Anatomical Considerations When Treating Compensatory Hypertrophy of the Upper Part of the Masseter after Long-Term Botulinum Neurotoxin Type A Injections

 , ,
, ,
Abstract
:1. Introduction
2. Results
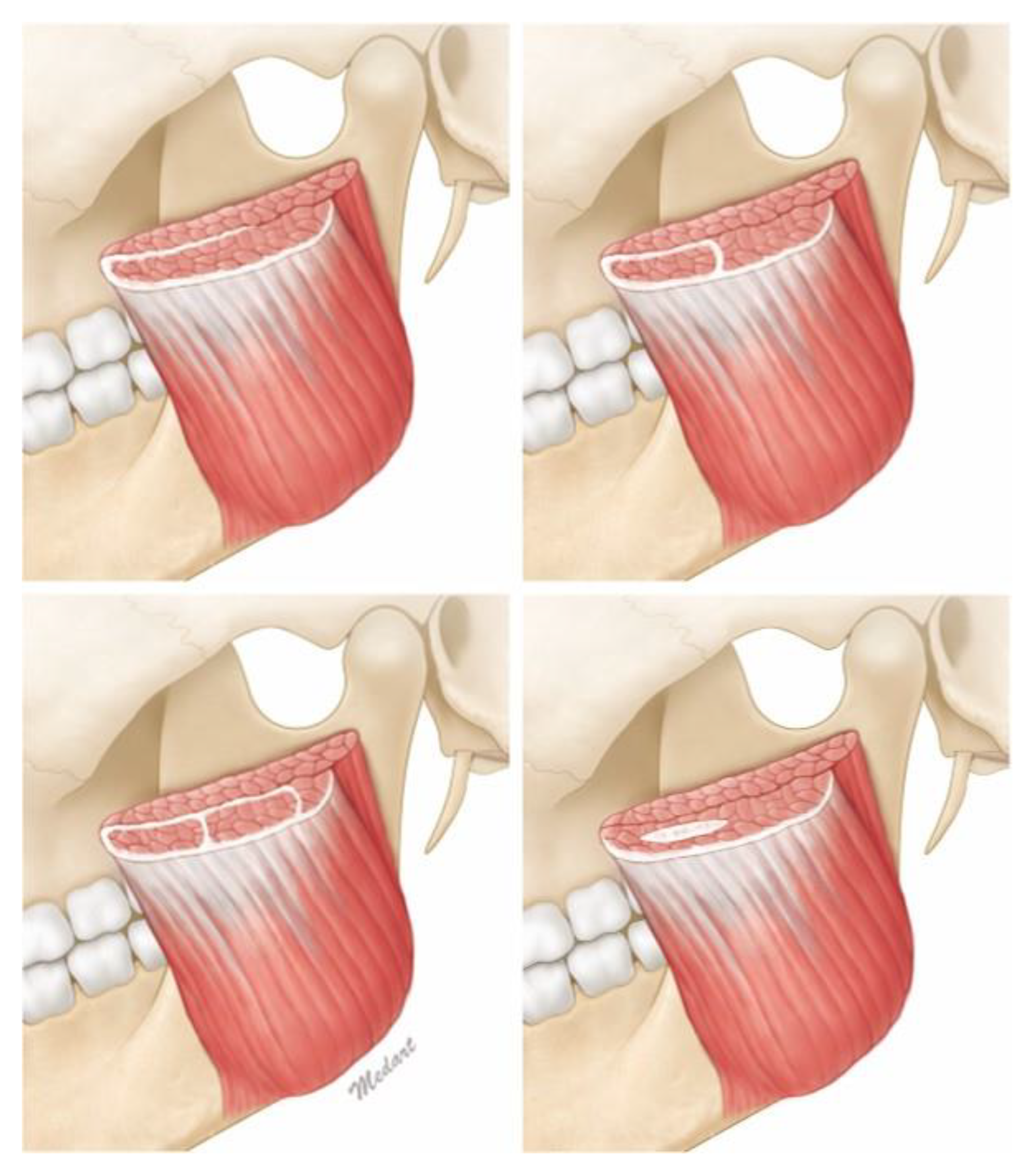
