Chronodisruption: A Poorly Recognized Feature of CKD
by

Sol Carriazo
1,2, 
Adrián M Ramos
1,2,
Ana B Sanz
1,2,
Maria Dolores Sanchez-Niño
1,2,
Mehmet Kanbay
3 and
Alberto Ortiz
1,2,* 1
IIS-Fundacion Jimenez Diaz, Department of Medicine, Universidad Autonoma de Madrid, Fundacion Renal Iñigo Alvarez de Toledo-IRSIN, 28040 Madrid, Spain
2
Red de Investigación Renal (REDINREN), 28040 Madrid, Spain
3
Division of Nephrology, Department of Medicine, Koc University School of Medicine, 34010 Istanbul, Turkey
*
Author to whom correspondence should be addressed.
Toxins 2020, 12(3), 151; https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030151
Submission received: 30 January 2020
/
Revised: 17 February 2020
/
Accepted: 20 February 2020
/
Published: 28 February 2020
(This article belongs to the Special Issue Comorbidities in Chronic Kidney Disease (CKD))
Abstract
:Multiple physiological variables change over time in a predictable and repetitive manner, guided by molecular clocks that respond to external and internal clues and are coordinated by a central clock. The kidney is the site of one of the most active peripheral clocks. Biological rhythms, of which the best known are circadian rhythms, are required for normal physiology of the kidneys and other organs. Chronodisruption refers to the chronic disruption of circadian rhythms leading to disease. While there is evidence that circadian rhythms may be altered in kidney disease and that altered circadian rhythms may accelerate chronic kidney disease (CKD) progression, there is no comprehensive review on chronodisruption and chronodisruptors in CKD and its manifestations. Indeed, the term chronodisruption has been rarely applied to CKD despite chronodisruptors being potential therapeutic targets in CKD patients. We now discuss evidence for chronodisruption in CKD and the impact of chronodisruption on CKD manifestations, identify potential chronodisruptors, some of them uremic toxins, and their therapeutic implications, and discuss current unanswered questions on this topic.
Keywords:
chronodisruption; chronodisruptor; circadian rhythm; internal clock; chronic kidney diseaseKey Contribution: Chronodisruption refers to the chronic disruption of circadian rhythms leading to disease. We now review evidence for chronodisruption, its causes (chronodisruptors) and consequences in chronic kidney disease (CKD).
1. Introduction: The Growing Global Health Burden of Chronic Kidney Disease
Chronic kidney disease (CKD) is currently defined as abnormalities of kidney structure or function, present for longer than 3 months, with implications for health [1]. The abnormalities of kidney structure or function may be recognized by several criteria. Just one of these criteria is enough to diagnose CKD. The most commonly used criteria are the ones that characterize CKD categories: An abnormal function defined by a decreased glomerular filtration rate (GFR, <60 mL/min/1.73 m2, that is, G categories G3–G5) or evidence of kidney damage such as albuminuria (albumin excretion rate ≥ 30 mg/24 h; urinary albumin creatinine ratio ≥ 30 mg/g, that is, A categories A2 or A3). As for the concept of “implications for health”, it reflects the fact that CKD is associated with an increased risk of all-cause or cardiovascular death, of CKD progression and of development of acute kidney injury (AKI). In this regard, the contribution of CKD to the global disease burden has increased sharply in recent decades. CKD is estimated to become the fifth global cause of death by 2040 and in countries with long life expectancies, it has been projected to become one of the two top causes of death before the end of the century [2,3]. The increasing contribution of CKD to the global burden of disease can be traced to several causes. On one hand, age-adjusted mortality for some key causes of death is actually decreasing. On the other, the longer life expectancy of the population and the increasing prevalence of risk factors for CKD such as obesity, diabetes and hypertension, together with the underdeveloped therapeutic armamentarium, are driving up the prevalence and impact of CKD. There is hope in the recent characterization of a dramatic nephroprotective impact of sodium-glucose transport protein 2 (SGLT2) inhibitors when added on top of renin angiotensin system (RAS) blockade for diabetic kidney disease and potentially other kidney diseases [4,5,6]. However, data from the hypertension field have clearly demonstrated that the availability of effective drugs is not enough, especially in polymedicated populations, where guidelines now emphasize measures to facilitate compliance [7]. In any case, the increasing burden of CKD at a time when other major causes of death are decreasing should be viewed in the context of the paucity of new therapeutic options that have become available in recent years, when compared, for example, with the cancer field [8]. This points towards major deficiencies in our understanding of the pathogenesis of CKD and of the pathophysiology of the CKD-associated increase in cardiovascular risk and premature aging. A key feature of advanced CKD is accumulation of uremic toxins that are no longer excreted by damaged kidneys, although in some instances increased toxin production also contributes to CKD manifestations [9,10,11]. However, this would not explain why there is already an increased risk of death when GFR is preserved, i.e., in patients in whom CKD is diagnosed because of abnormally high albuminuria yet GFR is still above 60 mL/min/1.73 m2. Additional pathogenic events have been recently identified in these patients, such as loss of the kidney production of the anti-aging factor Klotho [12]. A long-recognized feature of CKD is an alteration of well characterized circadian rhythms, including circadian changes in blood pressure and urine concentrating ability. The widespread use of 24 h ambulatory blood pressure monitoring has familiarized physicians with the concept of the sleep time dip of blood pressure and the lack of such dip in CKD patients: CKD patients are characteristically non-dippers [13]. However, the molecular basis of this altered blood pressure circadian rhythm and the existence of other altered rhythms as well as the consequences of these altered rhythms for CKD progression and CKD-associated morbidity and mortality are less well known. We now review the basics of internal clocks and circadian rhythms, the concept of chronodisruption and how this concept applies to CKD leading to the identification of kidney and central chronodisruptors characteristic of the CKD situation and how this may change our approach to CKD management.
2. Biological Rhythms
Exposure to periodic environmental changes during evolution is thought to have driven the development of adaptive biological rhythms of which the best known are the circadian rhythms, which have a period length of around 24 h. However, there are also ultradian rhythms (>24 h) and infradian rhythms (<24 h) [14,15]. Biological rhythms allow the adaptation to changing environments, from the light-night cycle, to the seasons or feed-fast cycles. However, current 24/7 lifestyles dim the environmental differences between day and night, resulting in weak zeitgebers (weak day light, absence of darkness during night, constant environmental temperature, sedentarism and frequent snacking), which may impair the circadian system [16].
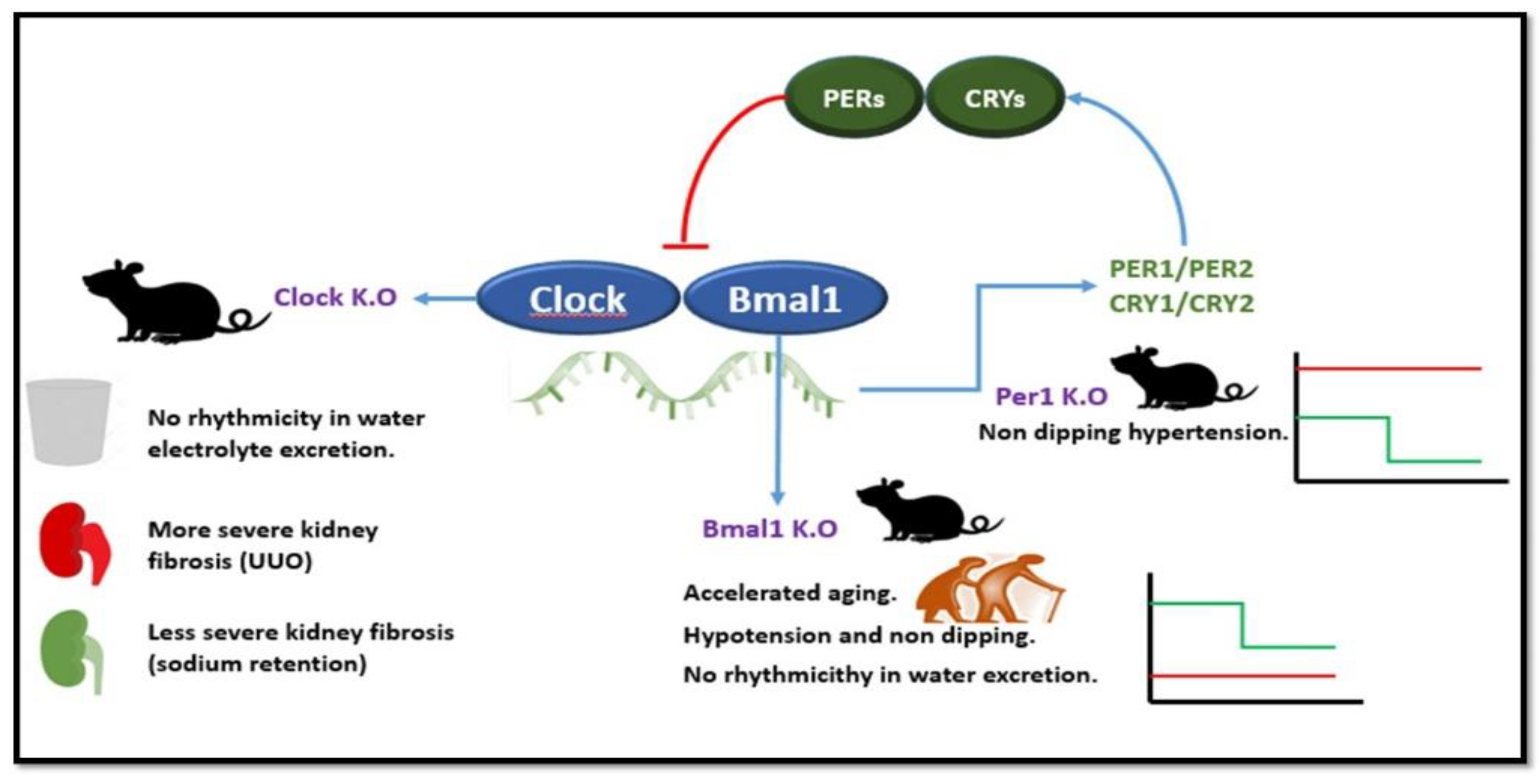
The central circadian clock lies in the suprachiasmatic nucleus in the anterior hypothalamus and coordinates peripheral clocks, including the kidney circadian clock which, in turn, coordinate local physiologic functions with patterns of activity and/or feeding [17]. Several signals contribute to coordinate peripheral circadian rhythms, including hormone secretion (e.g., production of the melatonin hormone by the pineal gland during nighttime, circadian production of aldosterone), neuronal activity (including physical activity and feeding) and body temperature. In addition, canonical clock genes (e.g., Clock, Bmal1, Rev-erbα, Cry1, Cry2, Per1, Per2) are expressed and/or active in a cyclical manner within cells, driving cell autonomous circadian rhythms [14,15]. In the most basic regulatory loop, Clock and Bmal1 are transcription factors that promote Cry and Per gene expression, and Cry and Per in turn suppress Clock/Bmal1 induction of their own transcription [18] (Figure 1). On top of this basic regulatory loop, associated elements account for the circadian regulation of 13% of kidney expressed genes. Furthermore, posttranslational modifications (e.g., phosphorylation, acetylation) are also responsible for circadian changes in protein activity. Functional circadian molecular clockwork evolves in the late fetal and early postnatal kidney. During the nursing period, oscillations are entrained by nutritional cues [19].
