
Self-Rated Health and Socioeconomic Status in Old Age: The Role of Gender and the Moderating Effect of Time and Welfare Regime in Europe


Abstract
:1. Introduction
2. Literature Review
3. Research Objectives
4. Materials and Methods
4.1. Sample
4.2. Variables
4.2.1. Dependent Variable
4.2.2. Independent Variables
4.3. Data Analysis
5. Results
5.1. Descriptive Statistics
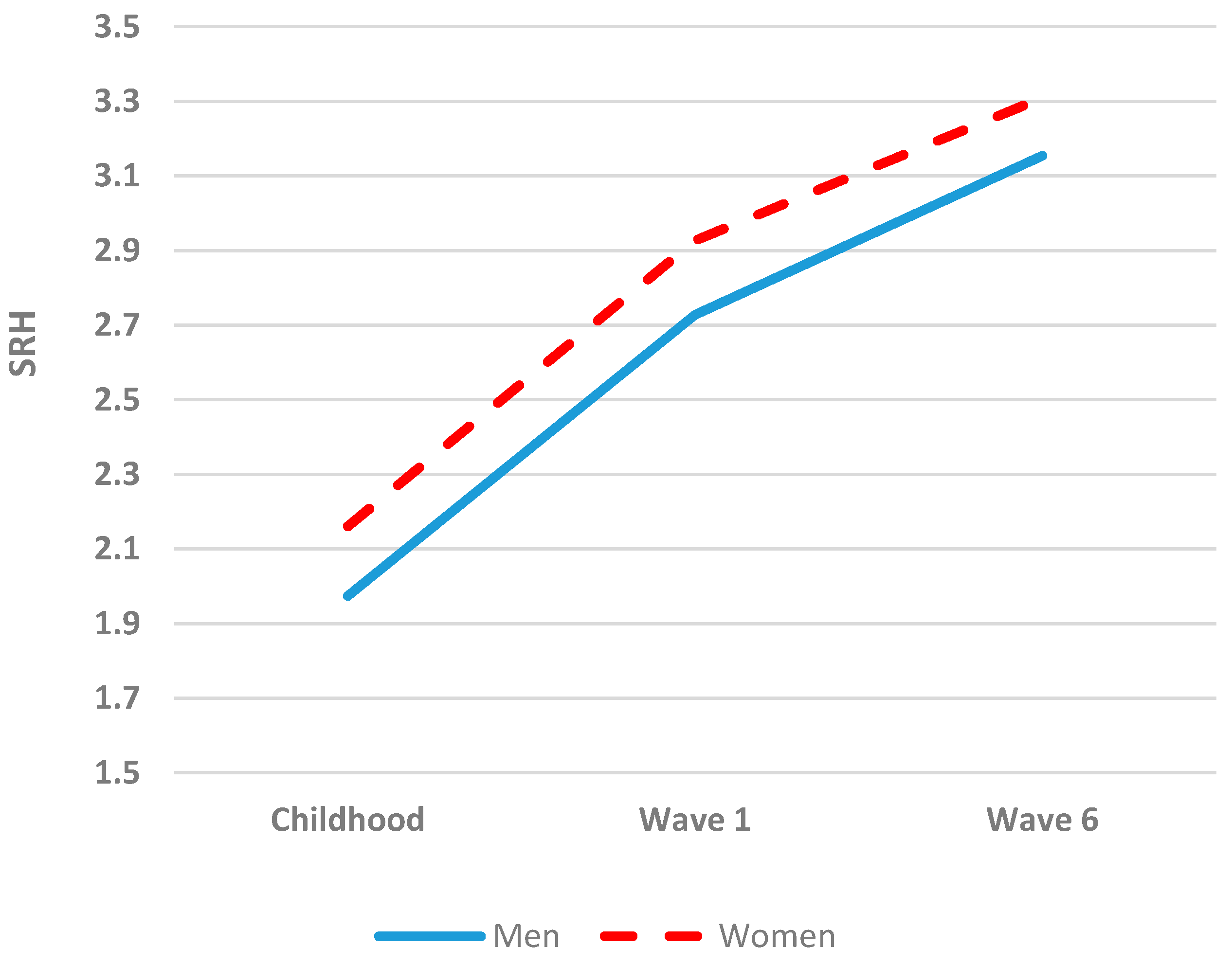
5.2. Analyzing Gender Differences in SRH
5.3. Analyzing the Association between Socioeconomic Status and SRH
5.4. SRH and Socioeconomic Status over Time
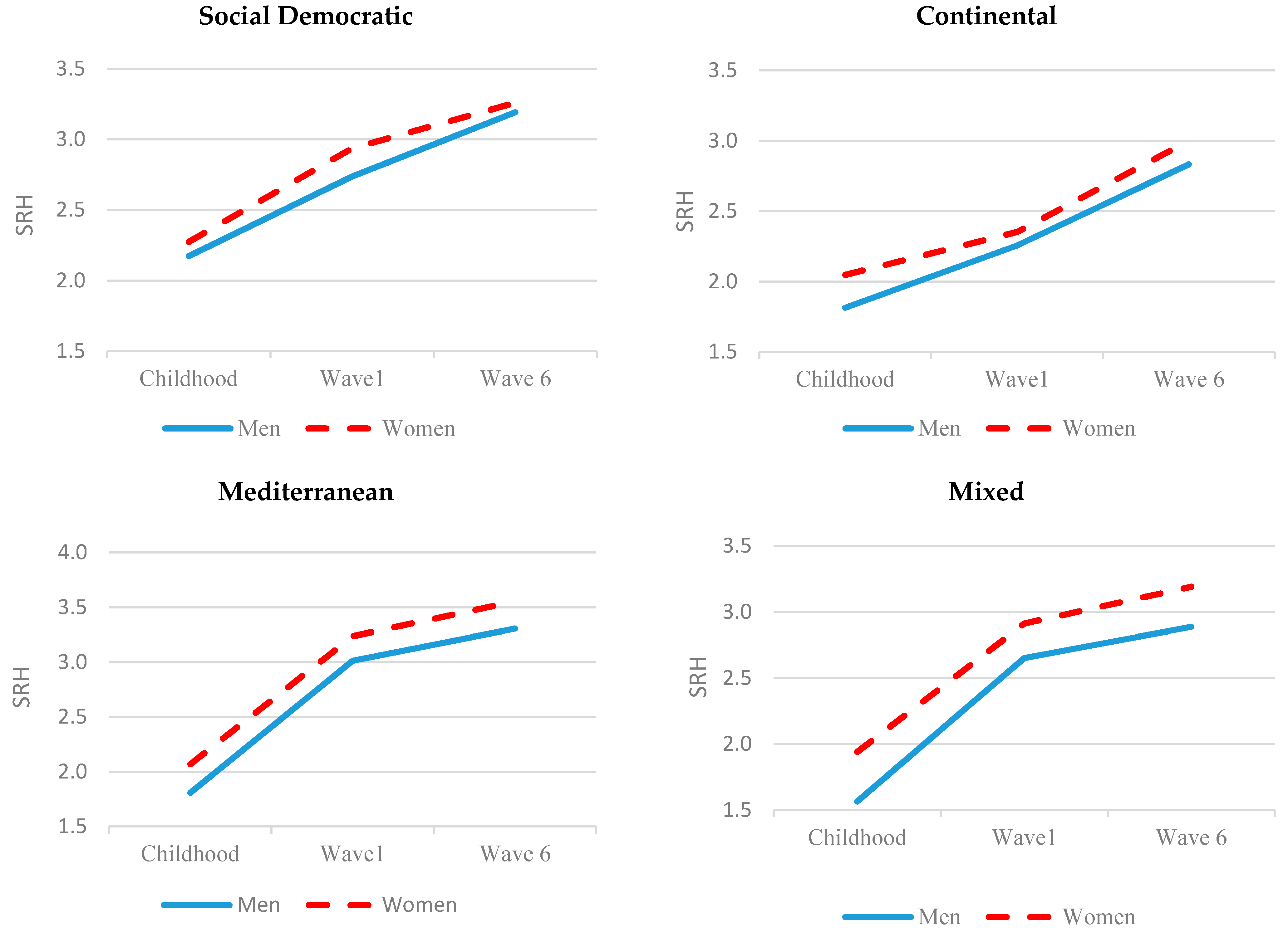
5.5. SRH and Socioeconomic Status within a Welfare State Regime
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathers, C.D.; Stevens, G.A.; Boerma, T.; White, R.A.; Tobias, M.I. Causes of international increases in older age life expectancy. Lancet 2015, 385, 540–548. [Google Scholar] [CrossRef]
- Macintyre, S.; Hunt, K.; Sweeting, H. Gender differences in health: Are things really as simple as they seem? Soc. Sci. Med. 1996, 42, 617–624. [Google Scholar] [CrossRef]
- Idler, E.L.; Benyamini, Y. Self-Rated Health and Mortality: A Review of Twenty-Seven Community Studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [Green Version]
- Franks, P.; Gold, M.R.; Fiscella, K. Sociodemographics, self-rated health, and mortality in the US. Soc. Sci. Med. 2003, 56, 2505–2514. [Google Scholar] [CrossRef]
- Stenholm, S.; Westerlund, H.; Head, J.; Hyde, M.; Kawachi, I.; Pentti, J.; Kivimäki, M.; Vahtera, J. Comorbidity and Functional Trajectories From Midlife to Old Age: The Health and Retirement Study. J. Gerontol. Ser. A 2014, 70, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Szwarcwald, C.L.; Souza-Júnior, P.R.B.D.; Esteves, M.A.P.; Damacena, G.N.; Viacava, F. Socio-demographic determinants of self-rated health in Brazil. Cad. De Saúde Pública 2005, 21, S54–S64. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Health and Ageing: A Discussion Paper. Available online: http://apps.who.int/iris/bitstream/10665/66682/1/WHO_NMH_HPS_01.1.pdf (accessed on 24 March 2022).
