
Effects of Multicomponent Exercise Training Program on Biochemical and Motor Functions in Patients with Alzheimer’s Dementia

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Mini-Mental State Examination (MMSE)
2.3. Tinetti Test
2.4. The Berg Balance Scale
2.5. Six-Minute Walking Test (6MWT)
2.6. Timed up and Go Test
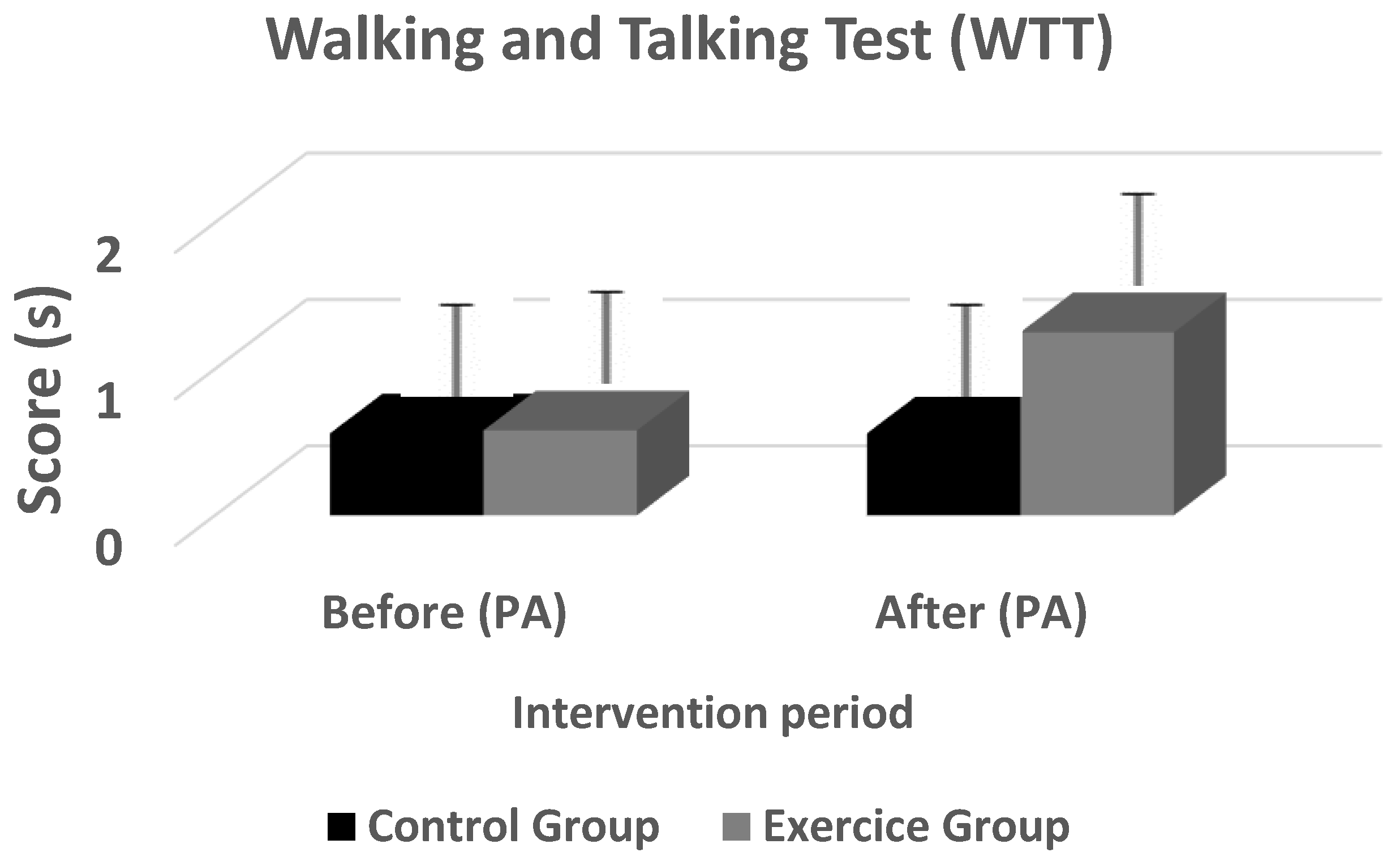
2.7. The Walking and Talking Test (WTT)
2.8. Blood Analysis and Biomechanical Assays
2.9. Multicomponent Exercise Training Program
2.10. Statistical Analysis
3. Results
3.1. Change in Physical Function
3.2. Effect of Physical Activity on Biochemical Parameters
4. Discussion
4.1. Intervention
4.2. Effects of Physical Activity on Functional Parameters
4.3. Effects of Physical Activity on Biochemical Parameters
4.4. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blennow, K.; Leon, M.J.; Zetterberg, H. Alzheimer’s disease. Lancet 2006, 368, 387–403. [Google Scholar] [CrossRef]
- Paulson, H.L.; Igo, I. Genetics of dementia. Semin. Neurol. 2011, 31, 449–460. [Google Scholar] [CrossRef] [PubMed]
- Brookmeyer, R.; Johnson, E.; Ziegler-Graham, K.; Arrighi, H.M. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007, 3, 186–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health and Aging. 2019. Available online: https://www.who.int/ageing/publications/global_health.pdf (accessed on 27 January 2022).
- Emery, V.O. Alzheimer disease. Are we intervening too late. Pro. J. Neural. Transm. 2011, 118, 1361–1378. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Azimzadeh, E.; Hassanlouei, H.; Badicu, G.; Pérez-Gómez, J.; Ardigò, L.P. Effect of Physical Guidance on Learning a Tracking Task in Children with Cerebral Palsy. Int. J. Environ. Res. Public Health 2021, 18, 7136. [Google Scholar] [CrossRef]
- Matsunga, S.; Kishi, T.; Iwata, N. Combination therapy with cholinesterase inhibitors and memantine for Alzheimer’s disease: A systematic review and meta-analysis. Int. J. Neuropsychopharmacol. 2014, 18, 115. [Google Scholar] [CrossRef]
- Buschert, V.; Bokde, L.W.; Hampel, H. Cognitive intervention in Alzheimer disease. Nat. Rev. Neurol. 2010, 6, 508–517. [Google Scholar] [CrossRef]
- Reijnders, J.; van Heugten, C.; van Boxtel, M. Cognitive interventions in healthy older adults and people with mild cognitive impairment: A systematic review. Ageing. Res. Rev. 2013, 12, 263–275. [Google Scholar] [CrossRef]
- Nobari, H.; Ahmadi, M.; Sá, M.; Pérez-Gómez, J.; Clemente, F.M.; Adsuar, J.C.; Minasian, V.; Afonso, J. The effect of two types of combined training on bio-motor ability adaptations in sedentary females. J. Sports Med. Phys. Fit. 2021, 61, 1317–1325. [Google Scholar] [CrossRef]
- Nobari, H.; Rezaei, S.; Sheikh, M.; Fuentes-García, J.P.; Pérez-Gómez, J. Effect of Virtual Reality Exercises on the Cognitive Status and Dual Motor Task Performance of the Aging Population. Int. J. Environ. Res. Public Health 2021, 18, 8005. [Google Scholar] [CrossRef] [PubMed]