- Type 1. Continuous patterns
- ○
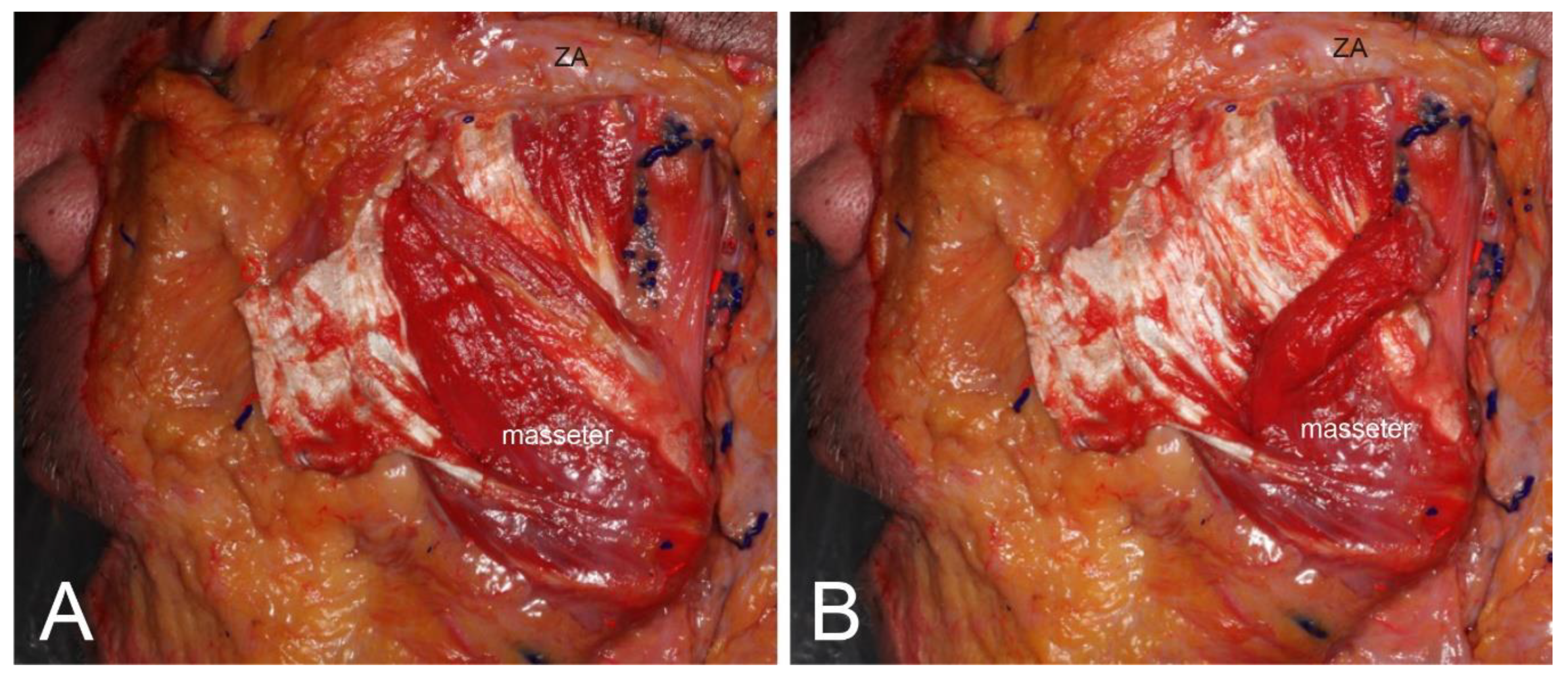
- 1a. Simply continuous pattern, in which the deep and the superficial tendons of the masseter are connected and surround the muscle belly.
