Transitioning from Unilateral to Bilateral Upper Limb Tremor Therapy for Parkinson’s Disease and Essential Tremor Using Botulinum Toxin: Case Series


Abstract
:1. Introduction
2. Results
2.1. Study Population
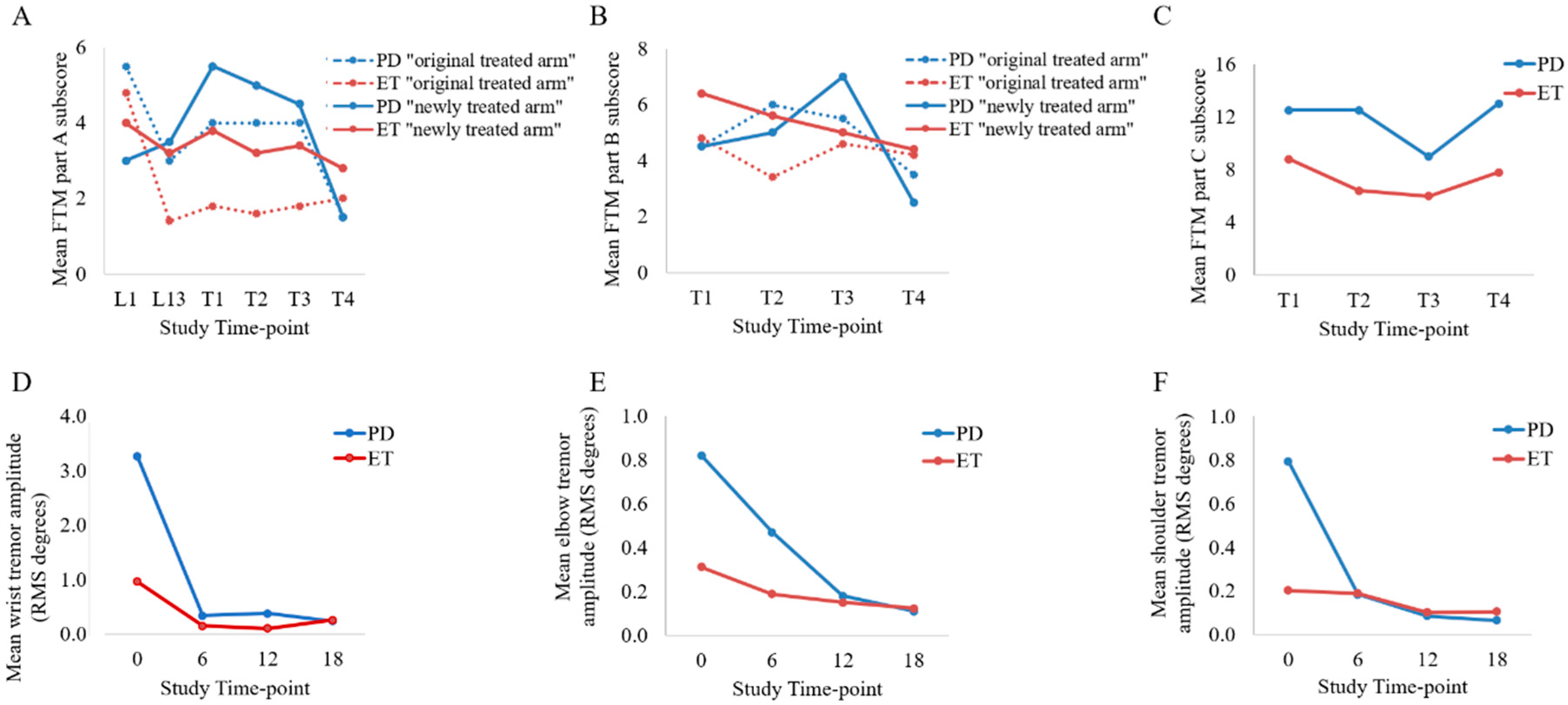
2.2. Fahn-Tolosa-Marin (FTM) Tremor Rating and Arm Functionality
2.3. Kinematic Tremor Analysis
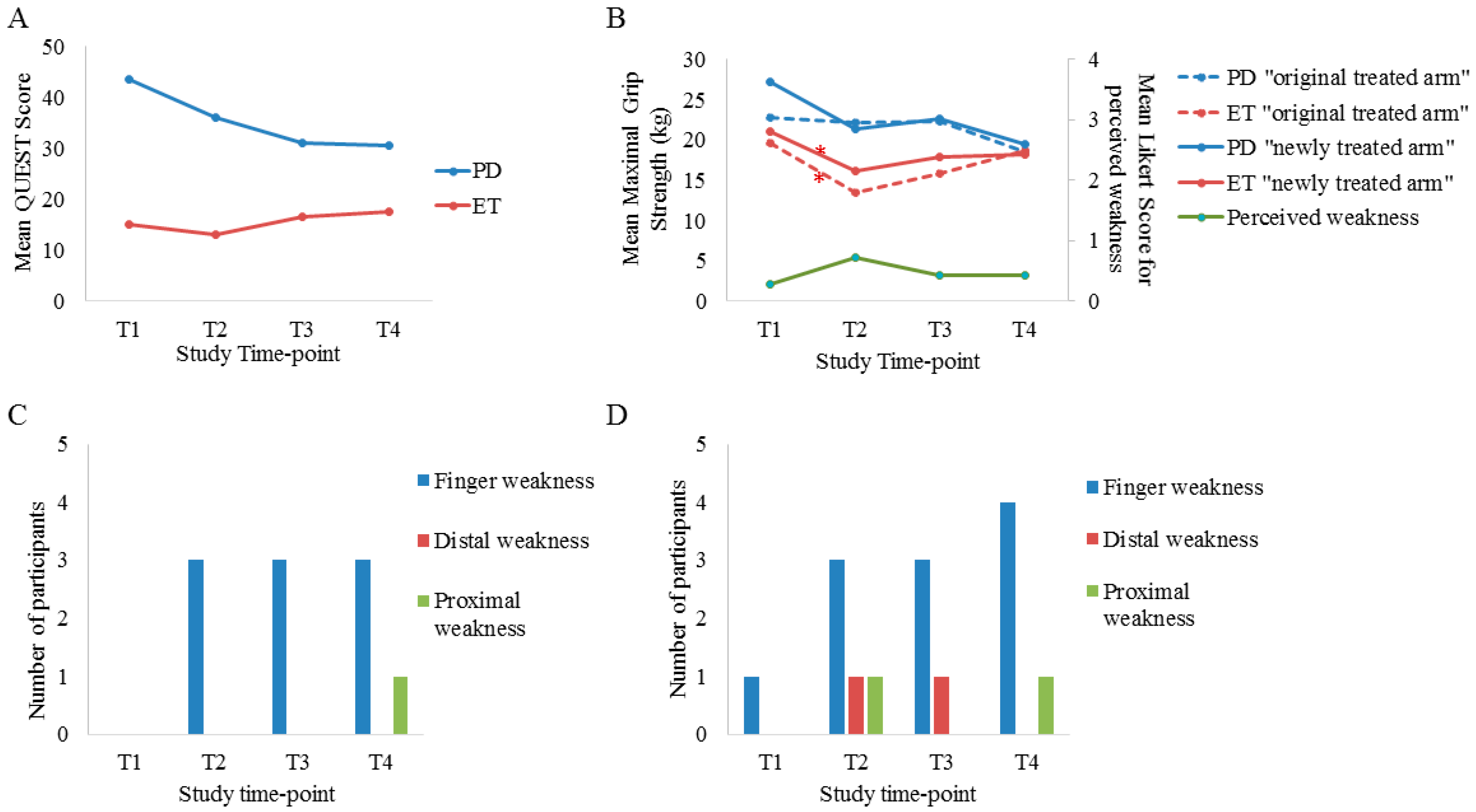
2.4. Quality of Life Measures and Safety Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design and Participants
4.2. Clinical Outcome Measures and Kinematic Tremor Analysis
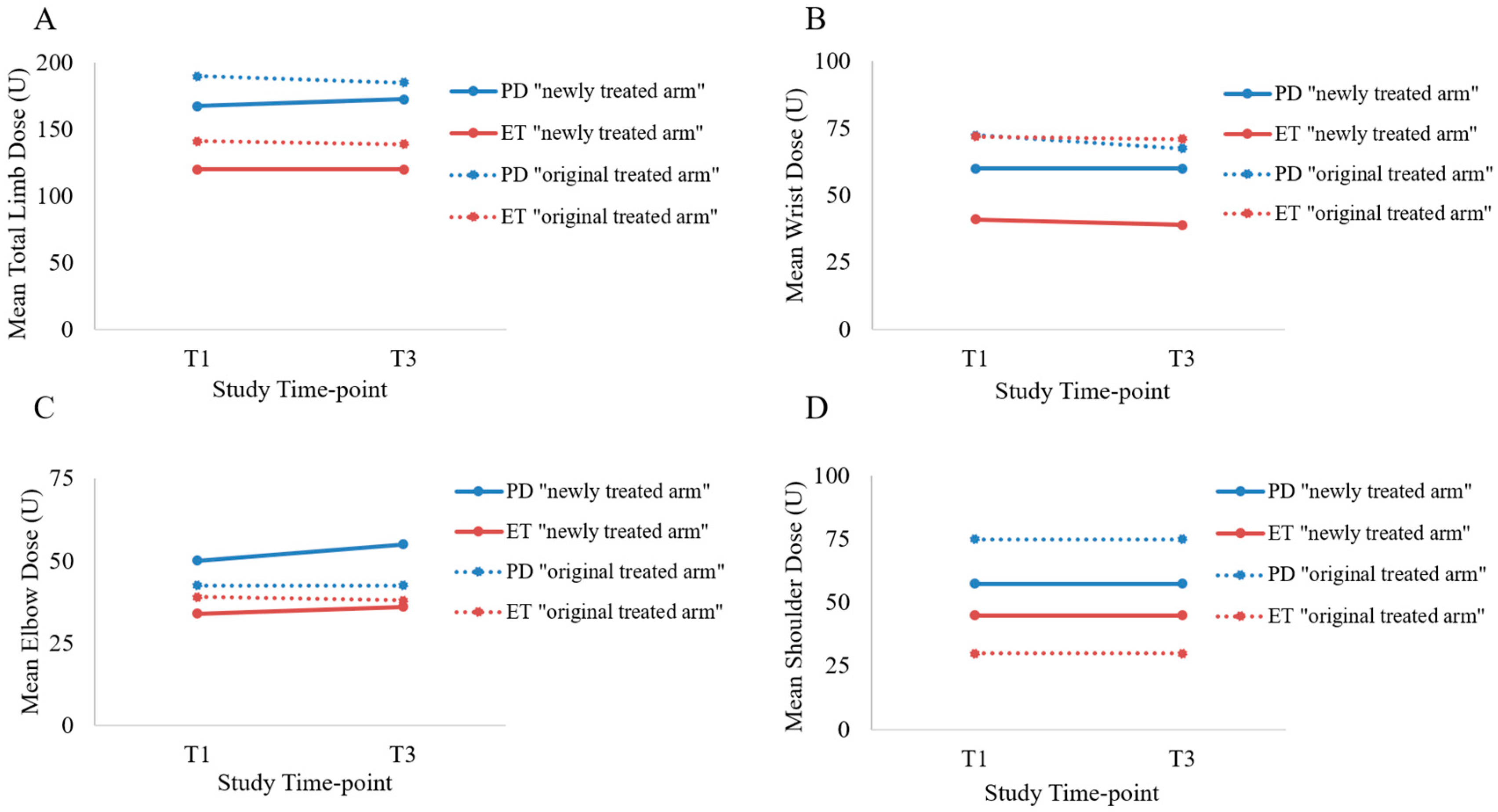
4.3. Treatment
4.4. Analysis
5. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BoNT-A | botulinum toxin type A |
| DOF | degree of freedom |
| ET | essential tremor |
| FTM | Fahn-Tolosa-Marin |
| MMT | manual muscle testing |
| PD | Parkinson’s disease |
| QoL | quality of life |
| QUEST | Quality of Life in Essential Tremor Questionnaire |
| RMS | root mean square |
References
- Louis, E.D.; Machado, D.G. Tremor-related quality of life: A comparison of essential tremor vs. Parkinson’s disease patients. Parkinsonism Relat. Disord. 2015, 21, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Hedera, P.; Cibulčík, F.; Davis, T.L. Pharmacotherapy of essential tremor. J. Cent. Nerv. Syst. Dis. 2013, 5, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Machowska-Majchrzak, A.; Pierzchała, K.; Łabuz-Roszak, B.; Bartman, W. The usefulness of accelerometric registration with assessment of tremor parameters and their symmetry in differential diagnosis of