effortless self-regulation. Effortless self-regulation, in other words, non-conscious self-regulation, can promote a fundamental goal, that is, unlearning. Well-established beliefs, and painful memories, waste cognitive resources and prevent people from taking appropriate conscious decisions. Thus, VR subconscious techniques minimize conscious awareness and reduce the resistance derived from conscious control processes, providing a powerful tool for unlearning and behavior modification.
VR can be a part of educational transformation, bringing changes not only to the everyday life of society but also to humans’ cognitive capacity, equipping them with the possibility to see objects, places, and situations that cannot be seen in reality [20,21,34]. VR, combined with well-recognized therapeutic metacognitive techniques, promises spectacular outcomes for people with or without disabilities. Societies can integrate VR metacognitive techniques as training methods in school settings and workplaces to maximize performance and inclusion. Finally, this study highlights the need to design virtual metacognitive learning environments as a means to cultivate higher-order meta-abilities.
The integration of digital technologies in the field of education is quite effective and rewarding and promotes educational procedures through the use of mobile devices [95,96,97,98,99,100,101,102,103], different ICTs applications [104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120], AI and STEM [121,122,123,124,125,126,127,128,129,130], and games [131,132,133,134,135]. In addition, the blending of ICTs with metacognition theories and models, mindfulness, meditation, and emotional intelligence theories [136,137,138,139,140,141,142,143,144,145], as well as with knowledge about the role of environmental factors and nutrition [146,147,148], advances and boosts educational outcomes and contributes to sustainable living.
The effectiveness of these techniques should be tested in additional contexts by specialized practitioners [65,72,149]. More research is needed, with large-scale experimental studies testing the efficacy of VR-assisted metacognitive methods in learning and other disabilities. Furthermore, additional study on virtual environment design is required to optimize the benefits of these techniques. Finally, research on the deployment of VR metacognitive methods in various contexts, such as school settings, is critical.
Author Contributions
A.D., E.M. and C.S. contributed equally in the conception, development, writing, editing and analysis of this manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
The research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Widiger, T.A.; Costa, P.T., Jr. Personality Disorders and the Five-Factor Model of Personality: Rationale for the Third Edition; American Psychological Association: Washington, DC, USA, 2013; pp. 3–11. [Google Scholar] [CrossRef]
- Joyce-Beaulieu, D.; Sulkowski, M.L. The Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (DSM-5) Model of Impairment. In Assessing Impairment; Springer: Boston, MA, USA, 2016; pp. 167–189. [Google Scholar] [CrossRef]
- Muktamath, V.R.; Hegde, P.; Chand, S. Types of Specific Learning Disability. In Learning Disabilities-Neurobiology, Assessment, Clinical Features and Treatments; IntechOpen: London, UK, 2022. [Google Scholar] [CrossRef]
- Karyotaki, M.; Drigas, A.; Skianis, C. Attentional control and other executive functions. Int. J. Emerg. Technol. Learn. 2017, 12, 3. [Google Scholar] [CrossRef]
- Alloway, T.P.; Gathercole, S.E.; Kirkwood, H.; Elliott, J. The cognitive and behavioral characteristics of children with low working memory. Child Dev. 2009, 80, 606–621. [Google Scholar] [CrossRef]
- Cheng, D.; Xiao, Q.; Chen, Q.; Cui, J.; Zhou, X. Dyslexia and dyscalculia are characterized by common visual perception deficits. Dev. Neuropsychol. 2008, 43, 497–507. [Google Scholar] [CrossRef]
- Tarver, S.G.; Hallahan, D.P. Attention deficits in children with learning disabilities: A review. J. Learn. Disabil. 1974, 7, 560–569. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. Metacognition, stress-relaxation balance & related hormones. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2020, 9, 4–16. [Google Scholar] [CrossRef]
- Alexopoulou, A.; Batsou, A.; Drigas, A. Resilience and Academic Underachievement in Gifted Students: Causes, Consequences and Strategic Methods of Prevention and Intervention. Int. J. Online Biomed. Eng. 2019, 15, 78. [Google Scholar] [CrossRef]
- Doulou, A.; Drigas, A. Behavioral Problems in schools: A theoretical overview and the role of ICTs. Technium. Soc. Sci. J. 2022, 29, 54. [Google Scholar] [CrossRef]
- Sideraki, A.; Papageorgiou, E.; Tsiava, M.; Drigas, A. Stress, Hormones & the role of ICT in autism. Tech. BioChemMed 2022, 3, 49. [Google Scholar] [CrossRef]
- Shibata, Y.; Matsushima, M.; Takeuchi, M.; Kato, M.; Yabe, I. Inappropriate metacognitive status increase state anxiety in genetic counseling clients. Front. Psychol. 2022, 13, 871416. [Google Scholar] [CrossRef]