- ○
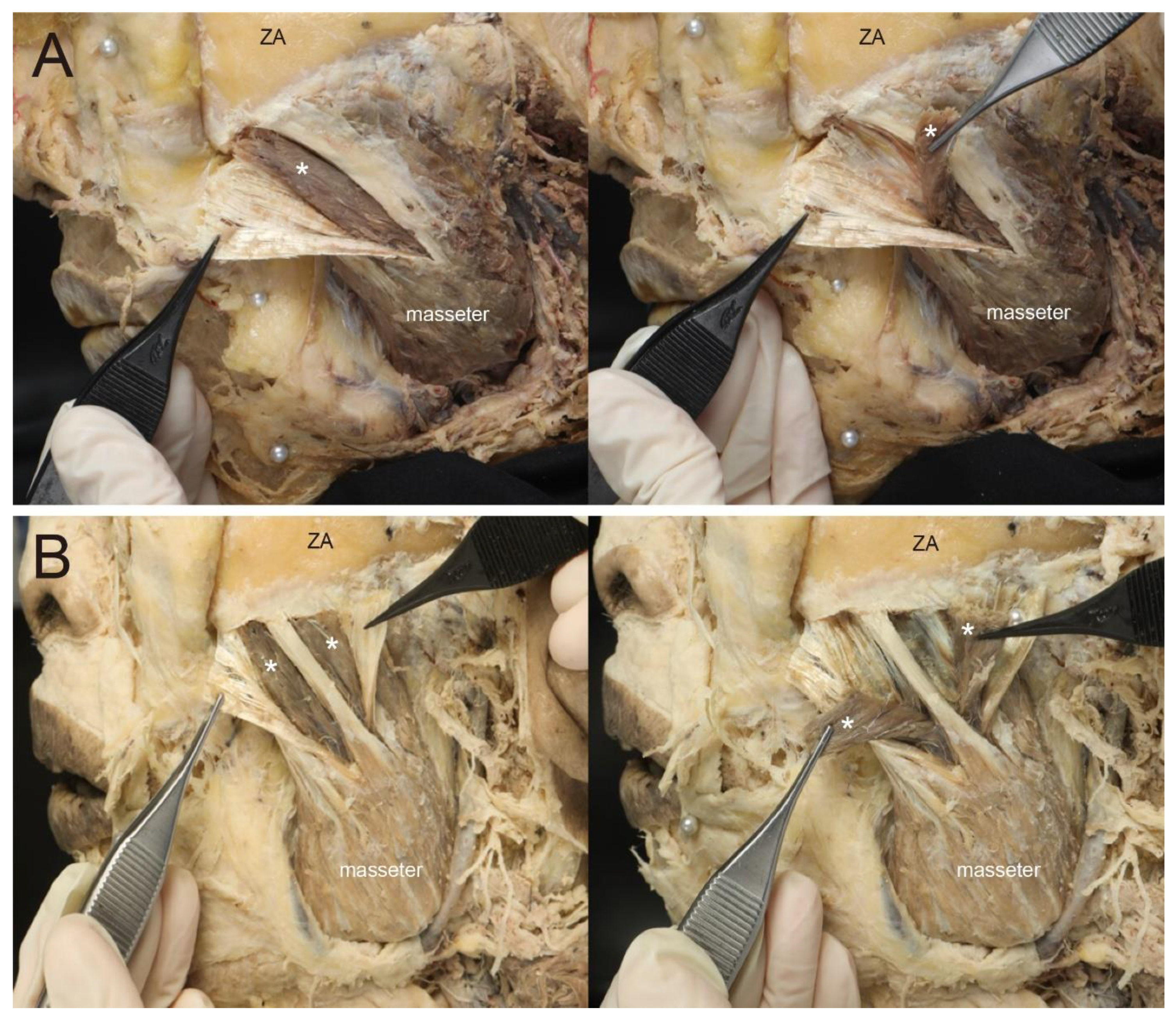
- 1b. One-unit capsule pattern, in which the deep tendons completely enclose the parts of the muscle belly as a single capsule.