parkinsonian, essential and cerebella tremor. Neurologia i Neurochirurgia Polska 2012, 46, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J. What is Essential Tremor? Curr. Neurol. Neurosci. Rep. 2013, 13, 353. [Google Scholar] [CrossRef] [PubMed]
- Schadt, C.R.; Duffis, E.I.; Charles, P.D. Pharmacological treatment of disabling tremor. Expert Opin. Pharmacother. 2005, 6, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Katzenschlager, R.; Sampaio, C.; Costa, J.; Lees, A. Anticholinergics for symptomatic management of Parkinson’s disease. Cochrane Database Syst. Rev. 2003, 2, CD003735. [Google Scholar] [CrossRef]
- Rajput, A.H.; Rajput, A. Medical treatment of essential tremor. J. Cent. Nerv. Syst. Dis. 2014, 6, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Koller, W.C.; Vetere-Overfield, B. Acute and chronic effects of propranolol and primidone in essential tremor. Neurology 1989, 39, 1587–1588. [Google Scholar] [CrossRef] [PubMed]
- Louis, E.D.; Rios, E.; Henchcliffe, C. How are we doing with the treatment of essential tremor (ET)? Persistence of ET patients on medication: Data from 528 patients in three settings. Eur. J. Neurol. 2010, 17, 882–884. [Google Scholar] [CrossRef] [PubMed]
- Zesiewicz, T.A.; Elble, R.; Louis, E.D.; Hauser, R.A.; Sullivan, K.L.; Dewey, R.B.; Ondo, W.G.; Gronseth, G.S.; Weiner, W.J. Practice parameter: Therapies for essential tremor—Report of the quality standards subcommittee of the American academy of neurology. Neurology 2005, 64, 2008–2020. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.D.; Yiannikas, C.; Mahant, N.; Vucic, S.; Fung, V.S.C. Treatment of proximal upper limb tremor with botulinum toxin therapy. Mov. Disord. 2014, 29, 835–838. [Google Scholar] [CrossRef] [PubMed]