- Stoller, M.A.; Stoller, E.P. Perceived income adequacy among elderly retirees. J. Appl. Gerontol. 2003, 22, 230–251. [Google Scholar] [CrossRef]
- Arber, S.; Cooper, H. Gender differences in health in later life: The new paradox? Soc. Sci. Med. 1999, 48, 61–76. [Google Scholar] [CrossRef]
- Kunst, A.E.; Geurts, J.J.; Berg, J.V.D. International variation in socioeconomic inequalities in self reported health. J. Epidemiol. Community Health 1995, 49, 117–123. [Google Scholar] [CrossRef] [Green Version]
- van Kippersluis, H.; O’Donnell, O.; van Doorslaer, E.; Van Ourti, T. Socioeconomic differences in health over the life cycle in an Egalitarian country. Soc. Sci. Med. 2010, 70, 428–438. [Google Scholar] [CrossRef] [Green Version]
- Leão, T.; Campos-Matos, I.; Bambra, C.; Russo, G.; Perelman, J. Welfare states, the Great Recession and health: Trends in educational inequalities in self-reported health in 26 European countries. PLoS ONE 2018, 13, e0193165. [Google Scholar] [CrossRef] [Green Version]
- Stronks, K.; Van De Mheen, H.; Bos, J.V.D.; MacKenbach, J.P. Smaller Socioeconomic Inequalities in Health among Women: The Role of Employment Status. Int. J. Epidemiol. 1995, 24, 559–568. [Google Scholar] [CrossRef]
- Newman, A.B.; Brach, J.S. Gender Gap in Longevity and Disability in Older Persons. Epidemiol. Rev. 2001, 23, 343–355. [Google Scholar] [CrossRef] [Green Version]
- Dykstra, P.A. Cross-national Differences in Intergenerational Family Relations: The Influence of Public Policy Arrangements. Innov. Aging 2018, 2, igx032. [Google Scholar] [CrossRef] [Green Version]
- Eikemo, T.A.; Bambra, C.; Judge, K.; Ringdal, K. Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2281–2295. [Google Scholar] [CrossRef] [Green Version]
- Lynn, J.; Adamson, D. Living Well at the End of Life: Adapting Health Care to Serious Chronic Illness in Old Age; Rand Corporation: Santa Monica, CA, USA, 2003. [Google Scholar]
- Linn, B.S.; Linn, M.W. Objective and self-assessed health in the old and very old. Soc. Sci. Med. Part A Med. Psychol. Med. Sociol. 1980, 14, 311–315. [Google Scholar]
- DeSalvo, K.B.; Bloser, N.; Reynolds, K.; He, J.; Muntner, P. Mortality prediction with a single general self-rated health question. A meta-analysis. J. Gen. Intern. Med. 2006, 21, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Kawada, T. Self-rated health and life prognosis. Arch. Med Res. 2003, 34, 343–347. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2015: OECD Indicators; OECD Publishing: Paris, France, 2015. [Google Scholar]
- McFadden, E.; Luben, R.; Bingham, S.; Wareham, N.; Kinmonth, A.-L.; Khaw, K.-T. Social inequalities in self-rated health by age: Cross-sectional study of 22 457 middle-aged men and women. BMC Public Health 2008, 8, 230. [Google Scholar] [CrossRef] [Green Version]
- Henchoz, K.; Cavalli, S.; Girardin, M. Health perception and health status in advanced old age: A paradox of association. J. Aging Stud. 2008, 22, 282–290. [Google Scholar] [CrossRef]
- Calasanti, T. Feminist Gerontology and Old Men. J. Gerontol. 2004, 59, S305–S314. [Google Scholar] [CrossRef] [Green Version]
- Freixas, A.; Luque, B.; Reina, A. Critical Feminist Gerontology: In the Back Room of Research. J. Women Aging 2012, 24, 44–58. [Google Scholar] [CrossRef]
- Hooyman, N.; Browne, C.V.; Ray, R.; Richardson, V. Feminist Gerontology and the Life Course. Gerontol. Geriatr. Educ. 2002, 22, 3–26. [Google Scholar] [CrossRef]