- ○
- 1c. Two-unit capsules pattern, in which the deep tendons completely enclose the parts of the muscle belly as two capsules.
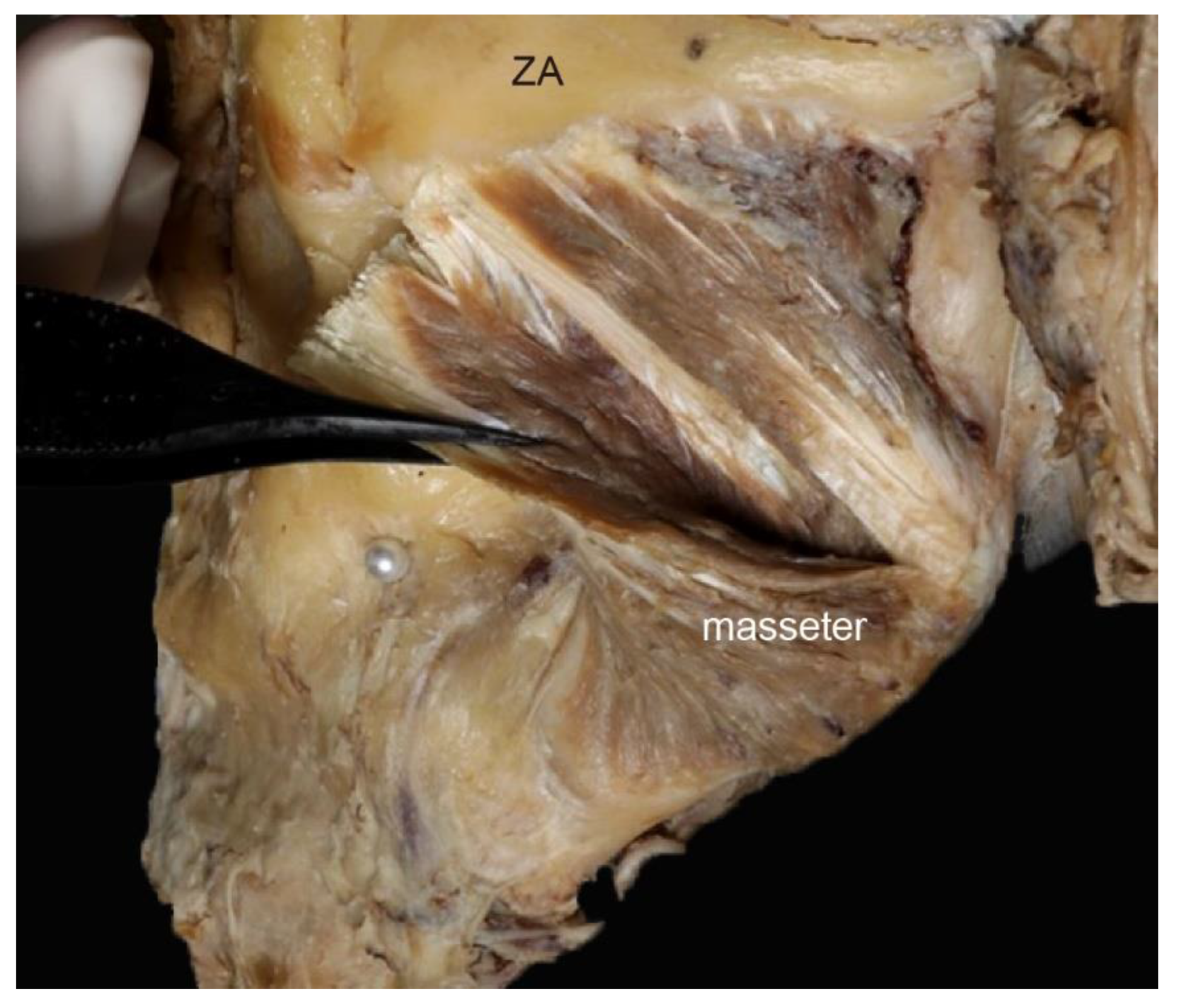
- Type 2. Interdigitation pattern, in which the deep tendons are located sporadically in the muscle belly.