Kidney function has circadian rhythms (Table 1). The amplitude of circadian oscillations in GFR and renal plasma flow are around 50%, while water and electrolyte (sodium, potassium, calcium, magnesium, and phosphate) excretion may be several fold higher during the active phase and this is paralleled by circadian changes in kidney oxygenation and the corticomedullary interstitial osmolarity gradient and in the expression of genes involved in its regulation (e.g., vasopressin receptors V1aR, V2R, urea transporter UT-A2 and water channel Aqp2) [14]. Changes in kidney oxygenation modulate HIF-1α activation and erythropoietin levels, which display an amplitude of more than 10-fold under constant darkness and normoxia in mice [15]. Blood pressure peaks early in the beginning of the active period of both diurnal and nocturnal animals [20]. Molecular clocks regulate sodium balance, sympathetic function and vascular tone, all contributing to blood pressure regulation. Altered kidney circadian rhythms have been associated with the development of hypertension, chronic kidney disease, and kidney stones (reviewed in [14]).
Insights into the circadian regulation of kidney functions is derived from genetic defects in clock genes [14] (Figure 1). Thus, Per1 KO mice develop non-dipping hypertension under conditions of sodium retention while Clock KO mice lose the circadian rhythmicity in urinary water and electrolyte excretion and develop more severe kidney fibrosis upon ureteral obstruction but were protected from kidney fibrosis driven by sodium retention conditions [14]. Additionally, Clock mutants had some features suggesting increased severity of adenine-induced CKD, such as higher blood pressure and expression as some gelatinase genes, but there were no differences in kidney fibrosis or serum creatinine [21]. Bmal1 KO mice develop accelerated aging, hypotension and a non-dipping blood pressure pattern and lose the circadian variations in interstitial medullary osmolarity suggesting a role of circadian clocks in the control of urine volume beyond dietary clues [14,22]. Kidneys from conditional nephron-specific Bmal1 deletion mice exhibited a decrease in NAD+-to-NADH ratio, increase in plasma urea and creatinine and a reduced capacity of the kidney to secrete anionic drugs (furosemide) paralleled by changes in the expression of tubule transporters such as organic anion transporter 3 (SLC22a8) [23]. Na+-H+ exchanger 3 (NHE3) activity also has rhythmic oscillations causing daily fluctuations in Na+ and water transport of the proximal tubule cell.
3. Concept of Chronodisruption
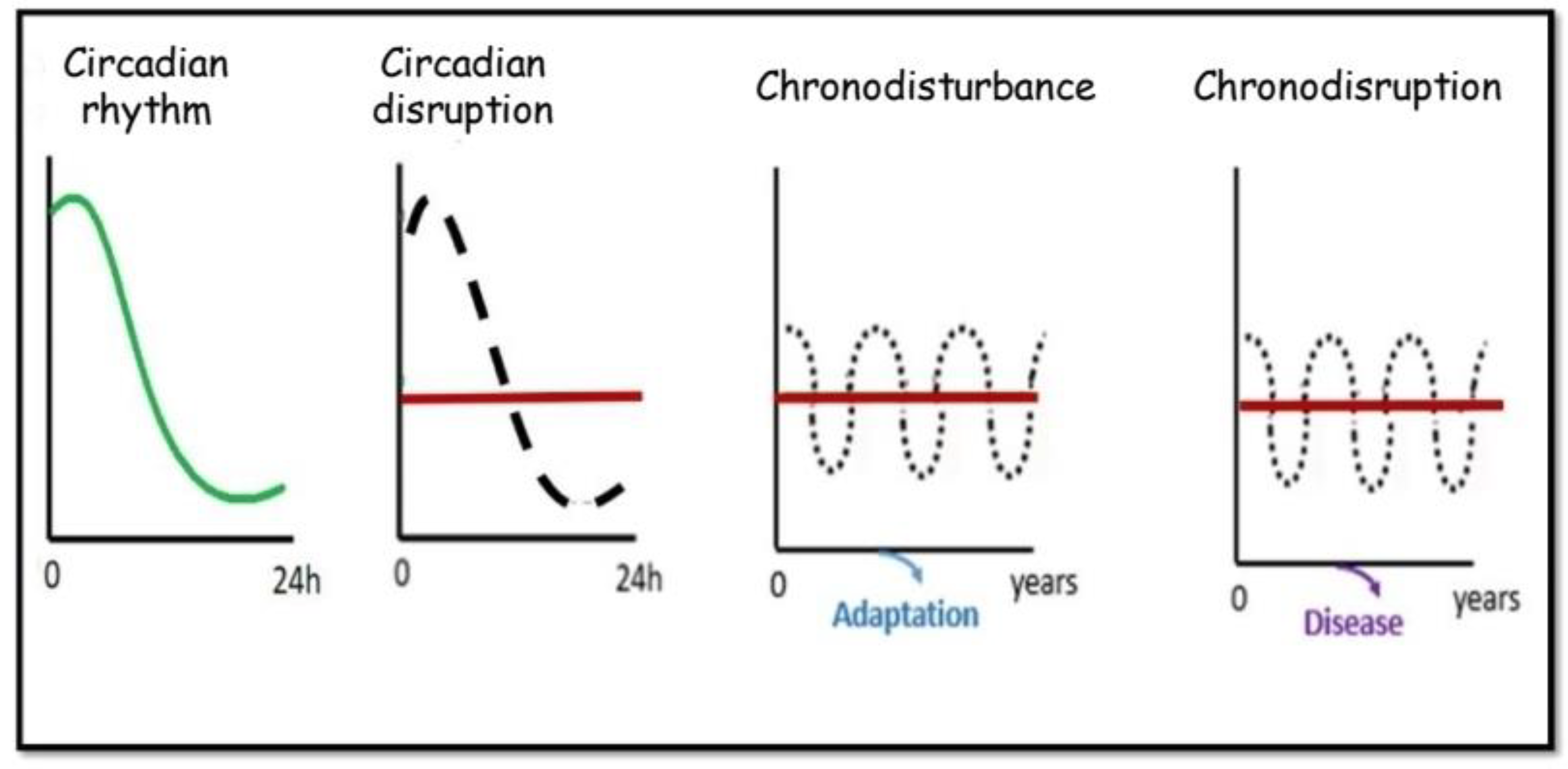
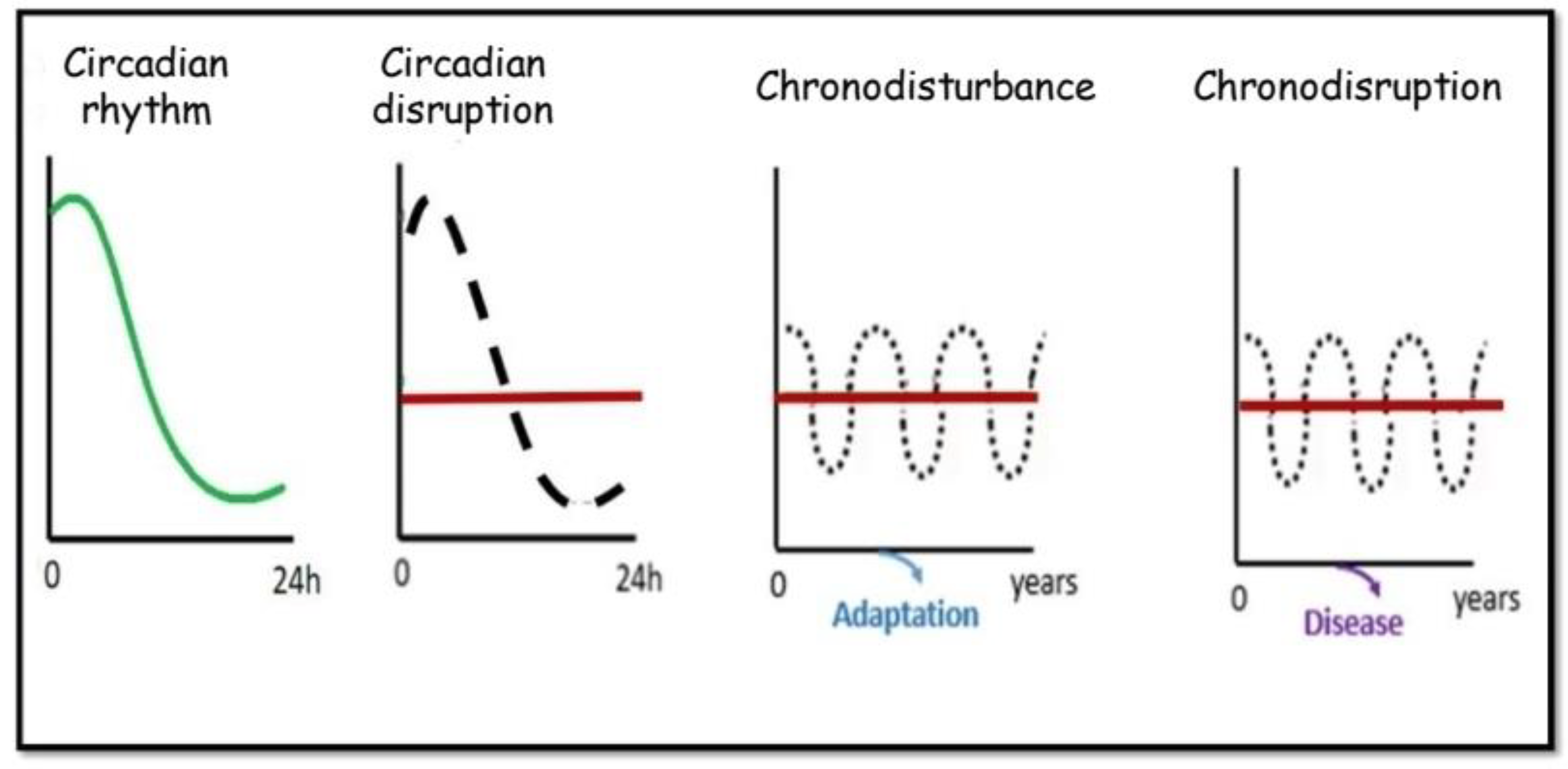
The concept of chronodisruption was coined in 2003 by Thomas C. Erren, Russel J. Reiter and Claus Piekarski from the University of Cologne [24] (Figure 2). The term was meant to go beyond the concept of chronodisturbance, a general term they proposed to refer to modulations of rhythms over time that are not necessarily deleterious since physiological compensations may prevent the development of chronic disease resulting from altered rhythms. Chronodisturbance itself was a conceptual leap from more common concepts such as “circadian disruption” or “disruption of circadian rhythms” that suggest that rhythms over 24 h can become desynchronized and that this may have adverse health effects, since these common terms may be more limited in time scope than chronodisturbance which may have a decade scope. Thus, circadian disruption may be caused by travel across several time zones, however, within a limited period of time within this new time zone, adaptation of the circadian rhythms to the new time zone occurs and there are no long-term consequences. By contrast, chronic work in night shifts will lead to chronodisturbance, that is to persistent desynchronization between time and activity. In 2009, they further elaborated on the chronodisruption concept, stating that “chronodisruption can be understood as a critical loss of time order, i.e., a disorder or chaos of an otherwise physiological timing at different organizational levels, including the gene expression levels in individual cells” and thus, it is “a breakdown of phasing internal biological systems appropriately relative to the external, i.e., environmental changes, which leads to chronobiological disorders” [25]. Following with the chronic night shift example, this would be considered chronodisturbance as long as there are no adverse consequences for health, and chronodisruption if this leads to adverse consequences for health. Furthermore, they characterized chronodisruptors as “exogenous and endogenous exposures or effectors which are chronobiologically active and can thus disrupt the timing and order, i.e., the temporal organization of physiologic functions and hierarchies” [25]. A clear example of a chronodisruptor is the use of artificial light or backlit screens during the night. They additionally proposed that assessment of melatonin levels in saliva, urine and blood may be a robust biomarker of chronodisruption. While in some fields the concept was immediately grasped (In 2007, the International Agency for Research on Cancer classified shift-work that involves circadian disruption as probably carcinogenic to humans), it was not until 2013 that the term chronodisruption was used in the context of CKD [26] and only in 2019 was a second manuscript published on the topic [27].