- Liu, Y.; Arai, A.; Kanda, K.; Lee, R.B.; Glasser, J.; Tamashiro, H. Gender gaps in life expectancy: Generalized trends and negative associations with development indices in OECD countries. Eur. J. Public Health 2013, 23, 563–568. [Google Scholar] [CrossRef] [Green Version]
- McMullin, J.A.; Cairney, J. Self-esteem and the intersection of age, class, and gender. J. Aging Stud. 2004, 18, 75–90. [Google Scholar] [CrossRef]
- Anson, O.; Paran, E.; Neumann, L.; Chernichovsky, D. Gender differences in health perceptions and their predictors. Soc. Sci. Med. 1993, 36, 419–427. [Google Scholar] [CrossRef]
- Adler, N.E.; Boyce, T.; Chesney, M.A.; Cohen, S.; Folkman, S.; Kahn, R.L.; Syme, S.L. Socioeconomic status and health: The challenge of the gradient. Am. Psychol. 1994, 49, 15. [Google Scholar] [CrossRef]
- Deaton, A.S.; Paxson, C.H. Aging and inequality in income and health. Am. Econ. Rev. 1998, 88, 248–253. [Google Scholar]
- Smith, J.P.; Kington, R. Demographic and economic correlates of health in old age. Demography 1997, 34, 159–170. [Google Scholar] [CrossRef]
- Huisman, M.; Read, S.; Towriss, C.A.; Deeg, D.J.H.; Grundy, E. Socioeconomic Inequalities in Mortality Rates in Old Age in the World Health Organization Europe Region. Epidemiol. Rev. 2013, 35, 84–97. [Google Scholar] [CrossRef] [Green Version]
- Esping-Andersen, G. The Three Political Economies of the Welfare State. Int. J. Sociol. 1990, 20, 92–123. [Google Scholar] [CrossRef] [Green Version]
- Esping-Andersen, G. Social Foundations of Postindustrial Economies; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Katz, R.; Lowenstein, A.; Halperin, D.; Tur-Sinai, A. Generational Solidarity in Europe and Israel. Can. J. Aging/La Rev. Can. Du Vieil. 2015, 34, 342–355. [Google Scholar] [CrossRef] [PubMed]
- Srakar, A.; Hrast, M.F.; Hlebec, V.; Majcen, B. Social exclusion, welfare-state regime and unmet long-term care need: Evidence from SHARE. Ageing Eur. Supporting Policies Incl. Soc. 2015, 17, 189. [Google Scholar]
- Wallace, L.M.K.; Theou, O.; Pena, F.; Rockwood, K.; Andrew, M.K. Social vulnerability as a predictor of mortality and disability: Cross-country differences in the survey of health, aging, and retirement in Europe (SHARE). Aging Clin. Exp. Res. 2015, 27, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Bambra, C.; Pope, D.; Swami, V.; Stanistreet, D.; Roskam, A.; Kunst, A.; Scott-Samuel, A. Gender, health inequalities and welfare state regimes: A cross-national study of 13 European countries. J. Epidemiol. Community Health 2009, 63, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Silverstein, M.; Tur-Sinai, A.; Lewin-Epstein, N. Intergenerational Support of Older Adults by the ‘Mature’ Sandwich Generation: The Relevance of National Policy Regimes. Theor. Inq. Law 2020, 21, 55–76. [Google Scholar] [CrossRef] [Green Version]
- Bambra, C.; Eikemo, T.A. Welfare state regimes, unemployment and health: A comparative study of the relationship between unemployment and self-reported health in 23 European countries. J. Epidemiol. Community Health 2008, 63, 92–98. [Google Scholar] [CrossRef] [Green Version]
- Majeed, T.; Forder, P.; Mishra, G.; Byles, J. Women, Work, and Illness: A Longitudinal Analysis of Workforce Participation Patterns for Women Beyond Middle Age. J. Womens Health 2015, 24, 455–465. [Google Scholar] [CrossRef]
- World Health Organization. Women, Ageing and Health: A Framework for Action: Focus on Gender. Available online: https://apps.who.int/iris/bitstream/handle/10665/43810/9789241563529_eng.pdf?sequence=1&isAllowed=y (accessed on 24 March 2022).