- Pitkälä, K.H.; Pöysti, M.M.; Laakkonen, M.L.; Tilvis, R.S.; Savikko, N.; Kauti¬ainen, H. Effects of the Finnish Alzheimer disease exercise trial (FINALEX): A randomized controlled trial. JAMA. Intern. Med. 2013, 173, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Bull, F.; Guthold, R. Physical activity: Progress and challenges. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- Norton, S.; Matthews, F.E.; Barnes, D.E.; Yaffe, K.; Brayne, C. Potential for primary prevention of Alzheimer’s disease: An analysis of population based data. Lancet Neurol. 2014, 13, 788–794. [Google Scholar] [CrossRef] [Green Version]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; American College of Sports Medicine: Indianapolis, IN, USA, 2014. [Google Scholar]
- Radak, Z.; Hart, N.; Sarga, L. Exercice plays a preventive role against Alzheimer’s disease. J. Alzheimers Dis. 2010, 20, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Allali, G.; Verghese, J. Management of gait changes and fall risk in MCI and dementia. Curr. Treat. Options Neurol. 2017, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.X.; Liang, J.H.; Xu, Y. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef]
- Valenzuela, P.L.; Castillo-García, A.; Morales, J.S.; de la Villa, P.; Hampel, H.; Emanuele, E.; Lista, S.; Lucia, A. Exercise benefits on Alzheimer’s disease: State-of-the-science. Ageing Res. Rev. 2020, 62, 101108. [Google Scholar] [CrossRef]
- Shams, A.; Nobari, H.; Afonso, J.; Abbasi, H.; Mainer-Pardos, E.; Pérez-Gómez, J.; Bayati, M.; Bahrami, A.; Carneiro, L. Effect of Aerobic-Based Exercise on Psychological Well-Being and Quality of Life Among Older People: A Middle East Study. Front. Public Health 2021, 9, 764044. [Google Scholar] [CrossRef]
- McGurran, H.; Glenn, J.M.; Madero, E.N. Prevention and treatment of Alzheimer’s disease: Biological mechanisms of exercise. J. Alzheimers Dis. 2019, 69, 311–338. [Google Scholar] [CrossRef]
- Fiuza-Luces, C.; Garatachea, N.; Berger, N.A. Exercise is the real polyplill. Physiology 2013, 28, 330–358. [Google Scholar] [CrossRef] [Green Version]
- Lox, C.L.; Ginis, K.A.; Petruzzello, S.J. The Psychology of Exercise: Integrating Theory and Practice; Taylor & Francis: Abingdon, UK, 2016; Available online: https://www.amazon.com/Psychology-Exercise-Integrating-Theory-Practice/dp/1621590062 (accessed on 27 January 2022).
- Gibson-Moore, H. UK Chief Medical Officers’ physical activity guidelines. What’s new and how can we get people more active? Nutr. Bull. 2019, 44, 320–328. [Google Scholar] [CrossRef]
- Blondell, S.J.; Hammersley-Mather, R.; Veerman, J.L. Does physical activity prevent cognitive decline and dementia? A systematic review and meta-analysis of longitudinal studies. BMC Public Health 2014, 14, 510. [Google Scholar] [CrossRef] [Green Version]