- Mitsea, E.; Drigas, A.; Skianis, C. Metacognition in Autism Spectrum Disorder: Digital Technologies in Metacognitive Skills Training. Tech. Soc. Sci. J. 2022, 31, 153–173. [Google Scholar] [CrossRef]
- Pappas, M.A.; Polychroni, F.; Drigas, A.S. Assessment of mathematics difficulties for second and third graders: Cognitive and psychological parameters. Behav. Sci. 2019, 9, 76. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. The 8 Pillars of Metacognition. Int. J. Emerg. Technol. Learn. (iJET) 2020, 15, 162–178. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. 8 Pillars X 8 Layers Model of Metacognition: Educational Strategies, Exercises &Trainings. Int. J. Online Biomed. Eng. 2021, 17, 8. [Google Scholar] [CrossRef]
- Villena-Taranilla, R.; Tirado-Olivares, S.; Cózar-Gutiérrez, R.; González-Calero, J.A. Effects of virtual reality on learning outcomes in K-6 education: A meta-analysis. Educ. Res. Rev. 2022, 35, 100434. [Google Scholar] [CrossRef]
- Huang, H.M.; Rauch, U.; Liaw, S.S. Investigating learners’ attitudes toward virtual reality learning environments: Based on a constructivist approach. Comput. Educ. 2010, 55, 1171–1182. [Google Scholar] [CrossRef]
- Papanastasiou, G.; Drigas, A.; Skianis, C.; Lytras, M.; Papanastasiou, E. Virtual and augmented reality effects on K-12, higher and tertiary education students’ twenty-first century skills. Virtual Real. 2019, 23, 425–436. [Google Scholar] [CrossRef]
- Daniela, L.; Aierken, Y. The educational perspective on Virtual Reality experiences of cultural heritage. In New Perspectives on Virtual and Augmented Reality: Finding New Ways to Teach in a Transformed Learning Environment; Daniela, L., Ed.; Taylor & Francis: Abingdon, UK, 2020; ISBN 9780367432119. [Google Scholar]
- Daniela, L.; Lytras, M.D. Editorial: Themed issue on enhanced educational experience in virtual and augmented reality. Virtual Real. 2019, 23, 325–327. [Google Scholar] [CrossRef]
- Cieślik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepańska-Gieracha, J. Virtual reality in psychiatric disorders: A systematic review of reviews. Complementary Ther. Med. 2020, 52, 102480. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. Clinical Hypnosis & VR, Subconscious Restructuring-Brain Rewiring & the Entanglement with the 8 Pillars of Metacognition X 8 Layers of Consciousness X 8 Intelligences. Int. J. Online Biomed. Eng. 2022, 18, 78–95. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. The Role of Clinical Hypnosis and VR in Special Education. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2021, 9, 4–17. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. Neuro-Linguistic Programming & VR via the 8 Pillars of Metacognition X 8 Layers of Consciousness X 8 Intelligences. Tech. Soc. Sci. J. 2021, 26, 159. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. Neuro-Linguistic Programming, Positive Psychology & VR in Special Education. Sci. Electron. Arch. 2022, 15, 30–39. [Google Scholar] [CrossRef]
- Bravou, V.; Oikonomidou, D.; Drigas, A.S. Applications of virtual reality for autism inclusion. A review. Retos Nuevas Tend. Educ. Fís. Deporte Recreación 2022, 45, 779–785. [Google Scholar] [CrossRef]
- Doulou, A.; Drigas, A. Electronic, VR & Augmented Reality Games for Intervention in ADHD. Tech. Soc. Sci. J. 2022, 28, 159. [Google Scholar] [CrossRef]
- Alcañiz, M.; Chicchi-Giglioli, I.A.; Carrasco-Ribelles, L.A.; Marín-Morales, J.; Minissi, M.E.; Teruel-García, G.; Abad, L. Eye gaze as a biomarker in the recognition of autism spectrum disorder using virtual reality and machine learning: A proof of concept for diagnosis. Autism Res. 2022, 15, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, C.; Areces, D.; García, T.; Cueli, M.; González-Castro, P. Comparison between two continuous performance tests for identifying ADHD: Traditional vs. virtual reality. Int. J. Clin. Health Psychol. 2018, 18, 254–263. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, D.J.; Lee, U.; Na, E.J.; Jeon, H.J. A literature overview of virtual reality (VR) in treatment of psychiatric disorders: Recent advances and limitations. Front. Psychiatry 2019, 10, 505. [Google Scholar] [CrossRef]
- Papoutsi, C.; Drigas, A.; Skianis, C. Virtual and augmented reality for developing emotional intelligence skills. Int. J. Recent Contrib. Eng. Sci. IT (IJES) 2021, 9, 35–53. [Google Scholar] [CrossRef]
- Kellems, R.O.; Yakubova, G.; Morris, J.R.; Wheatley, A.; Chen, B.B. Using augmented and virtual reality to improve social, vocational, and academic outcomes of students with autism and other developmental disabilities. In Research Anthology on Inclusive Practices for Educators and Administrators in Special Education; IGI Global: Hershey, PA, USA, 2022; pp. 737–756. [Google Scholar] [CrossRef]
- Daniela, L. Virtual museums as learning agents. Sustainability 2020, 12, 2698. [Google Scholar] [CrossRef]