- Liu, C.; Zhang, M.; Zheng, M.; Chen, Y. Step-by-Step Regression: A More Efficient Alternative for Polynomial Multiple Linear Regression in Stream Cube. In Proceedings of the Pacific-Asia Conference on Knowledge Discovery and Data Mining, Seoul, Korea, 30 April–2 May 2003; Springer: Berlin/Heidelberg, Germany, 2003; pp. 437–448. [Google Scholar]
- Andreev, A.O.; Demina, N.; Nefedyev, Y.; Demin, S.A.; Zagidullin, A.A. Modeling of the physical selenocentric surface using modern satellite observations and harmonic analysis methods. J. Phys. Conf. Ser. 2018, 1038, 012003. [Google Scholar] [CrossRef]
- Schaie, K.W. What Can We Learn From Longitudinal Studies of Adult Development? Res. Hum. Dev. 2005, 2, 133–158. [Google Scholar] [CrossRef] [Green Version]
- Nelson, E.A.; Dannefer, D. Aged Heterogeneity: Fact or Fiction? The Fate of Diversity in Gerontological Research. Gerontologist 1992, 32, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- Juster, F.T.; Suzman, R. An Overview of the Health and Retirement Study. J. Hum. Resour. 1995, 30, S7. [Google Scholar] [CrossRef]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. (Version: 6.0.0); SHARE-ERIC: Munich, Germany, 2017. [Google Scholar]
- Carmel, S.; Tur-Sinai, A. Cognitive decline among European retirees: Impact of early retirement, nation-related and personal characteristics. Ageing Soc. 2021, 1–27. [Google Scholar] [CrossRef]
- Tur-Sinai, A.; Casanova, G.; Lamura, G. Changes in the Provision of Family Care to Frail Older People in Familistic Welfare States: Lessons From Israel and Italy. J. Aging Health 2020, 32, 972–986. [Google Scholar] [CrossRef]
- Tur-Sinai, A.; Spivak, A. How Generous are Societies Toward Their Elderly? A European Comparative Study of Replacement Rates, Well-Being and Economic Adequacy. Soc. Indic. Res. 2021, 1–35. [Google Scholar] [CrossRef]
- Tur-Sinai, A.; Teti, A.; Rommel, A.; Hlebec, V.; Yghemonos, S.; Lamura, G. Cross-national data on informal caregivers of older people with long-term care needs in the European population: Time for a more coordinated and comparable approach. J. Biosoc. Sci. 2022, 5, 1–5. [Google Scholar] [CrossRef]
- Bergman, M.; De Luca, G.; Scherpenzeel, A. Sampling Design and Weighting Strategies. In SHARE Wave 6: Panel Innovations and Collecting Dried Blood Spots; Malter, F., Börsch-Supan, A., Eds.; Munich Center for the Economics of Aging (MEA): Munich, Germany, 2017. [Google Scholar]
- Murata, C.; Kondo, T.; Tamakoshi, K.; Yatsuya, H.; Toyoshima, H. Determinants of self-rated health: Could health status explain the association between self-rated health and mortality? Arch. Gerontol. Geriatr. 2006, 43, 369–380. [Google Scholar] [CrossRef]
- Tur-Sinai, A.; Soskolne, V. Socioeconomic status and health behaviors as predictors of changes in self-rated health among older persons in Israel. Health Soc. Care Community 2021, 29, 1461–1472. [Google Scholar] [CrossRef]
- Dwyer, D.S.; Mitchell, O.S. Health problems as determinants of retirement: Are self-rated measures endogenous? J. Health Econ. 1999, 18, 173–193. [Google Scholar] [CrossRef] [Green Version]
- Jylhä, M.; Guralnik, J.M.; Ferrucci, L.; Jokela, J.; Heikkinen, E. Is Self-Rated Health Comparable across Cultures and Genders? J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 1998, 53, S144–S152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossey, J.M.; Shapiro, E. Self-rated health: A predictor of mortality among the elderly. Am. J. Public Health 1982, 72, 800–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, S.L.; Kogan, I. The International Standard Classification of Education 1997: Challenges in the Application to National Data and the Implementation in Cross-National Surveys in The International Standard Classification of Education (ISCED-97). An Evaluation of Content and Criterion Validity for 15 European Countries; MZES: Mannheim, Germany, 2018; pp. 13–46. [Google Scholar]
- UNESCO. International Standard Classification of Education-ISCED 1997; UNESCO: Montreal, QC, Canada, 1997. [Google Scholar]
- Castro-Costa, E.; Dewey, M.; Stewart, R.; Banerjee, S.; Huppert, F.; Mendonca-Lima, C.; Büla, C.; Reisches, F.; Wancata, J.; Ritchie, K.; et al. Prevalence of depressive symptoms and syndromes in later life in ten European countries. Br. J. Psychiatry 2007, 191, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.; Bobak, M.; Murphy, M.; Rose, R.; Marmot, M. Socio-economic influences on self-rated health in Russian men and women—A life course approach. Soc. Sci. Med. 2005, 61, 2345–2354. [Google Scholar] [CrossRef] [Green Version]
- Tur-Sinai, A.; Halperin, D.; Ben David, N.; Lowenstein, A.; Katz, R. Cessation of Care for Frail Older Adults: Physical, Psychological and Economic Outcomes for Family Carers. Int. J. Environ. Res. Public Health 2022, 19, 3570. [Google Scholar] [CrossRef]
- McCullough, M.E.; Laurenceau, J.-P. Gender and the Natural History of Self-Rated Health: A 59-Year Longitudinal Study. Health Psychol. 2004, 23, 651–655. [Google Scholar] [CrossRef] [Green Version]
- Cesaretti, R.; Lobo, J.; Bettencourt, L.M.A.; Ortman, S.G.; Smith, M.E. Population-Area Relationship for Medieval European Cities. PLoS ONE 2016, 11, e0162678. [Google Scholar] [CrossRef] [Green Version]
- Ganguli, I.; Hausmann, R.; Viarengo, M. Gender Differences in Professional Career Dynamics: New Evidence from a Global Law Firm. Economica 2020, 88, 105–128. [Google Scholar] [CrossRef]
- Collins, C. Is Maternal Guilt a Cross-National Experience? Qual. Sociol. 2021, 44, 1–29. [Google Scholar] [CrossRef]
- Foster, L.; Walker, A. Gender and active ageing in Europe. Eur. J. Ageing 2013, 10, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Reynolds, M.C.; Palmer, S.B.; Barton, K.N. Supporting Active Aging for Persons with Severe Disabilities and Their Families Across the Life Course. Res. Pract. Pers. Sev. Disabil. 2019, 44, 211–223. [Google Scholar] [CrossRef]
- World Health Organization. A Framework for Action on Women, Ageing and Health (No. WHO/FCH/ALC/2008.1). Available online: https://apps.who.int/iris/bitstream/handle/10665/70713/WHO_FCH_ALC_2008.1_eng.pdf (accessed on 24 March 2022).