- Sofi, F.; Valecchi, D.; Bacci, D.; Abbate, R.; Gensini, G.; Casini, A. Physical activity and risk of cognitive decline: A meta-analysis of prospective studies. J. Intern. Med. 2011, 269, 107–117. [Google Scholar] [CrossRef]
- Teri, L.; Gibbons, L.E.; McCurry, S.M. Exercise plus behavioral management in patients with Alzheimer disease: A randomized controlled trial. JAMA 2013, 290, 2015–2022. [Google Scholar] [CrossRef]
- Paillard, T.; Rolland, Y.; de Souto Barreto, P. Protective effects of physical exercise in Alzheimer’s disease and Parkinson’s disease: A narrative review. J. Clin. Neurol 2015, 11, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Sinaei, M.; Alaei, H.; Nazem, F.; Kargarfard, M.; Feizi, A.; Talebi, A.; Esmaeili, A.; Nobari, H.; Pérez-Gómez, J. Endurance exercise improves avoidance learning and spatial memory, through changes in genes of GABA and relaxin-3, in rats. Biochem. Biophys. Res. Commun. 2021, 566, 204–210. [Google Scholar] [CrossRef]
- Rovio, S.; Kareholt, I.; Viitanen, M.; Winblad, B.; Tuomilehto, J.; Soininen, H. Work-related physical activity and the risk of dementia and Alzheimer’s disease. Int. J. Psychiatry 2007, 22, 874–882. [Google Scholar] [CrossRef]
- Kemoun, G.; Thibaud, M.; Roumagne, N.; Carette, P.; Albinet, C.; Toussaint, L. Effects of a physical training programme on cognitive function and walking efficiency in elderly persons with dementia. Dement. Geriatr. Cogn. Disord. 2010, 29, 109–114. [Google Scholar] [CrossRef]
- Krause, M.; Rodrigues-Krause, J.; O’Hagan, C.; Medlow, P.; Davison, G.; Susta, D. The effects of aerobic exercise training at two different intensities in obesity and type 2 diabetes: Implications for oxidative stress, low-grade inflammation and nitric oxide production. Eur. J. Appl. Physiol. 2014, 114, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Hamman, R.F.; Wing, R.R.; Edelstein, S.L.; Lachin, J.M.; Bray, G.A.; Delahanty, L. Effect of weight loss with lifestyle intervention on risk of diabetes. Diabetes Care 2006, 26, 2102–2107. [Google Scholar] [CrossRef] [Green Version]
- Adlard, P.A.; Perreau, V.M.; Pop, V.; Cotman, C.W. Voluntary exercise decreases amyloid load in a transgenic model of Alzheimer’s disease. J. Neurosci. 2005, 25, 4217–4221. [Google Scholar] [CrossRef]
- Kim, B.K.; Shin, M.S.; Kim, C.J.; Baek, S.B.; Ko, Y.C.; Kim, Y.P. Treadmill exercise improves short-term memory by enhancing neurogenesis in amyloid beta-induced Alzheimer disease rats. J. Exerc. Rehabil. 2014, 10, 2–8. [Google Scholar] [CrossRef]
- Um, H.; Kang, E.; Leem, Y.; Cho, I.; Yang, C.; Chae, K. Exercise training acts as a therapeutic strategy for reduction of the pathogenic phenotypes for Alzheimer’s disease in an NSE/APP-transgenic model. Int. J. Mol. 2008, 4, 529–539. [Google Scholar]