- Mitsea, E.; Drigas, A.; Mantas, P. Soft Skills & Metacognition as Inclusion Amplifiers in the 21st Century. Int. J. Online Biomed. Eng. 2021, 17, 4. [Google Scholar] [CrossRef]
- Shrestha, M.; Lautenschleger, J.; Soares, N. Non-pharmacologic management of attention-deficit/hyperactivity disorder in children and adolescents: A review. Transl. Pediatr. 2020, 9, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Lambez, B.; Harwood-Gross, A.; Golumbic, E.Z.; Rassovsky, Y. Non-pharmacological interventions for cognitive difficulties in ADHD: A systematic review and meta-analysis. J. Psychiatr. Res. 2020, 120, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Anton, R.; Opris, D.; Dobrean, A.; David, D.; Rizzo, A. Virtual reality in rehabilitation of attention deficit/hyperactivity disorder The instrument construction principles. In Proceedings of the 2009 Virtual Rehabilitation International Conference, Haifa, Israel, 29 June–2 July 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 59–64. [Google Scholar] [CrossRef]
- Maskey, M.; Rodgers, J.; Ingham, B.; Freeston, M.; Evans, G.; Labus, M.; Parr, J.R. Using virtual reality environments to augment cognitive behavioral therapy for fears and phobias in autistic adults. Autism Adulthood 2019, 1, 134–145. [Google Scholar] [CrossRef]
- Ip, H.H.; Wong, S.W.; Chan, D.F.; Byrne, J.; Li, C.; Yuan, V.S.; Wong, J.Y. Enhance emotional and social adaptation skills for children with autism spectrum disorder: A virtual reality enabled approach. Comput. Educ. 2018, 117, 1–15. [Google Scholar] [CrossRef]
- Wang, M.; Reid, D. Using the virtual reality-cognitive rehabilitation approach to improve contextual processing in children with autism. Sci. World J. 2013, 2013, 716890. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.J.; Brown, T.; Ross, V.; Moncrief, M.; Schmitt, R.; Gaffney, G.; Reeve, R. Can youth with autism spectrum disorder use virtual reality driving simulation training to evaluate and improve driving performance? An exploratory study. J. Autism Dev. Disord. 2017, 47, 2544–2555. [Google Scholar] [CrossRef]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing specific phobia/fear in young people with autism spectrum disorders (ASDs) through a virtual reality environment intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef]
- Colombo, D.; Díaz-García, A.; Fernandez-Álvarez, J.; Botella, C. Virtual reality for the enhancement of emotion regulation. Clin. Psychol. Psychother. 2021, 28, 519–537. [Google Scholar] [CrossRef]
- Potter, M.C.; Wyble, B.; Hagmann, C.E.; McCourt, E.S. Detecting meaning in RSVP at 13 ms per picture. Atten. Percept. Psychophys. 2014, 76, 270–279. [Google Scholar] [CrossRef]
- Rodríguez, M.L.; García, Á.G.; Loureiro, J.P.; García, T.P. Personalized Virtual Reality Environments for Intervention with People with Disability. Electronics 2022, 11, 1586. [Google Scholar] [CrossRef]
- Li, P.; Zelong, F.; Tan, J. Research Into improved Distance Learning Using VR Technology. Front. Educ. 2022, 7, 757874. [Google Scholar] [CrossRef]
- Pan, Z.; Cheok, A.D.; Yang, H.; Zhu, J.; Shi, J. Virtual reality and mixed reality for virtual learning environments. Comput. Graph. 2006, 30, 20–28. [Google Scholar] [CrossRef]
- Ulmer, J.; Braun, S.; Cheng, C.T.; Dowey, S.; Wollert, J. Gamification of Virtual Reality assembly training: Effects of a combined point and level system on motivation and training results. Int. J. Hum.-Comput. Stud. 2022, 165, 102854. [Google Scholar] [CrossRef]
- Herrera, F.; Bailenson, J.; Weisz, E.; Ogle, E.; Zaki, J. Building long-term empathy: A large-scale comparison of traditional and virtual reality perspective-taking. PLoS ONE 2018, 13, e0204494. [Google Scholar] [CrossRef]
- O’Connor, S. Virtual reality and avatars in health care. Clin. Nurs. Res. 2019, 28, 523–528. [Google Scholar] [CrossRef]
- Yoon, G.; Vargas, P.T. Know thy avatar: The unintended effect of virtual-self representation on behavior. Psychol. Sci. 2014, 25, 1043–1045. [Google Scholar] [CrossRef]
- Bandura, A. Social Learning Theory; Englewood Cliffs: Prentice Hall, NJ, USA, 1977. [Google Scholar]
- Elkins, G.; Barabasz, A.F.; Council, J.R.; Spiegel, D. Advancing research and practice: The revised APA Division 30 definition of hypnosis. Int. J. Clin. Exp. Hypn. 2015, 63, 1–9. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. Subliminal Training Techniques for Cognitive, Emotional and Behavioural Balance. The role of Emerging Technologies. Tech. Soc. Sci. J. 2022, 33, 164–186. [Google Scholar] [CrossRef]
- Mitsea, E.; Drigas, A.; Skianis, C. ICTs and Speed Learning in Special Education: High-Consciousness Training Strategies for High-Capacity Learners through Metacognition Lens. Tech. Soc. Sci. J. 2022, 27, 230. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. Conscious Breathing: A Powerful Tool for Physical & Neuropsychological Regulation. The role of Mobile Apps. Tech. Soc. Sci. J. 2022, 28, 135–138. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. Intermittent Oxygen Fasting & Digital Technologies: From Antistress & Hormones Regulation to Wellbeing, Bliss & higher Mental States. Tech. BioChemMed 2022, 3, 55–72. [Google Scholar] [CrossRef]