{kind=link}
{kind=link}
| Variable | Categories | Wave 1 | Wave 6 | F/X2 | |||
|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | ||||
| 45.22 | 54.78 | 45.22 | 54.78 | ||||
| Self-rated health—% | Excellent | 13.57 | 10.56 | 27.80 *** | 6.12 | 4.21 | 16.89 ** |
| Very good | 24.63 | 20.47 | 18.12 | 14.9 | |||
| Good | 41.10 | 40.54 | 38.35 | 37.56 | |||
| Fair | 16.78 | 22.54 | 29.02 | 32.32 | |||
| Poor | 3.92 | 5.89 | 8.39 | 11.01 | |||
| Age—mean (SD) | 65.2 (2.83) | 65.03 (2.77) | 2.66 | 75.87 (2.88) | 75.66 (2.81) | 3.58 | |
| Living with spouse—% | Yes | 85.2 | 71.7 | 109.70 *** | 78.3 | 57.9 | 205.90 *** |
| No | 14.80 | 28.3 | 28.70 | 42.1 | |||
| Children—mean (SD) | 2.41 (1.46) | 2.42 (1.54) | 0.05 | 2.39 (1.53) | 2.42 (1.54) | 0.29 | |
| Grandchildren—mean (SD) | 2.75 (3.13) | 3.41 (3.42) | 27.66 *** | 3.88 (3.50) | 4.16 (3.54) | 4.65 * | |
| Welfare regime—% | Social Democratic | 21.10 | 19.11 | 1.99 | |||
| Continental | 45.25 | 46.76 | |||||
| Mediterranean | 25.41 | 25.32 | |||||
| Mixed | 8.24 | 8.81 | |||||
| Education—% | University | 24.71 | 17.94 | 20.14 *** | 24.86 | 17.94 | 20.89 *** |
| High school | 42.27 | 44.43 | 42.27 | 44.62 | |||
| Elementary school | 33.02 | 37.63 | 32.86 | 37.44 | |||
| Employment status—% | Employed/self-emp. | 19.14 | 11.14 | 364.66 *** | 2.43 | 1.3 | 296.32 *** |
| Retired | 76.47 | 61.20 | 95.53 | 75.06 | |||
| Homemaker | 24.22 | 19.17 | |||||
| Unemployed | 4.39 | 3.43 | 2.04 | 4.47 | |||
| Make ends meet—% | Easily | 32.78 | 29.08 | 14.07 ** | 47.37 | 40.09 | 24.37 ** |
| Fairly easily | 35.53 | 32.71 | 29.49 | 29.21 | |||
| Some difficulty | 24.31 | 28.3 | 17.49 | 22.09 | |||
| Great difficulty | 7.37 | 9.91 | 5.65 | 8.61 | |||
| Net household income (ln) | 9.51 (2.52) | 9.19 (2.69) | 10.3 ** | 10.14 (1.04) | 9.89 (1.12) | 37.88 *** | |
| ADL—% | No ADL | 94.43 | 92.64 | 6.53 * | 86.40 | 84.37 | 1.62 |
| 1 ADL or more | 5.57 | 7.36 | 13.60 | 15.63 | |||
| Chronic diseases—mean (SD) | 1.39 (1.25) | 1.73 (1.48) | 41.58 *** | 1.96 (1.55) | 2.30 (1.67) | 31.01 *** | |
| Depression—mean (SD) | 1.58 (1.72) | 2.62 (2.22) | 186.5 *** | 1.96 (1.93) | 2.89 (2.31) | 132.31 *** | |
| Childhood health status—% | Excellent | 41.25 | 33.03 | 24.40 *** | |||
| Very good | 29.73 | 31.09 | |||||
| Good | 21.10 | 24.94 | |||||
| Fair | 6.12 | 8.55 | |||||
| Poor | 1.80 | 2.40 | |||||
| Variables | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 1 | Model 2 | Model 3 | Model 4 | |
| Education (Ref. university) | ||||||||
| High school | 1.363 * | 1.417 ** | 1.455 ** | 1.420 ** | 1.753 *** | 1.716 *** | 1.694 *** | 1.656 *** |
| Elementary school and less | 2.024 *** | 2.117 *** | 1.942 *** | 1.963 *** | 2.262 *** | 1.980 *** | 1.759 *** | 1.735 *** |
| Current job situation (Ref. employed/self-employed) | ||||||||
| Retired | 1.644 *** | 1.512 ** | 1.223 | 1.238 | 2.548 *** | 2.147 *** | 1.773 ** | 1.765 ** |
| Homemaker | 3.133 *** | 2.128 *** | 1.858 ** | 1.901 ** | ||||
| Unemployed | 1.885 * | 1.898 * | 1.417 | 1.491 | 4.753 *** | 4.006 *** | 2.345 ** | 2.364 ** |
| Make ends meet (Ref. easily) | ||||||||
| Fairly easily | 1.286 * | 1.221 | 1.198 | 1.199 | 1.350 * | 1.219 | 1.147 | 1.144 |