- Guyatt, G.H.; Pugsley, S.O.; Sullivan, M.J.; Thompson, P.J.; Berman, L.; Jones, N.L.; Fallen, E.L.; Taylor, D.W. Effect of encouragement on walking test performance. Thorax 1984, 93, 812–822. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412b-4. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall risk index for elderly patients based on number of chronic disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef]
- Canbek, J.; Fulk, G.; Nof, L.; Echternach, J. Test-retest reliability and construct validity of the Tinetti performance-oriented mobility assessment in people with stroke. J. Neurol. Phys. Ther. 2013, 37, 14–19. [Google Scholar] [CrossRef]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Pub. Health 1992, 2, S7–S11. [Google Scholar]
- Enright, P.L.; Sherrill, D.L. Reference equations for the six-minute walk in healthy adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troosters, T.; Gosselink, R.; Decramer, M. Six minute walking distance. Eur. Respir. J. 1999, 14, 270–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stiliwell, K.M.; Forman, D.E.; McElwain, D.; Simpson, C.; Garber, C.E. The 6 minutes walk test for evaluation of functional capacity in elderly adults. Med. Sci. Sport Exerc. 1996, 28, S152. [Google Scholar] [CrossRef]
- Guerra-Balic, M.; Oviedo, G.R.; Javierre, C.; Fortuño, J.; Barnet-López, S.; Niño, O. Reliability and validity of the 6-min walk test in adults and seniors with intellectual disabilities. Res. Dev. Disabil. 2015, 47, 144–153. [Google Scholar] [CrossRef]
- Lord, S.R.; Menz, H.B. Physiologic, psychologic, and health predictors of 6-minute walk performance in older people. Arch. Phys. Med. Rehabil. 2002, 83, 907–911. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Verghese, J.; Kuslansky, G.; Holtzer, R.; Katz, M.; Xue, X.N.; Buschke, H. Walking while talking: Effect of task prioritization in the elderly. Arch. Phys. Med. Rehabil. 2007, 88, 50–53. [Google Scholar] [CrossRef] [Green Version]
- Anwar, Y.A.; Giacco, S.; McCabe, E.J.; Tendler, B.E.; White, W.B. Evaluation of the efficacy of the Omron HEM-737 IntelliSense device for use on adults according to the recommendations of the Association for the Advancement of Medical Instrumentation. Blood Press. Monit. 1998, 3, 261–265. [Google Scholar]
- Albinet, C.; Bernard, P.L.; Palut, Y. Attentional control of postural stability in institutionalised elderly people: Effects of a physical exercise program. Ann. Readapt. Med. Phys. 2006, 9, 625–631. [Google Scholar] [CrossRef]
- Van Doorn, C.; Gruber-Baldini, A.L.; Zimmerman, S.; Hebel, J.R.; Port, C.; Baumgarten, M.; Quinn, C.C.; Taler, G.; May, C.; Magaziner, J. Epidemiology of Dementia in Nursing Home Research Group: Dementia as a risk factor for falls and fall injuries among nursing home residents. J. Am. Geriatr. Soc. 2003, 51, 1213–1218. [Google Scholar] [CrossRef]