- Trosch, R.M.; Pullman, S.L. Botulinum toxin A injections for the treatment of hand tremors. Mov. Disord. 1994, 9, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Pullman, S.L.; Greene, P.; Fahn, S.; Pedersen, S.F. Approach to the treatment of limb disorders with botulinum toxin A. Experience with 187 patients. Arch. Neurol. 1996, 53, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; Schwartz, K.; Clemence, W.; Aswad, A.; Mordaunt, J. A randomized, double-blind, placebo-controlled study to evaluate botulinum toxin type A in essential hand tremor. Mov. Disord. 1996, 11, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, F.; Samotus, O.; Lee, J.; Jog, M. Effective Management of Upper Limb Parkinsonian Tremor by IncobotulinumtoxinA Injections Using Sensor-based Biomechanical Patterns. Tremor Other Hyperkinet Mov. 2015, 5, 348. [Google Scholar] [CrossRef]
- Samotus, O.; Rahimi, F.; Lee, J.; Jog, M. Functional Ability Improved in Essential Tremor by IncobotulinumtoxinA Injections Using Kinematically Determined Biomechanical Patterns—A New Future. PLoS ONE 2016, 11, e0153739. [Google Scholar] [CrossRef] [PubMed]
- Samotus, O.; Lee, J.; Jog, M. Long-term tremor therapy for Parkinson and essential tremor with sensor-guided botulinum toxin type A injections. PLoS ONE 2017, 12, e0178670. [Google Scholar] [CrossRef] [PubMed]