| Some difficulty | 2.200 *** | 1.874 *** | 1.491 ** | 1.506 ** | 2.780 *** | 2.280 *** | 1.748 ** | 1.736 *** |
| Great difficulty | 1.953 ** | 1.642 * | 1.095 | 1.057 | 4.035 *** | 3.234 *** | 1.798 ** | 1.776 ** |
| Net household income | 0.965 | 0.986 | 0.979 | 0.979 | 0.981 | 0.962 | 0.968 | 0.967 |
| Living with spouse | 0.772 | 0.876 | 0.871 | 0.959 | 1.058 | 1.056 | ||
| No. of children | 1.016 | 1.015 | 1.011 | 1.025 | 1.057 | 1.057 | ||
| No. of grandchildren | 0.972 | 0.971 | 0.974 | 1.001 | 0.975 | 0.975 | ||
| Welfare regime (Ref. Social Democratic) | ||||||||
| Continental | 2.362 *** | 2.623 *** | 1.922 ** | 2.149 *** | 2.079 *** | 1.749 ** | ||
| Mediterranean | 2.624 *** | 3.112 *** | 3.655 *** | 2.903 *** | 2.491 *** | 2.689 *** | ||
| Mixed | 2.630 ** | 2.285 ** | 3.710 *** | 1.445 | 1.455 | 1.827 | ||
| ADL | 5.677 *** | 5.595 *** | 4.629 *** | 4.668 *** | ||||
| Chronic diseases | 1.857 *** | 1.864 *** | 1.662 *** | 1.670 *** | ||||
| Depression | 1.222 *** | 1.223 *** | 1.235 *** | 1.235 *** | ||||
| Childhood health status | 1.285 *** | 1.276 *** | 1.203 *** | 1.201 *** | ||||
| Health expenditure | 1.318 * | 1.159 | ||||||
| Variables | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 1 | Model 2 | Model 3 | Model 4 | |
| Education (Ref. university) | ||||||||
| High school | 1.349 * | 1.342 * | 1.234 | 1.162 | 1.435 ** | 1.395 * | 1.074 | 1.036 |
| Elementary school and less | 1.666 *** | 1.734 *** | 1.417 * | 1.343 | 2.068 *** | 1.738 *** | 1.175 | 1.153 |
| Current job situation (Ref. employed/self-employed) | ||||||||
| Retired | 2.756 ** | 2.618 ** | 3.278 ** | 3.405 *** | 2.563 * | 2.563 ** | 1.969 | 2.114 |
| Homemaker | 2.822 * | 2.385 * | 1.907 | 2.144 | ||||
| Unemployed | 5.674 *** | 5.543 ** | 2.553 | 2.512 * | 9.677 *** | 8.816 *** | 3.275 * | 3.619 * |
| Make ends meet (Ref. easily) | ||||||||
| Fairly easily | 1.321 * | 1.240 | 1.222 | 1.248 | 1.258 * | 1.255 | 1.139 | 1.133 |
| Some difficulty | 1.662 *** | 1.541 ** | 1.148 | 1.177 | 2.275 *** | 2.242 *** | 1.363 * | 1.364 * |
| Great difficulty | 1.886 ** | 1.693 * | 1.087 | 1.101 | 3.801 *** | 3.577 *** | 1.861 ** | 1.829 * |
| Net household income | 0.948 | 0.960 | 1.055 | 1.045 | 0.925 | 0.917 | 0.954 | 0.948 |
| Living with spouse | 0.897 | 1.031 | 1.020 | 1.127 | 1.220 | 1.216 | ||
| No. of children | 0.991 | 0.948 | 0.949 | 0.998 | 0.983 | 0.982 | ||
| No. of grandchildren | 0.987 | 0.989 | 0.993 | 1.038 | 1.045 * | 1.044 * | ||
| Welfare regime (Ref. Social Democratic) | ||||||||
| Continental | 1.950 *** | 1.259 | 1.418 * | 1.504 ** | 0.861 | 0.942 | ||
| Mediterranean | 1.840 *** | 1.336 | 5.243 *** | 1.961 *** | 1.245 | 3.054 ** | ||
| Mixed | 1.750 ** | 1.291 | 16.565 *** | 0.959 | 0.661 | 3.728 * | ||
| ADL | 3.875 *** | 4.035 *** | 2.615 *** | 2.653 *** | ||||
| Chronic diseases | 1.368 *** | 1.383 *** | 1.405 *** | 1.418 *** | ||||
| Depression | 1.298 *** | 1.300 *** | 1.269 *** | 1.268 *** | ||||
| Childhood health status | 1.091 | 1.071 | 1.107 * | 1.102 * | ||||
| Self-rated health in Wave 1 | 2.071 *** | 2.065 *** | 2.002 *** | 2.003 *** | ||||
| Health expenditure | 2.076 *** | 1.626 ** | ||||||