- Li, X.; Guo, R.; Wei, Z.; Jia, J.; Wei, C. Effectiveness of Exercise Programs on Patients with Dementia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BioMed Res. Int. 2019, 2019, 2308475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, L.E.; Padilla, R. Effectiveness of interventions to prevent falls in people with Alzheimer’s disease and related dementias. Am. J. Occup. Ther. 2011, 65, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1094–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manckoundia, P.; Taroux, M.; Kubicki, A.; Mourey, F. Impact of ambulatory physiotherapy on motor abilities of elderly subjects with Alzheimer’s disease. Geriatr. Gerontol. Int. 2014, 14, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Toulotte, C.; Thévenon, A.; Fabre, C. Effects on training on static and dynamic balance in elderly subjects who have a fall or not. Ann. Readapt. Med. Phys. 2004, 47, 604–610. [Google Scholar] [CrossRef]
- De Andrade, L.P.; Gobbi, L.T.; Coelho, F.G.; Christofoletti, G.; Costa, J.L.; Stella, F. Benefits of multimodal exercise intervention for postural control and frontal cognitive functions in individuals with Alzheimer’s disease: A controlled trial. J. Am. Geriatr. Soc. 2013, 61, 1919–1926. [Google Scholar] [CrossRef]
- Yao, L.; Giordani, B.J.; Algase, D.L.; You, M.; Alexander, N.B. Fall Risk-Relevant Functional Mobility Outcomes in Dementia Following Dyadic Tai Chi Exercise. West. J. Nurs. Res. 2012, 35, 281–296. [Google Scholar] [CrossRef] [Green Version]
- Vitório, R.; Teixeira-Arroyo, C.; Lirani-Silva, E.; Barbieri, F.A.; Caetano, M.J.D.; Gobbi, S. Effects of 6-month, multimodal exercise program on clinical and gait parameters of patients with idiopathic Parkinson’s disease: A pilot study. ISRN Neurol. 2011, 2011, 714947. [Google Scholar] [CrossRef] [Green Version]
- Fasola, J.; Mataric, M.J. Using socially assistive human–robot interaction to motivate physical exercise for older adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Gras, L.Z.; Kanaan, S.F.; McDowd, J.M.; Colgrove, Y.M.; Burns, J.; Pohl, P.S. Balance and gait of adults with very mild Alzheimer disease. J. Geriatr. Phys. 2015, 38, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [PubMed] [Green Version]
- Steinberg, M.; Leoutsakos, J.S.; Podewils, L.J.; Lyketsos, C. Evaluation of home-based exercise program in the treatment of Alzheimer’s disease: The maximizing independence in dementia (MIND) study. Int. J. Geriatr. Psychiatry 2009, 24, 680–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, T.; Makizako, H.; Shimada, H.; Yoshida, D.; Tsutsumimoto, K.; Sawa, R.; Misu, S.; Suzuki, T. Effects of multicompo-nent exercise on spatial-temporal gait parameters among the elderly with amnestic mild cognitive impairment (aMCI): Preliminary results from a randomized controlled trial (RCT). Arch. Gerontol. Geriatr. 