- Mitsea, E.; Drigas, A.; Skianis, C. Breathing, Attention & Consciousness in Sync: The role of Breathing Training, Metacognition & Virtual Reality. Tech. Soc. Sci. J. 2022, 29, 79. [Google Scholar] [CrossRef]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Drigas, A.; Mitsea, E. A Metacognition Based 8 Pillars Mindfulness Model and Training Strategies. Int. J. Recent Contrib. Eng. Sci. IT 2020, 8, 4–17. [Google Scholar] [CrossRef]
- Cairncross, M.; Miller, C.J. The effectiveness of mindfulness-based therapies for ADHD: A meta-analytic review. J. Atten. Disord. 2020, 24, 627–643. [Google Scholar] [CrossRef]
- Johnson, L.S.; Johnson, D.L.; Olson, M.R.; Newman, J.P. The uses of hypnotherapy with learning disabled children. J. Clin. Psychol. 1981, 37, 291–299. [Google Scholar] [CrossRef]
- Austin, D.W.; Abbott, J.A.M.; Carbis, C. The use of virtual reality hypnosis with two cases of autism spectrum disorder: A feasibility study. Contemp. Hypn. 2008, 25, 102–109. [Google Scholar] [CrossRef]
- Askay, S.W.; Patterson, D.R.; Sharar, S.R. Virtual reality hypnosis. Contemp. Hypn. 2009, 26, 40–47. [Google Scholar] [CrossRef]
- Sugarman, L.I.; Garrison, B.L.; Williford, K.L. Symptoms as solutions: Hypnosis and biofeedback for autonomic regulation in autism spectrum disorders. Am. J. Clin. Hypn. 2013, 56, 152–173. [Google Scholar] [CrossRef]
- Thompson, T.; Steffert, T.; Steed, A.; Gruzelier, J. A randomized controlled trial of the effects of hypnosis with 3-D virtual reality animation on tiredness, mood, and salivary cortisol. Int. J. Clin. Exp. Hypn. 2010, 59, 122–142. [Google Scholar] [CrossRef]
- Hirsch, J.A. Virtual reality exposure therapy and hypnosis for flying phobia in a treatment-resistant patient: A case report. Am. J. Clin. Hypn. 2012, 55, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Kraft, T.; Kraft, D. Creating a virtual reality in hypnosis: A case of driving phobia. Contemp. Hypn. 2004, 21, 79–85. [Google Scholar] [CrossRef]
- Patterson, D.R.; Tininenko, J.R.; Schmidt, A.E.; Sharar, S.R. Virtual reality hypnosis: A case report. Int. J. Clin. Exp. Hypn. 2004, 52, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Teeley, A.M.; Soltani, M.; Wiechman, S.A.; Jensen, M.P.; Sharar, S.R.; Patterson, D.R. Virtual reality hypnosis pain control in the treatment of multiple fractures: A case series. Am. J. Clin. Hypn. 2012, 54, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Patterson, D.R.; Jensen, M.P.; Wiechman, S.A.; Sharar, S.R. Virtual reality hypnosis for pain associated with recovery from physical trauma. Int. J. Clin. Exp. Hypn. 2010, 58, 288–300. [Google Scholar] [CrossRef]
- Banakou, D.; Kishore, S.; Slater, M. Virtually being Einstein results in an improvement in cognitive task performance and a decrease in age bias. Front. Psychol. 2018, 9, 917. [Google Scholar] [CrossRef]
- Osimo, S.A.; Pizarro, R.; Spanlang, B.; Slater, M. Conversations between self and self as Sigmund Freud—A virtual body ownership paradigm for self counselling. Sci. Rep. 2015, 5, 13899. [Google Scholar] [CrossRef]
- Rosenberg, R.S.; Baughman, S.L.; Bailenson, J.N. Virtual superheroes: Using superpowers in virtual reality to encourage prosocial behavior. PLoS ONE 2013, 8, e55003. [Google Scholar] [CrossRef]
- Habak, S.; Bennett, J.; Davies, A.; Davies, M.; Christensen, H.; Boydell, K.M. Edge of the present: A virtual reality tool to cultivate future thinking, positive mood, and wellbeing. Int. J. Environ. Res. Public Health 2021, 18, 140. [Google Scholar] [CrossRef]
- Ganschow, B.; Cornet, L.; Zebel, S.; Van Gelder, J.L. Looking back from the future: Perspective taking in virtual reality increases future self-continuity. Front. Psychol. 2021, 12, 664687. [Google Scholar] [CrossRef]
- Van Gelder, J.L.; Cornet, L.J.; Zwalua, N.P.; Mertens, E.C.; van der Schalk, J. Interaction with the future self in virtual reality reduces self-defeating behavior in a sample of convicted offenders. Sci. Rep. 2022, 12, 2254. [Google Scholar] [CrossRef] [PubMed]
- Chalfoun, P.; Frasson, C. Subliminal priming enhances learning in a distant virtual 3D Intelligent Tutoring System. IEEE Multidiscip. Eng. Educ. Mag. 2008, 3, 125–130. [Google Scholar]
- Blanchfield, A.; Hardy, J.; Marcora, S. Non-conscious visual cues related to affect and action alter perception of effort and endurance performance. Front. Hum. Neurosci. 2014, 8, 967. [Google Scholar] [CrossRef] [PubMed]
- Larsen, C.B. Subliminal perception in 3D computer games—Towards an invisible tutorial. In Proceedings of the CHI’13, Paris, France, 27 April–2 May 2013. [Google Scholar] [CrossRef]