While this is surprising given the chronic nature of CKD, its similarities with aging and the widely known fact that circadian rhythms may be disturbed in CKD, it does not mean that the nephrological community is not aware of disruption of circadian rhythms in CKD. Indeed, very active research is going on as attested by recent reviews [14,15,26,28,29]. However, CKD researchers may benefit from a wider use of the terms and concepts of chronodisruption and chronodisruptor. Thus, the mere concept of chronodisruptor may facilitate the search of chronodisruptors involved in CKD manifestations. These may potentially be abnormal levels of uremic toxins or abnormally low levels of uremia-related factors, among others.
4. Chronodisruption in CKD
Several alterations of circadian rhythms are well characterized in CKD patients and there is accumulating evidence that at least some of them may adversely affect health, thus fulfilling criteria to be considered chronodisruption. These include disordered sleep, non-dipping hypertension, failure to properly concentrate urine at night and the circadian pattern of proteinuria in patients with nephrotic syndrome: Peak protein excretion occurs at around 16.00 h and the nadir at 03.00 h and is independent of GFR [14]. Ultradian rhythms have also been described in CKD. For example, in patients with end-stage renal disease treated with hemodialysis, blood pressure varies seasonally, with higher values in the winter and lower values in the summer [30]. However, this pattern has not been directly compared to that of non-CKD individuals. Of the diverse altered circadian rhythms in CKD, the ones best characterized with adverse consequences for health, meeting the criterion to define chronodisruption are disordered sleep and non-dipping hypertension and will be discussed more extensively.
Sleep timing, quality and/or duration are frequently disturbed in CKD patients and this can be reproduced by subtotal nephrectomy in rats [26] or in mice with adenine-induced CKD [21]. In patients with mild to moderate CKD, lower eGFR was associated with shorter sleep duration (−1.1 mL/min/1.73 m2 per hour less sleep), greater sleep fragmentation (−2.6 mL/min/1.73 m2 per 10% higher fragmentation) and later timing of sleep (−0.9 mL min/1.73 m2 per hour later). Higher proteinuria was also associated with greater sleep fragmentation (approximately 28% higher per 10% higher fragmentation) [31]. However, from these studies, potential causality and direction of the association is unclear, since CKD may cause chronodisruption but chronodisruption may theoretically lead to CKD progression. The nocturnal melatonin peak appears to be preserved just in nocturnal hemodialysis patients but not in patients on other dialysis modalities. In this regard, exogenous melatonin may improve intrarenal renin angiotensin system activation and renal injury in experimental CKD [32]. Specific conditions associated to CKD may contribute to disrupted sleep patterns. These include nocturia elated to decreased urine concentration capacity and obstructive sleep apnea. The prevalence of obstructive sleep apnea increases as kidney function declines and is higher among patients with ESRD. obstructive sleep apnea may contribute to higher nocturnal blood pressure and to pulmonary hypertension and these may improve on continuous positive airway pressure (CPAP) [33,34,35].
In CKD patients, the prevalence of reverse dipping (night-time blood pressure peak) for systolic blood pressure and episodes of hypotension during daytime is doubled, independently of blood pressure control [36]. Uninephrectomy by itself interfered with blood pressure rhythms. Albuminuria in hypertensive patients is also accompanied by quantitatively striking higher nighttime systolic blood pressure, particularly in patients with diabetes with very high albuminuria and low eGFR [37]. Although studies regarding causality are needed, this observation may point out to a CKD A2/A3-dependent altered clock: That is, albuminuria itself may potentially be a chronodisruptor, even when global kidney function (GFR) is preserved, on top of any potential chronodisruptor activity of uremic toxins that accumulate when GFR falls. Further supporting a potential role of albuminuria itself, in minimal change nephrotic syndrome patients with overall preserved GFR (around 75 mL/min/1.73 m2), sleeping/waking systolic and diastolic blood pressure ratios were higher than in healthy controls and this was reversed by remission of proteinuria [38].
Non-dipping is a recognized cardiovascular risk factor. In the general population, there is a linear relationship between the nocturnal decline in blood pressure and cardiovascular mortality. On average, each 5% decrease in the decline in nocturnal systolic/diastolic blood pressure was associated with an approximately 20% greater risk of cardiovascular mortality and this was observed even when 24-h blood pressure values were within the normal range (average 118/69 mmHg), diminished nocturnal decreases [39]. In CKD patients this may be magnified, as they have higher systolic blood pressure during the night-time and greater prevalence of non-dipping. Indeed, nocturnal systolic blood pressure correlated more strongly with cardiac organ damage [40]. In hemodialysis patients, increased short-term nighttime pulse pressure variability but not ambulatory blood pressure levels were significantly predictive of long-term all-cause mortality [41].
Several individual contributors to the circadian regulation of blood pressure have been identified and these include local kidney molecular clocks, whose local expression may be potentially altered by kidney disease mediators. Thus, Bmal1 deficiency in juxtaglomerular renin-secreting granular cells resulted in polyuria, changes in the circadian rhythm of urinary sodium excretion, increased GFR, and lower plasma aldosterone levels and lower blood pressure [42]. The sodium-chloride cotransporter (NCC, SLC12A3) in distal convoluted tubules contributes to sodium balance and blood pressure regulation. Disturbing this rhythm induces “nondipping” blood pressure. Both mineralocorticoids and glucocorticoids regulate NCC activity. Mineralocorticoid receptor activation maintains the NCC protein pool while glucocorticoid receptor activation regulates NCC phosphorylation and the diurnal rhythm of NCC activity [43]. ATP1B1 encodes the β1 subunit of the Na+/K+-ATPase. Atp1b1 mRNA and protein levels in mouse kidney have a circadian rhythm that was antiphasic to the blood pressure rhythm. In Dec1-deficient mice, kidney Atp1b1 expression was increased and blood pressure was lower. In contrast, in Clock-mutant mice, Atp1b1 expression was low and blood pressure high [44]. The expression of both NCC and ATP1B1 is altered in kidney injury, potentially linking kidney injury to an altered expression of kidney circadian genes regulating blood pressure [45,46].
The location of disrupted timekeeping in CKD merits further study. In murine adenine-induced CKD, in vivo disrupted timekeeping could be dissociated in vitro into a suprachiasmatic nucleus pacing, which remained uncompromised, and a kidney clock that became a less robust circadian oscillator with a longer period, suggesting that the kidney contributes to overall circadian timekeeping and that there is local kidney disruption of circadian rhythms during CKD [47]. By contrast, in vivo exploration of mice with adenine-induced CKD disclosed low amplitude PER2:luciferase rhythms in their central suprachiasmatic nucleus circadian clock and in intact kidney, liver, and submandibular gland, as well as altered expression patterns of circadian genes including canonical clock genes and kidney genes such as Hif, Aqp2, and V2r [21]. Overall, these results point to interference of peripheral clocks with the central clock in CKD.
Failure to properly concentrate urine at night may further aggravate CKD-associated sleep disruption through nocturia. However, there are potentially more severe consequences. Thus, improper water excretion will promote the secretion of antidiuretic hormone (vasopressin, ADH). There is increasing evidence that overactivation of ADH may be detrimental. Specifically, the vasopressin 2 receptor (V2R) blocker tolvaptan slows the progression of autosomal dominant polycystic kidney disease (ADPKD) [48]. While this was initially thought to be related to kidney cyst specific intracellular signaling events, an adverse impact of ADH on glomerular hyperfiltration was later identified that may be a universal driver of CKD progression, not limited to ADPKD [49,50]. In this regard, circulating copeptin levels provide a better understanding of ADH activation that measuring ADH itself, which is short lived. Serum copeptin is increased in hypertension, CKD and cardiovascular disease, and ADH activation of V1R and/or V2R may be detrimental to the kidney and the cardiovascular system [51].
The altered circadian pattern of proteinuria may impact the assessment of the severity or proteinuria when different timed urine samples are assessed (12 h vs. 24 h vs. point collections), but whether this leads to any health consequence is currently unclear.
CKD has a bidirectional relationship with aging. On one hand, aging is associated with a progressive decrease in GFR. On the other, CKD causes accelerated aging and some of the factors responsible for this phenotype, such as decreased production of the anti-aging factor Klotho have been identified, as discussed below. Interestingly, aging is associated with altered central and peripheral circadian rhythms, and the sleep–wake cycle [52], leading to a phase advance, rhythm fragmentation and flattening [53]. This may in part be offset by regular physical activity [52]. Given the close association of CKD with aging, further studies are required that explore to what extent the age-associated loss of renal function contributes to age-associated circadian rhythm abnormalities and age-associated organ dysfunction and disease.
5. Chronodisruptors as Therapeutic Targets in CKD
A PubMed search for “chronodisruptors” in January 2020 resulted in only 5 hits, none of them related to CKD. This may relate to both limited understanding of chronodisruptors as with limited use of the term.
Identifying and targeting chronodisruptors may identify novel approaches to the prevention and therapy of CKD. Potential chronodisruptors include diet, the light–dark cycle, inflammatory mediators, uremic toxins, HIF abnormalities, and physical inactivity. We will briefly discuss examples of all of these (summarized in Table 2). While diet, light clues and inflammation may be active at all stages of CKD, even before GFR decreases, accumulation or uremic toxins would be expected to be active only after significant decrease of GFR has taken place, i.e., after significant loss of kidney mass.
5.1. Dietary Clues
There is some evidence that dietary lipids and sodium may behave as chronodisruptors and, more specifically, that salt may be a chronodisruptor in CKD. Indeed, salt loading aggravates the inverse relationship between melatonin secretion, assessed as urinary levels of its metabolite 6-sulfatoxymelatonin (aMT6s) and albuminuria in CKD patients [54]. High salt feeding led to region-specific alterations in circadian clock components within the kidney and caused a 5.5-h phase delay in the peak expression of Bmal1 and suppressed Cry1 and Per2 expression in the renal inner medulla, but not the renal cortex, of control rats. The phase delay in Bmal1 expression appears to be mediated by endothelin-1 because this phenomenon was not observed in endothelin receptor B (ETB)-deficient rats. Thus, high salt feeding leads to intrarenal circadian dyssynchrony in part through activation of ETB receptors within the renal inner medulla [55]. There is less information on the molecular mechanisms engaged by dietary lipids to influence circadian kidney rhythms. One possibility is through epigenetic regulation of gene expression. Thus, dietary lipids modulate the expression of miR-107, a miRNA that regulates the circadian system [56].
An area of research is focused on altering circadian rhythms by time-related dietary approaches (chrononutrition) or pharmacological substances (chronobiotics) [57]. In a randomized clinical trial, short chronotype-adjusted diet was more effective than the traditional hypocaloric diet in decreasing BMI, and waist circumference [58]. In a further trial, eating late was associated with decreased resting-energy expenditure, decreased fasting carbohydrate oxidation, decreased glucose tolerance and blunted daily profile in free cortisol concentrations [59]. In this regard, it is widely recognized that chronodisruption and mistimed eating have deleterious effects on metabolic health that may exceed those of eating an unbalanced diet, during the normal active phase [60]. How CKD may affect these relationships and to what extent chronotype-adjusted diets may provide any advantages to CKD patients is, at this point, unclear.