- Fahn, S.; Tolosa, E.; Marin, C. Clinical rating scale for tremor. In Parkinson’s Disease and Movement Disorders, 2nd ed.; Jankovic, J., Tolosa, E., Eds.; Williams and Wilkins: Baltimore, MD, USA, 1993; pp. 271–280. [Google Scholar]
- Tröster, A.I.; Pahwa, R.; Fields, J.A.; Tanner, C.M.; Lyons, K.E. Quality of life in Essential Tremor Questionnaire (QUEST): Development and initial validation. Parkinsonism Relat. Disord. 2005, 11, 367–373. [Google Scholar] [CrossRef] [PubMed]
- MacDermid, F. Measurement of Health Outcomes Following Tendon and Nerve Repair. J. Hand. Ther. 2005, 18, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Cutter, N.C.; Kevorkian, C.G. Handbook of Manual Muscle Testing, 1st ed.; McGraw-Hill Health Professions Division: New York, NY, USA, 1999; ISBN 0070331502. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| ID | Diagnosis | Gender | Age | Medications (Daily Dose) | Dominant Limb | First Injected Limb | 7th Injection–96 Weeks | ||
|---|---|---|---|---|---|---|---|---|---|
| Total Dose (Units) | # of Muscles Treated | # of Additional Unilateral Injections after 96-Weeks but before Transition | |||||||
| 1 | PD | M | 35 | Stalevo (400 mg) | R | R | 300 | 13 | 10 |
| 2 | ET | F | 74 | Primidone (125 mg) | R | R | 85 | 7 | 8 |
| 3 | ET | M | 78 | Primidone (125 mg) | R | R | 200 | 8 | 9 |
| 4 | PD | M | 68 | Sinemet (750 mg) | R | R | 200 | 11 | 7 |
| 5 | ET | F | 65 | - | R | R | 280 | 13 | 6 |
| 6 | ET | F | 80 | - | R | R | 165 | 11 | 2 |
| 7 | ET | M | 73 | - | R | R | 115 | 9 | 3 |
| ID | Diagnosis | Task with Highest Tremor Amplitude in the “Newly Treated Arm” (Left Arm) | Task with Highest Tremor Amplitude in the “Original Treated Arm” (Right Arm) * | ||||