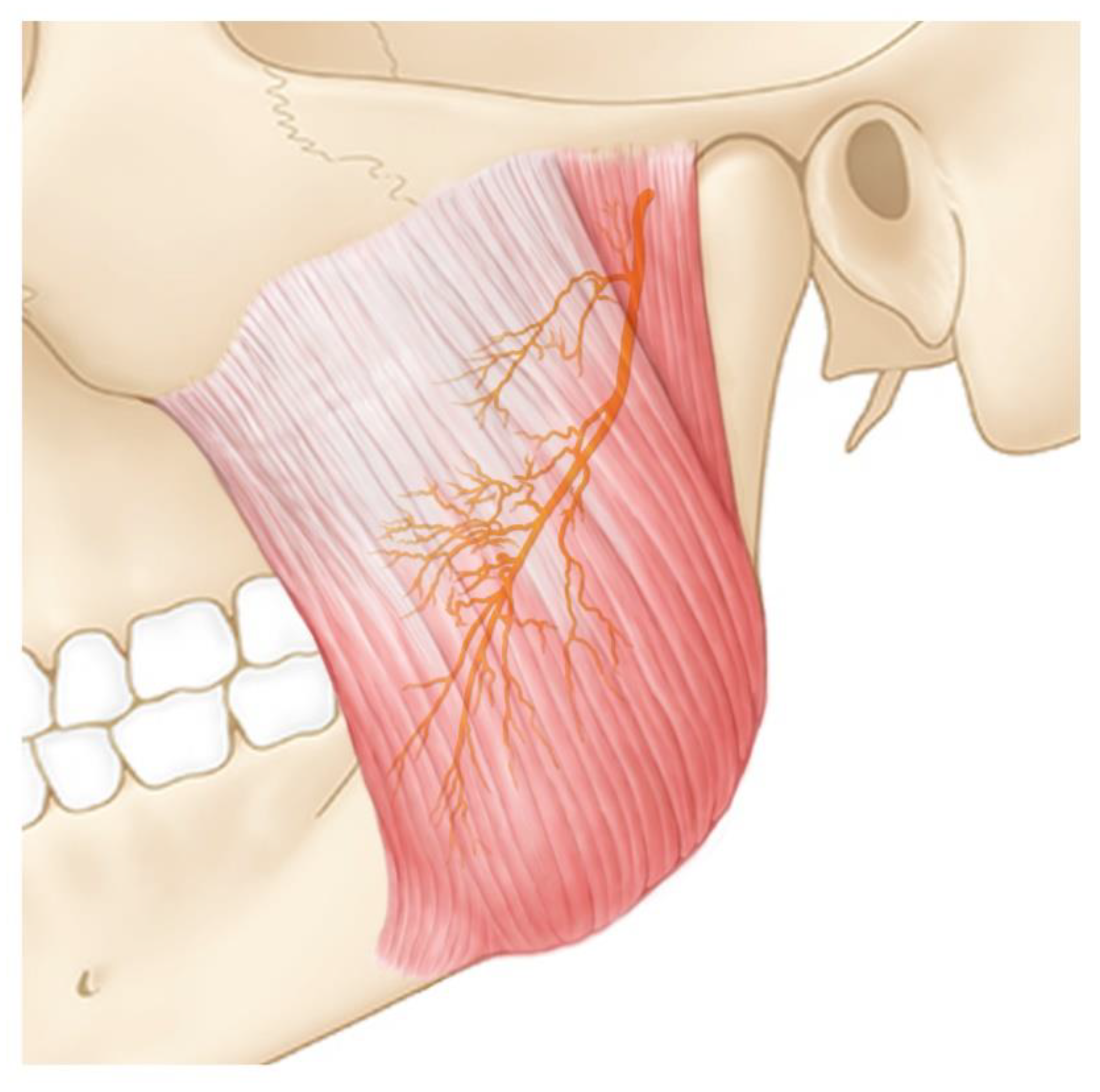
Deep Tendons of the Upper Part of the Masseter
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, H.J.; Kang, I.W.; Seo, K.K.; Choi, Y.J.; Kim, S.T.; Hu, K.S.; Kim, H.J. The anatomical basis of paradoxical masseteric bulging after botulinum neurotoxin type A injection. Toxins 2016, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Seo, K.K.; Lee, H.K.; Kim, J. Clinical Anatomy of the Face for Filler and Botulinum Toxin Injection; Springer: Berlin, Germany, 2015. [Google Scholar]
- Park, M.Y.; Ahn, K.Y.; Jung, D.S. Botulinum toxin type a treatment for contouring of the lower face. Dermatol. Surg. 2003, 29, 477–483. [Google Scholar] [PubMed]
- Kim, N.H.; Chung, J.H.; Park, R.H.; Park, J.B. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast. Reconstr. Surg. 2005, 115, 919–930. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Xu, H.; Dong, J.; Li, Q.; Dai, C. Prolonging the duration of masseter muscle reduction by adjusting the masticatory movements after the treatment of masseter muscle hypertrophy with botulinum toxin type A injection. Dermatol. Surg. 2015, 41, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Shim, W.H.; Yoon, S.H.; Park, J.H.; Choi, Y.C.; Kim, S.T. Effect of botulinum toxin type A injection on lower facial contouring evaluated using a three-dimensional laser scan. Dermatol. Surg. 2010, 36, 2061–2066. [Google Scholar] [CrossRef] [PubMed]
- Choe, S.W.; Cho, W.I.; Lee, C.K.; Seo, S.J. Effects of botulinum toxin type A on contouring of the lower face. Dermatol. Surg. 2005, 31, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, J.; Fagien, S.; Matarasso, S.L. Consensus recommendations on the use of botulinum toxin type a in facial aesthetics. Plast. Reconstr. Surg. 2004, 114, 1s–22s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baş, B.; Ozan, B.; Muğlali, M.; Celebi, N. Treatment of masseteric hypertrophy with botulinum toxin: A report of two cases. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e649–e652. [Google Scholar] [CrossRef] [Green Version]
- Liew, S.; Dart, A. Nonsurgical reshaping of the lower face. Aesthet. Surg. J. 2008, 28, 251–257. [Google Scholar] [CrossRef] [Green Version]