Diet may also influence the gut microbiota. Gut bacteria modulate host rhythms via microbial metabolites such as butyrate and others, and amines and disturbed microbiome rhythms have been proposed to at least partially contribute to an increased risk of obesity and metabolic syndrome associated with chronodisruption [61]. Although there is little information on microbiota and chronodisruption in CKD, both obesity and metabolic syndrome increase the risk of CKD. Conversely, CKD has been associated with altered microbiota patterns and metabolites accumulated in CKD may modulate the gut microbiota and butyrate production [62,63,64].
5.2. Light Clues
In June 2019, a working group convened by the International Agency for Research on Cancer (IARC) concluded that “night shift work” is probably carcinogenic to humans and considered a Group 2A carcinogen [65]. There is very little information on night shift work and CKD. However, in a Korean study, the risk of CKD was two-fold higher in female shift workers than in female non-shift workers, although there were no differences in males [66]. In experimental animals, maternal chronic photoperiod shifting during gestation led to kidney gene expression changes in the offsprings, including the expression of sodium handling genes subject to circadian rhythms, and higher blood pressure values [27].
5.3. Kidney Inflammation
Kidney inflammation is a feature of both AKI and CKD. TWEAK is a proinflammatory cytokine of the TNF superfamily that promotes AKI and CKD [67,68]. A key feature of the TWEAK cytokine is that, contrary to TNF, it recruits the NIK-mediated, non-canonical pathway for activation of the NFκB transcription factor in kidney cells on top of the canonical pathway for NFκB activation [69,70,71,72,73]. NFκB is a key proinflammatory transcription factor that also downregulates kidney protective molecules [74]. Non-canonical NFκB is characterized by the nuclear translocation of RelB/NFκB2 p52 heterodimers [75]. Interestingly, the RelB subunit of NFκB directly binds BMAL1 and acts as a negative regulator of circadian gene expression [76]. TWEAK also downregulates the kidney production of Klotho, an antiaging factor that is mainly expressed in the kidney, thus, potentially contributing to the accelerated aging of CKD [77,78]. Although the decrease in Klotho is mediated by the canonical NFκB pathway, it is nonetheless integrated within the cell response to TWEAK characterized by downregulation of tissue protective factors, as is a decrease in the mitochondrial biogenesis master regulator PGC1α [79,80]. In his regard, RelB also couples with the bioenergy NAD (+) sensor sirtuin 1 (SIRT1) to modulate cell metabolism and mitochondrial bioenergetics [81].
Kidney fibrosis sis very tightly linked to inflammation. In this regard, Smad3, a key signaling effector for the profibrotic cytokine TGFβ1, has circadian expression and modulates the expression of circadian rhythm genes such as Dec1, Dec2, and Per1 [82].
5.4. Uremic Toxins
A key feature of advanced CKD is the accumulation of uremic retention solutes, molecules usually excreted by the kidneys that accumulate in the circulation when GFR decreases [11]. Some of these uremic retention solutes have a clear adverse impact on pathophysiological processes, promoting CKD progression and manifestations, they are the so-called uremic toxins. When kidneys fail, renal function is replaced by dialysis or eventually by a kidney graft. Unfortunately, while dialysis prevents acute uremic death, it provides only a very limited capacity to clear uremic toxins, especially those of gut origin that circulate bound to serum proteins, which may be of special interest from the point of view of chronodisruption. Thus, several gut-derived uremic toxins bind and activate the Aryl Hydrocarbon Receptor (AhR). These include uremic toxins derived from tryptophan, some of gut microbiota origin, such as indolic uremic toxins (indoxyl sulfate, indole-3 acetic acid, and indoxyl-β-d-glucuronide) and uremic toxins from the kynurenine pathway (kynurenine, kynurenic acid, anthranilic acid, 3-hydroxykynurenine, 3-hydroxyanthranilic acid, and quinolinic acid) [83,84]. Interestingly, AhR exhibits a rhythmic expression and time-dependent sensitivity to activation by AhR agonists and in response to at least some ligands, AhR forms a heterodimer with Bmal1 and inhibits Clock/Bmal1 activity, modulating amplitude and phase of rhythms in circadian clock genes [85,86]. In this regard, AhR deficiency enhanced behavioral responses to changes in the light–dark cycle, increased rhythmic amplitude of circadian clock genes in the liver, and altered glucose and insulin rhythms [86].
Kidney proximal tubule cells sense elevated endogenous, gut microbiome-derived, uremic retention solutes which elicit a compensatory response consisting of up-regulating the organic anion transporter-1 (OAT1), thus increasing metabolite secretion in urine [87]. This was clearly illustrated for indoxyl sulfate which induced OAT1 expression via AhR and EGFR signaling, controlled by miR-223 [87]. AhR protein expression was additionally positively associated with plasma levels of another indolic uremic toxin, indole-3 acetic acid (IAA) [88]. IAA is responsible for some adverse effects potentially related to the increased cardiovascular risk of CKD patients, such as increasing the expression of tissue factor in human vascular cells via the AhR [89]. However, up to now it is unknown to what extent the circadian expression of AhR is disrupted in CKD, what role might uremic toxins and the microbiota have in this phenomenon and what the consequences in any alterations in this system circadian regulation might be for CKD patients.
5.5. Disrupted HIF Activation and EPO Production
Hypoxia-inducible factor (HIF) are a family of transcription factors that protect from hypoxia both at the local, autocrine/paracrine level and by driving erythropoietin production, also through an endocrine mediator of kidney origin. Thus, the kidney has the lowest pO2 in the body, a consequence of the existence of two consecutive capillary networks (glomerular and peritubular) and of the high metabolic rate of tubular cells which spend huge amounts of energy in recovering filtered molecules. This is the likely reason for the kidney location of erythropoietin-producing cells, a key defense mechanism against hypoxia that modulates hemoglobin availability and, thus, oxygen transport capacity by red blood cells.
The expression of a key HIF protein, HIF1α, is under circadian rhythm control. CRY1 reduces HIF-1α half-life and HIF binding to target gene promoters and abrogation of CRY1/2 stabilized HIF1α in response to hypoxia [90] while PER2 activates HIF-1α and facilitates its recruitment to promoter regions of its downstream genes. HIF-1α activation by PER2 was related to keeping the asparagine residue at position 803 of HIF-1α (HIF-1α N803) unhydroxylated by hypoxic stimulation in the absence of changes in HIF-1α protein levels [91]. In murine heart ischemia, Per2 was required for Hif-1α stabilization [92]. This may be exploited therapeutically. Thus, Per2 stabilization through adenosine activation of Adora2b or by exposure to intense light modified HIF-dependent cardiac metabolism, resulting in the transcriptional induction of glycolytic enzymes and Per2-dependent protection from ischemia [92]. So far, no such experiments have been reported for kidney disease. By contrast, BMAL1 deficiency increased HIF1α protein levels under hypoxic conditions. Induction of clock and HIF1α target genes in response to strenuous exercise varied according to the time of day in wild-type mice. Thus, interactions between circadian and HIF pathways influence metabolic adaptation to hypoxia [93].
Circadian transgenic zebrafish cells simulating a repressed or an overstimulated circadian clock, resulted in altered gene transcription levels of oxygen-regulated genes such as EPO and altered the hypoxia-induced increase in Hif-1α protein concentration. The amount of Hif-1α protein accumulated during the hypoxic response depended on the time of the day, with one maximum during the light phase and a second one during the dark phase [94].
The positive effects of HIF prolyl hydroxylase inhibitors (that is, HIF activators) over anemia and other cardiovascular risk parameters in CKD patients [95] raises the possibility that downregulation of HIF activation righter than loss of renal mass is a key driver of uremic anemia and may allow the exploration of the chronodisruption impact of uremic anemia itself.
5.6. Physical Inactivity
Both the drivers (e.g., obesity) and consequences (e.g., anemia, cardiovascular disease, malnutrition) of CKD may be associated to physical inactivity and this may act as a chronodisruptor. The impact of regular physical activity on kidney functions circadian misalignment should be studied, since regular endurance exercise appears to entrain peripheral clocks in muscle and heart [52].
5.7. Integration of Several Chronodisruptors
It is likely that the end result of the impact of several chronodisruptors relates to the integration of the different signaling events. In this regard, there is evidence that chronodisruptors potentially associated with CKD interact between them. Thus, RelB directly binds to the AhR and AhR interacts with dietary clues [81,96]. AhR-deficient mice are protected from high fat diet-induced disruption in metabolic rhythms, exhibiting enhanced insulin sensitivity and glucose tolerance [96].
6. The Way Forward
Table 3 summarizes some key answered questions regarding chronodisruption, chronodisruptors and CKD. A key to the clinical translation of the current state of knowledge regarding chronodisruption in CKD, beyond preventing and treating CKD itself, is to identify targetable chronodisruptors.
An issue frequently overlooked by researchers is that the most common laboratory animals used to study kidney disease are rats and mice, which are nocturnal animals. Thus, essentially all experiments are performed during their inactive period and manipulation during this period risks creating chronodisruption which may have an unknown impact on experimental results [20]. This emphasizes the need for human studies. However, clinical research into CKD-related chronodisruption would require easy access to non-invasive techniques that allow monitoring of biological rhythms beyond blood pressure. Wrist skin temperature has been proposed as a new index for evaluating circadian system status [97]. Development of chronodisruption scores [98] and computational model of the renal circadian clock [99] would also facilitate clinical research. Longitudinal studies and ideally, interventional trials, would provide information on the causality and direction in the clinical association of disturbed sleep (a likely manifestation of chronodisruption) and CKD. In this regard, in a prospective cohort study of over 4000 participants from the Nurses’ Health Study, shorter sleep duration was prospectively and independently associated with faster decline in renal function [100].
Chronopharmacology studies how biological rhythms influence pharmacokinetics, pharmacodynamics, and toxicity, and determines whether time-of-day administration modifies the pharmacological characteristics of the drug. Chronotherapy applies chronopharmacological studies to clinical treatments, determining the best biological time for dosing [101]. Well known examples in CKD patients include phosphate binders. In addition, there is a school of thought supported by meta-analyses results and clinical trials emphasizing the benefits of nighttime administration of anti-hypertensive medication [14].
In a recent clinical trial in hypertensive patients without CKD, ingestion of at least one blood pressure-lowering medication at bedtime resulted in improved ambulatory blood pressure control with a significant further decrease of asleep blood pressure and reduced risk of incident CKD than early morning administration [102].
While this may be initially viewed as CKD prevention, it is likely that it may additionally represent slowing of CKD progression, Thus, current diagnostic criteria for CKD are late events and patients who progressed to meet the diagnostic criteria for CKD during the trial likely had baseline subclinical CKD, maybe as cause of hypertension [103]. New upcoming drugs may also benefit from chronopharmacology studies. Thus, HIF activators were recently approved for clinical use in China and are expected to be soon available worldwide to treat uremic anemia [104]. Whether chronopharmacology may optimize timing of administration is currently unknown. Finally, cardiovascular and nephroprotective effects have been described for melatonin [105].
Author Contributions
All authors have contributed and read and agreed to the published version of the manuscript.