2013, 56, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Schwenk, M.; Zieschang, T.; Oster, P.; Hauer, K. Dual-task performances can be improved in patients with dementia: A randomized controlled trial. Neurology 2010, 74, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Santana-Sosa, E.; Barriopedro, M.I.; Lopez-Mojares, L.M.; Perez, M.; Lucia, A. Exercise training is beneficial for Alz-heimer’s patients. Int. J. Sports Med. 2008, 29, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Suttanon, P.; Hill, K.D.; Said, C.M.; Williams, S.B.; Byrne, K.N.; LoGiudice, D.; Lautenschlager, N.T.; Dodd, K.J. Feasi-bility, safety and preliminary evidence of the effectiveness of a home-based exercise programme for older people with Alzheimer’s disease: A pilot randomized controlled trial. Clin. Rehabil. 2013, 27, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Pillard, F.; Klapouszczak, A.; Reynish, E.; Thomas, D.; Andrieu, S.; Rivière, D.; Vellas, B. Exercise program for nursing home residents with Alzheimer’s disease: A 1-year randomized, controlled trial. J. Am. Geriatr. Soc. 2007, 55, 158–165. [Google Scholar] [CrossRef]
- Hill, K.D.; LoGiudice, D.; Lautenschlager, N.T.; Said, C.M.; Dodd, K.J.; Sut¬tanon, P. Effectiveness of balance training exercise in people with mild to moderate severity Alzheimer’s disease: Protocol for a randomised trial. BMC Geriatr. 2009, 9, 29. [Google Scholar] [CrossRef] [Green Version]
- Durstine, J.L. Effect of aerobic exercise training on serum level of high density lipoprotein cholesterol. Clin. J. Sport Med. 2008, 18, 107–108. [Google Scholar] [CrossRef]
- Adamopoulos, S.; Schmid, J.P.; Dendale, P.; Poerschke, D.; Hansen, D.; Dritsas, A. Combined aerobic/inspiratory muscle training vs. aerobic training in patients with chronic heart failure: The Vent-HeFT trial: A European prospective multicentre randomized trial. Eur. J. Heart Fail. 2014, 16, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Kraus, W.E.; Houmard, J.A.; Dusha, B.D.; Knetzger, K.J.; Wharton, M.B.; McCartnet, J.S. Effect of the amount and intensi-ty of exercice on plasma lipoprotein. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.W.; Roberts, M.D.; Church, T.S. Toward exercise as personalized medicine. Sports Med. 2013, 43, 157–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall Population | Control Group | Intervention Group |
|---|---|---|---|
| Patients (N) | 20 | 9 | 11 |
| Years | 84 ± 3.0 | 86 ± 2.6 | 84 ± 3.1 |
| Body Mass Index (kg/m2) | 26 ± 1.5 | 25 ± 1.3 | 27 ± 1.1 |
| Higher education level | 15 | 7 | 8 |
| Alcohol use | 7 | 3 | 4 |
| Comorbidities | 18 | 8 | 10 |
| Variable | Control Group | Delta Change (%) | Intervention Group | Delta Change (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Before | After | Before | After | Group | Time | Interaction | |||