- GURNEY, C.E. Chronic bilateral benign hypertrophy of the masseter muscle. Am. J. Surg. 1947, 73, 137. [Google Scholar] [CrossRef]
- Von Lindern, J.J.; Niederhagen, B.; Appel, T.; Bergé, S.; Reich, R.H. Type a botulinum toxin for the treatment of hypertrophy of the masseter and temporal muscle: An alternative treatment. Plast. Reconstr. Surg. 2001, 107, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Silva, K.D.; Mandel, L. Bilateral temporalis muscle hypertrophy: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.J.; Kim, S.G.; Kim, Y.J.; Han, J.Y.; Choi, S.H.; Lee, S.I. Electrophysiologic change and facial contour following botulinum toxin a injection in square faces. Plast. Reconstr. Surg. 2007, 120, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.H.; Choi, D.Y.; Lee, J.G.; Seo, K.K.; Tansatit, T.; Kim, H.J. Risorius muscle_ anatomic considerations with reference to botulinum neurotoxin injection or masseteric hypertrophy. Dermatol. Surg. 2014, 40, 1334–1339. [Google Scholar] [CrossRef]
- Hu, K.S.; Kim, S.T.; Hur, M.S.; Park, J.H.; Song, W.C.; Koh, K.S.; Kim, H.J. Topography of the masseter muscle in relation to treatment with botulinum toxin type A. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 110, 167–171. [Google Scholar] [CrossRef]
- Bae, G.Y.; Yune, Y.M.; Seo, K.; Hwang, S.I. Botulinum toxin injection for salivary gland enlargement evaluated using computed tomographic volumetry. Dermatol. Surg. 2013, 39, 1404–1407. [Google Scholar] [CrossRef]
- Standring, S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 41th ed.; Elsevier Limited: New York, NY, USA, 2016. [Google Scholar]
- Kim, D.H.; Hong, H.S.; Won, S.Y.; Kim, H.J.; Hu, K.S.; Choi, J.H.; Kim, H.J. Intramuscular nerve distribution of the masseter muscle as a basis for botulinum toxin injection. J. Craniofac. Surg. 2010, 21, 588–591. [Google Scholar] [CrossRef]
- Lee, W.K.; Bae, J.H.; Hu, K.S.; Kato, T.; Kim, S.T. Anatomical recommendations for safe botulinum toxin injection into temporalis muscle: A simplified reproducible approach. Surg. Radiol. Anat. 2017, 39, 263–269. [Google Scholar] [CrossRef]