Funding
This work was funded by FIS CP14/00133, PI16/02057, PI18/01366, PI19/00588, PI19/00815, DTS18/00032, ERA-PerMed-JTC2018 (KIDNEY ATTACK AC18/00064 and PERSTIGAN AC18/00071, National Institute of Health (2R01AI063331), ISCIII-RETIC REDinREN RD016/0009 Fondos FEDER, FRIAT, Sociedad Española de Nefrología, Comunidad de Madrid B2017/BMD-3686 CIFRA2-CM, Miguel Servet MS14/00133 to MDSN and ABS. IIS-Fundacion Jimenez Diaz Biobank, part of the Spanish Biobanks Platform (PT17/0015/0006). The APC was funded by PI19/00815.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Perez-Gomez, M.V.; Bartsch, L.A.; Castillo-Rodriguez, E.; Fernandez-Prado, R.; Fernandez-Fernandez, B.; Martin-Cleary, C.; Gracia-Iguacel, C.; Ortiz, A. Clarifying the concept of chronic kidney disease for non-nephrologists. Clin. Kidney J. 2019, 12, 258–261. [Google Scholar] [CrossRef]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef] [Green Version]
- Ortiz, A.; Sanchez-Niño, M.D.; Crespo-Barrio, M.; De-Sequera-Ortiz, P.; Fernández-Giráldez, E.; García-Maset, R.; Macía-Heras, M.; Pérez-Fontán, M.; Rodríguez-Portillo, M.; Salgueira-Lazo, M.; et al. The Spanish Society of Nephrology (SENEFRO) commentary to the Spain GBD 2016 report: Keeping chronic kidney disease out of sight of health authorities will only magnify the problem. Nefrologia 2019, 39, 29–34. [Google Scholar] [CrossRef]
- Fernandez-Fernandez, B.; Fernandez-Prado, R.; Górriz, J.L.; Martinez-Castelao, A.; Navarro-González, J.F.; Porrini, E.; Soler, M.J.; Ortiz, A. Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation and Study of Diabetic Nephropathy with Atrasentan: What was learned about the treatment of diabetic kidney disease with canagliflozin and atrasentan? Clin. Kidney J. 2019, 12, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Sarafidis, P.; Ferro, C.J.; Morales, E.; Ortiz, A.; Malyszko, J.; Hojs, R.; Khazim, K.; Ekart, R.; Valdivielso, J.; Fouque, D.; et al. SGLT-2 inhibitors and GLP-1 receptor agonists for nephroprotection and cardioprotection in patients with diabetes mellitus and chronic kidney disease. A consensus statement by the EURECA-m and the DIABESITY working groups of the ERA-EDTA. Nephrol. Dial. Transplant. 2019, 34, 208–230. [Google Scholar] [CrossRef]
- Herrington, W.G.; Preiss, D.; Haynes, R.; von Eynatten, M.; Staplin, N.; Hauske, S.J.; George, J.T.; Green, J.B.; Landray, M.J.; Baigent, C.; et al. The potential for improving cardio-renal outcomes by sodium-glucose co-transporter-2 inhibition in people with chronic kidney disease: A rationale for the EMPA-KIDNEY study. Clin. Kidney J. 2018, 11, 749–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the management of arterial hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2018, 36, 2284–2309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Niño, M.D.; Sanz, A.B.; Ramos, A.M.; Ruiz-Ortega, M.; Ortiz, A. Translational science in chronic kidney disease. Clin. Sci. (Lond.) 2017, 131, 1617–1629. [Google Scholar] [CrossRef]
- Fernandez-Prado, R.; Esteras, R.; Perez-Gomez, M.V.; Gracia-Iguacel, C.; Gonzalez-Parra, E.; Sanz, A.B.; Ortiz, A.; Sanchez-Niño, M.D. Nutrients Turned into Toxins: Microbiota Modulation of Nutrient Properties in Chronic Kidney Disease. Nutrients 2017, 9, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo-Rodríguez, E.; Pizarro-Sánchez, S.; Sanz, A.B.; Ramos, A.M.; Sanchez-Niño, M.D.; Martin-Cleary, C.; Fernandez-Fernandez, B.; Ortiz, A. Inflammatory Cytokines as Uremic Toxins: “Ni Son Todos Los Que Estan, Ni Estan Todos Los Que Son”. Toxins 2017, 9, 114. [Google Scholar]
- Duranton, F.; Cohen, G.; De Smet, R.; Rodriguez, M.; Jankowski, J.; Vanholder, R.; Argiles, A. European Uremic Toxin Work Group. Norm. Pathol. Conc. Urem. Toxins J. Am. Soc. Nephrol. 2012, 23, 1258–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Fernandez, B.; Izquierdo, M.C.; Valiño-Rivas, L.; Nastou, D.; Sanz, A.B.; Ortiz, A.; Sanchez-Niño, M.D. Albumin downregulates Klotho in tubular cells. Nephrol. Dial. Transplant. 2018, 33, 1712–1722. [Google Scholar] [CrossRef] [Green Version]
- Rossignol, P.; Massy, Z.A.; Azizi, M.; Bakris, G.; Ritz, E.; Covic, A.; Goldsmith, D.; Heine, G.H.; Jager, K.J.; Kanbay, M.; et al. The double challenge of resistant hypertension and chronic kidney disease. Lancet 2015, 386, 1588–1598. [Google Scholar] [CrossRef]
- Firsov, D.; Bonny, O. Circadian rhythms and the kidney. Nat. Rev. Nephrol. 2018, 14, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Firsov, D.; Bonny, O. Circadian regulation of renal function. Kidney Int. 2010, 78, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Nicolas, A.; Madrid, J.A.; Rol, M.A. Day-night contrast as source of health for the human circadian system. Chronobiol. Int. 2014, 31, 382–393. [Google Scholar] [CrossRef]
- Zhang, D.; Pollock, D.M. Diurnal Regulation of Renal Electrolyte Excretion: The Role of Paracrine Factors. Annu. Rev. Physiol. 2019, 82, 343–363. [Google Scholar] [CrossRef] [Green Version]
- Chiou, Y.Y.; Yang, Y.; Rashid, N.; Ye, R.; Selby, C.P.; Sancar, A. Mammalian Period represses and de-represses transcription by displacing CLOCK-BMAL1 from promoters in a Cryptochrome-dependent manner. Proc. Natl. Acad. Sci. USA 2016, 113, E6072–E6079. [Google Scholar] [CrossRef] [Green Version]
- Mészáros, K.; Pruess, L.; Szabó, A.J.; Gondan, M.; Ritz, E.; Schaefer, F. Development of the circadian clockwork in the kidney. Kidney Int. 2014, 86, 915–922. [Google Scholar] [CrossRef] [Green Version]
- Becker, B.K.; Zhang, D.; Soliman, R.; Pollock, D.M. Autonomic nerves and circadian control of renal function. Auton. Neurosci. 2019, 217, 58–65. [Google Scholar] [CrossRef]
- Motohashi, H.; Tahara, Y.; Whittaker, D.S.; Wang, H.B.; Yamaji, T.; Wakui, H.; Haraguchi, A.; Yamazaki, M.; Miyakawa, H.; Hama, K.; et al. The circadian clock is disrupted in mice with adenine-induced tubulointerstitial nephropathy. Kidney Int. 2020. [Google Scholar] [CrossRef] [Green Version]
- Hara, M.; Minami, Y.; Ohashi, M.; Tsuchiya, Y.; Kusaba, T.; Tamagaki, K.; Koike, N.; Umemura, Y.; Inokawa, H.; Yagita, K. Robust circadian clock oscillation and osmotic rhythms in inner medulla reflecting cortico-medullary osmotic gradient rhythm in rodent kidney. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nikolaeva, S.; Ansermet, C.; Centeno, G.; Pradervand, S.; Bize, V.; Mordasini, D.; Henry, H.; Koesters, R.; Maillard, M.; Bonny, O.; et al. Nephron-Specific Deletion of Circadian Clock Gene Bmal1 Alters the Plasma and Renal Metabolome and Impairs Drug Disposition. J. Am. Soc. Nephrol. 2016, 27, 2997–3004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erren, T.C.; Reiter, R.J.; Piekarski, C. Light, timing of biological rhythms, and chronodisruption in man. Naturwissenschaften 2003, 90, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Erren, T.C.; Reiter, R.J. Defining chronodisruption. J. Pineal Res. 2009, 46, 245–247. [Google Scholar] [CrossRef]
- Bonny, O.; Vinciguerra, M.; Gumz, M.L.; Mazzoccoli, G. Molecular bases of circadian rhythmicity in renal physiology and pathology. Nephrol. Dial. Transplant. 2013, 28, 2421–2431. [Google Scholar] [CrossRef] [Green Version]
- Mendez, N.; Torres-Farfan, C.; Salazar, E.; Bascur, P.; Bastidas, C.; Vergara, K.; Spichiger, C.; Halabi, D.; Vio, C.P.; Richter, H.G. Fetal Programming of Renal Dysfunction and High Blood Pressure by Chronodisruption. Front. Endocrinol. 2019, 10, 362. [Google Scholar] [CrossRef] [Green Version]
- Wuerzner, G.; Firsov, D.; Bonny, O. Circadian glomerular function: From physiology to molecular and therapeutical aspects. Nephrol. Dial. Transplant. 2014, 29, 1475–1480. [Google Scholar] [CrossRef] [Green Version]
- Firsov, D.; Tokonami, N.; Bonny, O. Role of the renal circadian timing system in maintaining water and electrolytes homeostasis. Mol. Cell. Endocrinol. 2012, 349, 51–55. [Google Scholar] [CrossRef] [Green Version]
- Argilés, A.; Mourad, G.; Mion, C. Seasonal changes in blood pressure in patients with end-stage renal disease treated with hemodialysis. N. Engl. J. Med. 1998, 339, 1364–1370. [Google Scholar] [CrossRef]
- Knutson, K.L.; Lash, J.; Ricardo, A.C.; Herdegen, J.; Thornton, J.D.; Rahman, M.; Turek, N.; Cohan, J.; Lawrence, J.; Bazzano, L.; et al. Habitual sleep and kidney function in chronic kidney disease: The Chronic Renal Insufficiency Cohort study. J. Sleep Res. 2018, 27, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, N.; Ishigaki, S.; Isobe, S. The pivotal role of melatonin in ameliorating chronic kidney disease by suppression of the renin-angiotensin system in the kidney. Hypertens. Res. 2019, 42, 761–768. [Google Scholar] [CrossRef]
- Voulgaris, A.; Marrone, O.; Bonsignore, M.R.; Steiropoulos, P. Chronic kidney disease in patients with obstructive sleep apnea. Narrat. Rev. Sleep Med. Rev. 2019, 47, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, P.A.; Persu, A.; Agarwal, R.; Burnier, M.; de Leeuw, P.; Ferro, C.J.; Halimi, J.M.; Heine, G.H.; Jadoul, M.; Jarraya, F.; et al. Hypertension in dialysis patients: A consensus document by the European Renal and Cardiovascular Medicine (EURECA-m) working group of the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) and the Hypertension and the Kidney working group of the European Society of Hypertension (ESH). Nephrol. Dial. Transplant. 2017, 32, 620–640. [Google Scholar] [PubMed]
- Bolignano, D.; Rastelli, S.; Agarwal, R.; Fliser, D.; Massy, Z.; Ortiz, A.; Wiecek, A.; Martinez-Castelao, A.; Covic, A.; Goldsmith, D.; et al. Pulmonary hypertension in CKD. Am. J. Kidney Dis. 2013, 61, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Di Daniele, N.; Fegatelli, D.A.; Rovella, V.; Castagnola, V.; Gabriele, M.; Scuteri, A. Circadian blood pressure patterns and blood pressure control in patients with chronic kidney disease. Atherosclerosis 2017, 267, 139–145. [Google Scholar] [CrossRef]