| Berg Balance Scale | 42.22 ± 2.68 | 41.00 ± 1.73 * | 2.8 | 41.92 ±2.78 | 43.25 ± 2.14 * | 3.17 | 0.306 | 0.914 | 0.021 |
| Tinetti test | 12.67 ± 2.24 | 13.56 ± 0.88 * | 7.02 | 12.17 ± 1.80 | 18.67 ± 1.07 * | 53.40 | <0.001 | <0.001 | <0.001 |
| 6-min walking test | 115.89 ± 9.53 | 150.67 ± 14.38 * | 30.01 | 111.00 ± 21.39 | 169.33 ± 16.51 * | 52.50 | 0.273 | <0.001 | 0.008 |
| Time up and go | 21.78 ± 2.82 | 23.33 ± 1.66 * | 7.11 | 23.50 ± 3.48 | 20.08 ± 1.51 * | −14.50 | 0.425 | 0.141 | 0.001 |
| Walking and Talking | 0.56 ± 0.53 | 0.56 ± 0.53 | 0 | 0.58 ± 0.67 | 1.25 ± 0.62 * | 115% | <0.001 | <0.001 | <0.001 |
| Variable | Control Group | Intervention Group | p-Value |
|---|---|---|---|
| Red blood cell count (×109/L) | 3.86 ± 0.57 | 4.11 ± 0.28 | 0.196 |
| White blood cell count (×109/L) | 6284.44 ± 545.85 | 6717.75 ± 552.13 | 0.090 |
| Hemoglobin (g/dL) | 13.52 ± 0.94 | 13.91 ± 0.61 | 0.262 |
| Platelet count | 279.08 ± 47.79 | 277.33 ± 28.67 | 0.918 |
| Hematocrit (%) | 43.35 ± 2.68 | 42.81 ± 2.44 | 0.635 |
| Triglycerides (mg/dL) | 2.14 ± 0.30 | 42.81 ± 2.44 | <0.001 |
| Cholesterol (mg/dL) | 4.12 ± 0.60 | 3.76 ± 0.88 | 0.310 |
| Total bilirubin (mg/dL) | 8.79 ± 0.89 | 8.76 ± 0.63 | 0.917 |
| Aspartate transaminase (ASAT) | 14.44 ± 1.42 | 14.50 ± 1.98 | 0.944 |
| Alanine transaminase (ALAT) | 12.00 ± 1.12 | 12.17 ± 1.47 | 0.780 |
| Blood pressure (mmHg) | 85.44 ± 6.04 | 84.88 ± 4.96 | 0.815 |
| Creatinine (mg/dL) | 138.44 ± 4.98 | 117.42 ± 17.73 | 0.003 |
| Urea (mg/dL) | 4.61 ± 0.81 | 4.90 ± 1.13 | 0.525 |
| Glucose (mg/dL) | 4.01 ± 0.88 | 3.93 ± 0.78 | 0.812 |
| Sodium (Na) (mEq/L) | 140.78 ± 9.67 | 142.50 ± 7.79 | 0.656 |
| Calcium (Ca) (mEq/L) | 3.68 ± 1.10 | 2.66 ± 0.54 | 0.011 * |
| Potassium (K) (mEq/L) | 4.27 ± 1.03 | 3.42 ± 0.70 | 0.036 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chortane, O.G.; Hammami, R.; Amara, S.; Chortane, S.G.; Suzuki, K.; Oliveira, R.; Nobari, H. Effects of Multicomponent Exercise Training Program on Biochemical and Motor Functions in Patients with Alzheimer’s Dementia. Sustainability 2022, 14, 4112. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074112
Chortane OG, Hammami R, Amara S, Chortane SG, Suzuki K, Oliveira R, Nobari H. Effects of Multicomponent Exercise Training Program on Biochemical and Motor Functions in Patients with Alzheimer’s Dementia. Sustainability. 2022; 14(7):4112. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074112
Chicago/Turabian StyleChortane, Oussama Gaied, Raouf Hammami, Sofiene Amara, Sabri Gaied Chortane, Katsuhiko Suzuki, Rafael Oliveira, and Hadi Nobari. 2022. "Effects of Multicomponent Exercise Training Program on Biochemical and Motor Functions in Patients with Alzheimer’s Dementia" Sustainability 14, no. 7: 4112. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074112