- Baumeister, J.; Marner, M.R.; Smith, R.T.; Kohler, M.; Thomas, B.H. Visual Subliminal Cues for Spatial Augmented Reality. In Proceedings of the 2015 IEEE International Symposium on Mixed and Augmented Reality Workshops IEEE, Fukuoka, Japan, 29 September–3 October 2015; pp. 4–11. [Google Scholar] [CrossRef]
- Chalfoun, P.; Frasson, C. Optimal affective conditions for subconscious learning in a 3D intelligent tutoring system. In Proceedings of the International Conference on Human-Computer Interaction, San Diego, CA, USA, 19–24 July 2009; Springer: Berlin/Heidelberg, Germany, 2009; pp. 39–48. [Google Scholar] [CrossRef]
- Chalfoun, P.; Frasson, C. Showing the positive influence of subliminal cues on learner’s performance and intuition: An ERP study. In Proceedings of the International Conference on Intelligent Tutoring Systems, Pittsburgh, PA, USA, 14–18 June 2010; Springer: Berlin/Heidelberg, Germany, 2010; pp. 288–290. [Google Scholar] [CrossRef]
- Chalfoun, P.; Frasson, C. Subliminal cues while teaching: HCI technique for enhanced learning. Adv. Hum. Comput. Interact. 2011, 2011, 968753. [Google Scholar] [CrossRef]
- Fassbender, E.; Heiden, W. The virtual memory palace. J. Comput. Inf. Syst. 2006, 2, 457–464. [Google Scholar]
- Krokos, E.; Plaisant, C.; Varshney, A. Virtual memory palaces: Immersion aids recall. Virtual Real. 2019, 23, 1–15. [Google Scholar] [CrossRef]
- Serra-Pla, J.F.; Pozuelo, M.; Richarte, V.; Corrales, M.; Ibáñez, P.; Bellina, M.; Ramos-Quiroga, J.A. Treatment of attention deficit hyperactivity disorder in adults using virtual reality through a mindfulness programme. Rev. Neurol. 2017, 64, S117–S122. [Google Scholar] [CrossRef]
- Modrego-Alarcon, M.; Lopez-del-Hoyo, Y.; Garcia-Campayo, J.; Perez-Aranda, A.; Navarro-Gil, M.; Beltran-Ruiz, M.; Montero-Marin, J. Efficacy of a mindfulness-based programme with and without virtual reality support to reduce stress in university students: A randomized controlled trial. Behav. Res. Ther. 2021, 142, 103866. [Google Scholar] [CrossRef]
- Asati, M.; Miyachi, T. A Short Virtual Reality Mindfulness Meditation Training for Regaining Sustained Attention. arXiv 2014, arXiv:1907.04487. [Google Scholar] [CrossRef]
- Navarro-Haro, M.V.; Modrego-Alarcón, M.; Hoffman, H.G.; Lopez-Montoyo, A.; Navarro-Gil, M.; Montero-Marin, J.; Garcia-Campayo, J. Evaluation of a mindfulness-based intervention with and without virtual reality dialectical behavior therapy® mindfulness skills training for the treatment of generalized anxiety disorder in primary care: A pilot study. Front. Psychol. 2019, 10, 55. [Google Scholar] [CrossRef]
- Nararro-Haro, M.V.; Hoffman, H.G.; Garcia-Palacios, A.; Sampaio, M.; Alhalabi, W.; Hall, K.; Linehan, M. The use of virtual reality to facilitate mindfulness skills training in dialectical behavioral therapy for borderline personality disorder: A case study. Front. Psychol. 2016, 7, 1573. [Google Scholar] [CrossRef]
- Shiban, Y.; Diemer, J.; Müller, J.; Brütting-Schick, J.; Pauli, P.; Mühlberger, A. Diaphragmatic breathing during virtual reality exposure therapy for aviophobia: Functional coping strategy or avoidance behavior? A pilot study. BMC Psychiatry 2017, 17, 29. [Google Scholar] [CrossRef]
- Yüksel, D.; Goldstone, A.; Prouty, D.; Forouzanfar, M.; Claudatos, S.; Lee, Q.; de Zambotti, M. 0916 The Use of Immersive Virtual Reality and Slow Breathing to Enhance Relaxation and Sleep in Adolescents. Sleep 2020, 43 (Suppl. S1), A348. [Google Scholar] [CrossRef]
- Vlachou, J.A.; Drigas, A.S. Mobile Technology for Students & Adults with Autistic Spectrum Disorders (ASD). Int. J. Interact. Mob. Technol. 2017, 11, 4. [Google Scholar] [CrossRef]
- Papoutsi, C.; Drigas, A.; Skianis, C. Mobile Applications to Improve Emotional Intelligence in Autism-A Review. Int. J. Interact. Mob. Technol. 2018, 12, 47. [Google Scholar] [CrossRef]
- Karabatzaki, Z.; Stathopoulou, A.; Kokkalia, G.; Dimitriou, E.; Loukeri, P.I.; Economou, A.; Drigas, A. Mobile Application Tools for Students in Secondary Education. An Evaluation Study. Int. J. Interact. Mob. Technol. 2018, 12, 2. [Google Scholar] [CrossRef]
- Drigas, A.S.; Angelidakis, P. Mobile Applications within Education: An Overview of Application Paradigms in Specific Categories. Int. J. Interact. Mob. Technol. 2017, 11, 17. [Google Scholar] [CrossRef]
- Stathopoulou, A.; Loukeris, D.; Karabatzaki, Z.; Politi, E.; Salapata, Y.; Drigas, A. Evaluation of mobile apps effectiveness in children with autism social training via digital social stories. Int. J. Interact. Mob. Technol. (iJIM) 2020, 14, 4–18. [Google Scholar] [CrossRef]
- Stathopoulou, A.; Karabatzaki, Z.; Kokkalia, G.; Dimitriou, E.; Loukeri, P.I.; Economou, A.; Drigas, A. Mobile Assessment Procedures for Mental Health and Literacy Skills in Education. Int. J. Interact. Mob. Technol. 2018, 12, 21. [Google Scholar] [CrossRef]
- Drigas, A.S.; Stavridis, G.; Koukianakis, L. A Modular Environment for E-learning and E-psychology Applications. WSEAS Trans. Comput. 2004, 3, 2062–2067. [Google Scholar]