- Ruiz-Hurtado, G.; Ruilope, L.; De la Sierra, A.; Sarafidis, P.; De la Cruz, J.; Gorostidi, M.; Segura, J.; Vinyoles, E.; Banegas, J. Association between High and Very High Albuminuria and Nighttime Blood Pressure: Influence of Diabetes and Chronic Kidney Disease. Diabetes Care 2016, 39, 1729–1737. [Google Scholar] [CrossRef] [Green Version]
- Ando, D.; Yasuda, G. Circadian Blood Pressure Rhythm Is Changed by Improvement in Hypoalbuminemia and Massive Proteinuria in Patients with Minimal Change Nephrotic Syndrome. Cardiorenal. Med. 2016, 6, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Ohkubo, T.; Hozawa, A.; Yamaguchi, J.; Kikuya, M.; Ohmori, K.; Michimata, M.; Matsubara, M.; Hashimoto, J.; Hoshi, H.; Araki, T.; et al. Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: The Ohasama study. J. Hypertens. 2002, 20, 2183–2189. [Google Scholar] [CrossRef]
- Fedecostante, M.; Spannella, F.; Cola, G.; Espinosa, E.; Dessì-Fulgheri, P.; Sarzani, R. Chronic kidney disease is characterized by “double trouble” higher pulse pressure plus night-time systolic blood pressure and more severe cardiac damage. PLoS ONE 2014, 9, e86155. [Google Scholar] [CrossRef]
- Huang, J.T.; Cheng, H.M.; Yu, W.C.; Lin, Y.P.; Sung, S.H.; Chen, C.H. Increased Nighttime Pulse Pressure Variability but Not Ambulatory Blood Pressure Levels Predicts 14-Year All-Cause Mortality in Patients on Hemodialysis. Hypertension 2019, 74, 660–668. [Google Scholar] [CrossRef] [PubMed]
- Tokonami, N.; Mordasini, D.; Pradervand, S.; Centeno, G.; Jouffe, C.; Maillard, M.; Bonny, O.; Gachon, F.; Gomez, R.A.; Sequeira-Lopez, M.L. Local renal circadian clocks control fluid-electrolyte homeostasis and BP. J. Am. Soc. Nephrol. 2014, 25, 1430–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ivy, J.R.; Jones, N.K.; Costello, H.M.; Mansley, M.K.; Peltz, T.S.; Flatman, P.W.; Bailey, M.A. Glucocorticoid receptor activation stimulates the sodium-chloride cotransporter and influences the diurnal rhythm of its phosphorylation. Am. J. Physiol. Renal Physiol. 2019, 317, F1536–F1548. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, A.; Kawamoto, T.; Noshiro, M.; Ueno, T.; Doi, S.; Honda, K.; Masaki, T.; Higashi, Y.; Kato, Y. Dec1 and CLOCK Regulate Na. Hypertension 2018, 72, 746–754. [Google Scholar] [CrossRef]
- Valiño-Rivas, L.; Cuarental, L.; Agustin, M.; Husi, H.; Cannata-Ortiz, P.; Sanz, A.B.; Mischak, H.; Ortiz, A.; Sanchez-Niño, M.D. MAGE genes in the kidney: Identification of MAGED2 as upregulated during kidney injury and in stressed tubular cells. Nephrol. Dial. Transplant. 2019, 34, 1498–1507. [Google Scholar] [CrossRef]
- Gil, R.B.; Ortiz, A.; Sanchez-Niño, M.D.; Markoska, K.; Schepers, E.; Vanholder, R.; Glorieux, G.; Schmitt-Kopplin, P.; Heinzmann, S. Increased urinary osmolyte excretion indicates chronic kidney disease severity and progression rate. Nephrol. Dial. Transplant. 2018, 33, 2156–2164. [Google Scholar] [CrossRef]
- Myung, J.; Wu, M.Y.; Lee, C.Y.; Rahim, A.R.; Truong, V.H.; Wu, D.; Piggins, H.D.; Wu, M.S. The Kidney Clock Contributes to Timekeeping by the Master Circadian Clock. Int. J. Mol. Sci. 2019, 20, 2765. [Google Scholar] [CrossRef] [Green Version]
- Gansevoort, R.; Arici, M.; Benzing, T.; Birn, H.; Capasso, G.; Covic, A.; Devuyst, O.; Drechsler, C.; Eckardt, K.U.; Emma, F.; et al. Recommendations for the use of tolvaptan in autosomal dominant polycystic kidney disease: A position statement on behalf of the ERA-EDTA Working Groups on Inherited Kidney Disorders and European Renal Best Practice. Nephrol. Dial. Transplant. 2016, 31, 337–348. [Google Scholar] [CrossRef]
- Torres, V.E.; Chapman, A.B.; Devuyst, O.; Gansevoort, R.T.; Perrone, R.D.; Koch, G.; Ouyang, J.; McQuade, R.D.; Blais, J.D.; Czerwiec, F.S.; et al. Tolvaptan in Later-Stage Autosomal Dominant Polycystic Kidney Disease. N. Engl. J. Med. 2017, 377, 1930–1942. [Google Scholar] [CrossRef]
- Montero, D.; Diaz-Canestro, C.; Oberholzer, L.; Lundby, C. The role of blood volume in cardiac dysfunction and reduced exercise tolerance in patients with diabetes. Lancet Diabetes Endocrinol. 2019, 7, 807–816. [Google Scholar] [CrossRef]
- Parizadeh, S.M.; Ghandehari, M.; Parizadeh, M.R.; Ferns, G.A.; Ghayour-Mobarhan, M.; Avan, A.; Hassanian, S. The diagnostic and prognostic value of copeptin in cardiovascular disease, current status, and prospective. J. Cell. Biochem. 2018, 119, 7913–7923. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, E.E.; Johnson, E.C.; Yusifova, M.; Bruns, D.R. The renal molecular clock: Broken by aging and restored by exercise. Am. J. Physiol. Renal Physiol. 2019, 317, F1087–F1093. [Google Scholar] [CrossRef]
- Batinga, H.; Martinez-Nicolas, A.; Zornoza-Moreno, M.; Sánchez-Solis, M.; Larqué, E.; Mondéjar, M.T.; Moreno-Casbas, M.; García, F.J.; Campos, M.; Rol, M.A.; et al. Ontogeny and aging of the distal skin temperature rhythm in humans. Age 2015, 37, 29. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, N.; Ishigaki, S.; Isobe, S.; Matsuyama, T.; Sato, T.; Fujikura, T.; Tsuji, T.; Kato, A.; Yasuda, H. Salt Loading Aggravates the Relationship between Melatonin and Proteinuria in Patients with Chronic Kidney Disease. Intern. Med. 2019, 58, 1557–1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speed, J.S.; Hyndman, K.A.; Roth, K.; Heimlich, J.B.; Kasztan, M.; Fox, B.M.; Johnston, J.G.; Becker, B.K.; Jin, C.; Gamble, K.L.; et al. High dietary sodium causes dyssynchrony of the renal molecular clock in rats. Am. J. Physiol. Renal Physiol. 2018, 314, F89–F98. [Google Scholar] [CrossRef] [PubMed]
- Daimiel-Ruiz, L.; Klett-Mingo, M.; Konstantinidou, V.; Micó, V.; Aranda, J.F.; García, B.; Martínez-Botas, J.; Dávalos, A.; Fernández-Hernando, C.; Ordovás, J.M. Dietary lipids modulate the expression of miR-107, a miRNA that regulates the circadian system. Mol. Nutr. Food Res. 2015, 59, 1865–1878. [Google Scholar] [CrossRef] [Green Version]
- Laermans, J.; Depoortere, I. Chronobesity: Role of the circadian system in the obesity epidemic. Obes. Rev. 2016, 17, 108–125. [Google Scholar] [CrossRef]
- Galindo Muñoz, J.S.; Gómez Gallego, M.; Díaz Soler, I.; Barberá Ortega, M.C.; Martínez Cáceres, C.M.; Hernández Morante, J.J. Effect of a chronotype-adjusted diet on weight loss effectiveness: A randomized clinical trial. Clin. Nutr. 2019. [Google Scholar] [CrossRef]
- Bandín, C.; Scheer, F.A.; Luque, A.J.; Ávila-Gandía, V.; Zamora, S.; Madrid, J.A. Meal timing affects glucose tolerance, substrate oxidation and circadian-related variables: A randomized, crossover trial. Int. J. Obes. 2015, 39, 828–833. [Google Scholar]
- Challet, E. The circadian regulation of food intake. Nat. Rev. Endocrinol. 2019, 15, 393–405. [Google Scholar] [CrossRef]
- Parkar, S.G.A.; Cheeseman, J.F. Potential Role for the Gut Microbiota in Modulating Host Circadian Rhythms and Metabolic Health. Microorganisms 2019, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilera-Correa, J.-J.; Madrazo-Clemente, P.; Martínez-Cuesta, M.D.C.; Peláez, C.; Ortiz, A.; Sánchez-Niño, M.D.; Esteban, J.; Requena, T. Lyso-Gb3 modulates the gut microbiota and decreases butyrate production. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perna, A.F.; Glorieux, G.; Zacchia, M.; Trepiccione, F.; Capolongo, G.; Vigorito, C.; Anishchenko, E.; Ingrosso, D. The role of the intestinal microbiota in uremic solute accumulation: A focus on sulfur compounds. J. Nephrol. 2019, 32, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Joossens, M.; Faust, K.; Gryp, T.; Nguyen, A.T.L.; Wang, J.; Eloot, S.; Schepers, E.; Dhondt, A.; Pletinck, A.; Vieira-Silva, S.; et al. Gut microbiota dynamics and uraemic toxins: One size does not fit all. Gut 2019, 68, 2257–2260. [Google Scholar] [CrossRef]
- Erren, T.C.; Morfeld, P.; Groß, J.V.; Wild, U.; Lewis, P. IARC 2019: “Night shift work” is probably carcinogenic: What about disturbed chronobiology in all walks of life? J. Occup. Med. Toxicol. 2019, 14, 29. [Google Scholar] [CrossRef]
- Uhm, J.Y.; Kim, H.R.; Kang, G.H.; Choi, Y.G.; Park, T.H.; Kim, S.Y.; Chang, S.S.; Choo, W.O. The association between shift work and chronic kidney disease in manual labor workers using data from the Korea National Health and Nutrition Examination Survey (KNHANES 2011–2014). Ann. Occup. Environ. Med. 2018, 30, 69. [Google Scholar] [CrossRef]
- Sanz, A.B.; Ruiz-Andres, O.; Sanchez-Niño, M.D.; Ruiz-Ortega, M.; Ramos, A.M.; Ortiz, A. Out of the TWEAKlight: Elucidating the Role of Fn14 and TWEAK in Acute Kidney Injury. Semin. Nephrol. 2016, 36, 189–198. [Google Scholar] [CrossRef]
- Sanz, A.B.; Izquierdo, M.C.; Sanchez-Niño, M.D.; Ucero, A.C.; Egido, J.; Ruiz-Ortega, M.; Ramos, A.M.; Putterman, C.; Ortiz, A. TWEAK and the progression of renal disease: Clinical translation. Nephrol. Dial. Transplant. 2014, 29 (Suppl. 1), i54–i62. [Google Scholar] [CrossRef] [Green Version]
- Valiño-Rivas, L.; Vaquero, J.J.; Sucunza, D.; Gutierrez, S.; Sanz, A.B.; Fresno, M.; Ortiz, A.; Sanchez-Niño, M.D. NIK as a Druggable Mediator of Tissue Injury. Trends Mol. Med. 2019, 25, 341–360. [Google Scholar] [CrossRef]
- Valiño-Rivas, L.; Gonzalez-Lafuente, L.; Sanz, A.B.; Ruiz-Ortega, M.; Ortiz, A.; Sanchez-Niño, M.D. Non-canonical NFκB activation promotes chemokine expression in podocytes. Sci. Rep. 2016, 6, 28857. [Google Scholar] [CrossRef] [Green Version]