|---|---|---|---|---|---|---|---|
| Wrist | Elbow | Shoulder | Wrist | Elbow | Shoulder | ||
| 1 | PD | Posture-1 | Posture-2 | Posture-2 | Load-1 | Posture-2 | Load-1 |
| 2 | ET | Posture-1 | Posture-2 | Posture-2 | Load-2 | Load-2 | Posture-2 |
| 3 | ET | Load-1 | Load-2 | Load-2 | Load-1 | Load-2 | Load-2 |
| 4 | PD | Posture-2 | Posture-2 | Posture-1 | Load-1 | Load-2 | Load-2 |
| 5 | ET | Load-2 | Load-1 | Load-1 | Rest-2 | Posture-1 | Load-2 |
| 6 | ET | Posture-1 | Load-2 | Load-2 | Load-1 | Load-2 | Load-2 |
| 7 | ET | Posture-1 | Posture-1 | Rest-2 | Posture-2 | Load-1 | Posture-2 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samotus, O.; Lee, J.; Jog, M. Transitioning from Unilateral to Bilateral Upper Limb Tremor Therapy for Parkinson’s Disease and Essential Tremor Using Botulinum Toxin: Case Series. Toxins 2018, 10, 394. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins10100394
Samotus O, Lee J, Jog M. Transitioning from Unilateral to Bilateral Upper Limb Tremor Therapy for Parkinson’s Disease and Essential Tremor Using Botulinum Toxin: Case Series. Toxins. 2018; 10(10):394. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins10100394
Chicago/Turabian StyleSamotus, Olivia, Jack Lee, and Mandar Jog. 2018. "Transitioning from Unilateral to Bilateral Upper Limb Tremor Therapy for Parkinson’s Disease and Essential Tremor Using Botulinum Toxin: Case Series" Toxins 10, no. 10: 394. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins10100394