- Drigas, A.; Ioannidou, R.E.; Kokkalia, G.; Lytras, M.D. ICTs, mobile learning and social media to enhance learning for attention difficulties. J. Univ. Comput. Sci. 2014, 20, 1499–1510. [Google Scholar] [CrossRef]
- Kokkalia, G.K.; Drigas, A.S. Mobile learning for special preschool education. Int. J. Interact. Mob. Technol. 2016, 10, 67. [Google Scholar] [CrossRef]
- Pappas, M.A.; Papoutsi, C.; Drigas, A.S. Policies, practices, and attitudes toward inclusive education: The case of Greece. Soc. Sci. 2018, 7, 90. [Google Scholar] [CrossRef]
- Drigas, A.; Kokkalia, G. ICTs and special education in kindergarten. Int. J. Emerg. Technol. Learn. (iJET) 2014, 9, 35–42. [Google Scholar] [CrossRef]
- Drigas, A.; Koukianakis, L.; Papagerasimou, Y. Towards an ICT-based psychology: E-psychology. Comput. Hum. Behav. 2011, 27, 1416–1423. [Google Scholar] [CrossRef]
- Drigas, A.S.; Pappas, M.A.; Lytras, M. Emerging technologies for ICT based education for dyscalculia: Implications for computer engineering education. Int. J. Eng. Educ. 2016, 32, 1604–1610. [Google Scholar]
- Pappas, M.A.; Drigas, A.S.; Papagerasimou, Y.; Dimitriou, H.; Katsanou, N.; Papakonstantinou, S.; Karabatzaki, Z. Female entrepreneurship and employability in the digital era: The case of Greece. J. Open Innov. Technol. Mark. Complex. 2018, 4, 15. [Google Scholar] [CrossRef]
- Papanastasiou, G.; Drigas, A.; Skianis, C.; Lytras, M.; Papanastasiou, E. Patient-centric ICTs based healthcare for students with learning, physical and/or sensory disabilities. Telemat. Inform. 2018, 35, 654–664. [Google Scholar] [CrossRef]
- Drigas, A.; Kontopoulou, M.T.L. ICTs based physics learning. Int. J. Eng. Pedagog. (iJEP) 2016, 6, 53–59. [Google Scholar] [CrossRef]
- Papanastasiou, G.; Drigas, A.; Skianis, C.; Lytras, M. Brain computer interface based applications for training and rehabilitation of students with neurodevelopmental disorders. A literature review. Heliyon 2020, 6, e04250. [Google Scholar] [CrossRef]
- Pappas, M.A.; Demertzi, E.; Papagerasimou, Y.; Koukianakis, L.; Kouremenos, D.; Loukidis, I.; Drigas, A.S. E-learning for deaf adults from a user-centered perspective. Educ. Sci. 2018, 8, 206. [Google Scholar] [CrossRef]
- Theodorou, P.; Drigas, A.S. ICTs and Music in Generic Learning Disabilities. Int. J. Emerg. Technol. Learn. 2017, 12, 101. [Google Scholar] [CrossRef]
- Drigas, A.; Kokkalia, G.; Lytras, M.D. ICT and collaborative co-learning in preschool children who face memory difficulties. Comput. Hum. Behav. 2015, 51, 645–651. [Google Scholar] [CrossRef]
- Drigas, A.; Pappas, M. ICT Based Screening Tools and Etiology of Dyscalculia. Int. J. Eng. Pedagog. (iJEP) 2015, 5, 61–66. [Google Scholar] [CrossRef]
- Drigas, A.S.; Politi-Georgousi, S. Icts as a distinct detection approach for dyslexia screening: A contemporary view. Int. J. Online Biomed. Eng. (iJOE) 2019, 15, 46–60. [Google Scholar] [CrossRef]
- Bakola, L.N.; Rizos, N.D.; Drigas, A. ICTs For Emotional and Social Skills Development for Children with ADHD And ASD Co-existence. Int. J. Emerg. Technol. Learn. 2019, 14, 122–131. [Google Scholar] [CrossRef]
- Kontostavlou, E.Z.; Drigas, A.S. The Use of Information and Communications Technology (ICT) in Gifted Students. Int. J. Recent Contrib. Eng. Sci. IT 2019, 7, 60–67. [Google Scholar] [CrossRef]
- Drigas, A.; Vlachou, J.A. Information and communication technologies (ICTs) and autistic spectrum disorders (ASD). Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2016, 4, 4–10. [Google Scholar] [CrossRef]
- Drigas, A.; Koukianakis, L. An open distance learning e-system to support SMEs e-enterprising. In Proceedings of the 5th WSEAS International Conference on Artificial Intelligence, Knowledge Engineering, Data Bases, San Diego, CA, USA, 27–31 October 2006. [Google Scholar] [CrossRef]
- Kefalis, C.; Drigas, A. Web Based and Online Applications in STEM Education. Int. J. Eng. Pedagog. (iJEP) 2019, 9, 76–85. [Google Scholar] [CrossRef]
- Drigas, A.S.; Ioannidou, R.E. A review on artificial intelligence in special education. In Proceedings of the 4th World Summit on the Knowledge Society, Mykonos, Greece, 21–23 September 2011; pp. 385–391. [Google Scholar]
- Drigas, A.S.; Vrettaros, J.; Koukianakis, L.G.; Glentzes, J.G. A Virtual Lab and e-learning system for renewable energy sources. In Proceedings of the 1st WSEAS/IASME International Conference on Educational Technologies, Tenerife, Spain, 16–18 December 2005. [Google Scholar]
- Drigas, A.S.; Argyri, K.; Vrettaros, J. Decade review (1999–2009): Artificial intelligence techniques in student modeling. In World Summit on Knowledge Society; Springer: Berlin/Heidelberg, Germany, 2009; pp. 552–564. [Google Scholar] [CrossRef]
- Vrettaros, J.; Tagoulis, A.; Giannopoulou, N.; Drigas, A. An empirical study on the use of Web 2.0 by Greek adult instructors in educational procedures. World Summit Knowl. Syst. (WSKS) 2009, 49, 164–170. [Google Scholar] [CrossRef]
- Drigas, A.; Dourou, A. A Review on ICTs, E-Learning and Artificial Intelligence for Dyslexic’s Assistance. Int. J. Emerg. Technol. Learn. (iJET) 2013, 8, 63–67. [Google Scholar] [CrossRef]