- Sanz, A.B.; Sanchez-Niño, M.D.; Izquierdo, M.C.; Jakubowski, A.; Justo, P.; Blanco-Colio, L.M.; Blanco-Colio, L.M.; Ruiz-Ortega, M.; Selgas, R.; Egido, J.; et al. TWEAK activates the non-canonical NFkappaB pathway in murine renal tubular cells: Modulation of CCL21. PLoS ONE 2010, 5, e8955. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.; Husi, H.; Gonzalez-Lafuente, L.; Valiño-Rivas, L.; Fresno, M.; Sanz, A.B.; Mullen, W.; Albalat, A.; Mezzano, S.; Vlahou, T.; et al. Mitogen-Activated Protein Kinase 14 Promotes AKI. J. Am. Soc. Nephrol. 2017, 28, 823–836. [Google Scholar] [CrossRef] [Green Version]
- Cuarental, L.; Sucunza-Sáenz, D.; Valiño-Rivas, L.; Fernandez-Fernandez, B.; Sanz, A.B.; Ortiz, A.; Vaquero, J.J.; Sanchez-Niño, M.D. MAP3K kinases and kidney injury. Nefrologia 2019, 39, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Sanz, A.B.; Sanchez-Niño, M.D.; Ramos, A.M.; Moreno, J.A.; Santamaria, B.; Ruiz-Ortega, M.; Mullen, W.; Albalat, A.; Mezzano, S.; Vlahou, T.; et al. NF-kappaB in renal inflammation. J. Am. Soc. Nephrol. 2010, 21, 1254–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poveda, J.; Tabara, L.C.; Fernandez-Fernandez, B.; Martin-Cleary, C.; Sanz, A.B.; Selgas, R.; Ortiz, A.; Sanchez-Niño, M.D. TWEAK/Fn14 and Non-Canonical NF-kappaB Signaling in Kidney Disease. Front. Immunol. 2013, 4, 447. [Google Scholar] [CrossRef] [Green Version]
- Bellet, M.M.; Zocchi, L.; Sassone-Corsi, P. The RelB subunit of NFκB acts as a negative regulator of circadian gene expression. Cell Cycle 2012, 11, 3304–3311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poveda, J.; Sanz, A.B.; Carrasco, S.; Ruiz-Ortega, M.; Cannata-Ortiz, P.; Sanchez-Niño, M.D.; Ortiz, A. Bcl3: A regulator of NF-κB inducible by TWEAK in acute kidney injury with anti-inflammatory and antiapoptotic properties in tubular cells. Exp. Mol. Med. 2017, 49, e352. [Google Scholar] [CrossRef] [Green Version]
- Moreno, J.A.; Izquierdo, M.C.; Sanchez-Niño, M.D.; Suárez-Alvarez, B.; Lopez-Larrea, C.; Jakubowski, A.; Blanco, J.; Ramirez, R.; Selgas, R.; Ruiz-Ortega, M.; et al. The inflammatory cytokines TWEAK and TNFα reduce renal klotho expression through NFκB. J. Am. Soc. Nephrol. 2011, 22, 1315–1325. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Andres, O.; Sanchez-Niño, M.D.; Moreno, J.A.; Ruiz-Ortega, M.; Ramos, A.M.; Sanz, A.B.; Ortiz, A. Downregulation of kidney protective factors by inflammation: Role of transcription factors and epigenetic mechanisms. Am. J. Physiol. Renal Physiol. 2016, 311, F1329–F1340. [Google Scholar] [CrossRef] [Green Version]
- Ruiz-Andres, O.; Suarez-Alvarez, B.; Sánchez-Ramos, C.; Monsalve, M.; Sanchez-Niño, M.D.; Ruiz-Ortega, M.; Egido, J.; Ortiz, A.; Sanz, A.B. The inflammatory cytokine TWEAK decreases PGC-1α expression and mitochondrial function in acute kidney injury. Kidney Int. 2016, 89, 399–410. [Google Scholar] [CrossRef] [Green Version]
- Millet, P.; McCall, C.; Yoza, B. RelB: An outlier in leukocyte biology. J. Leukoc. Biol. 2013, 94, 941–951. [Google Scholar] [CrossRef]
- Sato, F.; Otsuka, T.; Kohsaka, A.; Le, H.T.; Bhawal, U.K.; Muragaki, Y. Smad3 Suppresses Epithelial Cell Migration and Proliferation via the Clock Gene Dec1, Which Negatively Regulates the Expression of Clock Genes Dec2 and Per1. Am. J. Pathol. 2019, 189, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Sallée, M.; Dou, L.; Cerini, C.; Poitevin, S.; Brunet, P.; Burtey, S. The aryl hydrocarbon receptor-activating effect of uremic toxins from tryptophan metabolism: A new concept to understand cardiovascular complications of chronic kidney disease. Toxins 2014, 6, 934–949. [Google Scholar] [CrossRef]
- Castillo-Rodriguez, E.; Fernandez-Prado, R.; Esteras, R.; Perez-Gomez, M.V.; Gracia-Iguacel, C.; Fernandez-Fernandez, B.; Kanbay, M.; Tejedor, A.; Lazaro, A.; Ruiz-Ortega, M.; et al. Impact of Altered Intestinal Microbiota on Chronic Kidney Disease Progression. Toxins 2018, 10, 300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tischkau, S.A. Mechanisms of circadian clock interactions with aryl hydrocarbon receptor signalling. Eur. J. Neurosci. 2019, 51, 379–395. [Google Scholar] [CrossRef] [Green Version]
- Jaeger, C.; Khazaal, A.Q.; Xu, C.; Sun, M.; Krager, S.L.; Tischkau, S.A. Aryl Hydrocarbon Receptor Deficiency Alters Circadian and Metabolic Rhythmicity. J. Biol. Rhythms 2017, 32, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; Jansen, K.; Neven, E.; Poesen, R.; Othman, A.; van Mil, A.; Sluijter, J.; Sastre Torano, J.; Zaal, E.A.; Berkers, C.R.; et al. Remote sensing and signaling in kidney proximal tubules stimulates gut microbiome-derived organic anion secretion. Proc. Natl. Acad. Sci. USA 2019, 116, 16105–16110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, J.S.; Borges, N.A.; Anjos, J.S.D.; Nakao, L.S.; Stockler-Pinto, M.B.; Paiva, B.R.; Cardoso-Weide, L.C.; Cardozo, L.F.M.F.; Mafra, D. Aryl Hydrocarbon Receptor and Uremic Toxins from the Gut Microbiota in Chronic Kidney Disease Patients: Is There a Relationship between Them? Biochemistry 2019, 58, 2054–2060. [Google Scholar] [CrossRef]
- Addi, T.; Poitevin, S.; McKay, N.; El Mecherfi, K.E.; Kheroua, O.; Jourde-Chiche, N.; de Macedo, A.; Gondouin, B.; Cerini, C.; Brunet, P.; et al. Mechanisms of tissue factor induction by the uremic toxin indole-3 acetic acid through aryl hydrocarbon receptor/nuclear factor-kappa B signaling pathway in human endothelial cells. Arch. Toxicol. 2019, 93, 121–136. [Google Scholar] [CrossRef]
- Dimova, E.Y.; Jakupovic, M.; Kubaichuk, K.; Mennerich, D.; Chi, T.F.; Tamanini, F.; Oklejewicz, M.; Hänig, J.; Byts, N.; Mäkelä, K.A.; et al. The Circadian Clock Protein CRY1 Is a Negative Regulator of HIF-1α. iScience 2019, 13, 284–304. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Morinibu, A.; Koyasu, S.; Goto, Y.; Hiraoka, M.; Harada, H. A circadian clock gene, PER2, activates HIF-1 as an effector molecule for recruitment of HIF-1α to promoter regions of its downstream genes. FEBS J. 2017, 284, 3804–3816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckle, T.; Hartmann, K.; Bonney, S.; Reithel, S.; Mittelbronn, M.; Walker, L.A.; Lowes, B.D.; Han, J.; Borchers, C.H.; Buttrick, P.M.; et al. Adora2b-elicited Per2 stabilization promotes a HIF-dependent metabolic switch crucial for myocardial adaptation to ischemia. Nat. Med. 2012, 18, 774–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peek, C.B.; Levine, D.C.; Cedernaes, J.; Taguchi, A.; Kobayashi, Y.; Tsai, S.J.; Bonar, N.A.; Mc, M.R.; Ramsey, K.M.; Bass, J. Circadian Clock Interaction with HIF1α Mediates Oxygenic Metabolism and Anaerobic Glycolysis in Skeletal Muscle. Cell Metab. 2017, 25, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egg, M.; Köblitz, L.; Hirayama, J.; Schwerte, T.; Folterbauer, C.; Kurz, A.; Fiechtner, B.; Möst, M.; Salvenmoser, W.; Sassone, P.; et al. Linking oxygen to time: The bidirectional interaction between the hypoxic signaling pathway and the circadian clock. Chronobiol. Int. 2013, 30, 510–529. [Google Scholar] [CrossRef]
- Chen, N.; Hao, C.; Liu, B.C.; Lin, H.; Wang, C.; Xing, C.; Liang, X.; Jiang, G.; Liu, Z.; Li, X.; et al. Roxadustat Treatment for Anemia in Patients Undergoing Long-Term Dialysis. N. Engl. J. Med. 2019, 381, 1011–1022. [Google Scholar] [CrossRef] [PubMed]
- Jaeger, C.; Xu, C.; Sun, M.; Krager, S.; Tischkau, S.A. Aryl hydrocarbon receptor-deficient mice are protected from high fat diet-induced changes in metabolic rhythms. Chronobiol. Int. 2017, 34, 318–336. [Google Scholar] [CrossRef]
- Martinez-Nicolas, A.; Ortiz-Tudela, E.; Rol, M.A.; Madrid, J.A. Uncovering different masking factors on wrist skin temperature rhythm in free-living subjects. PLoS ONE 2013, 8, e61142. [Google Scholar] [CrossRef]
- Corbalán-Tutau, M.D.; Gómez-Abellán, P.; Madrid, J.A.; Canteras, M.; Ordovás, J.M.M. Toward a chronobiological characterization of obesity and metabolic syndrome in clinical practice. Clin. Nutr. 2015, 34, 477–483. [Google Scholar] [CrossRef]
- Wei, N.; Gumz, M.L.; Layton, A.T. Predicted effect of circadian clock modulation of NHE3 of a proximal tubule cell on sodium transport. Am. J. Physiol. Renal Physiol. 2018, 315, F665–F676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMullan, C.J.; Curhan, G.C.; Forman, J.P. Association of short sleep duration and rapid decline in renal function. Kidney Int. 2016, 89, 1324–1330. [Google Scholar] [CrossRef] [Green Version]
- De Lavallaz, L.; Musso, C.G. Chronobiology in nephrology: The influence of circadian rhythms on renal handling of drugs and renal disease treatment. Int. Urol. Nephrol. 2018, 50, 2221–2228. [Google Scholar] [CrossRef] [PubMed]
- Hermida, R.C.; Ayala, D.E.; Mojón, A.; Fernández, J.R. Risk of incident chronic kidney disease is better reduced by bedtime than upon-awakening ingestion of hypertension medications. Hypertens. Res. 2018, 41, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Niño, M.D.; Sanz, A.B.; Ramos, A.M.; Fernandez-Fernandez, B.; Ortiz, A. Clinical proteomics in kidney disease as an exponential technology: Heading towards the disruptive phase. Clin. Kidney J. 2017, 10, 188–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.; Hao, C.; Peng, X.; Lin, H.; Yin, A.; Hao, L.; Tao, Y.; Liang, X.; Liu, Z.; Xing, C. Roxadustat for Anemia in Patients with Kidney Disease Not Receiving Dialysis. N. Engl. J. Med. 2019, 381, 1001–1010. [Google Scholar] [CrossRef]
- Asfar, B.; Asfar, R.; Sag, A.; Kanbay, A.; Korkmaz, H.; Cipolla-Neto, J.; Covic, A.; Ortiz, A.; Kanbay, M. Sweet Dreams: Therapeutic Insights, Targeting Imaging and Physiologic Evidence Linking Sleep, Melatonin, and Diabetic Nephropathy. Clin. Kidney J. 2019. accepted. [Google Scholar]
Figure 1.