- Kwon, J.S.; Kim, S.T.; Jeon, Y.M.; Choi, J.H. Effect of botulinum toxin type A injection into human masseter muscle on stimulated parotid saliva flow rate. Int. J. Oral Maxillofac. Surg. 2009, 38, 316–320. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, W.J.; Lee, H.J.; Lee, K.W.; Kim, H.J.; Hu, K.S. Effective botulinum toxin injection guide for treatment of temporal headache. Toxins 2016, 8, 265. [Google Scholar] [CrossRef] [Green Version]
- Durham, P.L.; Cady, R. Insights into the mechanism of onabotulinumtoxinA in chronic migraine. Headache 2011, 51, 1573–1577. [Google Scholar] [CrossRef] [PubMed]
- Gaudy, J.F.; Zouaoui, A.; Bravetti, P.; Charrier, J.L.; Guettaf, A. Functional organization of the human masseter muscle. Surg. Radiol. Anat. 2000, 22, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Widmer, C.G.; English, A.W.; Morris-Wiman, J. Developmental and functional considerations of masseter muscle partitioning. Arch. Oral Biol. 2007, 52, 305–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cioffi, I.; Gallo, L.M.; Palla, S.; Erni, S.; Farella, M. Macroscopic analysis of human masseter compartments assessed by magnetic resonance imaging. Cells Tissues Organs 2012, 195, 465–472. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Superficial Tendon Only | Both Superficial and Deep Tendons | |||
|---|---|---|---|---|
| Type 1a | Type 1b | Type 1c | Type 2 | |
| 21.2% (7/33) | 24.2% (8/33) | 30.3% (10/33) | 15.2% (5/33) | 9.1% (3/33) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-L.; Cho, H.J.; Bae, H.; Park, H.J.; Park, M.S.; Kim, H.-J. Anatomical Considerations When Treating Compensatory Hypertrophy of the Upper Part of the Masseter after Long-Term Botulinum Neurotoxin Type A Injections. Toxins 2020, 12, 202. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030202
Lee K-L, Cho HJ, Bae H, Park HJ, Park MS, Kim H-J. Anatomical Considerations When Treating Compensatory Hypertrophy of the Upper Part of the Masseter after Long-Term Botulinum Neurotoxin Type A Injections. Toxins. 2020; 12(3):202. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030202
Chicago/Turabian StyleLee, Kyu-Lim, Hyun Jin Cho, Hyungkyu Bae, Hyun Jin Park, Min Sun Park, and Hee-Jin Kim. 2020. "Anatomical Considerations When Treating Compensatory Hypertrophy of the Upper Part of the Masseter after Long-Term Botulinum Neurotoxin Type A Injections" Toxins 12, no. 3: 202. https://0-doi-org.brum.beds.ac.uk/10.3390/toxins12030202