- Drigas, A.S.; Ioannidou, R.E. Artificial intelligence in special education: A decade review. Int. J. Eng. Educ. 2012, 28, 1366. [Google Scholar] [CrossRef]
- Drigas, A.; Leliopoulos, P. The Use of Big Data in Education. Int. J. Comput. Sci. Issues 2014, 11, 58–63. [Google Scholar]
- Anagnostopoulou, P.; Alexandropoulou, V.; Lorentzou, G.; Lykothanasi, A.; Ntaountaki, P.; Drigas, A. Artificial intelligence in autism assessment. Int. J. Emerg. Technol. Learn. (iJET) 2020, 15, 95–107. [Google Scholar] [CrossRef]
- Pappas, M.; Drigas, A. Incorporation of artificial intelligence tutoring techniques in mathematics. Int. J. Eng. Pedagog. 2016, 6, 12–16. [Google Scholar] [CrossRef]
- Papanastasiou, G.P.; Drigas, A.S.; Skianis, C. Serious games in preschool and primary education: Benefits and impacts on curriculum course syllabus. Int. J. Emerg. Technol. Learn. 2017, 12, 44–56. [Google Scholar] [CrossRef]
- Kokkalia, G.; Drigas, A.; Economou, A.; Roussos, P.; Choli, S. The use of serious games in preschool education. Int. J. Emerg. Technol. Learn. 2017, 12, 15–27. [Google Scholar] [CrossRef]
- Drigas, A.S.; Pappas, M.A. Online and Other Game-Based Learning for Mathematics. Int. J. Online Eng. 2018, 11, 62. [Google Scholar] [CrossRef]
- Papanastasiou, G.; Drigas, A.; Skianis, C.; Lytras, M.D. Serious games in K-12 education: Benefits and impacts on students with attention, memory and developmental disabilities. Program 2017, 51, 424–440. [Google Scholar] [CrossRef]
- Kokkalia, G.; Drigas, A.; Economou, A. The role of games in special preschool education. Int. J. Emerg. Technol. Learn. (iJET) 2016, 11, 30–35. [Google Scholar] [CrossRef]
- Drigas, A.; Papoutsi, C. Emotional intelligence as an important asset for HR in organizations: Leaders and employees. Int. J. Adv. Corp. Learn. 2019, 12, 56–66. [Google Scholar] [CrossRef]
- Drigas, A.S.; Pappas, M.A. The consciousness-intelligence-knowledge pyramid: An 8 × 8 layer model. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2017, 5, 14–25. [Google Scholar] [CrossRef]
- Drigas, A.; Papoutsi, C. The Need for Emotional Intelligence Training Education in Critical and Stressful Situations: The Case of COVID-19. Int. J. Recent Contrib. Eng. Sci. IT 2020, 8, 20–35. [Google Scholar] [CrossRef]
- Papoutsi, C.; Drigas, A. Games for Empathy for Social Impact. Int. J. Eng. Pedagog. 2016, 6, 36–40. [Google Scholar] [CrossRef]
- Karyotaki, M.; Drigas, A. Online and other ICT Applications for Cognitive Training and Assessment. Int. J. Online Biomed. Eng. 2015, 11, 36–42. [Google Scholar] [CrossRef]
- Chaidi, Ι.; Drigas, A. Autism, Expression, and Understanding of Emotions: Literature Review. Int. J. Online Biomed. Eng. 2020, 16, 94–111. [Google Scholar] [CrossRef]
- Drigas, A.S.; Karyotaki, M. A Layered Model of Human Consciousness. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2019, 7, 41–50. [Google Scholar] [CrossRef]
- Karyotaki, M.; Drigas, A. Latest trends in problem solving assessment. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2016, 4, 4–10. [Google Scholar] [CrossRef]
- Angelopoulou, E.; Drigas, A. Working Memory, Attention and their Relationship: A theoretical Overview. Res. Soc. Dev. 2021, 10, 5. [Google Scholar] [CrossRef]
- Kokkalia, G.; Drigas, A.; Economou, A.; Roussos, P. School Readiness from Kindergarten to Primary School. Int. J. Emerg. Technol. Learn. 2019, 14, 4. [Google Scholar] [CrossRef]
- Stavridou, T.; Driga, A.M.; Drigas, A. Blood Markers in Detection of Autism. Int. J. Recent Contrib. Eng. Sci. IT 2021, 9, 79–86. [Google Scholar] [CrossRef]
- Driga, A.M.; Drigas, A.S. Climate Change 101: How Everyday Activities Contribute to the Ever-Growing Issue. Int. J. Recent Contrib. Eng. Sci. IT 2019, 7, 22–31. [Google Scholar] [CrossRef]
- Driga, A.M.; Drigas, A. ADHD in the Early Years: Pre-Natal and Early Causes and Alternative Ways of Dealing. Int. J. Online Biomed. Eng. 2019, 15, 95. [Google Scholar] [CrossRef]
- Rousseaux, F.; Bicego, A.; Ledoux, D.; Massion, P.; Nyssen, A.S.; Faymonville, M.E.; Vanhaudenhuyse, A. Hypnosis associated with 3D immersive virtual reality technology in the management of pain: A review of the literature. J. Pain Res. 2020, 13, 1129. [Google Scholar] [CrossRef] [PubMed]


Figure 3.
The axes of VR implementation in Special Education.

Figure 4.
The core mechanism of behavior modeling is based on two vital control-regulation systems represented by the control-system modeling theory [25].
Figure 4.
The core mechanism of behavior modeling is based on two vital control-regulation systems represented by the control-system modeling theory [25].

Figure 5.
Metacognition in Breathing: Bidirectionality characterizes metacognition and breathing. Metacognition equips people with those meta-abilities (i.e., awareness, regulation, and adaptability) required to manage their breathing patterns to overcome learning challenges [57,58,59].