Canonical clock genes and the basic regulatory loop: impact on the kidney of genetic defects. In the most basic regulatory loop, Clock and Bmal1 are transcription factors that promote Cry and Per gene expression, and Cry and Per proteins, in turn, suppress Clock/Bmal1 induction of their Cry and Per transcription. Genetic disruption of some canonical clock genes has yielded renal-hypertension phenotypes as illustrated above for Clock, Bmal1, and Per1 in mice. Clock KO mice display loss of water and electrolyte excretion rhythmicity as well as differential responses to induction of kidney fibrosis, which appears specific of the driver of fibrosis (worse unilateral ureteral obstruction (UUO)-induced fibrosis but milder sodium overload-induced fibrosis). Bmal1 KO mice display accelerated aging, loss of rhythmicity of water excretion as well as non-dipping hypotension (red line) as compared to the normal blood pressure circadian rhythm (green line). Per1 KO mice display non-dipping hypertension (red line) as compared to the normal blood pressure circadian rhythm (green line).
Figure 1.
Canonical clock genes and the basic regulatory loop: impact on the kidney of genetic defects. In the most basic regulatory loop, Clock and Bmal1 are transcription factors that promote Cry and Per gene expression, and Cry and Per proteins, in turn, suppress Clock/Bmal1 induction of their Cry and Per transcription. Genetic disruption of some canonical clock genes has yielded renal-hypertension phenotypes as illustrated above for Clock, Bmal1, and Per1 in mice. Clock KO mice display loss of water and electrolyte excretion rhythmicity as well as differential responses to induction of kidney fibrosis, which appears specific of the driver of fibrosis (worse unilateral ureteral obstruction (UUO)-induced fibrosis but milder sodium overload-induced fibrosis). Bmal1 KO mice display accelerated aging, loss of rhythmicity of water excretion as well as non-dipping hypotension (red line) as compared to the normal blood pressure circadian rhythm (green line). Per1 KO mice display non-dipping hypertension (red line) as compared to the normal blood pressure circadian rhythm (green line).
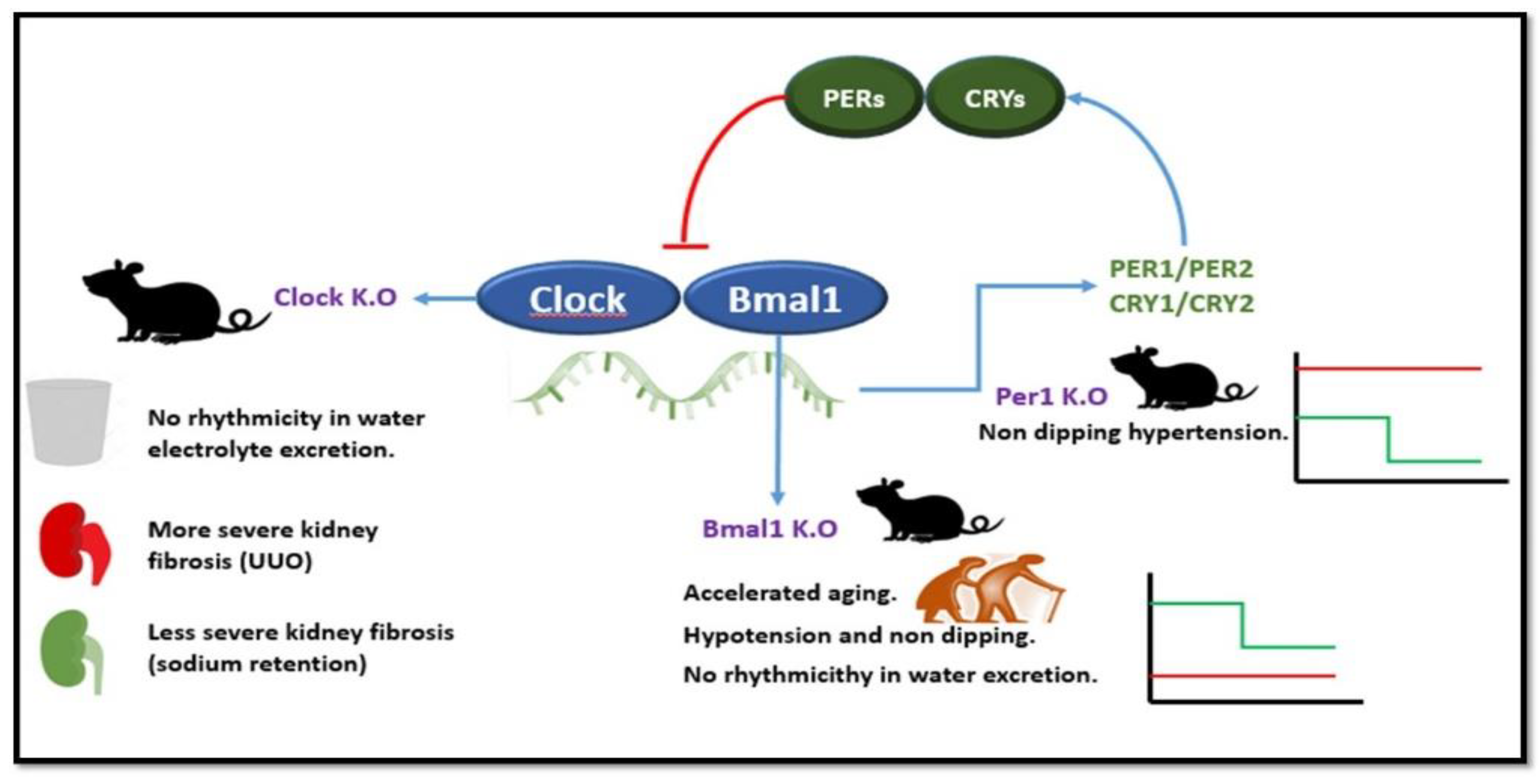
Figure 2.
Concepts of circadian disruption, chronodisturbance and chronodisruption. As compared to a normal circadian rhythm, circadian disruptions are characterized by altered circadian rhythm that may be short or long lived. Chronodisturbance is a chronic disruption of circadian rhythms that somehow leads to adaptive phenomena that limit its negative impact. Chronodisruption is a chronic disruption of circadian rhythms that results in disease. Chronodisruptors (not shown) are the factors driving chronodisruption. The normal circadian rhythm is shown as a green line in the left panel and as a discontinuous line in the other panels. A red line represents the altered circadian rhythm in the three left panels. Please note the different timelines shown in the horizontal axis, with chronodisturbance and chronodisruption implying chronicity.
Figure 2.
Concepts of circadian disruption, chronodisturbance and chronodisruption. As compared to a normal circadian rhythm, circadian disruptions are characterized by altered circadian rhythm that may be short or long lived. Chronodisturbance is a chronic disruption of circadian rhythms that somehow leads to adaptive phenomena that limit its negative impact. Chronodisruption is a chronic disruption of circadian rhythms that results in disease. Chronodisruptors (not shown) are the factors driving chronodisruption. The normal circadian rhythm is shown as a green line in the left panel and as a discontinuous line in the other panels. A red line represents the altered circadian rhythm in the three left panels. Please note the different timelines shown in the horizontal axis, with chronodisturbance and chronodisruption implying chronicity.

{kind=link}
{kind=link}
Table 1.
Some examples of kidney functions which have circadian rhythms.
| Glomeruli | Circulation and Interstitial | Tubular |
|---|---|---|
| Glomerular filtration rate | Renal plasma flow | Water and electrolyte (sodium, potassium, calcium, magnesium, phosphate) excretion and corticomedullary interstitial osmolarity gradient |
| Kidney oxygenation and erythropoietin production | H+ excretion |
Table 2.
Examples of potential chronodisruptors in chronic kidney disease (CKD) patients.
| Diet | Other Lifestyle Factors | Endogenous Factors |
|---|---|---|
| Dietary components, e.g., sodium | Night shift work | Gut microbiota and microbiota-associated uremic toxins |
| Mistimed eating | Kidney inflammation, non-canonical NFκB activation and RelB | |
| Mediators of kidney fibrosis such as Smad3 |
Table 3.
Some key answered questions regarding chronodisruption, chronodisruptors and CKD.
| When Does Chronodisruption Start in CKD Natural History? | What Are the Key Chronodisruptors in CKD and What Are Their Targets? Can Chronodisruptors Be Targeted Therapeutically? | Other Questions |
|---|---|---|
| Before or after the current GFR threshold to define CKD? | Can chronodisruptors be modified by altering the diet or timing of meals? | Is basic research in CKD tainted by chronodisruption resulting from performing mouse and rat experiments during daytime, which should be their inactive period? |
| Is a decreased GFR needed to trigger CKD-associated chronodisruption? | Or by altering the microbiota? | To what extent the age-associated loss of renal function contributes to age-associated circadian rhythm abnormalities? |
| Or is pathological albuminuria sufficient to trigger chronodisruption? | Or by drugs modulating their signaling pathways? | |
| Does therapeutic targeting of CKD-related chronodisruptors improve outcomes? | ||
| Has melatonin any role in managing CKD? | ||
| Has chronopharmacology a role in CKD? |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Carriazo, S.; Ramos, A.M.; Sanz, A.B.; Sanchez-Niño, M.D.; Kanbay, M.; Ortiz, A. Chronodisruption: A Poorly Recognized Feature of CKD. Toxins 2020, 12, 151. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030151
AMA Style
Carriazo S, Ramos AM, Sanz AB, Sanchez-Niño MD, Kanbay M, Ortiz A. Chronodisruption: A Poorly Recognized Feature of CKD. Toxins. 2020; 12(3):151. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030151
Chicago/Turabian StyleCarriazo, Sol, Adrián M Ramos, Ana B Sanz, Maria Dolores Sanchez-Niño, Mehmet Kanbay, and Alberto Ortiz. 2020. "Chronodisruption: A Poorly Recognized Feature of CKD" Toxins 12, no. 3: 151. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030151
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.