| Variables | Social Democratic | Continental | Mediterranean | Mixed | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| Wave 1 | ||||||||
| Gender | 1.218 | 0.988 | 1.236 * | 0.898 | 1.724 *** | 0.956 | 0.863 | 0.539 |
| Education (Ref University) | ||||||||
| High school | 1.876 ** | 1.648 * | 1.611 *** | 1.743 *** | 1.320 | 1.354 | 1.102 | 1.236 |
| Elementary school and less | 2.049 ** | 1.965 ** | 1.953 *** | 1.921 *** | 2.581 ** | 2.139 * | 0.862 | 0.921 |
| Current job situation (Ref. employed/self-employed) | ||||||||
| Retired | 1.826 ** | 1.690 ** | 1.843 *** | 1.530 * | 1.242 | 0.944 | 1.443 | 1.009 |
| Homemaker | 1.803 | 1.500 | 1.959 ** | 1.456 | 1.096 | 1.112 | 1.894 | 1.405 |
| Unemployed | 6.800 *** | 6.737 *** | 2.183 * | 1.294 | 2.060 | 0.999 | 1.477 | 0.758 |
| Make ends meet (Ref. easily) | ||||||||
| Fairly easily | 1.524 * | 1.359 | 1.117 | 1.061 | 1.180 | 1.246 | 1.762 | 1.591 |
| Some difficulty | 4.354 *** | 3.206 *** | 1.407 * | 1.064 | 2.841 *** | 2.363 ** | 2.681 ** | 2.334 * |
| Great difficulty | 2.405 | 1.219 | 1.589 | 1.074 | 3.226 *** | 2.038 * | 3.523 ** | 1.895 |
| Net household income | 0.970 | 0.923 | 0.917 * | 0.928 | 1.060 | 1.050 | 0.970 | 0.960 |
| Wave 6 | ||||||||
| Gender | 1.282 | 1.024 | 0.940 | 0.686 | 1.763 *** | 1.173 | 0.788 | 0.650 |
| Education (Ref. university) | ||||||||
| High school | 1.181 | 1.030 | 1.487 *** | 1.503 ** | 1.692 | 1.326 | 0.952 | 0.865 |
| Elementary school and less | 1.783 ** | 1.925 ** | 1.657 *** | 1.478 ** | 2.687 ** | 2.361 * | 0.609 | 0.276 ** |
| Current job situation (Ref. employed/self-employed) | ||||||||
| Retired | 4.256 * | 5.588 ** | 1.256 | 1.176 | 3.897 | 3.633 | 2.552 * | 3.797 ** |
| Homemaker | 4.490 | 0.892 | 1.117 | 1.124 | 3.310 | 3.354 | 6.908 ** | 6.902 ** |
| Unemployed | 120.9 *** | 35.39 *** | 2.734 | 1.449 | 9.941 ** | 5.161 | 6.218 ** | 1.708 |
| Make ends meet (Ref. easily) | ||||||||
| Fairly easily | 1.116 | 1.027 | 1.209 | 1.060 | 1.043 | 1.082 | 1.920 * | 2.888 ** |
| Some difficulty | 1.576 | 1.295 | 1.806 *** | 1.314 | 1.547 * | 1.203 | 4.460 *** | 3.536 ** |
| Great difficulty | 1.269 | 0.940 | 3.649 *** | 1.788 * | 1.997 ** | 1.403 | 5.855 *** | 4.439 ** |
| Net household income | 0.891 | 0.829 | 0.809 *** | 0.815 ** | 1.075 | 1.136 * | 1.090 | 1.154 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tur-Sinai, A.; Paz, A.; Doron, I. Self-Rated Health and Socioeconomic Status in Old Age: The Role of Gender and the Moderating Effect of Time and Welfare Regime in Europe. Sustainability 2022, 14, 4240. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074240
Tur-Sinai A, Paz A, Doron I. Self-Rated Health and Socioeconomic Status in Old Age: The Role of Gender and the Moderating Effect of Time and Welfare Regime in Europe. Sustainability. 2022; 14(7):4240. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074240
Chicago/Turabian StyleTur-Sinai, Aviad, Amira Paz, and Israel Doron. 2022. "Self-Rated Health and Socioeconomic Status in Old Age: The Role of Gender and the Moderating Effect of Time and Welfare Regime in Europe" Sustainability 14, no. 7: 4240. https://0-doi-org.brum.beds.ac.uk/10.3390/su14074240