{kind=link}
{kind=link}
{kind=link}
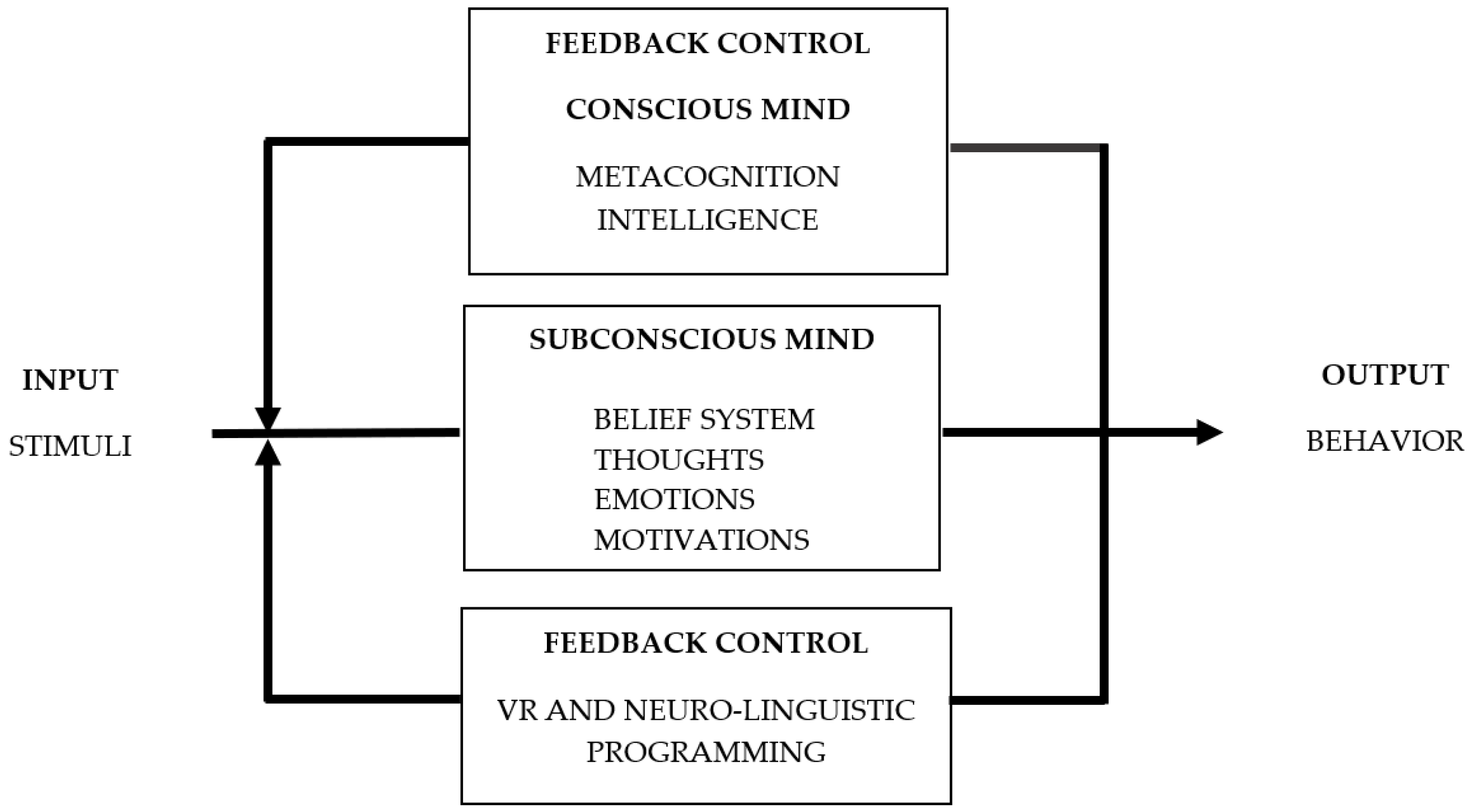{kind=link}
{kind=link}
Table 1.
The role of Clinical Hypnosis in Special Education [24].
Table 1.
The role of Clinical Hypnosis in Special Education [24].
| Type of Disorder | Main Findings |
|---|---|
| ADHD | Less inattentiveness and irritability |
| Optimism | |
| Better speed reaction | |
| AUTISM | Joint attention |
| Emotional receptivity and comprehension Improved motor behavior Self-control and social engagement Observation and recognition skills | |
| DYSLEXIA | Better working memory |
| Visuospatial skills | |
| PHYSICAL IMPAIRMENTS | Motor imagery Motor control Implicit learning |
| DOWN SYNDROME | Improved retrieval of information |
| LANGUAGE DISORDERS | Speech regulation, fluency Faster reading and listening Improved comprehension Resilience to failure |
| ANXIETY | Improved inhibition of the reaction of fear Decreased activation of the anxiety circuity |
| DEPRESSION | Disengagement from negative self-hypnosis Optimism |
| GIFTEDNESS | Creativity and problem solving Intrinsic motivation Flow, peak performance, enjoyment |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Drigas, A.; Mitsea, E.; Skianis, C. Virtual Reality and Metacognition Training Techniques for Learning Disabilities. Sustainability 2022, 14, 10170. https://0-doi-org.brum.beds.ac.uk/10.3390/su141610170
AMA Style
Drigas A, Mitsea E, Skianis C. Virtual Reality and Metacognition Training Techniques for Learning Disabilities. Sustainability. 2022; 14(16):10170. https://0-doi-org.brum.beds.ac.uk/10.3390/su141610170
Chicago/Turabian StyleDrigas, Athanasios, Eleni Mitsea, and Charalabos Skianis. 2022. "Virtual Reality and Metacognition Training Techniques for Learning Disabilities" Sustainability 14, no. 16: 10170. https://0-doi-org.brum.beds.ac.uk/10.3390/su141610170
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.